Percutaneous Fixation of Acute Scaphoid Fractures
DEFINITION
Located in the proximal carpal row, the scaphoid serves as an important link between the proximal and distal carpal rows. It is the most commonly fractured carpal bone, accounting for about 1 in every 100,000 emergency room visits. 17Scaphoid fractures typically result from a fall on an outstretched hand or less commonly following forced palmar flexion of the wrist 16 or axial loading of the flexed wrist such as in punching.14,26There are about 345,000 scaphoid fractures annually in the United States.
ANATOMY
The scaphoid has a complex three-dimensional geometry that has been described as a “twisted peanut.” 8 Anatomically, the scaphoid is organized into proximal pole, waist, and distal pole regions.Scaphoid dimensions vary between genders; the male scaphoid is usually longer and wider than the females. In addition, the diameter of most commercially available standard screws are larger than the proximal pole of thefemale scaphoid. 13The scaphoid articulates with the radius, lunate, capitate, trapezium, and trapezoid; thus, its surface is almost completely covered with hyaline cartilage. This feature has several important implications, including articular disruption during wire or screw insertion, paucity of vascular supply, and the absence of periosteum.Lacking periosteum, the scaphoid heals almost completely by primary bone healing, resulting in minimal callus and a biomechanically weak early union. 23Blood supply comes from branches of the radial artery that enter the scaphoid via two main routes 7:A dorsal branch, which enters the scaphoid via the dorsal ridge, provides the primary supply and 70% to 80% of the overall vascularity, including the entire proximal pole (via retrograde endosteal branches).A volar branch, which enters through the tubercle, supplies 20% to 30% of the internal vascularity, all in the distal pole.The precarious blood supply contributes to the high incidence of nonunion after a fracture at the scaphoid waist or proximal pole. It also places the proximal pole at risk for the development of avascular necrosis.
PATHOGENESIS
A scaphoid fracture classically occurs in a young, active adult most commonly following a fall onto an outstretched hand.Studies have demonstrated that wrist extension of more than 95 degrees combined with more than 10degrees of radial deviation is required for a scaphoid fracture to occur. In this position, the scaphoid abuts the distal radius, resulting in fracture.The scaphoid can also be fractured following a forced palmar flexion of the wrist injury such as punching an object. 14,26Seventy percent to 80% of scaphoid fractures occur at the waist region, whereas 10% to 20% involve the proximal pole and 5% occur at the distal pole and tuberosity.In children, the most common location for a scaphoid fracture is the distal pole. 2Although rare, scapholunate ligament injuries can occur in association with a scaphoid fracture. 15,22,28,31
NATURAL HISTORY
The true natural history of an untreated scaphoid fracture is unknown due to limitations in the existing literature, particularly with respect to study design. 16 However, several retrospective studies have suggested that if a nonunion occurs, a predictable pattern of wrist arthritis develops, usually within 10 years of the injury.19,21Unrecognized, untreated, or inadequately treated scaphoid fractures have an increased likelihood of nonunion and secondary carpal instability.A fracture through the proximal pole has the highest likelihood of nonunion, followed by a fracture of the scaphoid waist.If the scaphoid fracture is unstable, extension forces exerted on the proximal fragment (via the long radiolunate and the radioscaphocapitate ligaments) and flexion forces at the distal fragment result in a flexion (“humpback”) deformity of the scaphoid.This deformity and loss of scaphoid support results in carpal instability, most frequently a dorsal intercalated segment instability (DISI) pattern, which eventually leads to arthritis as previously described.The overall incidence of nonunion after fracture at the scaphoid waist region is about 5% to 10%. 18
PATIENT HISTORY AND PHYSICAL FINDINGS
A patient with an acute or subacute scaphoid fracture presents with radial-sided wrist pain, swelling, and loss of motion, particularly with dorsiflexion.Classic physical examination findings include the following:Edema over the dorsoradial aspect of the wristTenderness to palpation between the first and third dorsal compartments (the “anatomic snuffbox”) Tenderness with palpation volarly over the distal tuberclePain with axial compression of the wrist (scaphoid compression test) Acutely, swelling and ecchymosis over the volar radial wristP.333
IMAGING AND OTHER DIAGNOSTIC STUDIES
