Introduction & Epidemiology
Fractures of the proximal tibia, particularly those involving the articular surface, represent a significant orthopedic challenge due to their complex anatomy, weight-bearing function, and propensity for devastating long-term sequelae such as post-traumatic arthritis, malunion, and instability. Tibial plateau fractures account for approximately 1% of all fractures and 8% of fractures in the elderly population. The traditional classification systems, notably Schatzker and AO/OTA, have been instrumental in categorizing these injuries and guiding treatment. However, an increasing understanding of fracture morphology, particularly with advanced imaging modalities like computed tomography (CT) scans with 3D reconstructions, has highlighted the prevalence and biomechanical significance of posteromedial fragments.
Historically, the management of complex bicondylar tibial plateau fractures often relied on anterolateral approaches, sometimes combined with medial column buttressing via a separate medial incision or indirect reduction. However, this strategy frequently failed to adequately address posteromedial displacement and depression, leading to residual varus instability and functional deficits. The recognition that a large posteromedial fragment is commonly present in Schatzker Type IV, V, and VI fractures, as well as in specific AO/OTA classifications (e.g., 41-B3, 41-C3), has underscored the necessity for direct visualization and stable fixation of this critical posteromedial column. The posteromedial approach to the proximal tibia has emerged as an indispensable tool, allowing for direct reduction and buttress plating of these fragments, thereby providing crucial stability against varus collapse and improving long-term outcomes. This approach is often the initial stage in the surgical reconstruction of complex bicondylar fractures, establishing a stable foundation upon which the remaining articular and metaphyseal reconstruction can proceed.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the proximal tibia is paramount for safe and effective utilization of the posteromedial approach.
Bony Anatomy
The proximal tibia presents a complex architecture. Key anatomical landmarks relevant to this approach include:
*
Medial Tibial Condyle:
Forms the medial aspect of the knee joint.
*
Posteromedial Tibial Plateau:
The target area for fixation, often displaced or depressed. Its obliquity and the presence of the posterior oblique ligament insertion are crucial for stability.
*
Pes Anserinus Insertion:
Composed of the sartorius, gracilis, and semitendinosus tendons, inserting onto the anteromedial aspect of the proximal tibia, distal to the joint line. These tendons must be carefully managed.
*
Gerdy's Tubercle:
Located on the anterolateral aspect, often used as a reference point for other approaches but important to delineate its position relative to the posteromedial exposure.
*
Tibial Tuberosity:
Distal to the joint line, serving as the insertion of the patellar tendon.
Soft Tissue Anatomy
The layers encountered during the posteromedial approach are critical:
*
Skin and Subcutaneous Tissue:
Relatively robust on the posteromedial aspect compared to the anterior surface, often sparing this region from severe blistering or soft tissue compromise post-trauma.
*
Superficial Fascia:
Contains the great saphenous vein and the saphenous nerve (a terminal branch of the femoral nerve). These structures run obliquely across the field and require careful identification and protection. The saphenous nerve supplies sensation to the medial aspect of the leg and foot.
*
Pes Anserinus:
The conjoined tendons of the sartorius, gracilis, and semitendinosus insert as a broad sheet on the anteromedial tibia. These must be elevated as a single unit or individually retracted.
*
Deep Fascia:
Lies beneath the pes anserinus and covers the deep musculature.
*
Musculature:
*
Medial Head of Gastrocnemius:
Originates from the medial femoral condyle and forms part of the posterior wall.
*
Soleus Muscle:
Originates from the posterior aspect of the tibia and fibula, lying deep to the gastrocnemius.
*
Popliteus Muscle:
Located deep and superiorly, important for posterior knee stability.
*
Flexor Digitorum Longus and Tibialis Posterior:
Deeper muscles lying posterior to the tibia.
*
Neurovascular Structures:
*
Popliteal Artery and Vein:
These major neurovascular structures lie posteriorly in the popliteal fossa, deep to the gastrocnemius and superficial to the popliteus. While not directly in the field, aggressive retraction or misplaced dissection posteriorly carries a significant risk of injury.
