Introduction to Femoral Shaft Fixation
The management of femoral shaft fractures represents a cornerstone of orthopedic trauma surgery. Due to the high-energy mechanisms typically responsible for these injuries, patients often present with concomitant multisystem trauma, necessitating a meticulous, evidence-based approach to surgical stabilization. While intramedullary (IM) nailing has firmly established itself as the gold standard for the vast majority of diaphyseal femur fractures, plate and screw fixation remains an indispensable technique in the orthopedic surgeon's armamentarium. Plating is particularly valuable in cases of extreme canal narrowing, periprosthetic fractures, metaphyseal-diaphyseal extensions, or in the polytraumatized patient requiring rapid "damage control" stabilization.
This comprehensive guide delineates the biomechanical principles, step-by-step surgical techniques, and postoperative protocols for both plate and screw fixation and intramedullary nailing of femoral shaft fractures.
Plate and Screw Fixation of Femoral Shaft Fractures
Historically, plating of the femur was associated with higher rates of infection and nonunion compared to closed intramedullary nailing, largely due to the extensive soft tissue stripping required for traditional open reduction and internal fixation (ORIF). However, the advent of indirect reduction techniques, extraperiosteal dissection, and locked plating constructs has revitalized the utility of femoral plating.
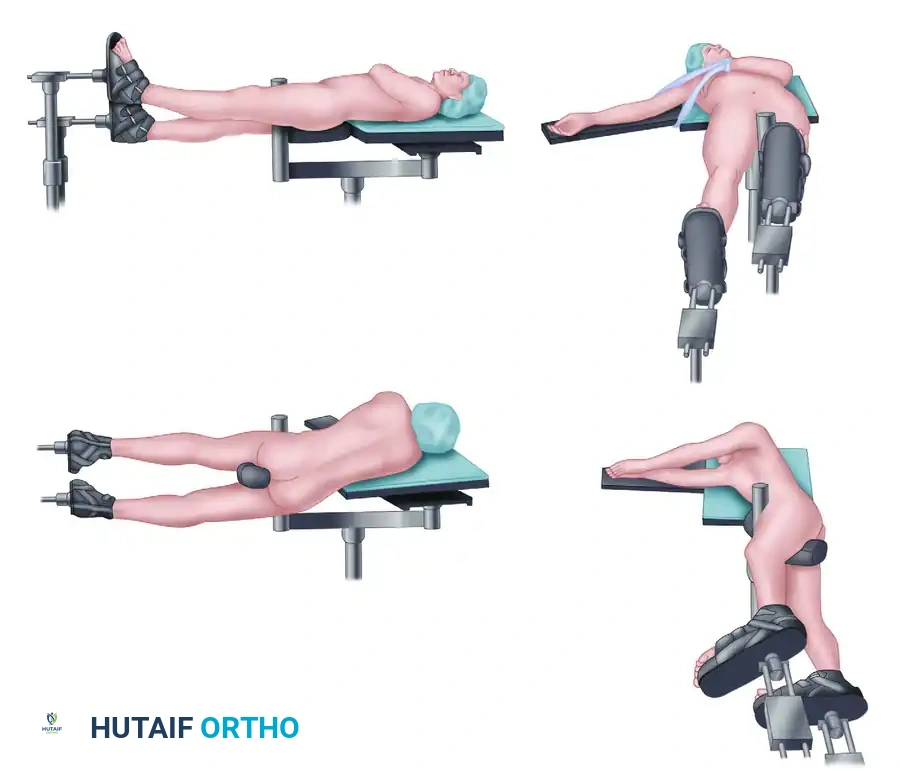
