Mastering the Tibial Plateau Posterolateral Approach
Introduction & Epidemiology
Tibial plateau fractures represent approximately 1% of all fractures, with a bimodal distribution affecting young males involved in high-energy trauma and elderly females with osteoporotic bone following low-energy falls. The posterolateral tibial plateau is a critical load-bearing region, and fractures involving this segment, particularly those with articular depression or displacement, pose significant surgical challenges. Historically, posterolateral fractures were often underdiagnosed or inadequately addressed due to the perceived difficulty of access and fixation through traditional anterolateral or medial approaches. However, improved understanding of fracture morphology, advancements in imaging, and evolving surgical techniques, including dedicated posterolateral approaches, have led to better outcomes.
Fractures involving the posterolateral corner can occur in isolation or as part of complex bicondylar injuries (e.g., Schatzker type VI, AO/OTA type 41-C3). Isolated posterolateral fractures typically result from axial loading combined with internal rotation or hyperextension, often leading to a shear fracture pattern with varying degrees of impaction. The stability of the posterolateral segment is crucial for knee kinematics, and untreated or inadequately treated injuries can result in persistent pain, instability, progressive arthritis, and functional impairment. The posterolateral approach allows for direct visualization, anatomical reduction, and stable buttress plate fixation, which is paramount for restoring articular congruity and mechanical axis.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics is fundamental for safe and effective surgical management of posterolateral tibial plateau fractures.
Osseous Anatomy
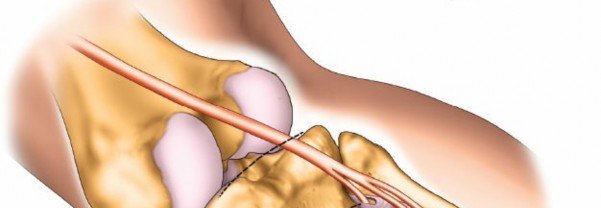
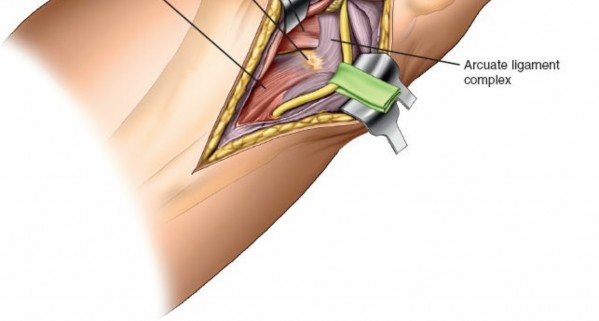
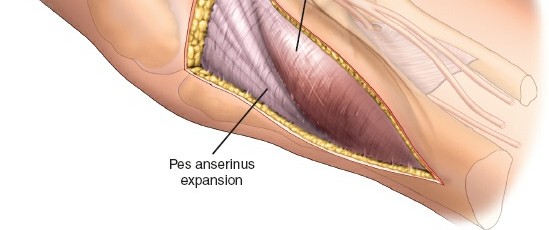
The proximal tibia consists of medial and lateral condyles, separated by the intercondylar eminence. The posterolateral plateau is characterized by its articular surface, which articulates with the lateral femoral condyle. This region is inherently less robust than the posteromedial plateau, contributing to its vulnerability. The fibular head is an important landmark, providing attachment for the biceps femoris tendon and the fibular collateral ligament (FCL). The posterolateral aspect of the proximal tibia also features the Gerdy's tubercle anteriorly and the posterolateral corner which anchors the popliteus tendon, arcuate ligament complex, and the posterior capsule.

Ligamentous and Muscular Anatomy
The posterolateral corner of the knee is a complex anatomical region composed of static and dynamic stabilizers. Key structures include:
*
Fibular Collateral Ligament (FCL):
Originates from the lateral femoral epicondyle and inserts on the fibular head.
*
Popliteus Tendon:
Originates from the lateral femoral epicondyle and inserts onto the posteromedial aspect of the proximal tibia. Its tendon runs deep to the FCL.
*
Popliteofibular Ligament (PFL):
Connects the popliteus tendon to the fibular head.
*
Arcuate Ligament Complex:
Comprises the arcuate ligament, popliteofibular ligament, and the capsular arm of the short head of the biceps femoris.
*
Biceps Femoris Tendon:
Inserts primarily onto the fibular head. The short head contributes to the posterolateral capsule.
*
Lateral Gastrocneimius Head:
Originates from the lateral femoral condyle.
*
Soleus Muscle:
Originates from the posterior aspect of the fibular head and proximal tibia.
*
Peroneus Longus and Brevis:
Originates from the fibular shaft.
These structures contribute to posterolateral rotatory stability. Surgical access through the posterolateral approach requires careful dissection between muscular layers while protecting vital neurovascular structures.
Neurovascular Structures
The
common peroneal nerve (CPN)
is the most critical neurovascular structure at risk during a posterolateral approach. It courses superficially around the fibular neck, deep to the biceps femoris tendon, before dividing into the superficial and deep peroneal nerves. Its identification and protection are paramount.