*
Posterior Tibial Artery and Tibial Nerve:
These descend distally in the deep posterior compartment.
*
Geniculate Arteries:
Multiple branches of the popliteal artery that supply the knee joint and surrounding structures. Careful dissection and electrocautery are required to manage these small vessels.
Biomechanics
The biomechanical rationale for the posteromedial approach and buttress plating is founded on the principles of fracture stability and load transmission:
*
Varus Deformity Prevention:
The posteromedial aspect of the proximal tibia is the primary site of compression during axial loading, especially during the stance phase of gait. When the medial column is fractured, it is prone to collapse into varus. A buttress plate applied to the posteromedial cortex directly resists this collapse, providing critical stability. This contrasts with plates placed solely on the anterior or anterolateral aspects, which may not effectively counteract varus collapse.
*
Load Sharing:
By placing a plate on the compression side, the implant shares the load with the bone, reducing stress shielding and promoting earlier weight-bearing capability compared to tension-sided plating.
*
Direct Reduction:
Direct visualization and reduction of the posteromedial fragment allow for anatomical restoration of the articular surface and metaphyseal support, which is often difficult to achieve indirectly through other approaches. This precise reduction is crucial for restoring joint congruity and preventing post-traumatic degenerative changes.
*
Soft Tissue Envelope:
As noted, the posteromedial soft tissue envelope often remains relatively uninjured compared to the anterior aspect, which can be subject to significant blistering, degloving, or open wounds, thereby offering a more favorable environment for surgical intervention and wound healing.
Indications & Contraindications
The posteromedial approach to the proximal tibia is indicated for a range of complex fractures and other conditions, primarily focusing on restoring the integrity of the medial and posterior aspects of the proximal tibia.
Indications
- Open Reduction and Internal Fixation (ORIF) of Fractures of the Medial Tibial Plateau (Schatzker Type IV): These fractures involve the medial condyle and often include significant posterior displacement or depression of the posteromedial fragment. The approach allows direct reduction and stable buttress plating.
- ORIF of Complex Bicondylar Tibial Plateau Fractures (Schatzker Types V and VI): In these high-energy injuries, the posteromedial fragment is frequently involved and crucial for establishing initial stability of the medial column. The posteromedial approach is often used in conjunction with an anterolateral approach (dual plating) to achieve comprehensive fixation.
- Specific AO/OTA Classification Patterns: Fractures involving the medial column and posterior aspects (e.g., 41-B3.1, 41-B3.2, 41-C1.3, 41-C2.3, 41-C3) where a significant posteromedial fragment requires direct reduction and fixation.
- Upper Tibial Osteotomy: For corrective osteotomies (e.g., high tibial osteotomy for varus malalignment), this approach provides excellent exposure for wedge resection and plate application.
- Drainage of Abscess: When an abscess is located on the posteromedial aspect of the proximal tibia, this approach provides direct access for drainage.
- Biopsy of Tumors: For suspicious lesions or tumors in the posteromedial proximal tibia, this approach allows for direct biopsy while minimizing contamination of other compartments.
Contraindications
Absolute Contraindications:
*
Active Infection:
Uncontrolled systemic or local infection in the surgical field.
*
Severe Soft Tissue Compromise:
Extensive local soft tissue damage, severe blistering, skin necrosis, or impending compartment syndrome that would preclude safe surgical exposure and wound closure. In such cases, external fixation with delayed definitive fixation or alternative treatment strategies may be required.
*
Inadequate Surgical Expertise:
The complexity of the approach and the surrounding neurovascular structures necessitate a surgeon proficient in proximal tibia trauma and posterior knee anatomy.
Relative Contraindications:
*
Extensive Comorbidities:
Patients with severe medical comorbidities (e.g., uncontrolled diabetes, severe peripheral vascular disease, immunosuppression) that significantly increase anesthetic and surgical risks.
*
Extremely Osteoporotic Bone:
While not a strict contraindication, severe osteoporosis can make stable fixation challenging, potentially requiring specialized implants or cement augmentation.
