- PATHOLOGIC FRACTURES ## DEFINITION
- A pathologic fracture is one that occurs when the normal integrity and strength of bone have been compromised by invasive disease or destructive processes.
- Causes include neoplasm (primary tumor or metastatic disease), necrosis, metabolic disease, disuse, infection, osteoporosis, alteration of normal bone repair mechanisms or iatrogenic causes (e.g., surgical defect).
- Fractures more common in benign tumors (vs. malignant tumors).
- Most are asymptomatic before fracture.
- Antecedent nocturnal symptoms are rare.
- Most common in children:
- Humerus
- Femur
- Unicameral bone cyst, nonossifying fibroma, fibrous dysplasia, and eosinophilic granuloma are common predisposing conditions.
- Primary malignant tumors
- These are relatively rare.
- Osteosarcoma, Ewing sarcoma, chondrosarcoma, malignant fibrous histiocytoma, and fibrosarcoma are examples.
-
They may occur later in patients with radiation-induced osteonecrosis (Ewing sarcoma,
lymphoma). - Suspect a primary tumor in younger patients with aggressive-appearing lesions:
- Poorly defined margins (wide zone of transition)
- Matrix production
- Periosteal reaction (Codman triangle)
- Large soft tissue component
- Patients usually have antecedent pain before fracture, especially night pain.
- Pathologic fracture complicates but does not mitigate against limb salvage.
- Local recurrence is higher.
- Patients with fractures and underlying suspicious lesions or history should be referred for evaluation and possibly biopsy.
- Always obtain a biopsy of a solitary destructive bone lesion, even in patients with a history of primary carcinoma, before proceeding with definitive fixation.
MECHANISM OF INJURY
- Pathologic fractures typically occur as a result of minimal trauma or even during normal activities.
- Alternatively, pathologic fractures may occur during high-energy trauma involving a region that is predisposed to fracture.
CLINICAL EVALUATION
-
History: Suspicion of pathologic fracture should be raised in patients presenting with fracture involving:
- Normal activity or minimal trauma
- Excessive pain at the site of fracture prior to injury
- Patients with a known primary malignant disease or metabolic disease
- A history of multiple fractures
- Risk factors such as smoking or environmental exposure to carcinogens
-
Physical examination: In addition to the standard physical examination performed for the specific fracture encountered, attention should be directed to evaluation of a possible soft tissue mass at fracture site or evidence of primary disease such as lymphadenopathy, thyroid nodules, breast masses, prostate nodules, and rectal lesions, as well as examination of other painful regions to rule out impending fractures.
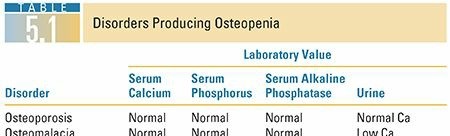
LABORATORY EVALUATION ( TABLE 5.1)


12. Complete blood cell count (CBC) with differential, red blood cell indices, and peripheral smear
13. Erythrocyte sedimentation rate (ESR)
14. ## Chemistry panel: electrolytes, with calcium, phosphate, albumin, globulin, alkaline phosphatase
15. Urinalysis
16. Stool guaiac
17. Serum and urine protein electrophoresis (SPEP, UPEP) to rule out possible myeloma
18. Twenty-four–hour urine hydroxyproline to rule out Paget disease
19. ## Specific tests: thyroid function tests (TFTs), carcinoembryonic antigen (CEA), parathyroid hormone (PTH), prostate-specific antigen (PSA)
RADIOGRAPHIC EVALUATION
-
Plain radiographs: As with all fractures, include the joint above and below the fracture. It is difficult to measure size accurately, particularly with permeative lesions; >30% of bone must be lost before it is detectable by plain radiography.
-
Chest radiograph: to rule out primary lung tumor or metastases in all cases.
-
Bone scan: This is the most sensitive indicator of skeletal disease. It gives information on the presence of multiple lesions, correlates “hot” areas with plain x-rays, and may be “cold” with myeloma and other hematologic malignancies
-
Computed tomography (CT): This is a more sensitive test for lesions that destroy <30% bone. It also shows soft tissue extension of a lesion.
