Introduction & Epidemiology
The posterior approach to the knee, while less commonly employed than its medial or lateral counterparts for routine arthroplasty or isolated ligamentous pathology, remains an indispensable tool in the armamentarium of the orthopedic surgeon. Its primary utility lies in providing direct access to the posterior neurovascular bundle, the posterior capsule, and the posterior aspects of the distal femur and proximal tibia. Historically, the evolution of surgical approaches has paralleled advances in anatomical understanding and diagnostic imaging, refining indications for posterior access to optimize outcomes and minimize iatrogenic morbidity.
Epidemiologically, conditions necessitating a posterior approach are often high-energy trauma-related, such as complex tibial plateau fractures with posterior column involvement, or those involving significant neurovascular compromise. Posterior cruciate ligament (PCL) avulsion fractures, particularly from the tibial insertion, frequently benefit from direct posterior fixation. Soft tissue pathologies, including symptomatic popliteal cysts (Baker's cysts) resistant to conservative management, or severe gastrocnemius/hamstring contractures requiring lengthening procedures, also fall within its indications. The inherent risks associated with dissection in the popliteal fossa, predominantly concerning the popliteal neurovascular bundle and its superficial branches, necessitate meticulous anatomical knowledge and precise surgical technique. Of particular emphasis is the safeguarding of the medial sural cutaneous nerve, a frequently encountered structure vulnerable during the initial stages of dissection.
Surgical Anatomy & Biomechanics
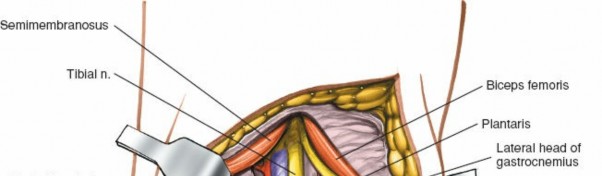
A thorough understanding of the topographical and layered anatomy of the popliteal fossa is paramount for safe and effective posterior knee access. The popliteal fossa is a diamond-shaped region bounded superiorly by the biceps femoris laterally and the semimembranosus and semitendinosus medially. Inferiorly, its borders are formed by the medial and lateral heads of the gastrocnemius muscle. The floor comprises the popliteal surface of the femur, the posterior capsule of the knee joint, and the popliteus muscle. The roof is formed by the skin and popliteal fascia.
Key Anatomical Structures:
-
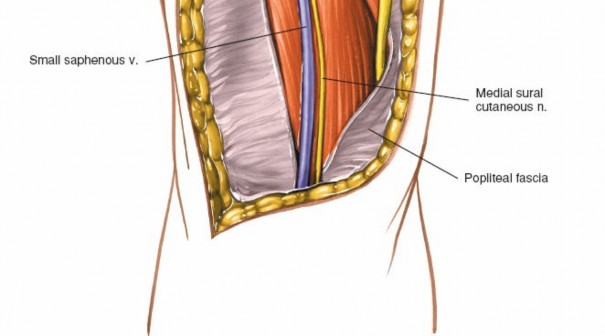
Skin and Subcutaneous Tissue: The skin in the popliteal fossa is relatively thin and mobile. Beneath the skin, the superficial fascia contains varying amounts of adipose tissue, the small saphenous vein, and critical cutaneous nerves.
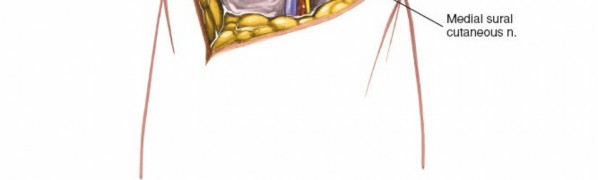
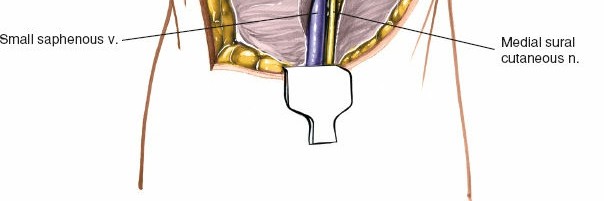
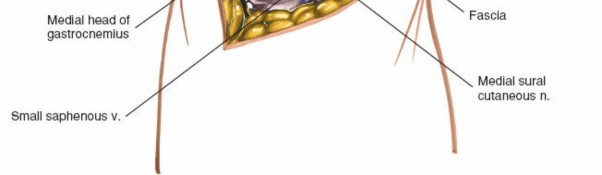
- Medial Sural Cutaneous Nerve: This nerve, a branch of the tibial nerve, typically pierces the deep fascia of the calf in the proximal one-third and descends subcutaneously to join the peroneal communicating branch, forming the sural nerve. In the popliteal fossa, it emerges superficial to the deep fascia, usually posteromedial to the midline, making it highly vulnerable during a midline or lazy-S incision. It supplies sensation to the posterolateral aspect of the leg and lateral foot. Its identification and careful retraction are crucial to prevent post-operative dysesthesia or numbness.