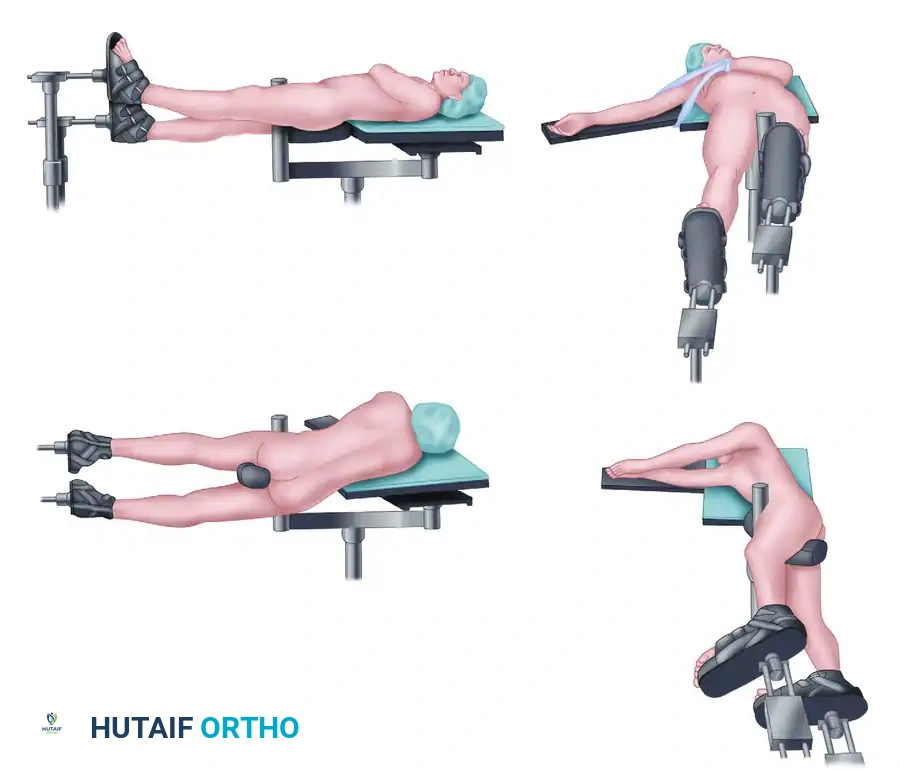
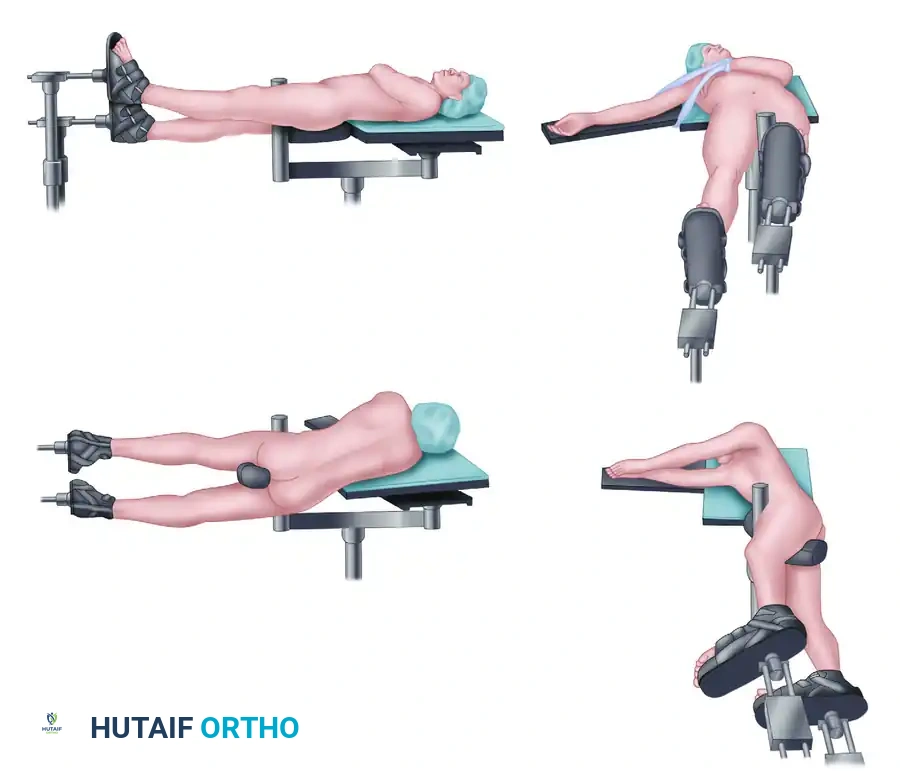
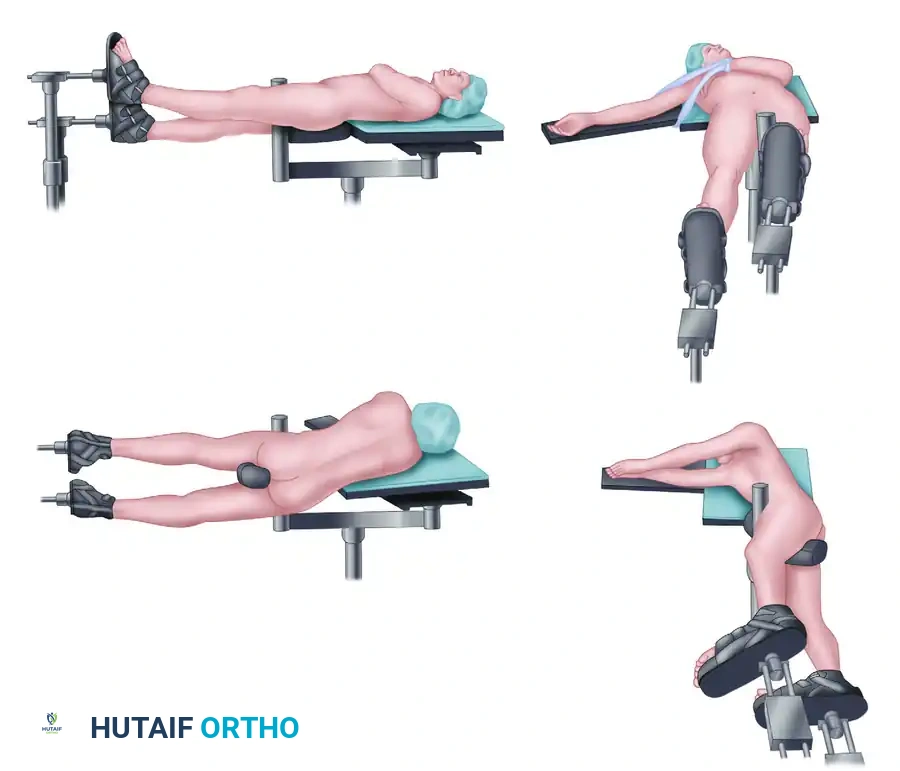
Patient Positioning and Preparation
Optimal positioning is critical for obtaining orthogonal fluoroscopic views and facilitating unimpeded surgical access.
- Place the patient supine on a fully radiolucent table. This is mandatory if fluoroscopy is planned, allowing for seamless anterior-posterior (AP) and lateral imaging.
- Place a well-padded bump under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the femur into a neutral, accessible position.
- Prepare and drape the entire leg freely, extending the sterile field to include the ipsilateral iliac crest and groin. This allows for assessment of rotational alignment and provides access for potential bone grafting.
Surgical Approach: The Lateral Extensile
The lateral approach to the femur provides direct access to the diaphysis while exploiting the internervous plane.
- Incision: Incise the skin, subcutaneous tissue, and fascia lata through a direct lateral approach centered over the fracture site.
- Deep Dissection: Incise the vastus fascia. Elevate the vastus lateralis muscle anteriorly off the lateral intermuscular septum. This is readily accomplished with a broad periosteal elevator.
- Vascular Management:
🔪 Surgical Warning: Perforating branches of the profunda femoris artery run perpendicular to the shaft of the femur approximately every 3 cm. These must be meticulously identified and ligated prior to transection. Small or medium vascular clips are highly recommended. Cauterization alone is often inadequate; subsequent muscle retraction can disrupt the clot, leading to massive postoperative hematoma.
- Retraction: Use only blunt rakes or Hohmann retractors placed carefully. Avoid placing retractors medially over the linea aspera, as this may injure the critical soft tissue attachments of butterfly fragments, devascularizing the bone and theoretically increasing the risk of nonunion.
- Periosteal Preservation: Elevate only a minimal amount of periosteum—just enough to view the fracture reduction. Expose the lateral femur in a strictly extraperiosteal fashion to preserve the cambium layer and local blood supply.
Fracture Reduction and Plate Application
Achieving anatomical alignment without compromising biology is the hallmark of modern plating.
- Visualization: Overlap the fracture ends and displace them into varus. This maneuver allows a direct, unobstructed view of the medullary canal.
- Debridement: Debride the fracture ends of any frayed soft tissue or muscle impaled on sharp bone edges. Irrigate the site copiously to remove hematoma and debris.
- Provisional Fixation: Hold the bone fragments with a thin Verbrugge-type bone-holding forceps. This instrument leaves a minimal biological "footprint."
💡 Clinical Pearl: If the Verbrugge forceps must be repositioned, completely remove and replace it rather than dragging it along the bone, which strips the periosteum and destroys cortical vascularity.