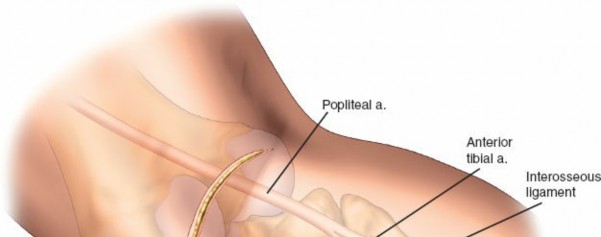
The posterior tibial neurovascular bundle (posterior tibial artery, posterior tibial veins, and tibial nerve) lies more medially and deep, generally not directly in the field of the posterolateral approach but can be at risk with extensive medial dissection or posterior instrumentation. The anterior tibial artery passes through the interosseous membrane distally.
Biomechanics
The posterolateral tibial plateau resists posterolateral translation and external rotation. Fractures in this region compromise knee stability, particularly in extension, leading to dynamic instability. Buttress plating, a cornerstone of fixation for these fractures, provides direct mechanical support to the articular segment, preventing collapse under axial load and resisting shear forces. The plate acts as a "buttress" against posterior and lateral displacement of the fracture fragment. The goal is to restore articular congruity and axial alignment to distribute joint contact forces evenly, thereby reducing the risk of post-traumatic arthritis.
Indications & Contraindications
Indications for the Posterolateral Approach
The posterolateral approach to the tibial plateau is specifically indicated for fractures involving the posterolateral corner, particularly when:
*
Direct Visualization and Reduction:
The fracture fragment is primarily posterolateral, requiring direct visualization for anatomical reduction and buttress plate application. This is essential for preventing articular incongruity.
*
Articular Depression/Displacement:
Significant articular depression (typically >2mm-3mm) or displacement (>2mm-5mm) of the posterolateral fragment.
*
Associated Instability:
Presence of posterolateral corner instability due to fracture patterns that compromise intrinsic ligamentous structures.
*
Specific Fracture Patterns:
* Pure posterolateral split or depression fractures (e.g., specific variations of Schatzker II/III, AO/OTA type 41-B3.3 with posterolateral involvement).
* Bicondylar tibial plateau fractures with a significant posterolateral component (e.g., Schatzker VI, AO/OTA type 41-C3) that cannot be adequately addressed via standard anterolateral or medial approaches.
* Posterior column fractures (e.g., Luo's three-column concept), specifically posterolateral column involvement.
*
Need for Buttress Plating:
The geometry of the fracture dictates a need for a buttress plate applied directly to the posterior aspect of the lateral tibial condyle to prevent posterior collapse.
Contraindications
Absolute contraindications for the posterolateral approach are rare and generally align with those for any open reduction and internal fixation (ORIF) procedure:
*
Active Infection:
Local or systemic active infection.
*
Severe Soft Tissue Compromise:
Compromised soft tissue envelope, significant open wounds, severe blistering, or impending compartment syndrome that would preclude safe surgical exposure or closure.
*
Insufficient Bone Stock:
Extreme comminution or bone loss making stable fixation unachievable.
*
Non-Ambulatory Status/Poor Health:
Patients with severe medical comorbidities that contraindicate prolonged anesthesia or surgical stress, or those with extremely limited functional expectations for whom the risks outweigh the benefits of aggressive fixation.
*
Unsuitability for Prone Position:
Medical conditions precluding prone positioning (e.g., severe cardiac or pulmonary compromise, morbid obesity).
Relative contraindications include severe peripheral vascular disease, uncontrolled diabetes, and prolonged tourniquet time.
Operative vs. Non-Operative Indications
The decision between operative and non-operative management for tibial plateau fractures is complex and multifactorial, depending on fracture morphology, patient factors, and associated injuries.
| Feature / Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Articular Depression | >2-3 mm depression | <2 mm depression |
| Articular Gap | >2-5 mm displacement | <2 mm displacement |
| Joint Instability | Clinical or radiographic instability (e.g., varus/valgus >10 degrees at full extension) | Stable knee |
| Open Fracture | All Gustilo-Anderson types | N/A |
| Neurovascular Injury | Acute nerve/vascular compromise requiring intervention | Intact neurovascular status |
| Compartment Syndrome | Acute onset | No signs/symptoms |
| Soft Tissue Status | Adequate for surgical exposure | Severe soft tissue swelling, blistering, or poor skin quality |
| Patient Factors | Physiologically fit, good bone quality, compliant with rehab | Significant comorbidities, severe osteoporosis with poor bone quality, non-compliance concerns |
| Associated Injuries | Polytrauma, ligamentous injuries requiring concomitant repair/reconstruction | Isolated, stable fracture without significant associated injuries |
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning is critical to anticipating challenges and ensuring a successful outcome.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: AP, lateral, and oblique views of the knee are initial screening tools. Stress radiographs may reveal instability.
-
Computed Tomography (CT) Scan:
Essential for delineating fracture morphology, articular depression, comminution, and fragment orientation. 3D reconstructions are invaluable for understanding the extent of posterolateral involvement and planning implant placement.