-
Small Saphenous Vein:
This superficial vein ascends posteriorly in the leg and typically drains into the popliteal vein, often piercing the deep fascia in the popliteal fossa. It is usually found in close proximity to the medial sural cutaneous nerve.
- Illustration of the superficial neurovascular structures in the popliteal fossa, highlighting the small saphenous vein and medial sural cutaneous nerve.
-
Popliteal Fascia: A strong, dense deep fascia that covers the popliteal fossa, providing a protective sheath for the underlying neurovascular structures. Its incision exposes the deeper compartment.
-
Muscles:
-
Superficial Layer:
- Gastrocnemius: The medial and lateral heads originate from the posterior aspects of the femoral condyles and form the most superficial muscular layer of the popliteal fossa. They are easily palpable.
- Plantaris: A small muscle belly with a long, thin tendon that lies between the gastrocnemius and soleus. Its tendon runs obliquely inferomedially.
-
Deep Layer:
- Popliteus: Originates from the lateral femoral condyle and inserts onto the posterior aspect of the tibia. It forms part of the floor of the fossa and contributes to knee stability, particularly in posterolateral rotatory stability.
-
Superficial Layer:
-
Neurovascular Structures (from superficial to deep, generally lateral to medial):
- Tibial Nerve: The most superficial and lateral of the major neurovascular structures in the popliteal fossa. It runs vertically down the midline, supplying all muscles of the posterior compartment of the leg and giving rise to the medial sural cutaneous nerve.
- Popliteal Vein: Lies deep and slightly medial to the tibial nerve. It is often the most anterior structure of the popliteal triad when viewed from a superficial posterior approach.
- Popliteal Artery: The deepest and most medial of the major neurovascular structures. It is a continuation of the femoral artery, and its distal branches include the anterior and posterior tibial arteries.
- Genicular Arteries: Five genicular arteries (superior medial, superior lateral, inferior medial, inferior lateral, middle) branch from the popliteal artery and supply the knee joint. They form an important collateral network.
- Common Peroneal Nerve: Branches off the sciatic nerve in the distal thigh or popliteal fossa. It runs along the medial border of the biceps femoris tendon, superficially crosses the lateral head of the gastrocnemius, and then winds around the neck of the fibula. It is particularly vulnerable during posterolateral approaches.
-
Ligamentous Structures:
- Posterior Capsule: A strong fibrous layer that reinforces the posterior aspect of the knee joint. It provides an attachment point for the popliteus muscle and is a key structure in PCL reconstruction and posterior capsular releases.
- Posterior Cruciate Ligament (PCL): Originates from the anterior part of the lateral aspect of the medial femoral condyle and inserts into the posterior intercondylar area of the tibia. It is the primary restraint to posterior translation of the tibia on the femur. Avulsion fractures of its tibial attachment are a common indication for posterior fixation.
Biomechanics Relevant to Posterior Approaches:
- PCL Stability: The PCL is crucial for resisting posterior tibial translation and, to a lesser extent, external rotation. Direct visualization and anatomical fixation of PCL avulsion fractures are critical for restoring posteroposterior knee stability.
- Posterior Tibial Plateau Fractures: These fractures often involve the posteromedial or posterolateral columns, leading to articular depression, varus/valgus instability, and posterior subluxation of the tibia. A posterior approach allows direct reduction and buttress plating, which is biomechanically superior for resisting shear forces and maintaining articular congruity.
- Gastrocnemius/Hamstring Contractures: These contribute to knee flexion contractures or equinus deformities. Release or lengthening procedures aim to restore joint kinematics and range of motion.
Indications & Contraindications
The posterior approach to the knee is reserved for specific pathologies where anterior, medial, or lateral approaches offer inadequate access or place critical structures at undue risk.
Indications:
- Repair of Neurovascular Structures: Primarily for acute trauma involving the popliteal artery, popliteal vein, or tibial nerve, due to knee dislocation or direct penetrating injuries.
- Posterior Cruciate Ligament (PCL) Avulsion Fractures: Direct reduction and internal fixation of tibial avulsion fractures of the PCL insertion, offering anatomical reduction and rigid fixation. Femoral avulsions are less common but can also be accessed.