*
Fractures Not Involving the Posteromedial Column:
If the fracture pattern does not involve the posteromedial aspect, alternative approaches may be more appropriate and less invasive.
Operative vs. Non-Operative Indications Table
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Pattern | Displaced Schatzker Type IV, V, VI, or complex AO/OTA patterns with significant posteromedial fragment displacement/depression. | Non-displaced or minimally displaced (≤2-3mm articular step-off/gap) Schatzker Type I, II, III (often without posteromedial involvement), or stable undisplaced medial condyle fractures. |
| Articular Incongruity | Articular step-off > 2mm or joint depression > 2mm. | Articular step-off ≤ 2mm, no significant joint depression. |
| Varus Malalignment | Varus angulation > 5-10 degrees or impending varus collapse. | Stable alignment without significant varus angulation. |
| Associated Injuries | Ligamentous instability requiring concomitant repair/reconstruction, compartment syndrome. | Isolated fracture without significant ligamentous injury or neurovascular compromise. |
| Soft Tissues | Favorable soft tissue envelope allowing safe surgical exposure. | Significant soft tissue compromise (severe blistering, open wounds, degloving) preventing immediate surgery; managed with initial external fixation then reassessment for delayed ORIF if deemed necessary. |
| Patient Factors | Young, active patient with high functional demands; medically fit for surgery. | Elderly, low-demand patient with significant comorbidities, where surgical risks outweigh benefits; or patient unwilling/unable to comply with post-operative rehabilitation. |
| Goals | Anatomic reduction, stable internal fixation, early range of motion, prevention of post-traumatic arthritis and deformity. | Symptomatic management, immobilization, gradual weight-bearing progression, acceptance of potential minor malunion in low-demand patients. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical to the success of complex proximal tibia fracture fixation via the posteromedial approach.
Pre-Operative Planning
-
Clinical Assessment:
- Neurovascular Status: Thorough assessment of distal pulses, sensation, and motor function is essential. Any deficits should be documented.
- Soft Tissue Envelope: Inspection for open wounds, abrasions, severe blistering, or signs of impending compartment syndrome. Staged management (external fixation followed by delayed ORIF) may be necessary if soft tissues are compromised.
- Compartment Syndrome Evaluation: High index of suspicion, especially with high-energy mechanisms.
-
Imaging Review:
- Plain Radiographs: Anteroposterior, lateral, and oblique views provide an initial assessment of the fracture pattern.
- Computed Tomography (CT) Scan with 3D Reconstructions: Indispensable for detailed understanding of articular depression, comminution, and fragment orientation, particularly for identifying and characterizing posteromedial fragments. 3D reconstructions are invaluable for visualizing the overall fracture morphology and planning reduction maneuvers.
- Magnetic Resonance Imaging (MRI): May be indicated if significant ligamentous or meniscal injuries are suspected, although typically not a primary tool for fracture planning itself.
-
Templating and Implant Selection:
- Plate Type: Specific pre-contoured posteromedial tibial plates are available and highly recommended. Alternatively, L-plates or T-plates can be used. The plate should be adequate in length to achieve sufficient working screws distally.
- Screw Type: Locking screws are generally preferred for metaphyseal comminution and osteoporotic bone to provide angular stability. Non-locking cortical screws may be used for compression in simple patterns.
- Reduction Tools: Have a variety of reduction clamps, pointed reduction forceps, bone hooks, and joysticks available.
-
Surgical Strategy:
- Approach Selection: Determine if a solitary posteromedial approach is sufficient or if a dual approach (e.g., posteromedial combined with anterolateral) is required for bicondylar injuries.
- Reduction Sequence: Plan the order of fragment reduction. Often, the posteromedial fragment is addressed first to establish a stable foundation.
- Contour of Implants: Pre-bending of plates should be considered based on the CT scan if pre-contoured plates are not available or fit perfectly.
Patient Positioning
Place the patient in a
supine position
on a radiolucent operating table.
*
Leg Preparation:
The affected limb should be prepared and draped freely to allow for full range of motion of the knee and hip during surgery.