 - Magnetic Resonance Imaging (MRI): Indicated if associated ligamentous injuries (e.g., popliteus, FCL, meniscus) are suspected, which is common in high-energy posterolateral injuries.
- Fracture Classification: Utilize Schatzker, AO/OTA, and Luo's three-column classification systems to fully characterize the fracture. The posterolateral column is distinct and requires specific attention.
- Implant Selection: Pre-contoured posterolateral-specific locking plates are generally preferred. These are designed to conform to the posterior anatomy of the lateral tibial condyle. Determine appropriate plate length and screw trajectory.
- Surgical Strategy: Plan the incision, anticipated dissection planes, reduction techniques (e.g., indirect reduction with an external fixator, direct visualization), and sequence of fixation.
- Tourniquet: A thigh tourniquet is typically used to minimize blood loss and improve visualization.
- Antibiotics: Prophylactic intravenous antibiotics administered within 60 minutes of incision.
Patient Positioning
The patient is positioned
prone
on the operating table, as indicated in the seed content.

Key considerations for prone positioning:
*
Support:
Ensure adequate padding to all pressure points (chest, pelvis, ankles) to prevent nerve compression or skin breakdown.
*
Limb Position:
* The operative limb is allowed to naturally externally rotate.
* A small pillow or bolster is placed under the ankle to flex the knee approximately 20 degrees. This provides optimal exposure of the posterolateral corner and relaxes soft tissues.
*
Fluoroscopy Access:
Confirm that the C-arm can obtain adequate AP, lateral, and oblique views of the proximal tibia and knee joint without repositioning the patient. The operating table should be radiolucent.
*
Sterile Prep and Drape:
A wide sterile field from the upper thigh to the foot is prepared and draped to allow for adequate exposure and manipulation of the limb.
*
Contralateral Limb:
Padded and positioned comfortably.
*
Potential for Conversion:
While not typically required, be prepared for a lateral or anterolateral approach if fracture pattern or concomitant injuries necessitate.
Detailed Surgical Approach / Technique
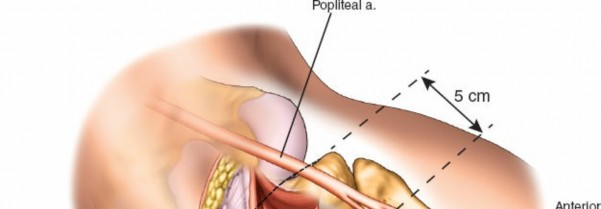
The posterolateral approach provides excellent direct visualization of the posterolateral tibial plateau and the posterior aspect of the fibular head. It is essentially an extensile approach to the posterolateral aspect of the proximal tibia.
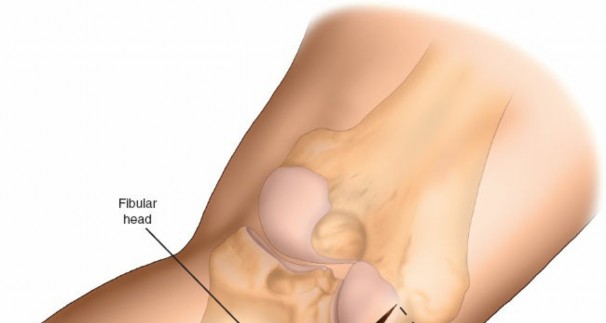
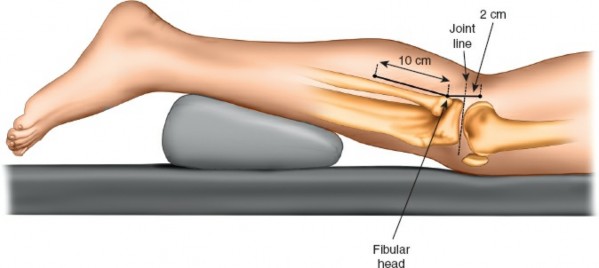
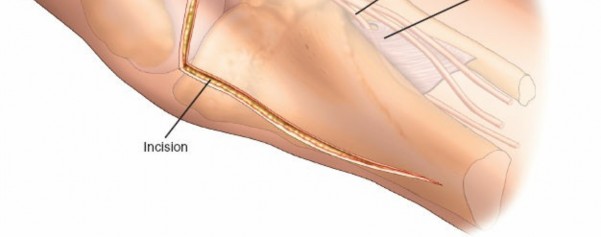
1. Landmarks and Incision
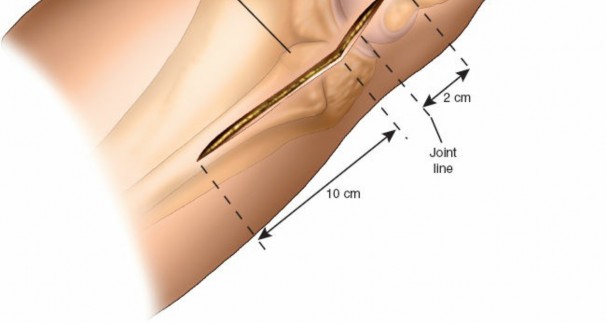
- Palpate the fibular head, which is approximately 2 to 3 cm below the lateral femoral condyle.
