POSTERIOR INSTABILITY OF THE SHOULDER
Posterior shoulder dislocations and recurrent posterior instability represent a complex and often misdiagnosed subset of glenohumeral pathology, accounting for only 2% to 4% of all shoulder dislocations. Due to its relative rarity and subtle clinical presentation, posterior instability demands a high index of suspicion, meticulous clinical evaluation, and a nuanced understanding of glenohumeral biomechanics.
The etiology of posterior instability is broadly categorized into macrotraumatic events, repetitive microtrauma, and atraumatic (often voluntary) conditions. Traumatic events resulting in acute posterior dislocation are classically associated with violent, uncoordinated muscle contractions—most notably seen during epileptic seizures, electrical shock, and severe intoxication. In these scenarios, the powerful internal rotators (subscapularis, pectoralis major, latissimus dorsi) overpower the weaker external rotators (infraspinatus, teres minor), driving the humeral head posteriorly. Additionally, posterior dislocation can be precipitated by a direct, high-energy blow to the anterior shoulder or by an axial load applied to a forward-flexed, adducted, and internally rotated extremity (e.g., a fall on an outstretched arm or a dashboard injury during a motor vehicle collision).
Pathoanatomy and the Role of Microtrauma
Recurrent posterior subluxation—whether atraumatic or acquired secondary to repetitive microtrauma—is significantly more common than recurrent instability following a discrete traumatic posterior dislocation. The posterior capsulolabral complex, specifically the posterior band of the inferior glenohumeral ligament (IGHL), is the primary static restraint to posterior translation when the arm is flexed and internally rotated.
Repetitive overuse and microtraumatic injuries progressively attenuate this posterior capsule. This is highly prevalent in sports requiring repetitive overhead motion or heavy axial loading. High-risk activities include:
* Overhead Sports: Pitching, tennis, and swimming (particularly the backstroke and breaststroke).
* Weightlifting: The bench press places immense posteriorly directed shear forces on the glenohumeral joint, especially at the bottom of the lift when the humerus is extended past the coronal plane.
* Contact Sports: Offensive linemen in American football frequently experience posterior capsular microtrauma due to repetitive blocking maneuvers with the arms forward-flexed and internally rotated.
Andrews and Phillips have extensively described recurrent posterior instability of the dominant shoulder in baseball batters. This pathology most commonly manifests during a "check swing" or when attempting to pull an outside pitch. These actions disrupt normal synchronous swing mechanics, generating massive, unattenuated posteriorly directed shear forces across the glenohumeral joint, leading to progressive capsular failure.
Clinical Evaluation and Classification
Posterior instability patterns must be evaluated with rigorous precision and categorized as unidirectional, bidirectional, or multidirectional. The exact direction of dislocations and symptomatic subluxations must be determined to guide both conservative and surgical management.
Clinical Pearl: The "Jerk Test" and the "Kim Test" are highly sensitive and specific physical examination maneuvers for diagnosing posterior labral tears and posterior capsular incompetence. A positive test elicits a sudden clunk or sharp pain as the subluxated humeral head reduces into the glenoid fossa.
Voluntary Subluxation vs. Psychological Overlay
Many patients with instability of microtraumatic or atraumatic origin learn to sublux their shoulder voluntarily through horizontal adduction and internal rotation. It is critical to understand that voluntary subluxation does not inherently imply a psychological overlay. Many athletes utilize this maneuver simply to demonstrate their pathology to the examining physician.
However, careful psychological assessment is paramount. A patient who presents with a bland, detached affect and who is capable of subluxating the shoulder posteriorly using isolated muscular contraction alone is highly likely to have an underlying psychological overlay or a secondary gain motive. With the shoulder in the abducted position, these patients selectively fire their internal rotators to drive the humeral head out the back of the joint.
🚨 Surgical Warning: Patients demonstrating voluntary posterior subluxation driven by psychological overlay or secondary gain should rarely, if ever, be treated surgically. Operative intervention in this cohort carries an unacceptably high failure rate and often exacerbates the underlying dysfunction.
The Influence of Glenoid Version
Historically, excessive glenoid retroversion has been heavily implicated in the pathogenesis of posterior instability. However, contemporary evidence-based consensus suggests that glenoid version contributes significantly to posterior instability only in patients with severe congenital glenoid dysplasia or traumatic disruption of the posterior bony architecture (e.g., a reverse bony Bankart lesion).
Fuchs, Jost, and Gerber previously stated that a corrective glenoid osteotomy is indicated when more than 10 degrees of retroversion is present.
FIGURE 47-38: Measurement of version of chondrolabral and osseous portions of the glenoid. a, reference line representing plane of chondrolabral portion of glenoid; b, reference line representing plane of scapular body; c, reference line representing plane of osseous portion of glenoid. Angle between a and b′ (perpendicular to b) represents version of chondrolabral portion of glenoid. Angle between c and b′ represents version of osseous portion of glenoid (Kim et al.).