*
Radiolucent Table:
Essential for intra-operative fluoroscopic imaging in both anteroposterior and lateral planes to confirm reduction and implant placement.
*
Tourniquet:
A pneumatic tourniquet applied high on the thigh is typically used to achieve a bloodless field, which is crucial for identifying neurovascular structures and achieving precise reduction.
*
Knee Flexion:
The knee is typically positioned in 15-20 degrees of flexion, which may be supported by a bolster or bump under the distal femur. This provides a relaxed posterior capsule and may facilitate exposure.
*
Hip Flexion/External Rotation:
To enhance exposure of the posteromedial aspect, the ipsilateral hip can be slightly flexed and externally rotated, which rotates the leg laterally. Alternatively, some surgeons prefer to slightly elevate the contralateral leg to maintain a neutral position for the affected limb.
*
C-arm Access:
Ensure unrestricted C-arm access from both sides of the table for true AP and lateral views. For the posteromedial approach, specific oblique views (e.g., posteromedial oblique) may also be useful to visualize the reduction of the fragment.
*
Padding:
Meticulous padding of all pressure points, especially the contralateral limb, is critical to prevent nerve palsies or skin breakdown during prolonged procedures.
Detailed Surgical Approach / Technique
The posteromedial approach offers direct access to the posteromedial aspect of the proximal tibia, enabling anatomical reduction and stable fixation of complex fragments.
Incision
A curvilinear incision is made, beginning proximally approximately 2-3 cm posterior to the posteromedial aspect of the medial femoral epicondyle, extending distally along the posteromedial border of the tibia. The incision generally follows the posteromedial crest of the tibia for about 8-12 cm, depending on the fracture pattern and required exposure.
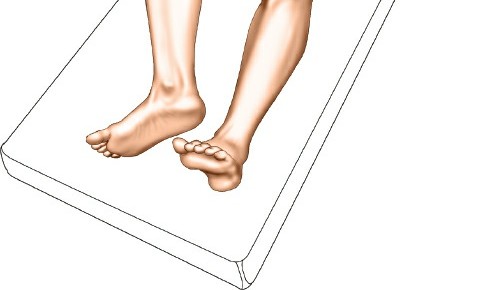
Figure 1: Skin incision for the posteromedial approach, extending along the posteromedial border of the proximal tibia.
Superficial Dissection
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue.
-
Great Saphenous Vein and Saphenous Nerve:
The great saphenous vein and its accompanying saphenous nerve branches are typically encountered superficially. These structures should be carefully identified, ligated if necessary (for the vein), or retracted anteriorly with the skin flap. Meticulous dissection is required to protect the saphenous nerve from injury.
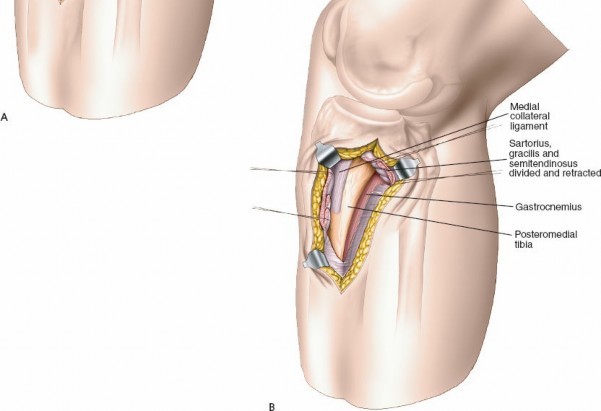
Figure 2: Superficial dissection demonstrating the identification and protection of the great saphenous vein and saphenous nerve.
Deep Dissection and Internervous Plane
- Deep Fascia and Pes Anserinus: Incise the deep fascia. The pes anserinus tendons (sartorius, gracilis, semitendinosus) insert broadly on the anteromedial aspect of the tibia, distal to the joint line. These tendons are sharply elevated as a single musculotendinous unit from their tibial insertion. This elevation creates an anteriorly based flap containing the pes anserinus.
