INTRODUCTION TO COMPLEX KNEE PATHOLOGIES
The management of complex knee pathologies requires a profound understanding of both soft-tissue biomechanics and high-energy trauma protocols. This masterclass delineates two distinct but equally critical domains in operative orthopaedics: the surgical correction of severe flexion contractures via the Posterior Capsulotomy (Yount Technique), and the evidence-based management of Open Wounds of the Knee Joint, with a specific focus on the rising incidence of civilian gunshot injuries.
For the practicing orthopedic surgeon, mastering these techniques ensures the restoration of joint kinematics in chronic deformities and the preservation of limb viability in acute, high-energy trauma.
PART I: POSTERIOR CAPSULOTOMY (THE YOUNT TECHNIQUE)
Biomechanics and Indications
Severe flexion contractures of the knee often result from a combination of capsular fibrosis, muscular shortening, and fascial tethering. Conditions such as poliomyelitis, cerebral palsy, prolonged immobilization, or severe intraarticular trauma can lead to adaptive shortening of the posterior structures.
The iliotibial (IT) band and the lateral intermuscular septum are primary deforming forces in lateral and flexion contractures. The Yount Procedure is specifically designed to address these lateral tethering structures. By excising a significant segment of the IT band and the intermuscular septum, the surgeon eliminates the bowstringing effect that perpetuates the contracture, allowing for subsequent extension of the joint.
Surgical Pearl: The Yount procedure is rarely performed in isolation for severe contractures (>30 degrees). It is frequently combined with hamstring lengthening and, if necessary, a formal posterior capsular release from the posterior aspect of the distal femur.
Preoperative Planning and Positioning
- Patient Positioning: The patient is placed in the supine position. A sandbag or bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the thigh and knee into clear view.
- Tourniquet: A proximal thigh tourniquet is applied and inflated after exsanguination to ensure a bloodless surgical field.
- Neurovascular Assessment: Document preoperative common peroneal nerve function, as correction of a severe flexion contracture places this nerve at high risk for traction neurapraxia.
Surgical Technique: Step-by-Step
1. Surgical Approach
Make a lateral longitudinal incision starting just proximal to the lateral femoral condyle and extending proximally along the line of the iliotibial band for approximately 10 to 12 cm. Dissect through the subcutaneous tissues to expose the glistening fibers of the fascia lata and the iliotibial band.
2. Division of the Fascia Lata
Identify the posterior and anterior borders of the iliotibial band.
* Posteriorly: Divide the iliotibial band and fascia lata back to the anterior margin of the biceps femoris tendon.
* Anteriorly: Continue the transverse division anteriorly to the midline of the thigh.
* Level of Resection: This transverse cut must be made at a precise level: 2.5 cm proximal to the superior pole of the patella.
Surgical Warning: When dissecting posteriorly near the biceps femoris tendon, maintain meticulous hemostasis and spatial awareness. The common peroneal nerve lies immediately posterior and medial to the biceps tendon. Avoid blind plunging with scissors or electrocautery in this quadrant.
3. Excision of the Iliotibial Segment
To prevent the recurrence of the contracture through bridging scar tissue, a simple release is insufficient.
* From the initial transverse cut, dissect proximally.
* Excise a robust segment of the iliotibial band and the underlying lateral intermuscular septum measuring 5 to 8 cm in length.
* Ensure the intermuscular septum is excised down to its attachment on the linea aspera of the femur.
4. Intraoperative Assessment and Closure
Before proceeding to closure, the surgeon must manually extend the knee and determine by palpation that all tight lateral and posterolateral bands have been divided. If the knee still resists extension, evaluate the posterior capsule and the hamstring tendons for secondary contractures.
* Closure: Suture only the subcutaneous tissue and the skin. Do not attempt to close the deep fascia, as this will immediately recreate the tethering effect you just surgically abolished.
Postoperative Care and Rehabilitation
The postoperative protocol is as critical as the surgical execution.
* Immobilization: Immediately postoperatively, the limb is fitted with a hinged knee brace locked in maximum achievable extension.
* Mobilization: Range-of-motion (ROM) exercises are initiated as soon as wound healing permits. The use of a Continuous Passive Motion (CPM) machine is highly beneficial in preventing intraarticular adhesions and maintaining the newly acquired extension.
* Monitoring: The patient must be examined frequently in the outpatient clinic to detect any recurrent flexion contracture.
* Serial Casting: If extension begins to regress, implement a protocol of serial extension casting or dynamic extension splinting to regain and hold the correction.