- Posterior Tibial Plateau Fractures: Especially Schatzker type V or VI fractures with significant posterior column involvement, posterior Hoffa fractures (coronal shear fractures of the posterior femoral condyle), or those requiring direct posterior buttressing. The approach facilitates direct visualization, reduction, and fixation, minimizing soft tissue stripping.
- Excision of Popliteal Cysts: Particularly large, symptomatic Baker's cysts that are recurrent or causing neurovascular compression, when less invasive measures have failed.
- Gastrocnemius Recession/Lengthening: For fixed equinus contractures secondary to spasticity (e.g., cerebral palsy) or acquired conditions, involving the medial or lateral heads of the gastrocnemius.
- Hamstring Tendon Lengthening: For severe flexion contractures of the knee, typically in neurological conditions.
- Access to the Posterior Capsule: For release in severe flexion contractures, or for removal of loose bodies or osteophytes from the posterior compartment.
- Posterior Meniscal Pathology: Rarely for complex posterior horn meniscal tears or root avulsions that are difficult to address arthroscopically from anterior portals or require open repair.
- Tumor Excision: Resection of benign or malignant tumors originating from the posterior aspect of the femur, tibia, or within the popliteal fossa.
Contraindications:
- Active Infection: Absolute contraindication due to risk of spreading infection.
- Severe Peripheral Vascular Disease: Relative contraindication; meticulous dissection and potentially intra-operative vascular assessment are crucial.
- Severe Soft Tissue Compromise: Extensive scarring, burns, or poor skin quality in the popliteal fossa may preclude safe dissection and wound healing.
- Inadequate Imaging or Surgical Planning: Lack of comprehensive pre-operative imaging (CT, MRI, angiogram) or insufficient surgical planning for complex cases.
- Unfamiliarity with Anatomy: Insufficient experience or anatomical knowledge of the popliteal fossa.
Table 1: Operative vs. Non-Operative Indications for Posterior Knee Pathology
| Pathology Type | Operative Indications (Posterior Approach) | Non-Operative Indications |
|---|---|---|
| Fractures | PCL tibial avulsion (displaced), complex posterior tibial plateau (Schatzker V/VI, Hoffa), posterior femoral condyle fractures requiring direct reduction. | Stable, non-displaced PCL avulsions (rare), isolated posterior tibial plateau rim fractures without instability, minimally displaced Hoffa fractures amenable to screw fixation from an anterior approach, stable non-displaced distal femur fractures without intra-articular extension to the posterior aspect. |
| Neurovascular | Popliteal artery/vein laceration/thrombosis (acute trauma), tibial nerve transection. | Minor nerve contusions (observation), stable pseudoaneurursms (consider endovascular repair first). |
| Soft Tissue | Large, symptomatic, recurrent popliteal cyst causing pain/compression, severe gastrocnemius/hamstring contracture impacting function/gait. | Asymptomatic popliteal cysts, small cysts, cysts responsive to aspiration/steroid injection, mild contractures responsive to physical therapy/stretching, PCL tears without avulsion (non-operative often considered if isolated and grade I/II). |
| Other | Excision of posterior knee tumors, removal of large posterior loose bodies causing mechanical symptoms. | Small, asymptomatic loose bodies, mild posterior capsular impingement amenable to arthroscopic debridement. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and minimizing complications with the posterior approach.
Pre-Operative Planning:
- Detailed History and Physical Examination: Assess for neurovascular deficits, compartment syndrome risk, and skin integrity. Document pre-existing numbness or weakness.
-
Imaging Review:
- Plain Radiographs (AP, Lateral, Oblique): Initial assessment for fractures, alignment, and joint effusions.
- Computed Tomography (CT) Scan: Essential for complex fractures (tibial plateau, Hoffa), providing detailed information on fracture morphology, fragment displacement, articular involvement, and comminution. CT angiography (CTA) is indicated if vascular injury is suspected.
- Magnetic Resonance Imaging (MRI): Useful for assessing soft tissue pathology (PCL tears, meniscal tears, popliteal cysts, tumors), and the integrity of the popliteal neurovascular bundle.
- Doppler Ultrasound/Angiography: If vascular injury is suspected based on clinical exam or mechanism of injury, especially with knee dislocations.
- Surgical Consent: Thorough discussion with the patient regarding potential risks, including nerve injury (medial sural cutaneous, tibial, common peroneal), vascular injury, infection, stiffness, and the possibility of conversion to other approaches.
- Equipment Preparation: Ensure availability of appropriate instrumentation, including retractors (e.g., Langenbeck, army-navy, Senn, specialized knee retractors), vascular loops, nerve stimulator, small plates and screws (for fractures), suture anchors (for PCL avulsions), and drills. Prepare for potential intra-operative fluoroscopy.