-
Gastrocnemius and Soleus:
Posterior to the elevated pes anserinus, the medial head of the gastrocnemius muscle is identified. The internervous plane for this approach is between the medial head of the gastrocnemius (innervated by the tibial nerve) posteriorly and the pes anserinus tendons (sartorius by femoral nerve, gracilis by obturator nerve, semitendinosus by tibial nerve) anteriorly. The medial head of the gastrocnemius and potentially the proximal fibers of the soleus muscle are then carefully elevated subperiosteally from the posterior aspect of the tibia. This dissection should proceed cautiously, staying close to the bone to protect the posterior neurovascular structures.
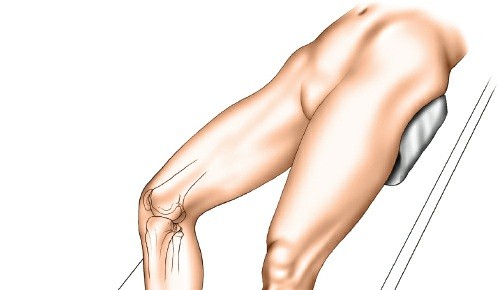
Figure 3: Elevation of the pes anserinus and medial head of gastrocnemius from the posterior tibia, exposing the posteromedial bone.
Exposure of the Fracture
Retract the elevated musculotendinous flap anteriorly, using broad retractors such as Hohmanns or specific posterior tibial retractors. The fracture site on the posteromedial aspect of the proximal tibia will now be directly visualized. Identify the posteromedial fragment, which often includes a portion of the articular surface and metaphyseal bone.

Figure 4: Direct visualization of the comminuted posteromedial fracture fragment after muscle retraction.
Fracture Reduction
- Debridement and Visualization: Clear the fracture site of hematoma, loose bone fragments, and soft tissue interposition to optimize visualization of the articular surface and fracture lines.
-
Direct Reduction:
- Articular Surface Restoration: Using pointed reduction forceps, bone hooks, or joysticks (K-wires driven into fragments), manipulate the posteromedial fragment back into its anatomical position. Direct visualization allows for precise restoration of the articular congruity.
- Metaphyseal Support: If there is metaphyseal comminution or void, bone graft (autograft or allograft) can be packed beneath the reduced articular surface to provide structural support.
-
Temporary Fixation:
Once anatomical reduction is achieved, secure the fragment temporarily with K-wires. These wires should be placed to avoid interfering with planned plate and screw placement.

Figure 5: Reduction of the articular surface of the posteromedial fragment using pointed reduction forceps and joystick technique.
Internal Fixation
-
Plate Application:
Select an appropriately contoured posteromedial tibial plate. Position the plate on the posteromedial aspect of the tibia, ensuring it buttresses the reduced fragment effectively. The plate should sit directly on the bone.
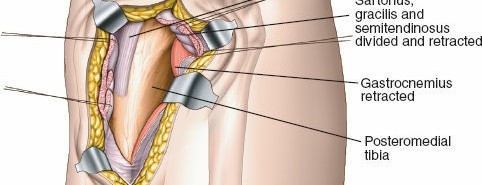
Figure 6: Application of a pre-contoured locking plate to the posteromedial aspect of the reduced tibia. -
Screw Insertion:
- Proximal Screws: Insert locking screws through the plate into the reduced articular fragment, ensuring subchondral support. Aim for bicortical purchase if possible and safe, considering the proximity to the knee joint. Care must be taken to avoid intra-articular screw placement. Fluoroscopy in multiple planes is essential to confirm screw length and position.
- Distal Screws: Insert locking screws into the tibial shaft to secure the plate. These typically aim for bicortical purchase.
-
Compression Screws (Optional):
If a simple fracture line exists, a non-locking cortical screw can be used in an eccentric hole to provide interfragmentary compression before locking screws are placed.