-
Magnetic resonance imaging (MRI): More useful for primary bone tumor. Shows the bony extent of the lesion, bone marrow changes, periosteal reaction, and soft tissue extension. Spine MRI is also useful to evaluate for spinal canal compromise.
-
Positron emission tomography (PET) scan: More sensitive than bone scan in finding metastatic lesions. Especially helpful in primary lung carcinoma.
- Other useful tests in evaluating a patient with suspected pathologic fracture of unknown origin include the following ( Table 5.2):
- Upper/lower gastrointestinal series
- Endoscopy
- Mammography
-
CT of the chest, abdomen, and pelvis


Despite an elaborate workup, the primary disease process will not be identified in 15% of patients with suspected metastatic disease.
CLASSIFICATION Springfield This is based on the pattern of bone invasion.
Systemic
27. ## Osteoporosis: This is the most common cause of pathologic fractures in the elderly population. The treatment of osteoporosis with bisphosphonates can alter normal bone remodeling processes, which increases the risk for femoral stress fractures.
28. ## Metabolic bone disease: Osteomalacia, hyperparathyroidism, and renal osteodystrophy may be present.
29. ## Paget disease: This is present in 5% to 15% of the elderly population. Pathologic fracture is the most common orthopaedic complication, seen in 10% to 30% of patients and often the first manifestation of unrecognized Paget disease.
Localized
30. This accounts for the majority of pathologic fractures and includes
1. Primary malignancy of bone
2. Hematopoietic disorders: myeloma, lymphoma, leukemia
3. Metastatic disease:
1. Most pathologic fractures (80%) from metastatic disease arise from lesions of the breast, lung, thyroid, kidney, and prostate.
2. Most common locations include the spine, ribs, pelvis, femur, and humerus.
Classification by Pathologic Process
Systemic Skeletal Disease
31. Bones are weak and predisposed to fracture. Healing and callus formation are normal.
32. Correctable disorders include osteomalacia, disuse osteoporosis, hyperparathyroidism, renal osteodystrophy, and steroid-induced osteoporosis.
33. Noncorrectable disorders include osteogenesis imperfecta, polyostotic fibrous dysplasia, osteopetrosis, postmenopausal osteoporosis, Paget disease, rheumatoid arthritis, and Gaucher disease.
Local Disease
34. Benign primary bone tumors
1. Nonossifying fibroma, unicameral bone cyst, aneurysmal bone cyst, enchondroma, chondromyxoid fibroma, giant cell tumor, osteoblastoma, chondroblastoma, eosinophilic granuloma
35. Malignant primary bone tumors
1. Ewing sarcoma, multiple myeloma, non-Hodgkin lymphoma, osteosarcoma, chondrosarcoma, fibrosarcoma, malignant fibrous histiocytoma
36. Carcinoma metastasized to bone
Miscellaneous
37. Irradiated bone
38. Congenital pseudarthrosis
39. Localized structural defects
TREATMENT Initial Treatment 40. ## Standard fracture care: reduction and immobilization
- Evaluation of underlying pathologic process
- Optimization of medical condition Nonoperative Treatment 43. In general, fractures through primary benign lesions of bone will heal without surgical management.
- Healing time is slower than in normal bone, particularly after radiation therapy and chemotherapy.
- Contrary to popular belief, the fracture will not stimulate involution of the lesion. Operative Treatment 46. Goals of surgical intervention are:
- Prevention of disuse osteopenia
- Mechanical support for weakened or fractured bone to facilitate performance of daily activities
- Pain relief
- Decreased length and cost of hospitalization
- Internal fixation, with or without cement augmentation, is the standard of care for most pathologic fractures, particularly long bones. Internal fixation will eventually fail if the bone does not unite.
- Resection and prosthetic reconstruction may be considered for impending pathologic fractures in periarticular locations or if attempts at internal fixation fail.