PART II: OPEN WOUNDS OF THE KNEE JOINT
While the management of war-related open joint injuries has been extensively documented in military literature, civilian trauma centers are increasingly burdened with high-energy open joint wounds, predominantly due to the rise in civilian gunshot injuries.
Of all open joint injuries, those involving the knee are by far the most common, accounting for 53% to 91% of cases. The superficial nature of the knee joint makes it highly susceptible to penetration, contamination, and subsequent septic arthritis if not managed with aggressive, evidence-based protocols.
Initial Assessment and the Treatment Algorithm
In any patient presenting with a gunshot wound (GSW) to the knee, the evaluation of neurovascular status supersedes all other orthopedic assessments. The kinetic energy of a projectile can cause severe intimal tearing or transection of the popliteal artery, even without direct physical contact (due to the temporary cavitation effect).
The Evidence-Based Algorithm (Bartlett et al.)
The management of these injuries dictates a systematic approach based on the energy of the weapon, the degree of contamination, and the presence of vascular compromise.
- High-Energy vs. Low-Energy: Determine if the wound is from a high-velocity rifle/close-range shotgun (high-energy) or a standard civilian handgun (low-energy).
- Vascular Assessment:
- Are there hard signs of vascular injury (pulsatile bleeding, expanding hematoma, absent distal pulses)? If Yes $\rightarrow$ Immediate surgical exploration.
- Are there soft signs or is the injury proximate to the neurovascular bundle? If Yes $\rightarrow$ Perform Duplex Doppler or CT Angiography.
- Joint Penetration: If intraarticular fractures are not radiographically evident, a saline load test or knee joint aspiration is mandatory. A bloody aspirate with fat globules (lipohaemarthrosis) strongly indicates joint penetration and necessitates formal joint irrigation.
Radiographic Evaluation
Anteroposterior (AP) and lateral radiographs must be carefully scrutinized for fracture patterns, intraarticular air (pneumarthrosis), bullet fragments, and osteochondral shear injuries. Computed Tomography (CT) is invaluable for preoperative planning, providing 3D spatial information regarding the extent and complexity of the fracture pattern.

FIGURE 1: Anteroposterior view of the right distal femur of an 18-year-old woman with a high-velocity rifle wound. Note the classic “lead snowstorm” pattern and severe comminution indicative of massive kinetic energy transfer. Arteriogram revealed no gross arterial damage.
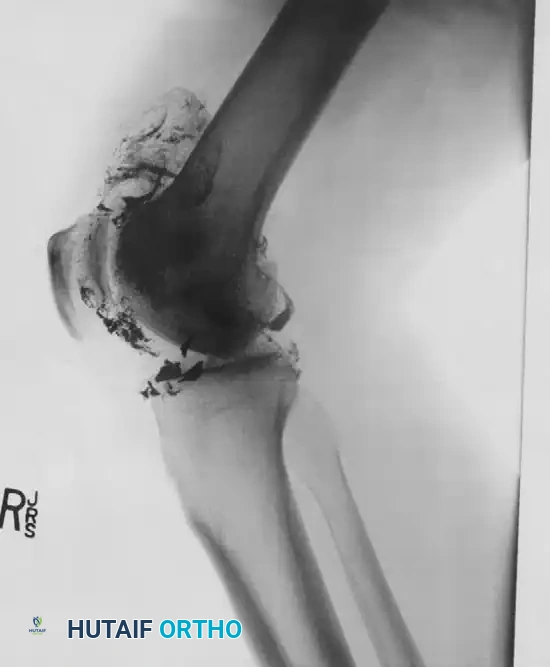
FIGURE 2: Lateral radiograph demonstrating severe intraarticular comminution of the femoral condyles with retained metallic fragments tracking through the posterior joint space.

FIGURE 3: AP radiograph showing a trans-articular trajectory with significant osteochondral defects and retained ballistic debris within the joint capsule.
Surgical Management Principles
The Patzakis Protocol
Patzakis et al. conducted a landmark review of 140 patients with penetrating joint injuries, dividing them into three cohorts: open joint injuries with fractures, open joint injuries without fractures, and gunshot wounds. Their protocol yielded remarkably good results, with an infection rate of only 2.1% (3 out of 140 patients).
Their core tenets include:
1. Broad-Spectrum Antibiotics: Administer IV antibiotics (e.g., Cefazolin 1g IV q8h) before, during, and for 48–72 hours after surgery. For severe contamination, protocols may extend to include Gram-negative coverage (e.g., Ciprofloxacin).
2. Surgical Débridement and Irrigation: Copious irrigation (minimum 9 liters of normal saline) and meticulous excision of all necrotic tissue.