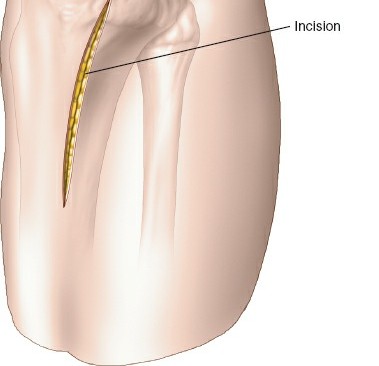
Figure 7: Fluoroscopic image (AP view) confirming adequate reduction and satisfactory plate and screw placement.
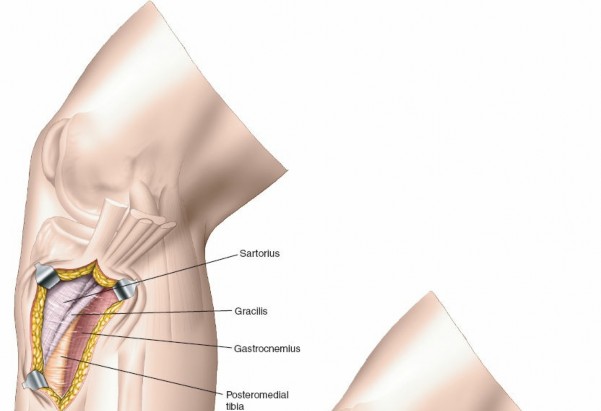
Figure 8: Fluoroscopic image (Lateral view) confirming appropriate posterior plate position and screw lengths, avoiding joint penetration.
-
Assessment of Stability:
After fixation, gently range the knee through its functional arc of motion to assess fracture stability and ensure no impingement or loss of reduction occurs.
Figure 9: Post-fixation clinical image showing stable construct and soft tissue closure.
Closure
- Hemostasis: Release the tourniquet and ensure meticulous hemostasis.
- Drain Placement: A suction drain may be placed in the deep tissues if significant bleeding or dead space is anticipated.
- Muscle and Fascia Repair: Reattach the elevated pes anserinus and gastrocnemius/soleus musculature to their original positions or to the deep fascia, restoring anatomical layers.
- Subcutaneous and Skin Closure: Close the subcutaneous tissue and skin in layers. A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique, complications can arise following the posteromedial approach to the proximal tibia. Prompt recognition and appropriate management are crucial for optimal outcomes.
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Infection | 2-10% (higher in open fractures or compromised soft tissues) | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, thorough irrigation, intravenous antibiotics, negative pressure wound therapy (NPWT), consideration of implant removal if infection persists or bone healing is achieved, or retention if stability is critical and organism is susceptible. Staged reconstruction if bone defect. |
| Non-Union/Malunion | 5-15% | Non-union: Revision ORIF with debridement, bone grafting (autograft/allograft), plate exchange (stronger construct), biologics (e.g., BMPs), external fixation. Malunion (Varus collapse): Corrective osteotomy (e.g., opening wedge HTO), revision ORIF if early, total knee arthroplasty (TKA) for symptomatic post-traumatic arthritis. |
| Post-traumatic Arthritis | Up to 50% in complex fractures, long-term | Symptomatic management (NSAIDs, injections, physical therapy), arthroscopy (debridement), osteotomy (if malalignment), unicompartmental knee arthroplasty, total knee arthroplasty. |
| Neurovascular Injury | Rare (<1%), but severe consequences | Saphenous Nerve: Reassurance, neurolysis if persistent painful neuroma. Popliteal/Posterior Tibial Vessels: Immediate surgical exploration, vascular repair (direct repair, interposition graft), fasciotomy for limb salvage. |
| Hardware Prominence/Irritation | 10-20% | Hardware removal after fracture union, typically 12-18 months post-surgery. |
| Compartment Syndrome | 1-5% (often pre-existing or early post-op) | Immediate four-compartment fasciotomy. |
| Wound Dehiscence/Necrosis | 5-10% (higher with compromised soft tissues) | Local wound care, NPWT, debridement, flap coverage (plastic surgery consultation) for larger defects, delayed closure. |
| Stiffness/Arthrofibrosis | Common, especially with prolonged immobilization | Aggressive physical therapy, continuous passive motion (CPM), manipulation under anesthesia, arthroscopic lysis of adhesions. |
| Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) | DVT: 10-40% (without prophylaxis); PE: 1-5% (without prophylaxis) | Pharmacological prophylaxis (LMWH, fondaparinux), mechanical prophylaxis (SCDs), early mobilization. Treatment involves anticoagulation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional outcomes and preventing stiffness and long-term disability. Protocols must be individualized based on fracture stability, bone quality, patient comorbidities, and surgeon preference. The general principles involve protection of the surgical repair, gradual restoration of range of motion, and progressive weight-bearing.