- Reduction: Bring the medial edges of the main fragments into contact while the fracture is still in varus. By gently levering against the medial bone hinge, reduce the fracture into anatomical alignment.
- Plate Placement: Apply a broad, heavy-duty plate (such as a 4.5mm broad dynamic compression plate or locking compression plate) to the flat posterolateral surface of the femur.
- Screw Insertion: Insert two fully threaded, nonlocking cortical screws adjacent to the fracture to compress the plate to the bone. Follow this by inserting the most proximal and distal screws, and then fill the remaining holes. Use standard AO compression plating techniques for simple fracture patterns.
- Bridging Constructs: For comminuted segments or osteoporotic bone, locking screw fixation should be utilized in a bridge-plating construct, bypassing the zone of comminution to preserve the fracture hematoma and promote secondary bone healing via callus formation.
- Biomechanical Considerations: Riemer et al. advocated obtaining at least 10 cortices of purchase above and below the fracture. They emphasized that only butterfly fragments necessary to determine anatomical length, axis, and rotation should be reduced. Perfect reduction of the medial cortex is not strictly necessary if length and alignment are restored.
- Bone Grafting: Historically, if stainless steel dynamic compression plates were used, autologous bone grafting from the lateral proximal tibial metaphysis was recommended to prevent hardware failure. Today, with the use of titanium alloys, locking technology, and indirect reduction maneuvers, medial bone grafting is rarely required.
Closure and Postoperative Protocol
- Closure: Do not tightly repair the vastus lateralis; simply lay it back in place over closed suction drains. Repair the fascia lata meticulously with a running or interrupted absorbable suture to prevent muscle herniation. Perform standard subcutaneous and skin closure.
- Postoperative Care:
- Patients are allowed to sit on the day of surgery.
- Drains are typically removed at 24 to 48 hours.
- Routine postoperative intravenous antibiotic prophylaxis is administered for 24 hours.
- Patients are restricted to touch-down weight bearing (TDWB) initially but are strongly encouraged to perform passive and active range-of-motion (ROM) exercises of the knee to prevent arthrofibrosis.
- Strengthening exercises are delayed until acute postoperative symptoms subside to avoid excessive shear forces at the plate-bone interface.
- Once radiographic union progresses (typically around 6-8 weeks), partial weight bearing is initiated, followed by aggressive strengthening. Unrestricted weight bearing is permitted once bridging callus is evident on three of four cortices.
Intramedullary Fixation: The Gold Standard
Internal fixation of femoral shaft fractures revolutionized orthopedic trauma care following World War II with the introduction of the Küntscher nail. Today, for a young adult patient with a diaphyseal fracture through the narrowest portion of the medullary canal (the isthmus), a locked intramedullary (IM) nail provides the ultimate biomechanical and biological treatment.
Successful IM nailing yields a short hospital stay, rapid restoration of joint motion, prompt return to ambulation, and minimized disability time. The load-sharing nature of the IM nail makes it biomechanically superior to load-bearing plates for diaphyseal fractures.
The Winquist-Hansen Classification of Comminution
The decision to use static locking (screws placed both proximally and distally) versus dynamic locking historically depended on the degree of comminution. The Winquist-Hansen classification remains the standard for describing femoral shaft comminution and guiding stability expectations.