- Make a 10-cm longitudinal incision centered over the posterolateral aspect of the lower leg.
-
Begin the incision approximately 2 cm above the knee crease and extend it distally to follow the medial border of the fibular head and neck.

This incision aims to avoid the common peroneal nerve anterior to the biceps femoris tendon.
2. Superficial Dissection
- Incise the skin and subcutaneous tissues.
- Identify the deep fascia.
-
Bluntly dissect through the subcutaneous fat, carefully preserving sensory nerves and superficial veins.
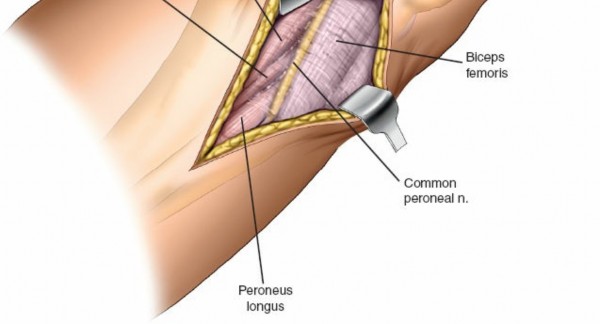
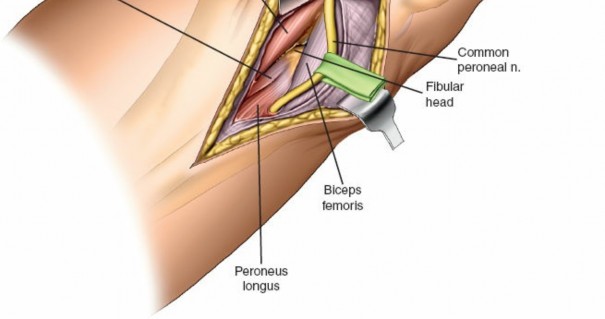
3. Common Peroneal Nerve Identification and Protection
This is the most critical step of the approach.
* Identify the biceps femoris tendon, which inserts onto the fibular head.
* The common peroneal nerve (CPN) typically runs along the medial border of the biceps femoris tendon, curving around the posteromedial aspect of the fibular neck. It lies deep to the tendon.
* Carefully expose the CPN as it wraps around the fibular neck. This typically involves dissecting between the biceps femoris tendon and the gastrocnemius.
* Once identified, gently mobilize the nerve and protect it with a vessel loop or Penrose drain. Retract it anteriorly and superiorly.

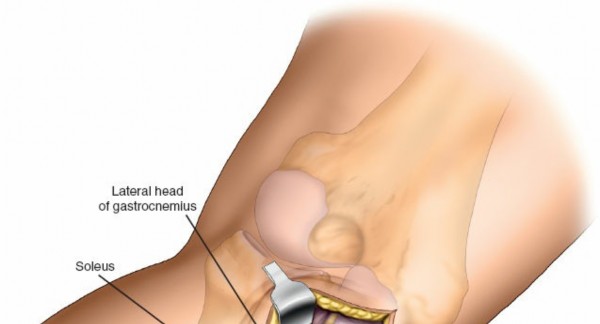
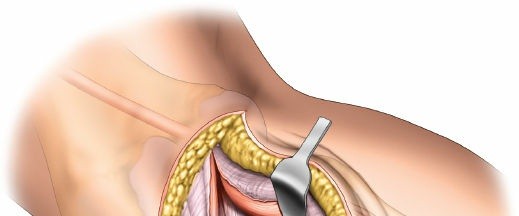
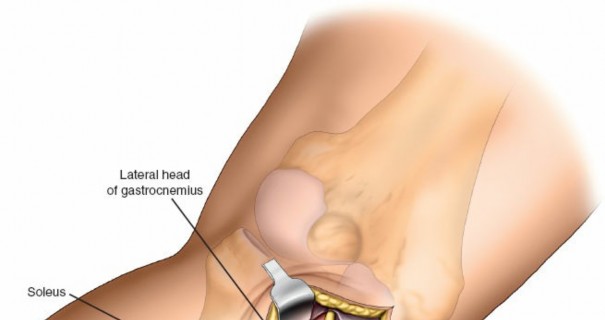
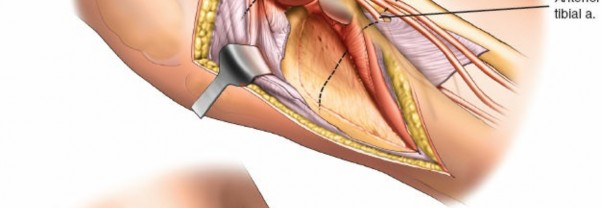
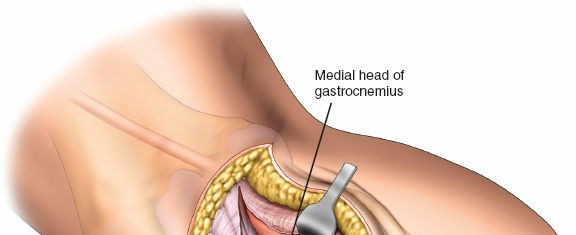
4. Deep Dissection and Internervous Plane
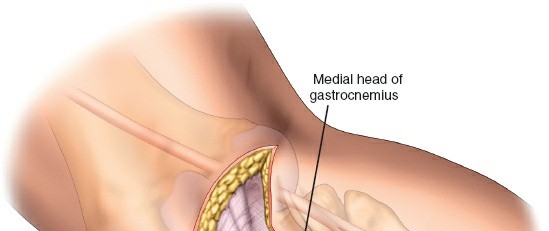
- The approach utilizes the internervous plane between the lateral head of the gastrocnemius and the soleus muscle, or sometimes between the lateral head of the gastrocnemius and the peroneal musculature.