Phase I: Immediate Post-Operative (Weeks 0-6)
Goals:
* Control pain and swelling.
* Protect the surgical repair.
* Initiate early, gentle range of motion (ROM) to prevent stiffness.
* Maintain strength in uninvolved joints.
Management:
*
Weight Bearing:
Strict non-weight bearing (NWB) on the affected limb. Crutches or a walker are used for ambulation.
*
Immobilization:
A hinged knee brace is typically applied, locked in extension or a limited flexion arc (e.g., 0-30 degrees) for protected transfers and sleep. The brace is unlocked for exercises.
*
Range of Motion (ROM):
*
Passive ROM:
Gentle, pain-free passive knee flexion and extension within the protected arc (e.g., 0-90 degrees by week 6, as tolerated) with a continuous passive motion (CPM) machine or therapist assistance.
*
Active-assisted ROM:
Progress to active-assisted exercises as pain allows.
*
Ankle Pumps:
Encourage frequently to reduce DVT risk.
*
Strengthening:
*
Isometric Exercises:
Quadriceps sets, gluteal sets, hamstring sets for the affected limb.
*
Upper Body Strengthening:
For ambulation with crutches/walker.
*
Wound Care:
Monitor surgical incision for signs of infection. Dressings are changed as per protocol.
*
Cryotherapy and Elevation:
To manage swelling and pain.
Phase II: Intermediate (Weeks 6-12)
Goals:
* Achieve full, pain-free knee ROM.
* Begin active strengthening.
* Initiate protected weight-bearing.
Management:
*
Weight Bearing:
Gradual progression to partial weight bearing (PWB) as per surgeon's instructions and radiographic evidence of healing (e.g., 25% at week 6-8, 50% at week 8-10). Progress to full weight bearing (FWB) by week 10-12, usually without the brace for ambulation, if bone healing is confirmed on radiographs.
*
Immobilization:
Discontinue knee brace when bone healing allows and adequate quadriceps control is achieved, typically by week 8-10.
*
Range of Motion (ROM):
Progress towards full knee flexion and extension. Continue passive, active-assisted, and active ROM exercises.
*
Strengthening:
*
Closed Chain Exercises:
Mini-squats, leg presses (light resistance), wall slides.
*
Open Chain Exercises:
Knee extension (short arc), hamstring curls (light resistance).
*
Proprioception:
Balance exercises (e.g., single-leg stance with support).
*
Cardiovascular:
Stationary cycling (high seat, low resistance) can be introduced.
Phase III: Advanced & Return to Activity (Weeks 12+)
Goals:
* Restore full strength, power, and endurance.
* Re-establish proprioception and neuromuscular control.
* Gradual return to sport-specific or work-specific activities.
Management:
*
Weight Bearing:
Full weight bearing without assistive devices.
*
Strengthening:
*
Progressive Resistance Exercises:
Increase resistance for closed and open chain exercises.
*
Functional Exercises:
Step-ups/downs, lunges, agility drills (cutting, pivoting, jumping) as appropriate for patient's goals and functional demands.
*
Core Strengthening:
Essential for overall stability.
*
Proprioception:
Advanced balance exercises (e.g., unstable surfaces, sport-specific drills).
*
Endurance Training:
Cycling, swimming, elliptical trainer.
*
Sport-Specific Training:
Gradually introduce activities relevant to the patient's desired level of function, under supervision.
