Pelvic Ring Fractures
Pelvic ring fractures are high energy fractures that typically occur due to blunt trauma. Here's what you need to know about their diagnosis, treatment, and prognosis:
Summary
Pelvic ring fractures are high energy fractures of the pelvic ring which typically occur due to blunt trauma. Diagnosis is made radiographically with pelvic radiographs and further characterized with CT scan. Treatment is typically operative fixation depending on degree of pelvis instability, fracture displacement and patient activity demands.
Etiology
- Associated injuries: Orthopaedic injuries include chest injury in up to 63%, long bone fractures in 50%, and spine fractures in 25%. Non-orthopaedic injuries can involve the urogenital system, with sexual dysfunction in up to 50%, and head and abdominal injury in 40%.
-
Pediatric pelvic ring fractures:
Children with open triradiate cartilage have different fracture patterns than do children whose triradiate cartilage has closed. Fractures usually involve the pubic rami and iliac wings and rarely require surgical treatment.
Figure 1: Pelvic Ring Fracture (Source: Hutaif Orthopedic Center)
Anatomy
| Osteology | Ring structure made up of the sacrum and two innominate bones. Stability is dependent on strong surrounding ligamentous structures. Displacement can only occur with disruption of the ring in two places. Neurovascular structures are intimately associated with posterior pelvic ligaments. |
|---|---|
| Ligaments https://hutaifortho.com/upload/1694718117.png | |
| 1. Anterior: Symphyseal ligaments resist external rotation. | |
| 2. Pelvic floor: Sacrospinous ligaments resist external rotation, while sacrotuberous ligaments resist shear and flexion. | |
| 3. Posterior sacroiliac complex (posterior tension band): Strongest ligaments in the body and more important than anterior structures for pelvic ring stability. Anterior sacroiliac ligaments resist external rotation after failure of pelvic floor and anterior structures, while interosseous sacroiliac resist anterior-posterior translation of pelvis, posterior sacroiliac resist cephalad-caudad displacement of pelvis and iliolumbar resist rotation and augment posterior SI ligaments. | |
| Vascular | Common iliac system begins near L4 at bifurcation of abdominal aorta. External iliac artery courses anteriorly along pelvic brim and emerges as the common femoral artery distal to the inguinal ligament. Internal iliac artery dives posteriorly near SI joint and divides in the posterior division (giving off superior gluteal artery) and anterior division (becoming obturator artery). Corona mortis is a connection between the obturator and external iliac systems, and has a mean distance of 6.2cm from the pubic symphysis. Venous plexus in posterior pelvis accounts for 90% of the hemorrhage associated with pelvic ring injuries. |
| Neurologic | Lumbosacral trunk crosses anterior sacral ala and SI joint. L5 nerve root exits below L5 TP a courses over sacral ala 2cm medial to SI joint. |
| ## Classification | |
| There are two classifications of pelvic ring fractures: | |
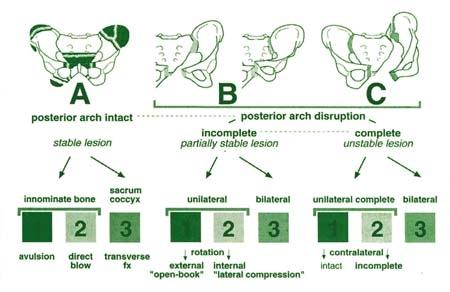
| 1. Tile classification: Classifies fractures based on stability and degree of rotation. Stable fractures are Type A, rotationally unstable and vertically stable fractures are Type B, and rotationally and vertically unstable fractures are Type C. (View Image) | |
| 2. Young-Burgess Classification: Classifies fractures based on mechanism of injury and direction of force. (View Image) | |
| ## Physical Exam | |
| Physical exam findings include pain and inability to bear weight. Inspect for stability by placing gentle rotational force on each iliac crest, and look for abnormal lower extremity positioning such as external rotation of one or both extremities and limb-length discrepancy. Check for skin hematoma, swelling, ecchymosis, and lacerations, as well as urogenital and neurologic injuries. A rectal exam may be performed to evaluate sphincter tone and perirectal sensation, and a vaginal exam may be performed to rule out occult open fracture. | |
| ## Imaging | |
| The recommended imaging for pelvic ring fractures includes: | |
| 1. AP pelvic radiograph | |
| 2. Inlet pelvic radiograph | |
| 3. Outlet pelvic radiograph | |
| 4. Single-leg stance AP pelvis ("flamingo views") | |
| CT is also typically performed and is considered routine. Findings may include radiographic signs of instability such as displacement or sacral fractures. | |
| ## Initial Management & Resuscitation | |
| The bleeding source must be identified and resuscitation should begin with PRBC, FFP, and platelet transfusion. A pelvic binder or sheet may be applied as initial management for an unstable ring injury before transitioning to external fixation or ORIF. Angiography and embolization may also be indicated in select cases. | |
| ## Definitive Treatment | |
| Definitive treatment for stable fractures is weight bearing as tolerated, while unstable fractures may require surgical treatment such as ORIF, external fixation, or diverting colostomy. Rehabilitation should be gradually advanced when radiographic healing has occurred. | |
| ## Complications | |
| Complications may include urogenital injuries, neurologic injury, DVT and PE, chronic instability, infection, and poor functional outcome associated with certain factors including SI joint incongruity, neurologic injury, and urethral injury. | |
| ## Prognosis | |
| Poor functional outcome with chronic pain and/or sexual dysfunction is common. Mortality rate is up to 15% for closed fractures and as much as 50% for open fractures. | |

|
|

|
|
| ## Test Your Knowledge | |
| Take the following quiz to see what you know about pelvic ring fractures: 1. What is the most common cause of pelvic ring fractures? Sports injuries and falls | |
| Non-accidental trauma | |
| Blunt trauma | |
| Infection 2. What type of ligament resists external rotation after failure of pelvic floor and anterior structures? Anterior sacroiliac ligaments | |
| Iliolumbar ligaments | |
| Interosseous sacroiliac ligaments | |
| Posterior sacroiliac ligaments 3. How are pelvic ring fractures typically diagnosed? MRI | |
| CT Scan | |
| X-ray of the hip | |
| Ultrasound 4. What is the recommended initial management for an unstable ring injury? ORIF | |
| External fixation | |
| Pelvic binder | |
| Diverting colostomy 5. What is the typical prognosis for pelvic ring fractures? | |
| Excellent with few complications | |
| Poor, with high rates of mortality and morbidity | |
| Average, with moderate rates of recovery | |
| Uncertain, with highly variable outcomes | |
| Submit |