Patient Positioning:
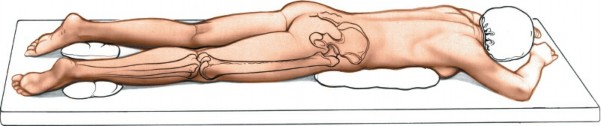
The most common and preferred position for a posterior approach to the knee is the prone position . This provides optimal exposure while minimizing the risk of contamination and facilitating C-arm access.
- Anesthesia: General anesthesia is typically employed. A regional block (e.g., femoral nerve block, sciatic nerve block) may be used adjunctively for post-operative pain control.
-
Table Setup:
The patient is carefully turned prone.
- Torso Support: Chest rolls or a well-padded Wilson frame are used to support the torso, ensuring free abdominal respiration and preventing pressure on the abdomen, which can increase epidural venous pressure and lead to increased bleeding.
- Lower Extremity Support: Both lower extremities should be carefully positioned. The operative leg is typically positioned at the end of the table. A bump or bolster is placed under the distal thigh to allow for slight knee flexion (10-20 degrees), which relaxes the hamstring and gastrocnemius muscles and opens the popliteal fossa. Alternatively, the leg can hang freely off the end of the table if more flexion is desired, with appropriate padding for the foot and ankle.
- Padding: Meticulous padding of all pressure points is critical to prevent nerve palsies (e.g., ulnar nerves at the elbows, peroneal nerves at the fibular heads, superficial peroneal nerves at the ankles).
- Tourniquet Application: A high thigh tourniquet is applied to the operative leg. This is crucial for obtaining a bloodless field, especially for vascular or fracture repairs where precise identification of structures is paramount.
- C-arm Access: Ensure unimpeded access for intra-operative fluoroscopy, particularly for fracture fixation. The C-arm can be brought in from the side or across the table.
-
Preparation and Drape:
The entire limb, from the iliac crest to the foot, is prepped and draped in a sterile fashion to allow for manipulation of the limb and access for potential graft harvest or extended incisions if needed.

-
Patient positioning in prone for posterior knee approach, showing appropriate padding and limb alignment.
- Close-up view of the knee in prone position, illustrating the use of a bolster for slight flexion.
-
Patient positioning in prone for posterior knee approach, showing appropriate padding and limb alignment.
Detailed Surgical Approach / Technique
The posterior approach to the knee requires a systematic, layered dissection to protect vital neurovascular structures, particularly the medial sural cutaneous nerve.
Landmarks and Incision
Before incision, carefully palpate the key anatomical landmarks.
*
Popliteal Fossa Crease:
The natural skin crease overlying the popliteal fossa.
*
Hamstring Tendons:
Medially, the semimembranosus and semitendinosus. Laterally, the biceps femoris. These form the superior boundaries of the fossa.
*
Gastrocnemius Heads:
The medial and lateral heads are palpable, forming the inferior boundaries. The medial head is typically more prominent.
*
Neurovascular Bundle:
While not directly palpable, its approximate course (midline) should be kept in mind.
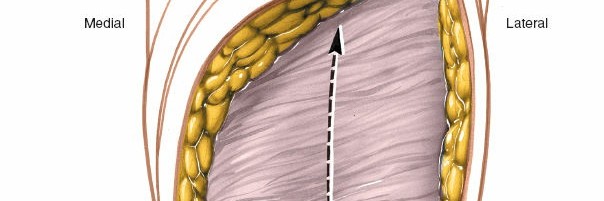
A
lazy-S or gentle curvilinear incision
is typically preferred over a straight longitudinal incision. This allows for greater extensibility, less tension on the wound edges during flexion, and often better cosmetic results. The incision should be centered over the popliteal crease, starting proximally in the distal thigh and extending distally into the proximal calf.
*
Initial marking of the lazy-S incision in the popliteal fossa.
Superficial Dissection
-
Skin Incision:
Incise the skin along the planned lazy-S mark.

- Skin incision made along the marked line.
-
Subcutaneous Tissue Dissection and Nerve Protection:
- Carefully dissect through the subcutaneous fat using a scalpel or electrocautery. The aim here is to identify and protect the medial sural cutaneous nerve and the small saphenous vein.
- The medial sural cutaneous nerve typically runs superficially and is often found emerging from the deep fascia more medially within the popliteal fossa. It usually lies medial to the small saphenous vein.
-
Use blunt dissection with small retractors or a hemostat to gently separate the subcutaneous fat. Once identified, the nerve and vein should be carefully isolated with vessel loops or rubber drains and retracted, usually medially, away from the operative field.