- Loss of fixation is the most common complication in the treatment of pathologic fractures, owing to poor bone quality.
- Contraindications to surgical management of pathologic fractures are:
- General condition of the patient inadequate to tolerate anesthesia and the surgical procedure
- Mental obtundation or decreased level of consciousness that precludes the need for local measures to relieve pain
- Life expectancy of <1 month (controversial)
- Adequate patient management requires multidisciplinary care by oncologists, internal medicine physicians, and radiation therapists.
- Radiation and chemotherapy are useful adjunctive therapies in the treatment of pathologic fractures, as well as potential mainstays of therapy in cases of metastatic disease.
-
These treatments are used to decrease the size of the lesion, stop lesion progression, and
alleviate symptoms. - They delay soft tissue healing and should not be administered until 10 to 21 days postoperatively.
- Renal cell carcinoma is more resistant to radiation and chemotherapy.
- Renal cell and thyroid carcinomas may be highly vascular and thus preoperative local embolization should be performed.
- Goals of surgery in treating patients with pathologic fractures are:
- Pain relief
- Restoration of function
- Facilitation of nursing care
- Pathologic fracture survival
- Seventy-five percent of patients with a pathologic fracture will be alive after 1 year.
- The average survival is ~21 months and varies according to primary diagnosis (e.g., shorter for lung carcinoma).
- Pathologic fracture treatment includes:
- Biopsy, especially for solitary lesions before proceeding with definitive surgery
- Nails versus plates versus arthroplasty
- Interlocked cephalomedullary nails to stabilize the entire bone (e.g., cephalomedullary nails for femoral lesions)
- Arthroplasty for periarticular fractures, especially around the hip
- Cement augmentation, which is often necessary
- Radiation and chemotherapy
- Aggressive rehabilitation Adjuvant Therapy: Radiation Therapy and Chemotherapy 55. Role in treatment of pathologic fractures:
- Palliate symptoms
- Diminish lesion size
- Prevent advancement of lesion Metastases of Unknown Origin 56. Three percent to 4% of all carcinomas have no known primary site.
-
Ten percent to 15% of these patients have bone metastases.
Management of Specific Pathologic Fractures
Femur Fractures - The proximal femur is involved in >50% of long bone pathologic fractures resulting from high weight-bearing stresses.
- Pathologic fractures of the femoral neck generally do not unite regardless of the degree of displacement; these require proximal femoral replacement. If the acetabulum is not involved, a hemiarthroplasty may be indicated; however, with acetabular involvement, total hip replacement is required.
- Pathologic femoral shaft fractures may be managed with cephalomedullary nailing.
- Indications for prophylactic fixation (Harrington) are
- Cortical bone destruction ≥50%
- Proximal femoral lesion ≥2.5 cm
- Pathologic avulsion of the lesser trochanter
- Persistent pain following irradiation
-
Mirel’s scoring system for prophylactic fixation (
Clin Orthop
1989) is useful (
Table 5.3).


- Advantages of prophylactic fixation compared to fixation after fracture occurs are as follows:
- Decreased morbidity
- Shorter hospital stay
- Easier rehabilitation
- Pain relief
- Faster and less complicated surgery
-
Decreased surgical blood loss
Humerus Fractures - The humeral shaft is frequently involved with metastatic disease, thus increasing the possibility of humeral shaft fracture.
- Prophylactic fixation of impending pathologic fractures is not recommended on a routine basis.
-
Operative stabilization of pathologic fractures of the humerus may be performed to alleviate pain, to reduce the need for nursing care, and to optimize patient independence.
Spine Fractures - If painful but no neurologic loss or loss of height, can treat with radiation therapy.
- For fractures caused by osteoporosis, myeloma, metastatic carcinoma, and percutaneous cement placement in the vertebral body can be used. There is concern for leakage of cement into the canal and adjacent veins.
- For neurologic loss, spinal decompression and fusion with internal fixation can be done anteriorly or posteriorly.