The following plain radiographs should routinely be ordered in the patient with a suspected scaphoid fracture: posteroanterior (PA), oblique, lateral, and dedicated scaphoid views.The PA view allows visualization of the proximal pole of the scaphoid.The semipronated oblique view provides the best visualization of the waist and distal pole regions. The semisupinated oblique view provides the best visualization of the dorsal ridge.The lateral view permits an assessment of fracture angulation, carpal alignment, and carpal instability.The dedicated scaphoid view is a PA view with the wrist in ulnar deviation. This results in scaphoid extension, allowing visualization of the scaphoid in profile.Displaced and unstable fractures are defined by the following criteria:At least 1 mm of displacementMore than 10 degrees of angular displacement Fracture comminutionRadiolunate angle of more than 15 degrees Scapholunate angle of more than 60 degrees Intrascaphoid angle of more than 35 degreesComputed tomography (CT) scan is helpful in identifying and characterizing an acute fracture and evaluating for a nonunion. Thin 1-mm cuts are obtained in the sagittal and coronal planes.Magnetic resonance imaging (MRI) is useful for diagnosing an occult fracture and, when combined with gadolinium administration, can be used to assess the vascularity of the proximal pole and the presence of avascular necrosis. Bone bruising without a fracture detected on MRI may eventually be found to be the resultof an occult fracture in 2% of cases. 27Technetium bone scan has been shown to be up to 100% sensitive in identifying occult fractures but lacks specificity. It is optimally used 48 hours after injury.
DIFFERENTIAL DIAGNOSIS
Scapholunate injury Wrist sprainWrist contusionFracture of other carpal bones Distal radius fracture
NONOPERATIVE MANAGEMENT
Nonoperative management, specifically cast immobilization, is indicated for a nondisplaced, acute ( <4 weeks from injury) fracture of the distal pole. For a nondisplaced, acute waist fracture, there is debate regarding the preferred treatment approach—cast immobilization or surgical stabilization.With cast immobilization, there is no consensus regarding the preferred position of the wrist, the need to immobilize other joints besides the wrist, and the duration of immobilization. 4Clinical studies have demonstrated no benefit with thumb immobilization nor any influence of wrist position on the rate of union.Studies have also demonstrated no difference in union rates with use of a long-arm versus short-arm cast;however, a small randomized prospective study by Gellman et al 9 demonstrated a shorter time to union and fewer nonunions and delayed unions with the initial use of a long-arm cast.In general, cast immobilization is required for 6 weeks after a distal pole fracture and 10 to 12 weeks following a nondisplaced waist fracture.Confirmation of fracture union requires serial plain radiographs demonstrating progressive obliteration of the fracture line and clear trabeculation across the fracture site. 6If there is any question regarding fracture union, particularly if the patient is returning to a contact sport, a CT scan should be obtained.
SURGICAL MANAGEMENT
Operative treatment is advocated for fractures that are unstable or displaced (see previously mentioned criteria) and following a significant treatment delay. 20Percutaneous fixation is indicated for the following:Nondisplaced fractures of the scaphoid waist Displaced fractures of the scaphoid waist Proximal pole fracturesPercutaneous stabilization of scaphoid fractures may be performed using either a volar or dorsal approach under fluoroscopic guidance. 3,11,12 If desired, a dorsal arthroscopically assisted reduction and fixation (AARF) technique can be used, which allows direct visualization after fracture reduction and stabilization.23,24,25Regardless of the technique used, the screw must be inserted in the middle third or central axis of the scaphoid, as this provides the greatest stability and stiffness, and decreases time to union. 1,29,30
PREOPERATIVE PLANNING
All imaging studies should be reviewed to identify the location of the fracture and the size of the scaphoid, both of which influence implant selection.Plain radiographs should be templated to determine the approximate screw length.The smaller size of the female scaphoid must be taken into consideration when planning internal fixation, as the diameters of most commercially available headless screws are larger than the proximal pole. 13Required equipmentPortable mini-fluoroscopy unit Kirschner wiresCannulated headless compression screw systemWrist arthroscopy equipment and traction tower for AARF
POSITIONING
The patient is positioned supine on the operating table, with the shoulder abducted 90 degrees and the arm on a radiolucent hand table.A pneumatic tourniquet is applied to the upper arm.The portable fluoroscopy unit is positioned at the end of the hand table.P.334
TECHNIQUES
Dorsal Arthroscopy-Assisted Reduction and Fixation
DORSAL ARTHROSCOPY-ASSISTED REDUCTION AND FIXATION
Nondisplaced Fracture of the Scaphoid Waist or Proximal Pole
DISPLACED SCAPHOID WAIST FRACTURE

TECH FIG 2 • A-C. Before screw insertion, the position of the Kirschner wire must be changed from its position used for arthroscopy. The Kirschner wire should be driven from volar to dorsal until the distal end lies just beneath the articular surface of the scaphoid. D,E. Screw fixation of minimally displaced scaphoid fracture via the dorsal percutaneous technique. The screw tip should rest within 1 to 2 mm of the distal cortex. Excellent compression should be obtained with this technique.