-
Subcutaneous dissection revealing the superficial neurovascular structures. Note the careful identification of the medial sural cutaneous nerve and small saphenous vein, which are subsequently retracted.

- Close-up view of the medial sural cutaneous nerve and small saphenous vein isolated with vessel loops.
-
Incision of Popliteal Fascia:
After retracting the superficial neurovascular structures, the deep popliteal fascia becomes visible. Incise this fascia longitudinally along the length of the exposure.
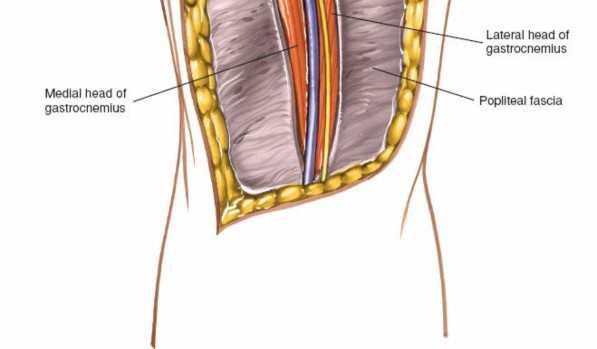
- Incision of the deep popliteal fascia, revealing the underlying muscular and neurovascular structures.
Deep Dissection and Internervous Planes
The deep dissection proceeds through the popliteal fossa, identifying the muscular and neurovascular structures. The key principle is to enter the popliteal fossa between the heads of the gastrocnemius, or to select a specific internervous plane based on the surgical target.
-
Identification of Main Neurovascular Bundle:
- After incising the deep fascia, the popliteal fat pad is encountered. Carefully dissect through this fat to expose the main neurovascular bundle.
- The tibial nerve is typically the most superficial and lateral of the major structures.
- The popliteal vein lies just deep and slightly medial to the tibial nerve.
- The popliteal artery is the deepest and most medial, often requiring gentle retraction of the nerve and vein to visualize fully.
-
These structures run roughly vertically through the center of the popliteal fossa. They should be protected meticulously, often by careful blunt dissection and isolation with vessel loops, and retracted (usually laterally) to provide access to the deeper structures.
-
Exposure of the popliteal fossa, showing the neurovascular bundle. The tibial nerve is superficial, with the popliteal vein and artery deeper.

-
Vessel loops placed around the main neurovascular structures for protection and gentle retraction.

- Another view of the protected neurovascular bundle, demonstrating gentle retraction.
- Common Peroneal Nerve: Identify the common peroneal nerve as it runs along the medial border of the biceps femoris, before wrapping around the fibular neck. It is particularly at risk with posterolateral approaches.
-
Access to the Deep Structures (Indications-Specific):
-
A. Central Posterior Approach (between gastrocnemius heads):
- This approach is useful for general posterior capsular access, PCL avulsion repairs, and excision of centrally located popliteal cysts.
- The two heads of the gastrocnemius muscle are identified. The neurovascular bundle typically lies between them or slightly medial.
- The interval between the medial and lateral heads of the gastrocnemius is developed. The medial head is innervated by the tibial nerve (medial gastrocnemius branch) and the lateral head by the tibial nerve (lateral gastrocnemius branch). The plantaris muscle and tendon are often seen deep to the gastrocnemius.
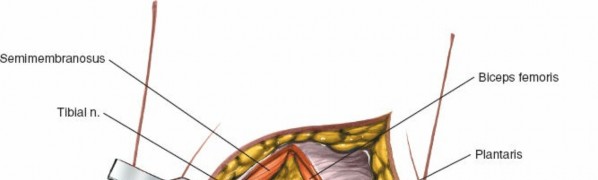
-
Retract the gastrocnemius heads to expose the posterior capsule and the popliteus muscle.
-
Dissection between the heads of the gastrocnemius, with the neurovascular bundle retracted laterally.

- Deeper view, exposing the popliteus muscle and posterior capsule after splitting the gastrocnemius.
- PCL Avulsion Repair: Incise the posterior capsule longitudinally to expose the PCL insertion site on the tibia. The avulsed fragment is identified, reduced anatomically, and fixed with suture anchors, screws, or a combination. The popliteus tendon is often anterior to the PCL insertion.
- Popliteal Cyst Excision: The cyst (typically a herniation of the semimembranosus-gastrocnemius bursa) is identified, dissected free from surrounding neurovascular structures, and excised at its stalk. Careful hemostasis is paramount.