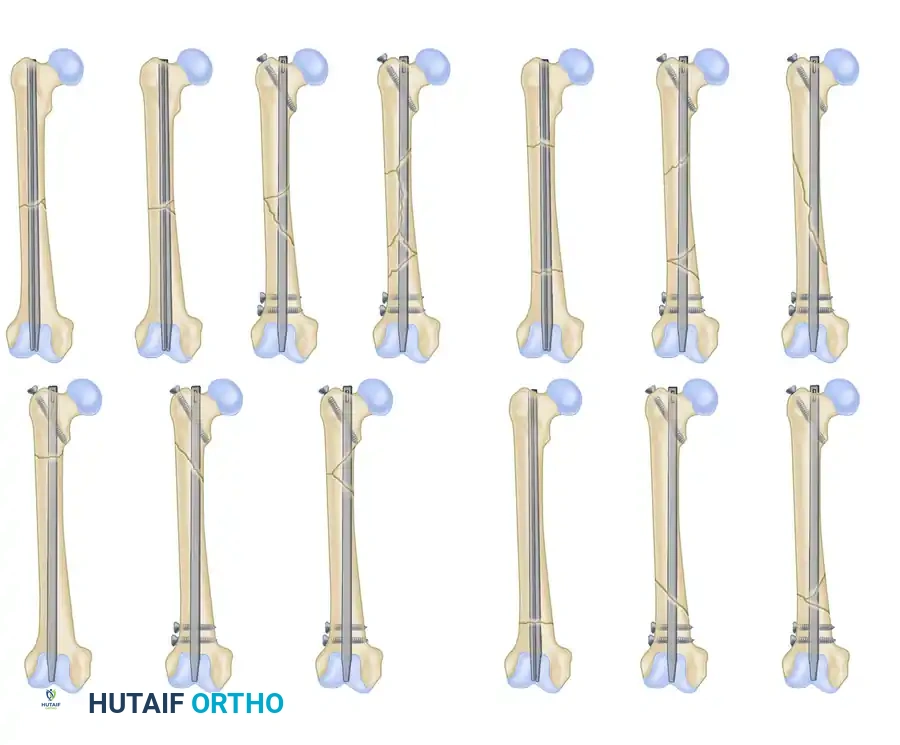
Type I: A minor comminuted fracture in which a small piece of bone (butterfly fragment) has broken off. This fragment is insignificant and does not affect the inherent cortical stability of the fracture once reduced.
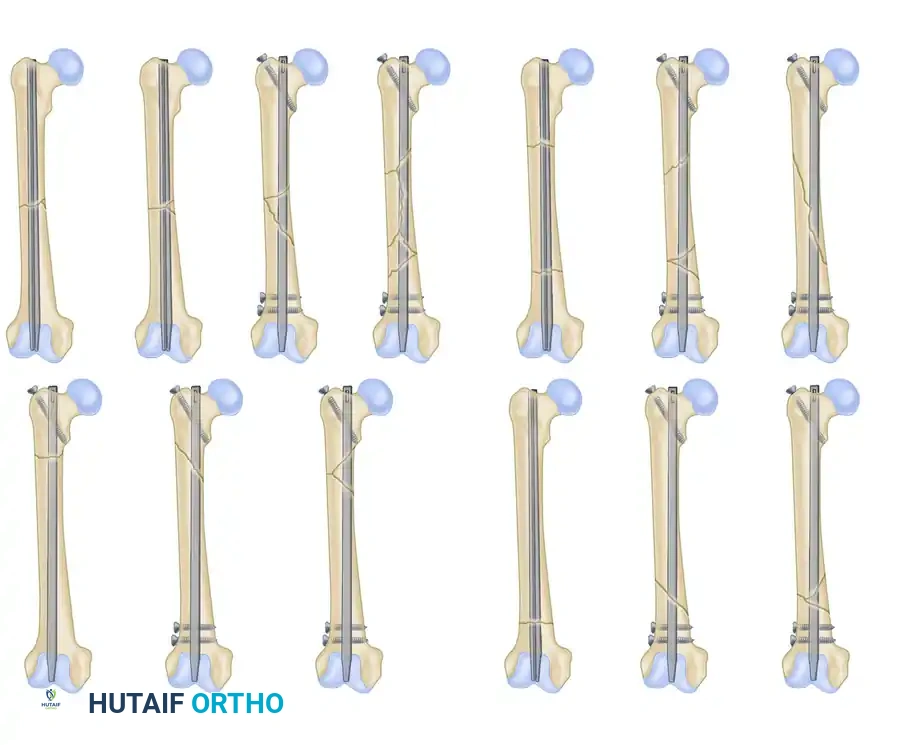
Type II: A comminuted fracture in which at least 50% contact of the abutting cortices remains. This intact cortex prevents shortening and helps control rotation, allowing sufficient proximal and distal cortical contact of the nail.