TECH FIG 3 • A. Reduction of a displaced scaphoid waist fracture using Kirschner wire joysticks. B. The Kirschner wire joystick technique for fracture reduction.(continued)
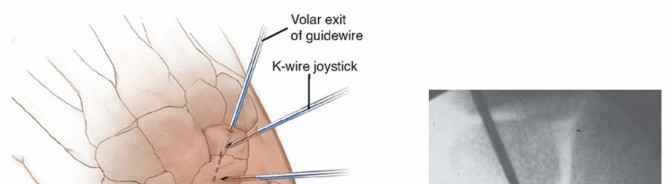
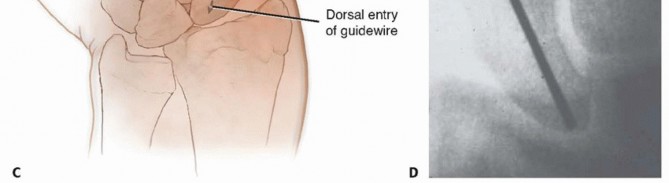
TECH FIG 3 •(continued)C. The guidewire is pulled volarly until it remains only in the distal fragment. The joysticks are then utilized to reduce the fracture. D. The guidewire is driven from volar to dorsal, transfixing the proximal fragment.
VOLAR PERCUTANEOUS APPROACH
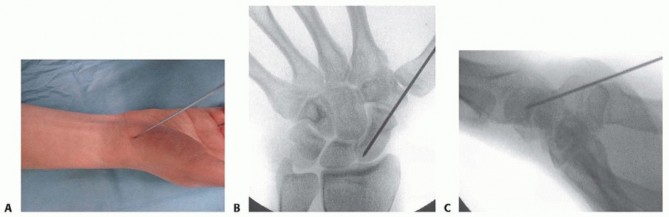
TECH FIG 4 • A-C. In the percutaneous volar approach, the guidewire is inserted into the scaphoid at the scaphotrapezial joint and into the center of the proximal pole. The wire should be inserted aiming for the Lister's tubercle. Alternatively, the guidewire may be placed directly through the trapezium into the scaphoid distal pole. 11 Advance the guidewire to the subchondral bone of the proximal pole.Place a second guidewire of equal length against the surface of the distal scaphoid, adjacent and parallelto the first guidewire. The difference between the lengths of the wires represents the length of the scaphoid.Subtract 4 mm from the length of the scaphoid to obtain the desired screw length. Use the cannulated reamer to ream the near cortex.Insert an Acutrak 2 or mini-Acutrak 2 screw (or a screw from the surgeon's chosen system) of appropriate length, remove the guidewire, and confirm satisfactory screw position and fracture reduction with fluoroscopy.P.337PEARLS AND PITFALLS
|Dorsal TechniqueInjury to dorsal ▪ Blunt dissection through the capsule minimizes the risk of injury. structuresMalpositioning of ▪ Pronate and flex the wrist until the ring sign is noted; the center of the ring is|guidewire the insertion point for the guidewire.Screw penetration1.Select a screw that is at least 4 mm shorter than the measured length of the scaphoid.2.A common mistake is to place a screw that ends up too long once the screw compresses the fragments.3.Confirm central position of guidewire via fluoroscopy.Reduction of unstable fracture1.Kirschner wires may be used as joysticks for reduction.2.A derotational Kirschner wire should be placed before reaming and screw insertion if the fragments are unstable.Extremely small proximal pole fractures1.Use a mini-Acutrak 2 screw to prevent comminution of the proximal fracture fragment.Volar TechniqueInjury to volar structures1.Blunt dissection to the scaphoid minimizes the risk of injury.Malpositioning of guidewire3.A central starting point on the distal scaphoid tuberosity can be hindered by the trapezium.4.Part of the volar trapezium can be resected to achieve a correct starting point for trajectory of the guidewire, or the wire may be inserted through the trapezium.Screw penetration1.Select a screw that is at least 4 mm shorter than the measured length of the scaphoid.2.Confirm central position of guidewire via fluoroscopy.