-
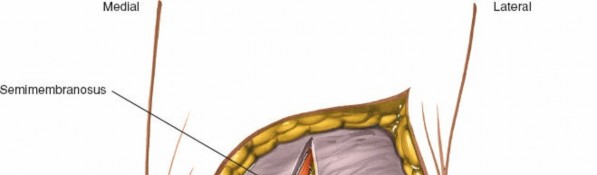
B. Posteromedial Approach (Henry's Approach, Modified):
- This approach provides excellent access to the posteromedial tibial plateau, the posteromedial capsule, and the medial aspect of the PCL insertion.
- After superficial dissection, identify the interval between the semimembranosus tendon (anterior and medial) and the medial head of the gastrocnemius (posterior and lateral).
- The saphenous nerve and great saphenous vein lie anterior to this plane and should be protected.
- The neurovascular bundle is lateral to this approach plane.
- Develop this interval. Retract the semimembranosus anteriorly and the medial gastrocnemius posteriorly. This exposes the posterior capsule and the posteromedial aspect of the proximal tibia.
-
Posteromedial Tibial Plateau Fractures:
Direct visualization allows for reduction of depressed or displaced fragments. A buttress plate can be applied to support the articular surface and prevent posterior subluxation.
-
View of the posteromedial approach, with semimembranosus retracted anteriorly and medial gastrocnemius posteriorly, revealing the posterior tibia.
-
Fracture of the posteromedial tibial plateau, exposed through the posteromedial approach.
-
Reduction and provisional fixation of the posteromedial tibial plateau fracture with K-wires.
-
Application of a buttress plate for definitive fixation of the posteromedial tibial plateau fracture.
- Final fixation construct for a posteromedial tibial plateau fracture.
-
C. Posterolateral Approach:
- This approach is suitable for posterolateral tibial plateau fractures, posterolateral corner injuries, or accessing the posterior aspect of the lateral femoral condyle (e.g., posterior Hoffa fracture).
- The interval is developed between the biceps femoris tendon (anterior and lateral) and the lateral head of the gastrocnemius (posterior and medial).
- The common peroneal nerve is a critical structure here, running along the medial border of the biceps femoris and then wrapping around the fibular neck. It must be identified and protected throughout the exposure.
-
Retract the biceps femoris anteriorly/laterally and the lateral gastrocnemius medially/posteriorly. This exposes the popliteus tendon, posterior capsule, and posterolateral aspect of the tibia and lateral femoral condyle.

- Image potentially showing the common peroneal nerve, which would be protected during a posterolateral approach.
-
-
Wound Closure:
- Achieve meticulous hemostasis.
- Perform a thorough saline washout.
- Consider placement of a suction drain if significant dead space or bleeding is anticipated.
- Close the deep fascia loosely, or not at all, to avoid compartment syndrome.
- Re-approximate the subcutaneous tissues.
-
Close the skin with interrupted sutures or staples, ensuring no undue tension.

-
Layered closure of the deep fascia and subcutaneous tissue.

-
Skin closure with interrupted sutures.

-
Final view of the incision after closure and dressing.

- Post-operative view of the incision after dressing application.
Complications & Management
Complications following a posterior approach to the knee, while relatively rare with meticulous technique, can be significant given the critical structures within the popliteal fossa. Understanding these potential complications and their management is crucial for all orthopedic surgeons.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Clinical Presentation | Management / Salvage Strategy | Populated with diverse injuries/conditions where a posterior approach is considered for superior outcomes. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a posterior approach to the knee is highly dependent on the specific surgical procedure performed, patient factors, and the presence of associated injuries. General principles include pain management, wound care, and deep venous thrombosis (DVT) prophylaxis. Specific rehabilitation protocols focus on protecting the surgical repair while progressively restoring range of motion (ROM), strength, and function.
General Considerations:
- Pain Management: Multimodal analgesia, including oral opioids, NSAIDs, acetaminophen, and regional blocks, is utilized.
- Wound Care: Daily inspection for signs of infection or hematoma. Dressing changes as per institutional protocol.
- DVT Prophylaxis: Pharmacological (e.g., LMWH) and/or mechanical (e.g., SCDs) prophylaxis is initiated post-operatively, especially for lower extremity trauma.
- Weight-Bearing Status: Dictated by the stability of any fixation and soft tissue healing.
Specific Rehabilitation Protocols:
1. Posterior Cruciate Ligament (PCL) Avulsion Repair / Reconstruction:
The primary goal is to protect the repair from posterior tibial sag while promoting healing.
-
Phase I: Protection (Weeks 0-6)
- Weight-Bearing: Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches, often for 4-6 weeks.