3. Primary Closure: The joint capsule should be closed primarily if soft tissue allows, but the superficial wound tracks are left open to heal by secondary intention.
Critical Pitfall: The Danger of Closed Suction Irrigation
In the Patzakis study, polyethylene tubes were initially installed for closed irrigation and suction. However, several patients developed positive cultures from these drainage tubes postoperatively, despite having negative cultures at the time of the initial surgery. The authors concluded that closed irrigation and suction systems act as a conduit for nosocomial contamination. Therefore, routine use of closed suction drains in open joint injuries is strictly contraindicated unless severe, established purulence dictates otherwise.
Arthroscopy vs. Arthrotomy
- Low-Energy / No Fracture: If open fracture reduction is not required, irrigation and débridement can be performed arthroscopically. Arthroscopy offers superior visualization of osteochondral fragments, results in a shorter hospital stay, causes less postoperative pain, and minimizes further soft-tissue morbidity.
- High-Energy / Severe Comminution: Requires formal arthrotomy. Fracture management depends on stability and may necessitate external fixation (spanning the knee), intramedullary nailing, or, rarely in the acute contaminated setting, open reduction and internal fixation (ORIF).
Large osteochondral fragments should be preserved, reattached, and fixed using arthroscopic or open techniques (e.g., headless compression screws or bioabsorbable pins). Damaged ligamentous structures (ACL, PCL, collateral ligaments) are generally not reconstructed in the acute, contaminated setting; they are addressed in a staged, delayed fashion once the soft-tissue envelope is pristine.
PART III: LATE COMPLICATIONS - INTRAARTICULAR LEAD TOXICITY
A rare but highly morbid late complication of intraarticular gunshot injuries is lead poisoning (Plumbism). While lead fragments embedded in muscle or subcutaneous tissue generally become encapsulated by fibrous tissue and remain biologically inert, the intraarticular environment is vastly different.
Pathophysiology of Synovial Lead Absorption
When bullet fragments are in direct contact with synovial fluid, the fluid acts as a solvent. The slightly acidic nature of synovial fluid, combined with the mechanical grinding of the joint during articulation, dissolves the lead. This leads to:
1. Severe foreign-body reactions.
2. Mechanical third-body wear of the articular cartilage.
3. Proliferative, hypertrophic synovitis.
4. Rapidly destructive arthritis.
More alarmingly, the dissolved lead is absorbed through the inflamed synovial membrane directly into the systemic circulation. The rate of absorption correlates directly with the degree of bullet fragmentation (the "lead snowstorm" effect increases the surface area exposed to synovial fluid).
Clinical Presentation and Management
Systemic lead toxicity has been reported to occur anywhere from 2 days to 52 years after the initial injury.
- Symptoms: Adults with lead poisoning may present with vague, insidious symptoms including nausea, chronic diarrhea, severe abdominal colic, peripheral motor neuropathy (weakness/wrist drop), and cognitive changes.
- Laboratory Findings: Lead poisoning must be high on the differential diagnosis for any patient with a history of an intraarticular GSW who presents with microcytic hypochromic anemia (often with basophilic stippling on the peripheral smear).
- Treatment: Management is a dual-pronged approach requiring immediate medical and surgical intervention.
- Medical: Systemic chelation therapy (e.g., EDTA, succimer) to lower blood lead levels.
- Surgical: Urgent arthroscopic or open arthrotomy to meticulously extract all retained intraarticular bullet fragments and perform a thorough synovectomy to remove lead-impregnated tissue.
CONCLUSION
The operative management of complex knee pathologies demands precision and adherence to established, evidence-based protocols. The Yount posterior capsulotomy remains a powerful tool for correcting severe lateral and flexion contractures, provided the surgeon respects the local neurovascular anatomy and commits to rigorous postoperative rehabilitation. Conversely, the management of open knee wounds, particularly high-velocity gunshot injuries, relies on aggressive initial debridement, appropriate antibiotic stewardship, and the vigilance to recognize and treat both acute vascular compromise and late systemic complications like lead toxicity.
📚 Medical References
- knee capsulotomy on posterior tibial translation during posterior cruciate ligament tibial inlay reconstruction, Am J Sports Med 32:1514, 2004.
- Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete, Am J Sports Med 14:35, 1986.
- Petersen W, Lenschow S, Weimann A, et al: Importance of femoral tunnel placement in double-bundle posterior cruciate ligament reconstruction: biomechanical analysis using a robotic/universal force-moment sensor testing system, Am J Sports Med 34:456, 2006.
