ANATOMY
Sreeharsha V. Nandyala Alejandro Marquez-Lara Junyoung Ahn
Kern Singh
Superficial landmarks enable gross determination of the anatomic level. Proximally, C7 and T1 are the largest spinous processes and may serve as palpable anatomic landmarks. Distally, the intercrestal line approximates the L4-L5 interspace.
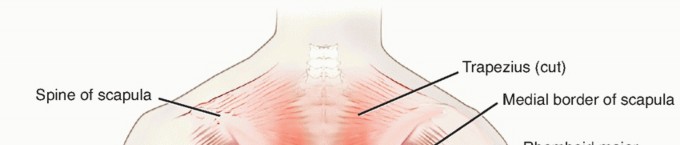
There are three layers to the posterior musculature of the spine (FIG 1; Table 1):
Superficial layer: trapezius, latissimus dorsi, rhomboid major and minor, and the levator scapulae Intermediate layer: superior and inferior serratus posterior and the levatores costarum
Deep layer: erector spinae, transversospinalis, interspinalis, and the intertransversarii
The superficial and intermediate layers receive their nervous supply from peripheral nerves, which are not encountered through the posterior approach (
FIG 2
). The deep layer receives its nervous supply segmentally from the posterior dorsal rami. There is a large amount of redundancy in the innervation of the deep layer.
The midline approach is a true internervous plane. Nerve injury occurs only with excessive lateral dissection.