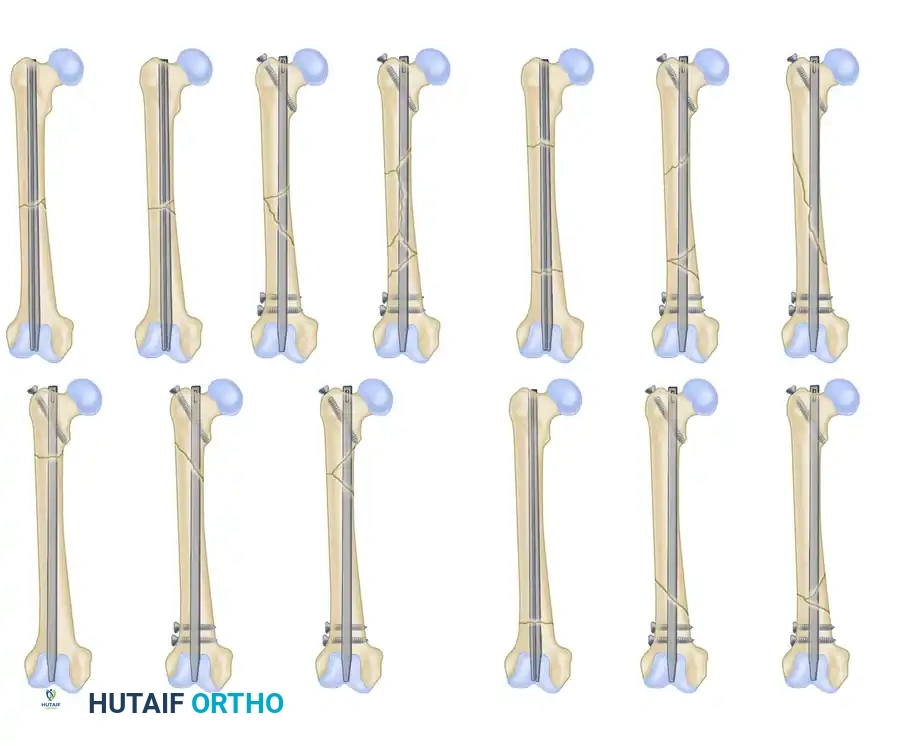
Type III: A severely comminuted fracture with less than 50% cortical contact. The purchase of the nail is poor in either the proximal or distal fragment, creating a high risk for postoperative rotation, translation, and shortening if not statically locked.
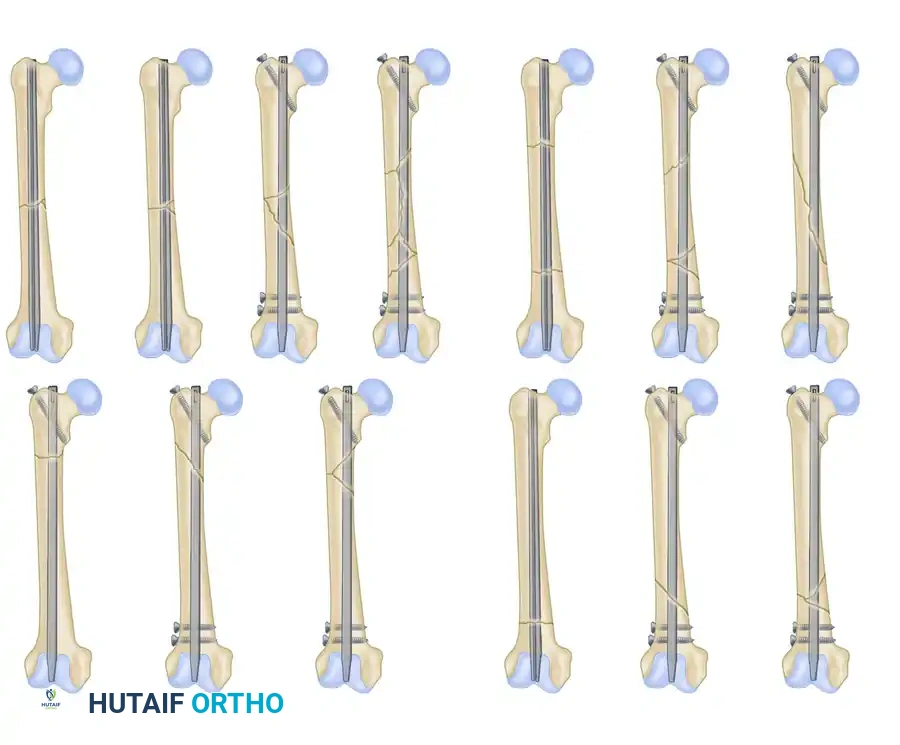
Type IV: A comminuted fracture in which the entire circumferential buttress of bone has been lost. There is absolutely no fixed contact between the major proximal and distal fragments to prevent shortening. Static interlocking is mandatory.