- Bracing: A hinged knee brace is typically worn, locked in extension or with limited flexion (e.g., 0-60 degrees) for the first 2-4 weeks. A PCL-specific brace designed to prevent posterior sag may be used for a longer duration.
- Range of Motion (ROM): Passive ROM is initiated. Emphasis on achieving full extension. Flexion is restricted to approximately 0-60 degrees initially to minimize stress on the healing PCL. Prone hangs or gravity-assisted extension can be used. Avoid active hamstring contraction against resistance.
- Exercises: Quadriceps sets, ankle pumps, straight leg raises (SLR) in the brace, gentle passive ROM.
- Precautions: Avoid isolated hamstring strengthening, resisted knee flexion, and activities that encourage posterior tibial translation.
-
Phase II: Controlled Mobility and Early Strengthening (Weeks 7-12)
- Weight-Bearing: Progress to partial weight-bearing (PWB) and then full weight-bearing (FWB) as tolerated, usually by week 8-10.
- Bracing: Continue brace use for ambulation, gradually increasing ROM as tolerated. May unlock brace for exercises.
- ROM: Gradually increase flexion, aiming for full ROM by week 12.
- Exercises: Continue quadriceps strengthening (open-chain terminal knee extension), gentle closed-chain exercises (mini-squats, leg press with caution to avoid posterior shear), gait training, balance exercises.
- Precautions: Still avoid aggressive hamstring resistance.
-
Phase III: Advanced Strengthening and Proprioception (Weeks 13-24)
- Weight-Bearing: Full weight-bearing without restrictions.
- Bracing: Wean off brace, depending on stability and surgeon preference.
- ROM: Full, pain-free ROM.
- Exercises: Progress closed-chain strengthening (squats, lunges), hamstring strengthening with increasing resistance (cautiously, emphasizing co-contraction), cardiovascular conditioning, proprioceptive training, sport-specific drills.
- Return to Activity: Gradual return to low-impact activities. High-impact or pivoting sports typically delayed until 6-9 months, pending functional assessment.
2. Posterior Tibial Plateau Fracture Fixation:
Rehabilitation focuses on protecting fracture fixation and preserving articular cartilage while promoting bone healing.
-
Phase I: Protection and Early ROM (Weeks 0-8)
- Weight-Bearing: Non-weight-bearing (NWB) for 6-8 weeks (or longer, based on fracture stability and healing).
- Bracing: Hinged knee brace for comfort and protection, locked in extension for ambulation.
- ROM: Gentle passive or active-assisted ROM, focusing on achieving full extension and controlled flexion to avoid stressing the repair. Continuous Passive Motion (CPM) machine may be used.
- Exercises: Quadriceps sets, ankle pumps, gluteal sets, SLR in brace. Upper body and core strengthening.
- Precautions: Avoid weight-bearing. Avoid aggressive ROM that causes pain or stress on the fixation.
-
Phase II: Progressive Weight-Bearing and Strengthening (Weeks 9-16)
- Weight-Bearing: Begin progressive weight-bearing (TDWB to PWB to FWB) with crutches or walker, once radiographic evidence of healing is present.
- Bracing: Continue brace as needed for stability and comfort during ambulation, weaning as strength improves.
- ROM: Progress ROM to achieve full, pain-free flexion and extension.
- Exercises: Gentle closed-chain strengthening (wall slides, mini-squats), stationary cycling, gait training, balance exercises.
-
Phase III: Advanced Strengthening and Return to Activity (Weeks 17+)
- Weight-Bearing: Full weight-bearing without assistive devices.
- Exercises: Advance strength training with increased resistance, proprioceptive exercises, agility drills, and sport-specific training.
- Return to Activity: Gradual return to activities, guided by pain, strength, and surgeon approval. High-impact activities typically delayed until 4-6 months post-op.
3. Popliteal Cyst Excision / Gastrocnemius Recession:
These procedures generally allow for earlier mobilization.
-
Popliteal Cyst Excision:
- Weight-Bearing: Weight-bearing as tolerated (WBAT) immediately post-op.
- ROM: Full ROM encouraged early to prevent stiffness.
- Exercises: Gentle stretching, light strengthening as tolerated.
- Precautions: Avoid excessive activity that could lead to hematoma formation in the early post-operative period.
-
Gastrocnemius Recession:
- Weight-Bearing: WBAT immediately, often with the foot/ankle in a neutral position (or slight dorsiflexion) if equinus was corrected.
- ROM: Early ROM, focusing on ankle dorsiflexion and knee extension.
- Exercises: Gentle stretching of the calf musculature, gait training.
- Bracing: May use a CAM walker or AFO initially to maintain dorsiflexion.