FIG 1 • The superficial, intermediate, and deep musculature of the back.
The vascular supply to the deep layer is from segmental branches of the aorta. These vessels enter the operative field at the level of the intertransverse ligament and can be a source of significant bleeding.
The facet joint capsules have a shiny white appearance and the individual fibers can be seen inserting onto the lateral edge of the laminar trough. Care should be taken to avoid violating the capsular fibers, unless that segment is being fused.
The ligamentum flavum has a yellow appearance with the fibers running in a cephalocaudal direction. The cephalad end of the ligament has a broad insertion from the base of the spinous process to between 50% and 70% of the anterior surface of the lamina. The caudal end of the ligament inserts from the superior edge of the
lamina to between 2 and 6 mm of the anterior surface of the lamina.4
Particularly at the L5-S1 level, the interspace may be widened or the posterior bony anatomy only partly formed. Care should be exercised when exposing this level as inadvertent plunging into the canal may occur.
Laterally, the intertransverse membrane overlies the iliopsoas and protects the neural structures that lie beneath.
1
Table 1 Musculature of the Back
| Muscle | Origin | Insertion | Innervation | Blood Supply |
|---|---|---|---|---|
| ### Superficial layer | ||||
| Trapezius Medial third of superior nuchal line of occiput, external occipital protuberance, and ligamentum nuchae; spinous processes of C7-T12 | ||||
| Lateral third of clavicle, acromion, spine of scapula | ||||
| Motor supply from spinal accessory nerve, sensory fibers from C3 to C4 | ||||
| Transverse cervical artery | ||||
| Latissimus dorsi Spinous processes | ||||
| of T7—sacrum, medial third of iliac crest, ribs 9-12, inferior angle of scapula | ||||
| Floor of bicipital groove | ||||
| Thoracodorsal nerve (C7, C8) | ||||
| Thoracodorsal artery | ||||
| Levator scapulae | ||||
| Transverse processes of C1-C4 | ||||
| Medial border of scapula | ||||
| Dorsal scapular nerve (C5), with branches of C3-C4 | ||||
| innervating upper part of muscle | ||||
| Dorsal scapular artery | ||||
| Rhomboid major Spinous processes | ||||
| of T2-T5 | ||||
| Medial border of scapula | ||||
| Dorsal scapular nerve (C5) | ||||
| Dorsal scapular artery | ||||
| Rhomboid minor Caudal end of | ||||
| ligamentum nuchae, spinous processes of C7-T1 | ||||
| Medial border of scapula | ||||
| Dorsal scapular nerve (C5) | ||||
| Dorsal scapular artery | ||||
| ### Intermediate layer | ||||
| Serratus posterior superior | ||||
| Spinous processes of C7-T3 | ||||
| Ribs 1-4 Intercostal nerves | ||||
| Posterior intercostals arteries of T1-T4 | ||||
| Serratus posterior inferior | ||||
| Thoracolumbar fascia, spinous processes of T11-L2 | ||||
| Ribs 9-12 Intercostal nerves | ||||
| Posterior intercostal arteries, subcostal artery, and L1-L2 lumbar arteries | ||||
| Levatores costarum | ||||
| Tip of transverse process of C7-T11 vertebrae | ||||
| Rib below level of origin | ||||
| Posterior rami of thoracic spinal nerves | ||||
| Dorsal intercostal arteries | ||||
| ### Deep layer | ||||
| ### Erector spinae (vertically oriented and superficial) | ||||
| Iliocostalis Longissimus Spinalis | ||||
| Iliac crest, sacrum, transverse and spinous processes of vertebrae, and supraspinal ligament | ||||
| Ribs, transverse and spinous processes of vertebrae, posterior aspect of skull | ||||
| Segmental innervation by dorsal primary rami of spinal nerves C1-S5 | ||||
| Segmental supply by deep cervical arteries, posterior intercostal arteries, subcostal artery, and lumbar arteries | ||||
| ### Transversospinalis (obliquely oriented and intermediate) | ||||
| Semispinalis Transverse processes T1-T12 | ||||
| Spinous processes of C2-T5 | ||||
| Dorsal rami of spinal nerves | ||||
| Segmental arteries from aorta | ||||
| Multifidus Articular processes of cervical vertebrae, transverse processes of thoracic vertebrae, mammillary processes of lumbar vertebrae, posterior superior iliac spine | ||||
| Spinous processes of C2-L5 | ||||
| Dorsal rami of spinal nerves | ||||
| Segmental branches from aorta | ||||
| Rotatores Transverse processes | ||||
| Base of spinous processes above Long skip one | ||||
| Dorsal rami of spinal nerves | ||||
| Segmental branches from aorta | ||||
| level; short attach | ||||
| at level above | ||||
| ### Deepest muscle | ||||
| Interspinales | ||||
| Spinous processes | ||||
| Spinous | ||||
| processes one level above | ||||
| Dorsal rami of | ||||
| spinal nerves | ||||
| Segmental | ||||
| branches from aorta | ||||
| Intertransversarii Anterior and | ||||
| posterior transverse processes of cervical vertebrae, transverse and mammillary processes of lumbar vertebrae | ||||
| Anterior and | ||||
| posterior processes of cervical vertebrae one level above, transverse and accessory processes of lumber vertebrae one level above | ||||
| Dorsal rami of | ||||
| spinal nerves | ||||
| Segmental | ||||
| branches from aorta | ||||
| 2 | ||||

|
||||

|
||||

|
||||

|
||||

|
||||
| ### FIG 2 • Cross-sectional anatomy of the thoracic and lumbar spine. | ||||
| In children, the spinous process apophysis has not fused. During dissection, the apophysis is split down to the bone and then elevated with the paraspinal musculature. | ||||
| ## SURGICAL MANAGEMENT | ||||
| ## Positioning | ||||
| Patients should be placed in the prone position on a radiolucent table ( FIG 3A ). Care is taken to ensure that the neck is in a neutral position with no hyperextension. | ||||
| The arms are positioned at 90 degrees or less of abduction to minimize the likelihood of rotator cuff impingement. The arms are allowed to slightly hang down in a forward-flexed position about 10 degrees. The axilla should be clear from any padding to prevent brachial plexus palsy. | ||||
| Elbow pads are placed along the medial epicondyle to protect the ulnar nerve. | ||||
| Pads are placed at the chest and iliac crests. | ||||
| The chest pad is placed just proximal to the level of the xiphoid process and distal to the axilla. In women, care is taken to tuck the breasts and ensure that the nipples are pressure-free. | ||||
| The iliac pads are placed two fingerbreadths distal to the anterior superior iliac spine, allowing the abdomen to hang freely and reducing any unnecessary epidural bleeding. | ||||
| Proper placement of the chest and iliac pads allows for restoration of normal sagittal alignment via gravity. | ||||
| Alternatively, for lumbar decompressive procedures alone, the knees are positioned in a sling, thereby allowing the hips to flex and eliminating lumbar lordosis and widening the laminar interspaces ( FIG 3B ). This position improves access | ||||
| 3 | ||||
| to the lumbar spinal canal but should be avoided when instrumenting as lumbar lordosis is decreased. | ||||