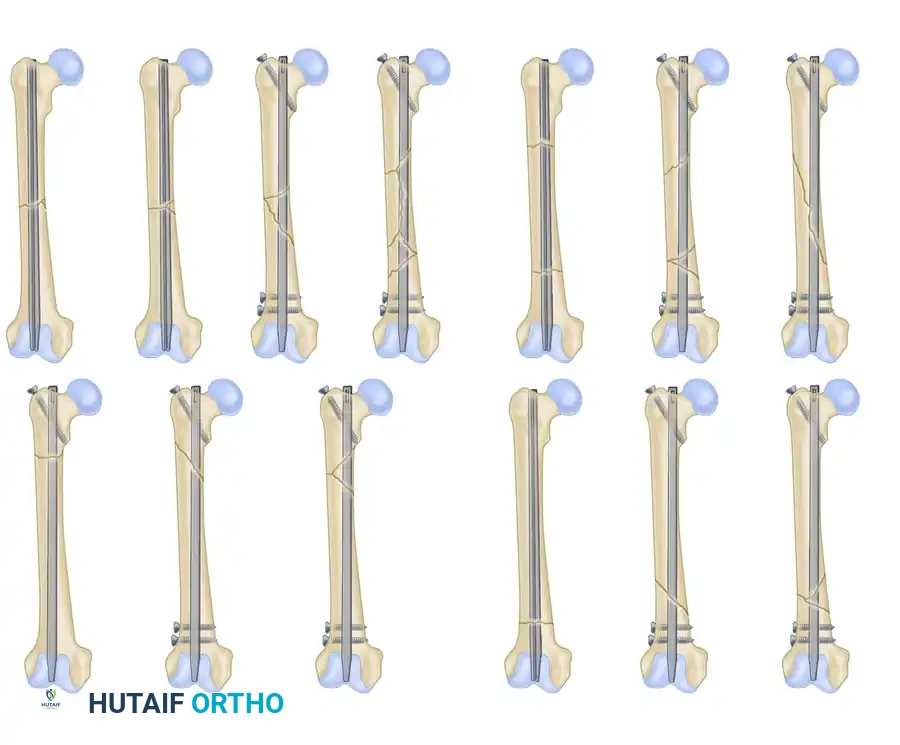
Segmental Transverse Pattern: A variant demonstrating a completely isolated diaphyseal segment with transverse fracture lines at both ends.
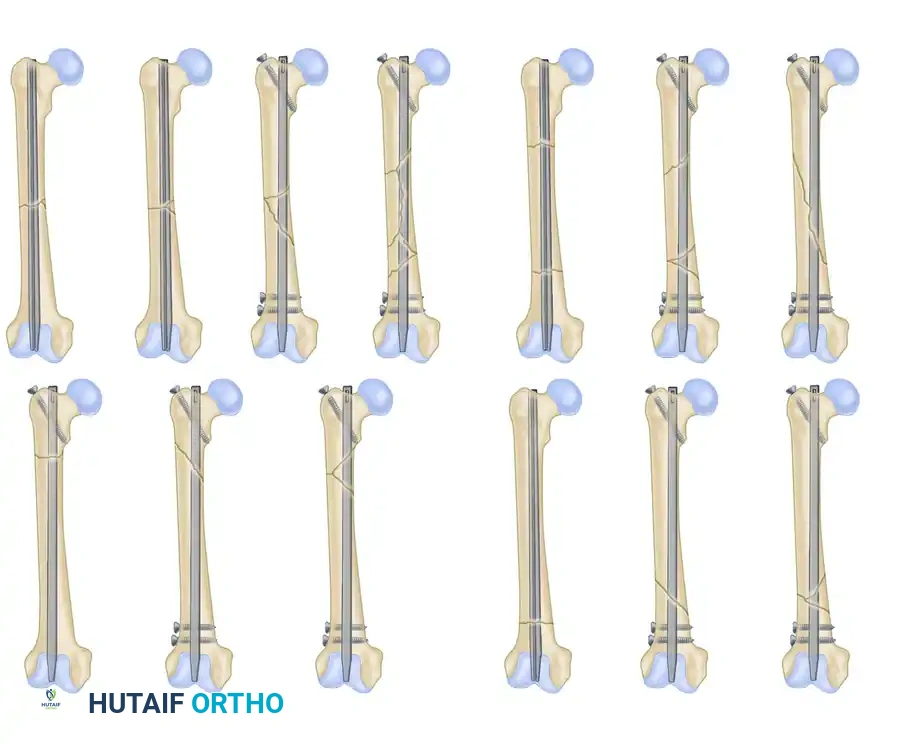
Segmental Oblique and Comminuted Pattern: A highly unstable variant requiring meticulous length and rotation control via a statically locked cephalomedullary or standard interlocking nail.