- Retract the lateral head of the gastrocnemius posteriorly and medially.
- Identify the soleus muscle and the deep fascia of the leg.
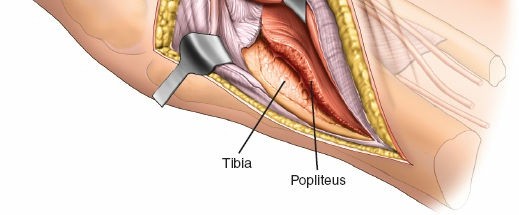
- Incise the fascia over the soleus muscle.
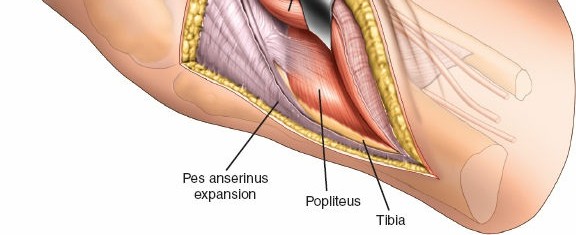
-
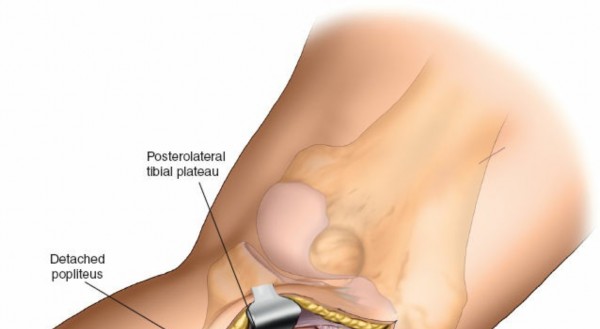
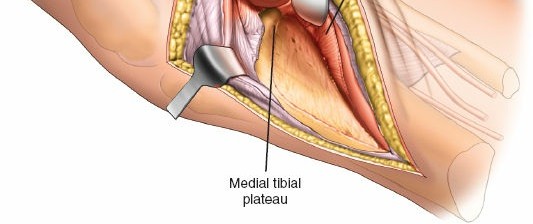
Elevate the soleus muscle anteriorly and laterally off the posterior surface of the proximal tibia and fibula.
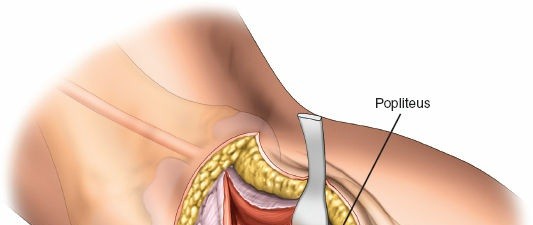
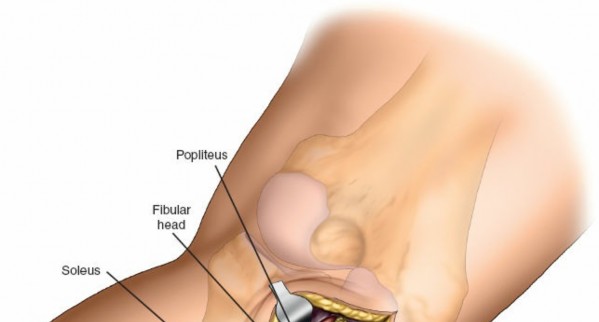
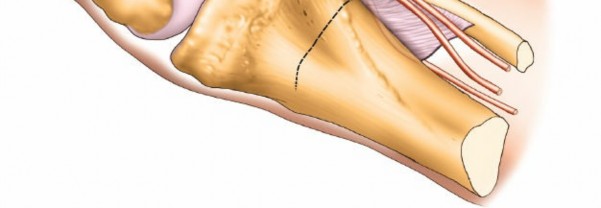
 - The popliteus muscle and its tendon run obliquely across the posterior aspect of the tibia. Its tibial insertion may need to be partially released to gain full access to the posterolateral plateau, especially for more posterior or distal fractures. Exercise caution to avoid injury to the neurovascular bundle lying medial to the popliteus.