Despite these historical indications, glenoid osteotomies have largely fallen out of favor in modern practice. The procedure is technically demanding and carries unacceptably high complication rates, including coracoid impingement, iatrogenic osteoarthritis, hardware failure, and avascular necrosis of the glenoid fragment. Today, soft tissue stabilization and bone-grafting techniques (e.g., posterior bone block) are preferred for managing critical bone loss.
CONSERVATIVE TREATMENT
The initial management of posterior shoulder instability must always be nonoperative. Most patients, particularly those with generalized ligamentous laxity or instability secondary to repetitive microtrauma, respond favorably to an aggressive, well-structured physical therapy program.
The conservative regimen includes:
1. Activity Modification: Educating the patient to avoid provocative activities and specific voluntary maneuvers that precipitate posterior subluxation.
2. Targeted Strengthening: A rigorous exercise program aimed at hypertrophy and neuromuscular control of the external rotators (infraspinatus, teres minor) and the posterior deltoid. These muscles act as dynamic buttresses against posterior humeral translation.
3. Scapular Stabilization: Strengthening the periscapular musculature (rhomboids, trapezius, serratus anterior) to correct scapular dyskinesia, ensuring the glenoid provides a stable platform during dynamic upper extremity movements.
4. Restoration of Motion: Normal, pain-free range of motion must be obtained before considering return to play.
In overhead athletes, observation and biomechanical instruction by a knowledgeable coach or sports biomechanist can correct the kinematic flaws responsible for the repetitive microtrauma.
SURGICAL MANAGEMENT: INDICATIONS AND DECISION MAKING
Surgical intervention is indicated only after a dedicated 3- to 6-month trial of conservative management has failed, and the patient continues to experience symptomatic, involuntary posterior subluxation or dislocation that limits activities of daily living or athletic participation.
The choice of surgical technique depends heavily on the patient's functional demands and the underlying pathoanatomy:
* Capsular Shift (Tibone or Neer and Foster): We prefer these techniques for atraumatic multidirectional instability in non-throwing athletes.
* Muscle-Splitting Technique with Medial Shift (Tibone et al.): This is our preferred approach for overhead athletes with recurrent posterior subluxation, as it minimizes disruption to the dynamic stabilizers.
* Hawkins and Janda Technique: Best reserved for heavy laborers or athletes involved in collision sports (e.g., American football, ice hockey) who present with recurrent posterior subluxation secondary to profound capsular deficiency.
We have observed good to excellent long-term results with open posterior capsulorrhaphy, and it remains a highly reliable technique for addressing severe capsular redundancy. The procedure involves advancing the inferior capsule superiorly and advancing the divided infraspinatus inferiorly (or overlapping it) to obliterate the posterior axillary pouch and provide a robust posterior buttress.
🔪 Surgical Technique 47-12: Open Posterior Capsulorrhaphy (Neer and Foster)
The Neer and Foster technique is a classic, highly effective open procedure designed to address posterior capsular redundancy and posterior labral pathology.
Patient Positioning and Anesthesia
- Following the induction of general anesthesia (often supplemented with an interscalene nerve block), place the patient on the operating table in the lateral decubitus position with the involved shoulder facing upward.
- Secure the patient rigidly using a vacuum beanbag and a kidney rest. Ensure all bony prominences (e.g., the contralateral fibular head and greater trochanter) are meticulously padded to prevent neurapraxia.
- The operative arm is prepped and draped free, allowing for full intraoperative manipulation. The arm is typically suspended using a sterile traction setup at approximately 30 to 45 degrees of abduction and 15 to 20 degrees of forward flexion.
Surgical Approach
- Incision: Make a 10-cm vertical "saber cut" skin incision beginning just posterior to the acromioclavicular joint and extending distally toward the posterior axillary fold, passing over the posterior aspect of the acromion and the spine of the scapula.
FIGURE 47-39A: Saber cut skin incision just posterior to the acromioclavicular joint toward the posterior axillary fold.
- Superficial Dissection: Undermine the subcutaneous tissue to expose the underlying deltoid muscle fascia.
- Deltoid Split: Split the deltoid muscle in line with its fibers, beginning 2 to 3 cm medial to the posterolateral corner of the acromion. Extend the split distally for no more than 4 to 5 cm to avoid iatrogenic injury to the axillary nerve, which courses transversely across the deep surface of the deltoid approximately 5 to 7 cm distal to the acromial edge.
