Partial Scaphoid Excision of Scaphoid Nonunions
DEFINITION
Scaphoid fractures are quite commonplace, representing the most frequently fractured carpal bone with an annual incidence of approximately 29 per 100,000.5 Fractures of the scaphoid, when treated acutelyand appropriately, have union rates greater than 90%.3,9 However, without proper diagnosis and treatment, scaphoid fractures frequently result in nonunion.Initial treatment for a scaphoid nonunion is typically open reduction and internal fixation (ORIF) with bone graft, be it a corticocancellous wedge or a vascularized graft.Despite appropriate internal fixation and bone grafting, failure rates are approximately 15% in waist fractures and 33% in proximal pole fractures.12If ORIF and bone grafting fails, the surgeon is then left with difficult choices.Revision ORIF with bone grafting (failure rate of 50%)2,16Salvage procedure which may have a higher rate of satisfactory resultsSilicone prostheses previously described have had poor results due to silicone synovitis and implant loosening, dislocation, and breakage.13When a patient has pain caused by a chronic scaphoid nonunion (FIG 1) with posttraumatic arthritis limited to the distal pole of the scaphoid and radial styloid, partial scaphoid excision (distal fragment) provides a reasonable, low-morbidity alternative treatment option.4,11,15
ANATOMY
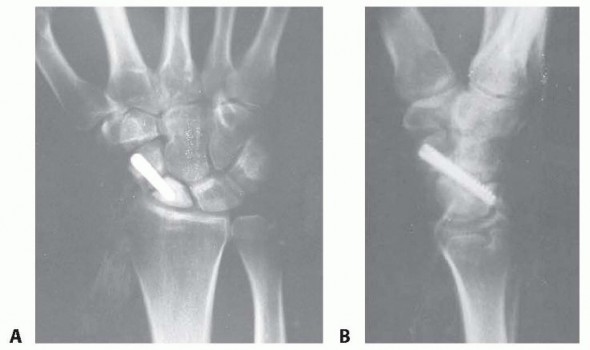
FIG 1 • Failed ORIF of a scaphoid nonunion (PA and lateral views). The scaphoid is mostly covered in articular cartilage and has important intrinsic and extrinsic ligamentous attachments.Most of the vascular supply to the scaphoid enters the bone distal to the waist and perfuses in a retrograde fashion (FIG 2).6,17The proximal pole is most at risk secondary due to its tenuous blood supply.All of these anatomic features make surgical management complex.
PATHOGENESIS
Patients with scaphoid fractures who present with delays (>4 weeks) in both diagnosis and treatment can develop a nonunion. Other risk factors for nonunion include proximal fracture location, comminution, fragment displacement or angulation, and associated carpal instability. As with other fractures, smokers are at increased risk for nonunion.Acute scaphoid fractures with fracture fragment displacement more than 1.0 mm, an intrascaphoid angle more than 45 degrees, or a height-to-length ratio more than 0.65 have a higher incidence of nonunion.18Because the scaphoid serves as a bridge between the proximal and distal carpal rows, a scaphoid fracture can severely disrupt wrist biomechanics and normal loading patterns.Scaphoid fractures disrupt the normal linkage between the two rows, and thus the proximal fragment remains with the lunate via the scapholunate ligament and the distal fragment flexes unimpeded.Scaphoid collapse reduces the carpal height and allows the lunate to rotate in a dorsal intercalated segmental instability (DISI) pattern.Scaphoid nonunion advanced collapse (SNAC) arthritis develops from the altered biomechanics.
NATURAL HISTORY
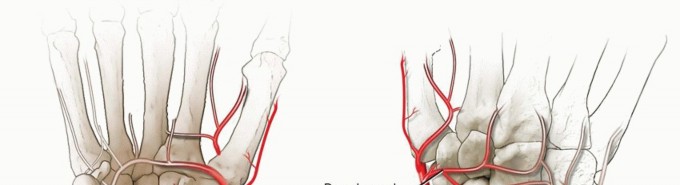
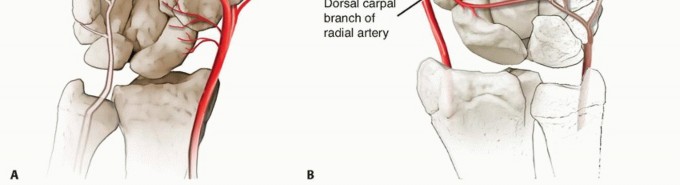
FIG 2 • A. Volar intraosseous blood supply to the scaphoid with laterovolar and distal vessels visualized. B. Dorsal intraosseous blood supply to the scaphoid.Many patients present once pain and decreased range of motion in the wrist has become increasingly severe. In these cases, salvage procedures requiring arthrodesis are often the only options left.
PATIENT HISTORY AND PHYSICAL FINDINGS

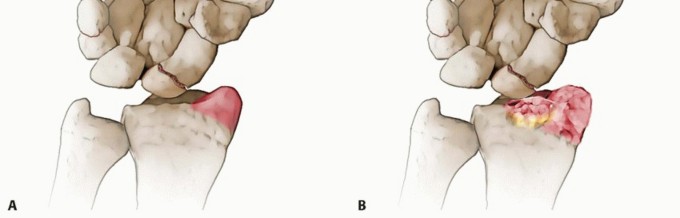
FIG 3 • A. Arthritis observed between the distal pole of the scaphoid and the radial styloid (SNAC grade I).