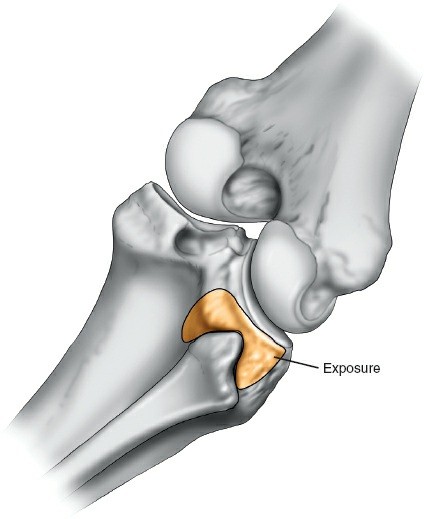
-
The posterolateral joint capsule is incised longitudinally to expose the fracture fragments.
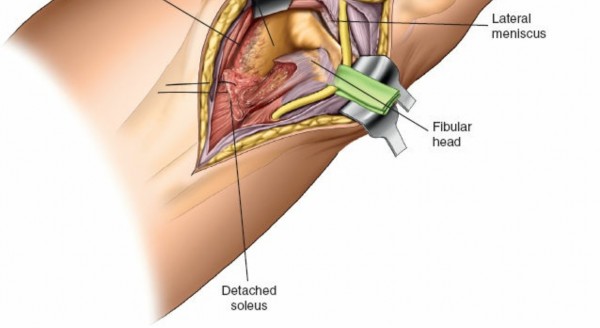
5. Fracture Reduction
- Debridement: Clear the fracture site of hematoma, loose bone fragments, and meniscal interposition. The lateral meniscus may be detached or torn; it should be carefully assessed.
- Visualization: Direct visualization of the articular surface is paramount. Use a periosteal elevator or a small retractor to lift the depressed articular segment.
-
Reduction Techniques:
- Indirect Reduction: For initial alignment, longitudinal traction or a temporary spanning external fixator can be employed. This helps restore overall limb length and alignment.
-
Direct Reduction:
- Use a large ball-tipped probe or a small curette to elevate the depressed articular fragments from below, working through the metaphyseal defect.
- Impacted cancellous bone beneath the articular surface must be elevated.
- Visualize the articular surface directly or indirectly with arthroscopy (if used) to confirm reduction.
-
Bone Grafting:
Once the articular surface is reduced and supported, the metaphyseal void created by the elevation should be filled with autogenous cancellous bone graft (e.g., iliac crest or local cancellous bone) or an allograft/bone substitute. This provides structural support and promotes healing.
-
Temporary Fixation:
Use K-wires or provisional screws to maintain reduction. Confirm articular congruity and overall alignment with fluoroscopy in multiple planes (AP, lateral, obliques).
6. Internal Fixation
- Plate Application: A pre-contoured posterolateral locking plate is carefully positioned along the posterolateral aspect of the tibia. The plate should buttress the fracture fragment and conform to the anatomy. Ensure the plate does not impinge on the joint capsule or articular cartilage.
-
Screw Insertion:
- Begin with a non-locking screw through a compression slot (if available) to pull the plate to the bone and provide initial stability.
- Insert locking screws, paying careful attention to trajectory. Screws should be directed towards stable bone fragments, avoiding joint penetration. Use fluoroscopy to confirm screw length and position.
- Lag screws can be used through the plate or separately to compress specific articular fragments, especially if pure shear fractures are present.
-
Ensure adequate purchase in both cortical bone layers distally and in the subchondral bone proximally, without violating the joint.
- Final Assessment: Perform a final fluoroscopic check to confirm anatomical reduction, stable fixation, appropriate alignment, and absence of intra-articular hardware. Assess knee stability through a full range of motion.
7. Wound Closure
- Thoroughly irrigate the wound.
- Place a suction drain if deemed necessary, typically deep to the muscle layers, to prevent hematoma formation.
- Repair the popliteus muscle insertion if it was released.
- Close the deep fascia over the soleus muscle.
- Release the tourniquet and achieve meticulous hemostasis.
-
Close the subcutaneous layer and skin in a layered fashion.
 - Apply a sterile dressing.
- A well-padded knee immobilizer or brace is typically applied post-operatively for comfort and protection.
Complications & Management
Despite meticulous surgical technique, complications can occur. Recognition and appropriate management are crucial for optimal patient outcomes.
Intraoperative Complications
-
Common Peroneal Nerve Injury (CPNI):
The most feared complication. Can result from direct trauma, traction, or compression during retraction.
- Incidence: Varies, but reported between 2-10% for posterolateral approaches.
- Management: Immediate identification and relief of compression. If transection or significant injury is noted, primary repair or nerve grafting may be considered. Post-operatively, monitor for foot drop and sensory deficits. Consider bracing (AFO).
-
Neurovascular Injury (other):
Injury to popliteal vessels, anterior/posterior tibial arteries/nerves. Less common with proper technique.
- Management: Immediate vascular surgical consultation for repair if detected.
-
Articular Penetration:
Screws or K-wires violating the joint surface.
- Management: Intraoperative fluoroscopy and direct visualization (or arthroscopy) are essential. Immediately revise screw position.
-
Inadequate Reduction/Fixation:
Failure to achieve anatomical reduction or stable fixation.
- Management: Re-reduction and re-fixation. Consider alternative fixation strategies or supplemental plating.
Early Postoperative Complications
-
Wound Infection:
Superficial or deep surgical site infection.
- Incidence: 1-5%.