*
Return to High-Impact Activities:
Typically not before 6-12 months, and only after thorough clinical and functional assessment, and radiographic confirmation of complete union. Patients should be counselled regarding the potential for persistent discomfort or activity limitations.
Summary of Key Literature / Guidelines
The evolution of surgical management for complex proximal tibia fractures, particularly those involving posteromedial fragments, has been significantly influenced by advancements in imaging and surgical techniques. The current literature strongly supports the use of direct posteromedial approaches for specific fracture patterns.
Early studies and classifications, such as Schatzker and AO/OTA, often focused on articular depression and medial/lateral condylar involvement. However, detailed CT analysis, particularly since the early 2000s, has highlighted that up to 60-70% of bicondylar tibial plateau fractures (Schatzker V, VI) involve a significant posteromedial fragment. This recognition has driven a paradigm shift from predominantly anterolateral-only approaches to strategies incorporating direct posteromedial access.
Key Findings and Recommendations from Literature:
- Importance of Posteromedial Fixation: Multiple biomechanical and clinical studies (e.g., Luo et al., Zhai et al., Egol et al.) have demonstrated that the posteromedial column is critical for axial and rotational stability of the proximal tibia. Failure to adequately reduce and stabilize posteromedial fragments, especially in varus-prone fractures, can lead to residual varus malalignment, loss of reduction, and subsequent post-traumatic arthritis.
- Dual Plating for Bicondylar Fractures: For complex bicondylar fractures (Schatzker V/VI, AO/OTA C-type), the contemporary standard of care often involves dual plating through separate anterolateral and posteromedial incisions. This approach provides a stable quadrilateral construct, restoring both articular congruity and metaphyseal alignment. Studies (e.g., Mthethwa et al., Phisitkul et al.) indicate superior stability and reduced rates of malunion with dual plating compared to single-plate constructs or indirect reduction techniques for posteromedial fragments.
- Anatomical Reduction of Posteromedial Fragment: Direct visualization afforded by the posteromedial approach allows for anatomical reduction of the articular surface. This is paramount, as residual articular step-off >2mm is a strong predictor of early degenerative changes and poor functional outcomes (Kendall et al., Rasmussen and Rehnberg scores).
- Plate Configuration: Pre-contoured anatomical locking plates designed for the posteromedial aspect of the tibia have shown excellent biomechanical properties and clinical results. These plates function as buttress plates, resisting varus collapse and promoting load sharing.
- Soft Tissue Considerations: The inherent advantage of the posteromedial soft tissue envelope, often less compromised by high-energy trauma compared to the anterior aspect, facilitates earlier surgical intervention and reduces wound complication rates compared to extensive anterior exposures for complex patterns. However, careful handling of the great saphenous vein and saphenous nerve is critical to prevent iatrogenic injury.
- Outcomes: While posteromedial fixation improves stability and reduces malunion, the overall complication rates for complex tibial plateau fractures remain substantial. Post-traumatic arthritis is a common long-term sequela, even with optimal surgical fixation, necessitating patient counseling. Functional outcomes are often assessed using validated scores such as the Rasmussen clinical and radiological scores, the Knee Society Score (KSS), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Studies generally report good to excellent outcomes in 70-80% of patients treated with appropriate surgical techniques, including the posteromedial approach for indicated fractures.
- Surgical Education: The posteromedial approach is considered an advanced technique due to the proximity of vital neurovascular structures. Training guidelines emphasize a detailed anatomical understanding and supervised experience for orthopedic residents and fellows to safely master this approach.
In conclusion, the posteromedial approach to the proximal tibia has become an indispensable technique in the orthopedic surgeon's armamentarium for managing complex tibial plateau fractures. Its ability to provide direct visualization, anatomical reduction, and stable buttress fixation of critical posteromedial fragments significantly contributes to restoring knee stability, preserving articular congruity, and ultimately improving long-term functional outcomes for patients. Continuous advancements in implant design and surgical education further solidify its role in modern trauma care.
Clinical & Radiographic Imaging