|
||||
| ### FIG 3 • A. Prone position on a radiolucent table. The abdomen is not compressed. B. The knee-chest position is obtained using a Wilson frame. | ||||
| ## Approach | ||||
| Two approaches are used: midline and paraspinal. | ||||
| The midline approach is used for most spinal procedures as it allows direct access to the spinal canal. | ||||
| The paraspinal approach, also known as the Wiltse approach, was initially described for spondylolisthesis but is now used for far lateral discectomies and minimally invasive muscle-sparing techniques. | ||||
| There is increased interest in the paraspinal approach, particularly in conjunction with transforaminal lumbar interbody fusion procedures. | ||||
| ## TECHNIQUES | ||||
| 1. ## Midline Posterior Approach | ||||
| ### Incision and Dissection | ||||
| Anatomic landmarks are identified to center the skin incision appropriately ( TECH FIG 1A ). A midline incision is made over the spinous processes down to the level of the fascia. | ||||
| A Cobb elevator is used to create 2-mm full-thickness skin flaps with subcutaneous fat. This allows for better visualization of the fascia during closure ( TECH FIG 1B,C ). | ||||

|
||||

|
||||
| ### TECH FIG 1 • A. Anatomic landmarks. B,C. The fascia is exposed with full-thickness skin flaps. | ||||
| The location of the spinous processes is again verified, and electrocautery is used to reflect the fascia from the tips of the spinous processes. | ||||
| Electrocautery is used to subperiosteally elevate the paraspinal musculature laterally to the trough of the lamina. The surgeon should avoid going beyond this point to protect the insertion of the facet joint capsule. | ||||
| A sponge and Cobb are then used to gently dissect the paraspinal musculature off the facet joint capsule. | ||||
| 4 | ||||

|
||||

|
||||
 TECH FIG 2
•
A.
Venous bleeding sites are adjacent to the pars interarticularis and at the junction of the facet and the transverse process.
B,C.
Probes (arrows) indicate the location of venous bleeders adjacent to the pars interarticularis (
B,C
) and the facet joint (
D
).
TECH FIG 2
•
A.
Venous bleeding sites are adjacent to the pars interarticularis and at the junction of the facet and the transverse process.
B,C.
Probes (arrows) indicate the location of venous bleeders adjacent to the pars interarticularis (
B,C
) and the facet joint (
D
).
|
||||
| ### Cautery | ||||
| Two venous bleeders are encountered that require electrocautery ( TECH FIG 2A ). | ||||
| The first is located adjacent to the pars interarticularis ( TECH FIG 2B,C ). The second is located just lateral to the facet joint ( TECH FIG 2D ). | ||||
| Electrocautery is used to elevate the paraspinal musculature off the transverse processes. Care should be taken to stay on the transverse process and not to violate the intertransverse membrane. | ||||
| Bipolar cautery should be used at the intertransverse ligament to avoid damage to the spinal nerves. | ||||

|
||||

|
||||
| ### TECH FIG 3 • A,B. Electrocautery is used to excavate a muscular pocket for the fusion mass. (continued) | ||||
| ### Paraspinal Resection | ||||
| In large and muscular patients, it is often necessary to excise a portion of the paraspinal muscles overlying the transverse processes to be fused. | ||||
| The muscle is resected beginning underneath the fascia and extending toward the lateral edge of the transverse processes. This creates a pocket over the transverse processes that serve as a bone graft cavity ( TECH FIG 3 ). | ||||
| 5 | ||||