- Precautions: Avoid aggressive plantarflexion or activities that could re-injure the lengthened muscle.
Throughout all protocols, communication between the surgeon, physical therapist, and patient is crucial to adjust the protocol based on individual healing, pain levels, and progress. Regular clinical and radiographic follow-up is essential.
Summary of Key Literature / Guidelines
The literature on posterior knee approaches spans decades, evolving with advancements in diagnostic imaging, surgical instrumentation, and understanding of biomechanics.
1. PCL Avulsion Fractures:
*
Early literature
emphasized open reduction for displaced PCL avulsions, recognizing the ligament's importance in knee stability.
*
Current consensus
favors anatomical reduction and rigid internal fixation for displaced PCL tibial avulsion fractures, irrespective of fragment size, due to superior outcomes in restoring knee stability and preventing post-traumatic osteoarthritis compared to non-operative management or inadequate fixation. Techniques vary, including cannulated screw fixation, suture anchors, or tension band wiring. The posterior approach offers direct visualization and secure fixation.
*
Clinical practice guidelines
often recommend considering surgical repair for PCL avulsion fractures with displacement >3-5 mm or rotational instability.
*
Level of evidence:
Primarily Level III and IV studies (case series, retrospective reviews), with some biomechanical studies supporting anatomical fixation. Prospective comparative studies are challenging due to the relative rarity of isolated PCL avulsions.
2. Posterior Tibial Plateau Fractures:
*
Hoffa's fractures (coronal shear fractures of the femoral condyle)
, particularly posterior Hoffa's, necessitate direct posterior or posterolateral access for anatomical reduction and stable fixation. Failure to achieve anatomical reduction often leads to articular incongruity and early arthrosis.
*
Complex tibial plateau fractures (Schatzker type V/VI) with posterior column involvement
are increasingly being addressed with posterior approaches. The traditional anterior/anterolateral approaches often provide indirect reduction and may fail to adequately buttress posterior fragments, leading to instability or subsidence.
*
Guidelines for tibial plateau fractures
increasingly incorporate dual plating (anterior and posterior) or isolated posterior approaches for complex patterns, particularly those involving the posteromedial and posterolateral columns. The posteromedial approach (e.g., modified Henry's) and posterolateral approach allow direct access for reduction and buttress plating, minimizing soft tissue disruption to the main neurovascular bundle compared to a single large posterior approach.
*
Level of evidence:
Numerous Level III and IV studies, systematic reviews, and meta-analyses support direct posterior fixation for specific tibial plateau fracture patterns. Biomechanical studies consistently demonstrate the superiority of posterior buttress plating for resisting shear and maintaining reduction in posterior column fractures.
3. Popliteal Cysts (Baker's Cysts):
*
Literature reviews
suggest that surgical excision of popliteal cysts is indicated for large, symptomatic, or recurrent cysts unresponsive to conservative measures.
*
Success rates
for excision vary, with recurrence rates reported between 5-40%. Factors influencing recurrence include identification and ligation of the communicating stalk with the joint capsule, and addressing underlying intra-articular pathology (e.g., meniscal tears, osteoarthritis).
*
Level of evidence:
Primarily Level III and IV studies, reflecting the benign nature of the condition and the variability in presentation.
4. Neurovascular Repair:
* The posterior approach is the definitive surgical access for direct repair of popliteal artery and vein injuries, which are frequently associated with knee dislocations.
*
Vascular surgical guidelines
emphasize the urgency of revascularization (ideally within 6-8 hours) to prevent limb loss. Early recognition and immediate surgical intervention are paramount.
*
Level of evidence:
Strong consensus based on clinical experience and outcomes data from trauma centers.
5. Medial Sural Cutaneous Nerve Safeguarding:
* A recurring theme across all literature describing the posterior approach is the vulnerability of superficial nerves, particularly the medial sural cutaneous nerve.
*
Anatomical studies
highlight the variable course of this nerve, often superficial and posteromedial, emphasizing the need for careful subcutaneous dissection and direct identification.
*
Clinical studies
on complications report nerve injury as a common morbidity, ranging from transient paresthesia to permanent numbness.
*
Technical recommendations
consistently advocate for a lazy-S incision and meticulous, layered dissection to identify and protect this nerve.
In conclusion, the posterior approach to the knee remains a specialized yet critical surgical technique. Its application is dictated by specific anatomical pathology, with robust evidence supporting its use for complex fractures, PCL avulsions, and neurovascular injuries. The academic emphasis continues to be on meticulous surgical planning, precise anatomical dissection with particular attention to nerve preservation, and evidence-based rehabilitation protocols to optimize patient outcomes.
Clinical & Radiographic Imaging