-
Management:
Superficial infections may respond to antibiotics and local wound care. Deep infections often require surgical debridement, pulsed lavage, culture-directed antibiotics, and potentially hardware removal.
-
Wound Dehiscence/Necrosis:
Particularly challenging in the posterolateral aspect due to thin soft tissue envelope and potentially extensive retraction.
- Incidence: Higher in smokers, diabetics, and those with poor tissue quality.
- Management: Local wound care, serial debridement. May require plastic surgical consultation for local flaps or free tissue transfer for coverage.
-
Compartment Syndrome:
Rare but critical.
- Management: Immediate fasciotomy if suspected.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Risk for all lower extremity trauma.
- Incidence: DVT 10-20% without prophylaxis, PE 1-2%.
- Management: Prophylaxis (chemical and mechanical) is standard. Treatment involves anticoagulation.
Late Postoperative Complications
-
Post-Traumatic Arthritis:
Most common long-term complication, even with anatomical reduction.
- Incidence: Varies widely, 20-60%, dependent on initial injury severity, reduction quality, and alignment.
- Management: Symptomatic management, physiotherapy, injections, osteotomy, or arthroplasty in severe cases.
-
Nonunion / Malunion:
Failure of fracture healing or healing in an unacceptable position.
- Incidence: <5% for nonunion, higher for malunion.
-
Management:
Nonunion may require revision surgery, bone grafting, and potentially different fixation. Malunion may require corrective osteotomy.
-
Hardware Irritation:
Symptomatic hardware requiring removal.
- Management: Hardware removal after fracture union.
-
Loss of Reduction:
Early collapse or displacement of fragments post-fixation.
- Management: Revision surgery if significant or symptomatic.
Table: Common Complications and Management Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Common Peroneal Nerve Palsy | 2-10% | Observation, neurolysis, nerve repair/grafting, AFO brace, tendon transfers. |
| Wound Infection (Deep) | 1-5% | Debridement, irrigation, culture-specific antibiotics, hardware retention/removal, flap coverage. |
| Wound Dehiscence/Necrosis | 3-7% | Local wound care, debridement, VAC therapy, primary or reconstructive soft tissue coverage (flaps). |
| Post-Traumatic Arthritis | 20-60% | Symptomatic management, intra-articular injections, osteotomy, partial/total knee arthroplasty. |
| Nonunion | <5% | Revision ORIF, bone grafting (autograft/allograft), electrical/ultrasound stimulation, exchange nailing. |
| Malunion | 5-15% | Corrective osteotomy to restore alignment and joint congruity. |
| Hardware Irritation | 10-20% | Hardware removal (after fracture union). |
| DVT/PE | 10-20% (DVT) | Prophylactic anticoagulation; therapeutic anticoagulation for confirmed DVT/PE. |
| Loss of Reduction | <5% | Revision surgery with improved fixation, potentially external fixation, bone grafting. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional outcomes following posterolateral tibial plateau fracture fixation. Protocols are individualized based on fracture stability, quality of fixation, patient comorbidities, and surgeon preference. The primary goals are to protect the repair, manage pain and swelling, restore range of motion (ROM), and gradually progress to weight-bearing and strengthening.
Phase I: Immediate Post-operative (Weeks 0-6)
- Goals: Protect fixation, control pain and swelling, initiate early, controlled motion.
- Weight-Bearing: Strictly non-weight-bearing (NWB) or touch-down weight-bearing (TTWB) on the operative extremity. Use crutches or a walker.
- Immobilization: A knee immobilizer or hinged knee brace (locked in extension) is typically used for comfort and protection, especially during transfers and ambulation. It may be removed for exercises.
-
ROM:
- CPM Machine: Continuous Passive Motion (CPM) machine may be used to aid in early, gentle ROM, typically starting from 0-30 degrees and gradually increasing as tolerated (e.g., 0-60 degrees by week 2, 0-90 degrees by week 6).
- Active-Assisted ROM (AAROM) & Gentle Passive ROM (PROM): Focus on knee flexion and extension within protected ranges.
- Ankle Pumps: Promote venous return and prevent DVT.
- Muscle Activation: Isometric quadriceps sets and gluteal sets to maintain muscle tone without stressing the fracture site.
-
Edema Control:
Elevation, compression (elastic stocking), ice.
Phase II: Early Mobility & Strengthening (Weeks 6-12)
- Goals: Increase ROM, gradually introduce weight-bearing, initiate gentle strengthening.
- Weight-Bearing: Progress from TTWB to partial weight-bearing (PWB) as tolerated, typically starting at 6-8 weeks, with progression to full weight-bearing (FWB) by 10-12 weeks, provided radiographic signs of healing are evident. Use crutches or a walker for support.
- ROM: Continue to advance knee flexion and extension towards full ROM.
-
Strengthening:
- Gentle Isometrics: Hamstring curls, straight leg raises (SLRs) with care to avoid knee flexion stress.
- Resistance Bands: Very light resistance for knee flexion/extension.
- Proprioception: Begin with balance exercises on the contralateral limb, progressing to supported single-limb stance on the operative limb.