|
||||

|
||||
| ### TECH FIG 3 • (continued) C,D. Complete posterior exposure. | ||||
| ## Paraspinal Approach | ||||
| The approach is typically performed two fingerbreadths lateral to the spinous process. | ||||
| After the fascia has been exposed, the paraspinal muscles are palpated, and the interval between the multifidus medially and longissimus laterally is identified. | ||||
| A sharp incision through the fascia is made at this interval ( TECH FIG 4 ). | ||||
| The interval is defined with blunt dissection down to the lateral edge of the facet joint and transverse | ||||
| process junction. | ||||
| ### TECH FIG 4 • Cross-section of spine showing Wiltse interval. | ||||

|
||||

|
||||
| PEARLS AND PITFALLS | ||||
| --- | ||||
| Pars ▪ Lateral to the pars; can be prophylactically identified and cauterized interarticularis | ||||
| bleeder | ||||
| Lateral facet ▪ A ball-tipped probe can be placed along the undersurface of the lateral edge of bleeder the superior articular process where the facet bleeder originates. Electrocautery | ||||
| can then be used to coagulate this vessel, which hinders intertransverse exposures. | ||||
| Facet capsule ▪ A sponge can be placed over the facet. Muscle stripping is then performed with preservation a Cobb elevator as the sponge protects the capsular fibers from being disrupted | ||||
| and accidentally incised. | ||||
| Widened ▪ An anteroposterior radiograph should be evaluated preoperatively to assess for lower lumbar spina bifida occulta and widened interlaminar windows. Extra caution should be interspace employed when working in these areas to avoid inadvertent injury to the thecal | ||||
| sac. | ||||
| 6 | ||||
| ## Table 2 Complications Associated with the Posterior Approach | ||||
| Complications | Occurrence | |||
| --- | --- | |||
| Major | Wound infection | 1%-10% | ||
| Pneumonia | 5% | |||
| Renal failure | 5% | |||
| Myocardial infarction | 3% | |||
| Respiratory distress | 2% | |||
| Neurologic deficit | 2% | |||
| Congestive heart failure | 2% | |||
| Cerebrovascular accident | 1% | |||
| Minor | Urinary tract infections | 34% | ||
| Anemia requiring transfusion | 27% | |||
| Confusion | 27% | |||
| Ileus | 22% | |||
| Arrhythmia | 7% | |||
| Transient hypoxia | 7% | |||
| Wound seroma | 5% | |||
| Leg dysesthesia | 2% | |||
| From Carreon LY, Puno RM, Dimar JR II, et al. Perioperative complications of posterior lumbar | ||||
| decompression and arthrodesis older in adults. J Bone Joint Surg Am 2003;85-A(11):2089-2092; Olsen MA, Mayfield J, Lauryssen C, et al. Risk factors for surgical site infection in spinal surgery. J Neurosurg 2003;98(2 suppl):149-155. | ||||
| ## COMPLICATIONS | ||||
| Major and minor complication rates of up to 80% have been reported in some series (Table 2).2 Risk factors for complications include patient age, length of surgery, levels exposed, blood loss, and | ||||
| postoperative urinary incontinence. Diabetes and other medical comorbidities have not been shown to be | ||||
| independent risk factors for the development of postoperative complications.1,2,3 | ||||
| ## |
Scientific References
- 1. Benz RJ, Ibrahim ZG, Afshar P, et al. Predicting complications in elderly patients undergoing lumbar decompression. Clin Orthop Relat Res 2001;(384):116-121. [View Source / PubMed]
- 2. Carreon LY, Puno RM, Dimar JR II, et al. Perioperative complications of posterior lumbar decompression and arthrodesis older in adults. J Bone Joint Surg Am 2003;85-A(11):2089-2092. [View Source / PubMed]
- 3. Olsen MA, Mayfield J, Lauryssen C, et al. Risk factors for surgical site infection in spinal surgery. J Neurosurg 2003;98(2 suppl): 149-155. [View Source / PubMed]
- 4. Olszewski AD, Yaszemski MJ, White AA III, et al. The anatomy of the human lumbar ligamentum flavum: new observations and their surgical importance. Spine 1996;21(20):2307-2312. [View Source / PubMed]