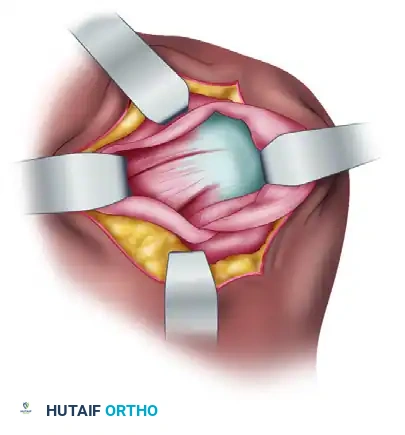
FIGURE 47-39B: Deltoid muscle is split in line with fibers beginning 2 to 3 cm medial to the posterolateral corner of the acromion.
- Deep Exposure: Retract the split deltoid medially and laterally using self-retaining retractors (e.g., Charnley or Gelpi retractors). This exposes the underlying deep fascia covering the infraspinatus and teres minor muscles.
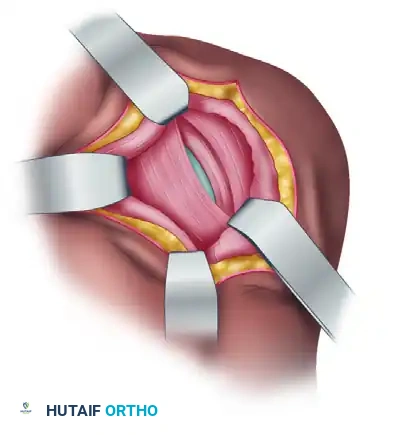
FIGURE 47-39C: Exposure of underlying infraspinatus and teres minor muscles.
Capsular Shift and Repair
- Identify the internervous plane between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve).
- Carefully elevate the infraspinatus off the underlying posterior joint capsule. In the Neer and Foster technique, the infraspinatus tendon is often divided obliquely.
- Perform a T-shaped capsulotomy. The vertical limb of the "T" is placed adjacent to the glenoid rim, and the horizontal limb splits the capsule longitudinally.
- Inspect the joint for intra-articular pathology, including posterior labral tears (reverse Bankart lesions) or chondral defects. If a labral tear is present, repair it to the decorticated glenoid rim using suture anchors.
- The Shift: To obliterate the redundant axillary pouch, advance the inferior capsular flap superiorly and medially, suturing it to the intact superior capsular cuff and the glenoid rim. Subsequently, bring the superior capsular flap inferiorly over the advanced inferior flap, creating a robust, double-layered capsular repair ("pants-over-vest" technique).
- Infraspinatus Imbrication: The previously divided infraspinatus is then repaired. It is advanced inferiorly and overlapped (shortened) to add a dynamic, muscular buttress to the posterior capsule, further reinforcing the repair against posterior translation.
- Closure: Thoroughly irrigate the wound. Allow the deltoid split to fall together; it requires only minimal, loose approximation with absorbable sutures. Close the subcutaneous tissue and skin in a standard layered fashion.
POSTOPERATIVE PROTOCOL
The success of a posterior capsulorrhaphy relies as much on strict postoperative rehabilitation as it does on surgical execution. The repaired posterior tissues must be protected from premature stretching.
- Phase I (0 to 4-6 Weeks): The patient is immobilized in a specialized orthosis (e.g., a "gunslinger" brace or an external rotation brace) that holds the shoulder in 10 to 20 degrees of external rotation and slight abduction. This position removes all tension from the posterior capsular repair. Active hand, wrist, and elbow motion is encouraged. Internal rotation, forward flexion, and cross-body adduction are strictly prohibited.
- Phase II (6 to 10 Weeks): The brace is discontinued. Active-assisted range of motion (AAROM) begins, gradually progressing to active range of motion (AROM). Stretching into internal rotation is introduced very cautiously.
- Phase III (10 to 16 Weeks): Isotonic strengthening of the rotator cuff and periscapular stabilizers is initiated. Emphasis is placed on the external rotators and posterior deltoid.
- Phase IV (4 to 6 Months): Progression to sport-specific or work-specific functional activities. Return to contact sports or heavy overhead lifting is generally not permitted until 6 months postoperatively, contingent upon the restoration of symmetric strength and dynamic stability.
Clinical Pearl: Postoperative stiffness, particularly a mild loss of internal rotation, is common and often desirable following posterior stabilization. Aggressive early stretching into internal rotation is the most common cause of surgical failure and recurrent instability.
📚 Medical References
- posterior shoulder instability: an anatomic reappraisal, Clin Orthop Relat Res 216:70, 1987.
- Gerber C, Terrier F, Ganz R: The Trillat procedure for recurrent anterior instability of the shoulder, J Bone Joint Surg 70B:130, 1988.
- Gill TJ, Micheli LJ, Gebhard F, et al: Bankart repair for anterior instability of the shoulder, J Bone Joint Surg 79A:850, 1997.