-
Cycling:
Stationary bicycle with high seat and no resistance, focusing on fluid motion once adequate ROM is achieved.
Phase III: Functional Recovery & Return to Activity (Weeks 12+)
- Goals: Achieve full pain-free ROM, restore strength, power, endurance, and proprioception; gradual return to functional activities.
- Weight-Bearing: Full weight-bearing. Discontinue assistive devices.
-
Strengthening:
- Progressive resistance exercises (PREs) for quadriceps, hamstrings, and calf muscles.
- Closed-chain exercises (mini-squats, lunges, leg press).
- Core strengthening.
- Cardiovascular: Continue stationary cycling, introduce elliptical or swimming.
- Proprioception & Agility: Balance boards, single-leg stance activities, sport-specific drills (if applicable).
-
Return to Activity:
Gradual return to light recreational activities, advancing based on strength, pain, and functional status. High-impact or pivoting sports may be restricted for 6-12 months post-surgery.
 - Radiographic Follow-up: Regular X-rays to monitor fracture healing and alignment.
Key Considerations:
*
Pain Management:
Critical throughout rehabilitation to allow active participation.
*
Swelling Control:
Continued elevation, compression, and cryotherapy.
*
Patient Education:
Emphasize adherence to weight-bearing precautions and exercise protocols.
*
Ligamentous Stability:
If concomitant ligamentous injuries were present or repaired, the rehabilitation protocol must be adjusted to protect those structures.
Summary of Key Literature / Guidelines
The management of tibial plateau fractures, particularly those involving the posterolateral corner, has evolved significantly with advances in imaging, surgical techniques, and implant technology.
-
Classification Systems: The Schatzker classification (1974) remains widely used for its simplicity, though it may not fully capture the complexity of posterior column involvement. The AO/OTA classification (e.g., 41-B3, 41-C3) provides a more detailed description of fracture morphology. Luo's three-column classification (2010) has gained prominence for addressing posterior tibial plateau fractures, dividing the proximal tibia into medial, lateral, and posterior columns. The posterolateral approach specifically addresses fractures of the lateral and posterior columns.
 -
Surgical Approaches: Historically, posterolateral fractures were often accessed via extended anterolateral approaches with fibular head osteotomy or posteromedial approaches. However, direct posterior approaches, such as the posterolateral approach described, have demonstrated superior outcomes for specific fracture patterns. The prone position posterolateral approach offers direct visualization of the posterolateral articular surface, allowing for accurate reduction and buttress plating without violating the anterior compartment or requiring a fibular head osteotomy, thus minimizing disruption to the FCL and biceps femoris. The alternative direct posterior approach (triceps surae split) allows access to both posteromedial and posterolateral quadrants but requires more extensive muscle dissection.
-
Fixation Principles:
- Buttress Plating: Current literature strongly supports the use of buttress plating for displaced articular fragments, especially in the posterolateral corner, to counteract shear and axial forces. Pre-contoured locking plates are preferred due to their anatomical fit and fixed-angle stability, which is advantageous in osteoporotic bone.
- Dual Plating: For complex bicondylar fractures with significant posterolateral involvement (Schatzker VI, AO/OTA 41-C3), dual plating (e.g., anterolateral and posterolateral, or posteromedial and posterolateral) is often necessary to achieve biomechanically stable fixation and restore both coronal and sagittal plane alignment. Studies have shown improved stability with dual plating compared to single plating in bicondylar fractures.
- Bone Grafting: Autogenous or allogenous bone graft or bone substitute is routinely used to fill metaphyseal defects after articular elevation, providing structural support and facilitating bone healing.
-
Outcomes:
- Functional Outcomes: Studies consistently report good to excellent functional outcomes (e.g., using Lysholm score, Knee Society Score, SF-36) in 70-85% of patients treated with ORIF for tibial plateau fractures, including those involving the posterolateral corner, especially with anatomical reduction.
- Complications: The common peroneal nerve remains a significant concern, with reported palsy rates varying but generally decreasing with improved surgical technique and nerve identification protocols. Post-traumatic arthritis is the most prevalent long-term complication, directly correlating with the quality of initial reduction, extent of cartilage damage, and restoration of mechanical axis.
-
Role of Arthroscopy: Arthroscopy can be a valuable adjunct during tibial plateau fracture fixation. It allows for direct visualization of the articular surface to confirm reduction, assess meniscal injuries, and remove loose bodies without additional surgical incisions, thus improving the accuracy of reduction. Its role in posterolateral approaches is primarily for intra-articular assessment.
-
Emerging Concepts: Patient-specific instrumentation and advanced navigation techniques are being explored, though not yet standard, to further improve reduction accuracy and minimize surgical morbidity. The increasing understanding of the distinct biomechanical roles of the individual columns of the tibial plateau has refined indications for specific approaches.
In conclusion, mastering the posterolateral approach to the tibial plateau requires a deep understanding of the surgical anatomy, meticulous pre-operative planning, and precise surgical execution. Adherence to established principles of anatomical reduction and stable internal fixation, coupled with vigilant post-operative management, is critical to optimize patient outcomes and mitigate potential complications.
Clinical & Radiographic Imaging