POSTOPERATIVE CARE
Dressings are applied, and the limb is immobilized in a forearm-based splint, immobilizing only the wrist. The thumb and fingers remain free for range-of-motion exercises.The patient is instructed in the importance of limb elevation and finger range-of-motion exercises.At 2 weeks postoperatively, the sutures are removed, a removable wrist splint is applied, and a wrist range-of-motion exercise program is initiated if fixation is rigid, the fracture is stable, and bone quality is good.If the patient is noncompliant, the fracture is deemed unstable, the fixation is less than ideal, or bone quality is poor, then a short-arm cast is applied for at least 6 weeks.Plain radiographs are obtained at 2, 6, 12, and 24 weeks postoperatively.The splint (or cast) is discontinued when union is confirmed on serial plain radiographs. If there is any question regarding fracture union, a CT scan is obtained.Unprotected strenuous activity or contact sports are not permitted until 3 months postoperatively.Contact sports may be permitted sooner in a brace depending on the type of sport, player position, and quality of fixation.
OUTCOMES
Results of contemporary techniques of percutaneous fixation are excellent; it has been shown to allow for earlier mobilization and return to activity and high satisfaction rates compared to nonoperative measures. 3,5,11,12,23,24,32The surgical approach (dorsal vs. volar percutaneous) does not affect the clinical and functional outcome. 11 Use of the transtrapezial approach does not lead to symptomatic scaphotrapezial arthritis at the short- to medium-term follow-up.10Earlier mobilization avoids complications such as muscle atrophy and joint stiffness. Percutaneous techniques result in decreased soft tissue damage compared to conventional open techniques. 32In a series of 27 consecutive patients, the union rate (confirmed by CT) was 100%. The average time to union was 12 weeks, with a prolonged time to union noted in patients with a proximal pole fracture. 24
COMPLICATIONS
The risks associated with open reduction and internal fixation, such as damage to the ligamentous support of the carpus and disruption of the dorsal blood supply, are minimized.Possible complications include the following 25: NonunionMalunionInjury to the dorsal sensory branch of the radial nerve Extensor tendon injuryInfectionTechnical problems: screw protrusion, screw malposition, bending or breakage of guidewireErosion of the trapezium and discomfort from the head of the screw has been reported with the use of a percutaneous cannulated screw inserted via the volar approach. 32
REFERENCES
- Adams BD, Blair WF, Reagan DS, et al. Technical factors related to Herbert screw fixation. J Hand Surg Am 1988;13(6):893-899.
- Amadio PC, Moran SL. Fractures of the carpal bones. In: Green D, Hotchkiss R, Pederson WC, eds. Green's Operative Hand Surgery, ed5. Philadelphia: Churchill Livingstone, 2005:711-740.
- Bond CD, Shin CA. Percutaneous cannulated screw fixation of acute scaphoid fractures. Tech Hand Up Extrem Surg 2000;4:81-87.
- Burge P. Closed cast treatment of scaphoid fractures. Hand Clin 2001;17:541-552.
- Chen AC, Chao EK, Hung SS, et al. Percutaneous screw fixation for unstable scaphoid fractures. J Trauma 2005;59:184-187.P.338
- Dias JJ, Taylor M, Thompson J, et al. Radiographic signs of union of scaphoid fractures: an analysis of inter-observer agreement and reproducibility. J Bone Joint Surg Br 1988;70:299-301.
- Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5:508-513.
- Gelberman RH, Wolock BS, Siegel DB. Fractures and non-unions of the carpal scaphoid. J Bone Joint Surg Am 1989;71A:1560-1565.