- Glousman R, Jobe F, Tibone J, et al: Dynamic electromyographic analysis of the throwing shoulder with glenohumeral instability, J Bone Joint Surg 70A:220, 1988.
- Goss TP: Anterior glenohumeral instability, Orthopedics 11:87, 1988.
- Goss TP, Costello G: Recurrent symptomatic posterior glenohumeral subluxation, Orthop Rev 17:1024, 1988.
- Griegshauser L: Recurrent anterior shoulder subluxation, Orthopedics 7:122, 1984.
- Harryman D, Sidles J, Matsen F: The role of the rotator interval capsule in passive motion and stability of the shoulder, J Bone Joint Surg 74A:53, 1992.
- Hastings DE, Coughlin LP: Recurrent subluxation of the glenohumeral joint, Am J Sports Med 9:352, 1981.
- Hawkins RJ, Janda DH: Posterior instability of the glenohumeral joint: a technique of repair, Am J Sports Med 24:275, 1996.
- Hawkins RJ, Koppert G, Johnston G: Recurrent posterior instability (subluxation) of the shoulder, J Bone Joint Surg 66A:169, 1984.
- Hawkins RJ, McCormack RG: Posterior shoulder instability, Orthopedics 11:101, 1988.
- Helfet AJ: Coracoid transplantation for recurring dislocation of the shoulder, J Bone Joint Surg 40B:198, 1958.
- Henry JH, Genung JA: Natural history of glenohumeral dislocation—revisited, Am J Sports Med 10:135, 1982.
- Hill HA, Sachs MD: The grooved defect of the humeral head: a frequently unrecognized complication of dislocations of the shoulder joint, Radiology 35:690, 1940.
- Hill JA, Lombardo SJ, Kerlan RK, et al: The modifi ed BristowHelfet procedure for recurrent anterior shoulder subluxations and dislocations, Am J Sports Med 9:283, 1981.
- Hill JA, Tkach L, Hendrix, RW: A study of glenohumeral orientation in patients with anterior recurrent shoulder dislocations using computerized axial tomography, Orthop Rev 18:84, 1989.
- Hodgkinson JP, Case DB: The modifi ed staple capsulorrhaphy for the correction of recurrent anterior dislocation of the shoulder, Injury 18:51, 1987.
- Hovelius L: Anterior dislocation of the shoulder in teen-agers and young adults, J Bone Joint Surg 69A:393, 1987.
- Hovelius L, Eriksson K, Fredin H, et al: Recurrences after initial dislocation of the shoulder: results of a prospective study of treatment, J Bone Joint Surg 65A:343, 1983.
- Hovelius L, Körner L, Lundberg B, et al: The coracoid transfer for recurrent dislocation of the shoulder: technical aspects of the Bristow-Laterjet procedure, J Bone Joint Surg 65A:926, 1983.
- Howell SM, Galinat BJ, Renzi AJ, et al: Normal and abnormal mechanics of the glenohumeral joint in the horizontal plane, J Bone Joint Surg 70A:227, 1988.
- Hybbinette S: De la transposition d’un fragment osseux pour rémé dier aux luxations récidivantes l’épaule: constatations et résultats opératoires, Acta Orthop Scand 71:411, 1932.
- Iannotti JP, Antoniou J, Williams GR, et al: Iliotibial band reconstruction for treatment of glenohumeral instability associated with irreparable capsular defi ciency, J Shoulder Elbow Surg 11:618, 2002.
- Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: a preliminary study, J Shoulder Elbow Surg 12:413, 2003.
- Itoi E, Lee S-B, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: a cadaver study, J Bone Joint Surg 82A:35, 2000.
- Jobe FW, Giangarra CE, Kvitne RS, et al: Anterior capsulolabral reconstruction of the shoulder in athletes in overhand sports, Am J Sports Med 19:428, 1991.
- Jobe FW, Glousman RE: Anterior capsulolabral reconstruction, Tech Orthop 3:29, 1989.
- Jobe FW, Kvitne RS: Shoulder pain and the overhand or throwing athlete: the relationship of anterior instability and rotator cuff impingement, Orthop Rev 18:963, 1989.
- Jobe FW, Kvitne RS: Personal communication, 1991.
- Jost B, Gerber C: Pectoralis major transfer for subscapularis insuffi ciency, Tech Shoulder Elbow Surg 5:157, 2004.
- Karadimas J, Rentis G, Varouchas G: Repair of recurrent anterior dislocation of the shoulder using transfer of the subscapularis tendon, J Bone Joint Surg 62A:1147, 1980.
- Kim SH, Ha KI, Cho YB, et al: Arthroscopic anterior stabilization of the shoulder: two to six-year follow-up, J Bone Joint Surg 85A:1511, 2003.
- Kim SH, Ha KI, Kim SH: Bankart repair in traumatic