Evolution of Nailing Techniques
While Küntscher introduced closed intramedullary nailing in the 1940s, it gained widespread popularity in North America in the 1970s with the advent of intraoperative image intensification (fluoroscopy). Closed nailing drastically reduced the risk of deep infection compared to open plating.
Early unlocked nails struggled with proximal/distal third fractures and severe comminution (Winquist III and IV). The development of interlocking screws solved this by providing length and rotational control.
💡 Clinical Pearl: Always examine the ipsilateral knee under anesthesia after femoral fracture fixation. High-energy femoral shaft fractures have a high concomitant rate of ligamentous knee injuries (up to 30%), which are easily missed during the acute trauma evaluation.
Various intramedullary nail constructs demonstrating antegrade and retrograde options, as well as cephalomedullary locking configurations for proximal extension fractures.
Reamed vs. Unreamed Intramedullary Nailing
The debate between reamed and unreamed nailing has been extensively studied. Reaming generates bone debris that acts as an autogenous bone graft, stimulates the periosteal blood supply via the inflammatory response, and allows for the insertion of a larger, biomechanically stiffer nail.
Studies by Tornetta and Tiburzi, among others, have found no significant advantage to unreamed nail insertion in the femur. There are no differences in operative time, transfusion requirements, or pulmonary complications between the two techniques in isolated fractures. However, delayed unions are reported more frequently after unreamed nailing. Because the femur is enveloped by a massive, highly vascular muscle envelope, the theoretical risk of devascularizing the endosteum via reaming is clinically negligible compared to the tibia. Therefore, reamed statically locked intramedullary nailing remains the procedure of choice.
Management of Open Fractures
The incidence of infection after closed reamed nailing of closed femoral fractures is exceptionally low (<1%). For open fractures, historical protocols mandated delayed nailing to allow soft tissue stabilization. However, modern trauma literature refutes this.
Immediate reamed nailing of open femoral fractures (within 8 hours) does not significantly increase the risk of infection, with overall rates remaining between 2% and 5%.
- Protocol: Initiate immediate intravenous antibiotics based on the Gustilo-Anderson classification. Perform urgent, meticulous surgical debridement and pulsatile irrigation.
- Fixation: Stabilize the femur with a statically locked reamed IM nail.
- Wound Management: Surgically clean, lower-grade open wounds can be closed primarily over suction drains. Massive, grossly contaminated wounds (Type IIIB/IIIC) should be left open, managed with vacuum-assisted closure (VAC) dressings, and subjected to repeat debridements every 24 to 48 hours until delayed primary closure or flap coverage can be safely achieved.
Surgical Timing and the "Borderline" Polytrauma Patient
The optimal timing for IM nailing in the polytraumatized patient is a subject of intense academic debate. The concept of Early Total Care (ETC) advocates for definitive stabilization of all long bone fractures within 24 hours to reduce the systemic inflammatory response, decrease pain, and facilitate upright pulmonary mechanics.
However, Pape et al. identified a subset of "borderline" polytrauma patients—specifically those with severe blunt thoracic trauma, head injuries, or hemodynamic instability. In these patients, the "second hit" phenomenon caused by the embolization of marrow fat and the systemic inflammatory response during femoral reaming can precipitate Acute Respiratory Distress Syndrome (ARDS) and multiorgan failure.
For these borderline or unstable patients, Damage Control Orthopedics (DCO) is indicated. This involves rapid, temporary stabilization of the femur using external fixation or simple bridge plating, followed by conversion to a definitive reamed IM nail 5 to 10 days later once the patient's physiology has normalized.
Conclusion
The operative fixation of femoral shaft fractures requires a nuanced understanding of biomechanics, soft tissue handling, and systemic patient physiology. While reamed, statically locked intramedullary nailing stands as the undisputed gold standard for diaphyseal fractures, modern extraperiosteal plating techniques remain vital for specific complex fracture patterns. By adhering to strict evidence-based protocols regarding surgical timing, reduction techniques, and postoperative rehabilitation, orthopedic surgeons can reliably achieve high union rates and excellent functional outcomes.