- Gellman H, Caputo RJ, Carter V, et al. Comparison of short and long thumb-spica casts for non-displaced fractures of the carpal scaphoid. J Bone Joint Surg Am 1989;71(3):354-357.
- Geurts G, van Riet R, Meermans G, et al. Incidence of scaphotrapezial arthritis following volar percutaneous fixation of nondisplaced scaphoid waist fractures using a transtrapezial approach. J Hand Surg Am 2011;36(11):1753-1758.
- Gürbüz Y, Kayalar M, Bal E, et al. Comparison of dorsal and volar percutaneous screw fixation methods in acute Type B scaphoid fractures. Acta Orthop Trauma Tur 2012;46(5):339-345.
- Haddad FS, Goddard NJ. Acute percutaneous scaphoid fixation. A pilot study. J Bone Joint Surg Br 1998;80(1):95-99.
- Heinzelmann AD, Archer G, Bindra RR. Anthropometry of the human scaphoid. J Hand Surg 2007;32(7):1005-1008.
- Horii E, Nakamura R, Watanabe K, et al. Scaphoid fracture as a “puncher's fracture.” J Ortho Trauma 1994;8:107-110.
- Jørgsholm P, Thomsen NO, Björkman A, et al. The incidence of intrinsic and extrinsic ligament injuries in scaphoid waist fractures. J Hand Surg 2010;35(3):368-374.
- Kerluke L, McCabe SJ. Nonunion of the scaphoid: a critical analysis of recent natural history studies. J Hand Surg Am 1993;18(1):1-3.
- Kozin SH. Incidence, mechanism, and natural history of scaphoid fractures. Hand Clin 2001;17:515-524.
- Leslie IJ, Dickson RA. The fractured carpal scaphoid. Natural history and factors influencing outcome. JBone Joint Surg Br 1981;63-B(2): 225-230.
- Mack GR, Bosse MJ, Gelberman RH, et al. The natural history of scaphoid nonunion. J Bone Joint Surg Am 1984;66(4):504-509.
- Martus JE, Bedi A, Jebson PJ. Cannulated variable pitch compression screw fixation of scaphoid fractures using a limited dorsal approach. Tech Hand Upper Ext Surg 2005;9:202-206.
- Ruby LK, Stinson J, Belsky MR. The natural history of scaphoid non-union: a review of fifty-five cases. J Bone Joint Surg Am 1985;67(3):428-432.
- Schädel-Höpfner M, Junge A, Böhringer G. Scapholunate ligament injury occurring with scaphoid fracture—a rare coincidence? J Hand Surg Br 2005;30:137-142.
- Slade JF III, Dodds SD. Minimally invasive management of scaphoid nonunions. Clin Orthop 2006;445:108-119.
- Slade JF III, Gutow AP, Geissler WB. Percutaneous internal fixation of scaphoid fractures via an arthroscopically assisted dorsal approach. J Bone Joint Surg Am 2002;84:21-36.
- Slade JF III, Jaskwhich D. Percutaneous fixation of scaphoid fractures. Hand Clin 2001;17:553-574.
- Sutton PA, Clifford O, Davis TRC. A new mechanism of injury for scaphoid fractures: ‘test your strength’ punch-bag machines. J Hand Surg Eur Vol 2010;35(5):419-420.
- Thavarajah D, Syed T, Shah Y, et al. Does scaphoid bone bruising lead to occult fractures? A prospective study of 50 patients. Injury 2011;42:1303-1306.
- Thomsen L, Falcone MO. Lesions of the scapholunate ligament associated with minimally displaced or non-displaced fractures of the scaphoid waist. Which incidence? Chir Main 2012;31:234-238.
- Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid. Treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 1996;78(12):1829-1837.
- Trumble TE, Gilbert M, Murray LW, et al. Displaced scaphoid fractures treated with open reduction and internal fixation with a cannulated screw. J Bone Joint Surg Am 2000;82(5):633-641.
- Wong TC, Yip TH, Wu WC. Carpal ligament injuries with acute scaphoid fractures: a combined wrist injury. J Hand Surg Br 2005;30:415-418.
- Yip HS, Wu WC, Chang RY, et al. Percutaneous cannulated screw fixation of acute scaphoid waist fracture. J Hand Surg Br 2002;27(1):42-46.