- Petrie RS, Harner CD: Double bundle posterior cruciate ligament reconstruction technique: University of Pittsburgh approach, Oper Tech Sports Med 7:118, 1999.
- Pournaras J, Symeonides PP: The results of surgical repair of acute tears of the posterior cruciate ligament, Clin Orthop Relat Res 267:103, 1991.
- Pournaras J, Symeonides PP, Karkavelas G: The signifi cance of the posterior cruciate ligament in the stability of the knee: an experimental study in dogs, J Bone Joint Surg 65B:204, 1983.
- Prietto MP, Bain JR, Stonebrook SN, et al: Tensile strength of the human posterior ligament (PCL), Trans Orthop Res Soc 13:195, 1988.
- Richter M, Kiefer H, Hehl G, et al: Primary repair for posterior cruciate ligament injuries: an eight-year follow-up of fi ftythree patients, Am J Sports Med 24:298, 1996.
- Ritchie JR, Bergfeld JA, Kambic H, et al: Isolated sectioning of the medial and posteromedial capsular ligaments in the posterior cruciate ligament–defi cient knee: infl uence on posterior tibial translation, Am J Sports Med 26:389, 1998.
- Roth JH, Bray RC, Best TM, et al: Posterior cruciate ligament reconstruction by transfer of the medial gastrocnemius tendon, Am J Sports Med 16:21, 1988.
- Sallay PI, McCarroll JR: Posterior cruciate ligament reconstruction using a transpatellar tendon exposure, J Orthop Tech 2:155, 1994.
- Sekiya JK, Haemmerle MJ, Stabile KJ, et al: Biomechanical analysis of a combined double-bundle posterior cruciate ligament and posterolateral corner reconstruction, Am J Sports Med 33:360, 2005.
- Shelbourne KD, Benedict F, McCarroll JR, et al: Dynamic posterior shift test: an adjuvant in evaluation of posterior tibial subluxation, Am J Sports Med 17:275, 1989.
- Shelbourne KD, Rubinstein RA: Methodist Sports Medicine Center’s experience with acute and chronic isolated posterior cruciate ligament injuries, Clin Sports Med 13:53, 1994.
- Southmayd WW, Rubin BD: Reconstruction of the posterior cruciate ligament using the semimembranosus tendon, Clin Orthop Relat Res 150:196, 1980.
- Stäubli HU, Jakob RP: Posterior instability of the knee near extension: a clinical and stress radiographic analysis of acute injuries of the posterior cruciate ligament, J Bone Joint Surg 72B:225, 1990.
- Stone JD, Carlin GJ, Ishibashi Y, et al: Assessment of posterior cruciate ligament graft performance using robotic technology, Am J Sports Med 24:824, 1996.
- Tibone JE, Antich TJ, Perry J, et al: Functional analysis of untreated and reconstructed posterior cruciate ligament injuries, Am J Sports Med 16:217, 1988.
- Torg JS, Barton TM, Pavlov H, et al: Natural history of the posterior cruciate ligament–defi cient knee, Clin Orthop Relat Res 246:208, 1989.
- Trickey EL: Injuries to the posterior cruciate ligament: diagnosis and treatment of early injuries and reconstruction of late instability, Clin Orthop Relat Res 147:76, 1980.
- Van Dommelen BA, Fowler PJ: Anatomy of the posterior cruciate ligament: a review, Am J Sports Med 17:24, 1989.
- Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries, J Am Acad Orthop Surg 1:67, 1993.
- Wascher DC, Markolf KL, Shapiro MS, et al: Direct in vitro measurement of forces in the cruciate ligaments, J Bone Joint Surg 75A:377, 1993.
- Weinstabl R, Kern H, Wagner M: Experimental investigations of stress production on the cruciate ligaments after transpatellar Steinmann’s nail fi xation. In Müller W, Hackenbruch W, eds: Surgery and arthroscopy of the knee, Second European Congress of the European Society , Heidelberg, 1988, Springer-Verlag. Whiteside LA, Kasselt MR, Haynes DW: An anatomic rationale for triple reconstruction of the posterior cruciate, Trans Orthop Res Soc 7:361, 1982.
- Wiley WB, Askew MJ, Melby A III, et al: Kinematics of the posterior cruciate ligament/posterolateral corner–injured knee after reconstruction by singleand double-bundle intraarticular grafts, Am J Sports Med 34:741, 2006.
- Wirth CJ, Jager M: Dynamic double tendon replacement of the posterior cruciate ligament, Am J Sports Med 12:39, 1984.
- Dislocations of the Knee Joint Chhabra A, Cha PS, Rihn JA, et al: Surgical management of