FIG 3 •(continued)B,C. Stage I SNAC can progress to involve the scaphocapitate articulation (SNAC grade II) with eventual diffuse arthritis in the midcarpal joint (SNAC grade III). Measurements of grip strength and range of motion (ROM) need to be ascertained.Strength is often decreased by as much as 30% to 40% if the patient is experiencing pain.There will often be a decrease in dorsiflexion of the wrist relative to the contralateral unaffected side.
IMAGING AND OTHER DIAGNOSTIC STUDIES

FIG 4 • Chronic nonunion of the scaphoid with SNAC in a patient with no previous treatment. If the radiographs reveal intercarpal arthritis (FIG 5B) or a small avascular proximal pole fragment, partial scaphoid excision may be contraindicated.If minimal radioscaphoid arthritis is observed, ORIF (with nonvascularized or vascularized bone graft) to reconstruct the nonunited scaphoid might be the best option.A magnetic resonance imaging (MRI) is often ordered by physicians in the management of scaphoid nonunions to evaluate the blood supply of the proximal pole. However, these studies have little influence in patients who are candidates for a distal fragment excision.From a radiographic perspective, the ideal candidate for distal pole excision of the scaphoid has a nonunion of the scaphoid fracture at the level of the waist or distal pole with concomitant degenerative joint disease between the distal radius and distal pole only (SNAC stage I).
DIFFERENTIAL DIAGNOSIS
Acute scaphoid fractureFirst or second extensor compartment tendonitis Scapholunate ligament injuryBasilar thumb arthritis Scaphotrapeziotrapezoid arthritis Inflammatory arthritis
NONOPERATIVE MANAGEMENT
Nonoperative management of chronic wrist pain should always be considered in discussion with patients about treatment options. The symptoms may be months or even years old, so there is little rush to intervene if the patient desires further delay.The treatment of any painful joint begins with intermittent immobilization (wrist splinting), activity modification, and nonsteroidal anti-inflammatory drugs (NSAIDs).If immobilization and NSAIDs are ineffective, temporary pain relief can almost always be gained with a steroid injection. These temporizing treatments also put the pain in perspective for the patient. The patient may conclude that medication and splinting is all that is necessary.During the nonoperative management period, the surgeon gains a perspective on the degree of patient discomfort and simultaneously gauges the patient's expectations.The operation will work better and the patient will be more satisfied if the patient's and surgeon's expectations are similar.
SURGICAL MANAGEMENT

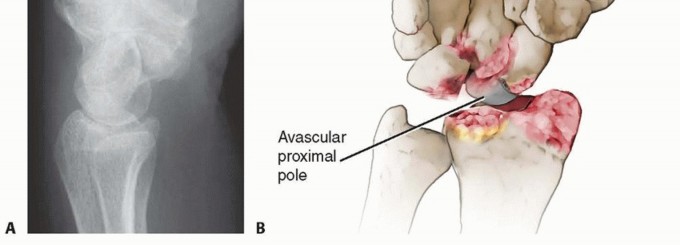
FIG 5 • A. Lateral plain radiograph displaying a DISI deformity. B. When intercarpal arthritis (SNAC grade III) or an avascular proximal pole is found, partial scaphoid excision may be contraindicated. A patient with an untreated scaphoid nonunion and no arthritis is best treated by ORIF of the scaphoid with bone grafting. In a patient with SNAC wrist stage II, it is too late for a distal pole excision; this patient may require a proximal row carpectomy or scaphoid excision with intercarpal fusion.Most patients requiring excision of the distal pole have undergone prior treatment that has failed, and both the surgeon and the patient are searching for a reliable procedure with low morbidity to help alleviate the patient's pain and improve function.Distal scaphoid excision requires robust and taut radioscaphocapitate and long radiolunate ligaments in order to support the remaining proximal carpus and prevent collapse (DISI) of the wrist.Contraindications to distal pole excision include the following:Preexisting significant DISI deformity. The DISI deformity may indeed get worse with distal pole excision in an individual with poor ligamentous support.Proximal pole that is less than half the entire size of the scaphoid. If the distal fragment is greater than 50% of the size of the scaphoid, resultant collapse of the carpus may occur with severe morbidity.
PREOPERATIVE PLANNING
Preoperative planning is done based on a thorough review of the patient's plain radiographs.If the distal pole is to be excised, there must be enough proximal pole (>½) left to support the distal row of the carpus. If only a very small (and possibly an avascular) proximal pole remains, the carpus is likely tocollapse, resulting in failure of the procedure.
POSITIONING
The patient is placed in the supine position with the extremity on an arm board. A proximal arm pneumatic tourniquet is applied.
APPROACH
The distal pole of the scaphoid can be excised through either a dorsal or palmar approach. The approach may be dictated by existing scars.The palmar approach is the preferred method due to the relatively accessible palmar position of the distal fragment.An advantage of the dorsal approach is the ease of excision of the posterior interosseous nerve for wrist denervation.A radial styloidectomy can be performed through either approach.P.365
TECHNIQUES
Volar Approach for Excision of the Distal Scaphoid Fragment
Volar Approach for Excision of the Distal Scaphoid Fragment
INCISION AND SCAPHOID EXCISION
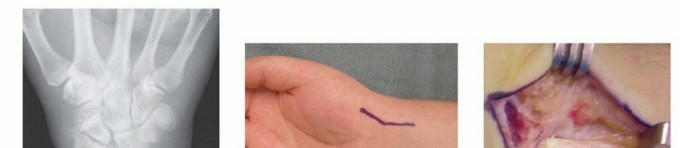



TECH FIG 1 • A. Chronic scaphoid nonunion with SNAC. The patient had no previous treatment. B. An incision is made directly over the FCR tendon. C. The tendon is retracted and its subsheath opened longitudinally. D. The radiocarpal joint is opened longitudinally and the scaphoid is visualized. E,F. The distal pole of the scaphoid is excised with osteotomes and rongeurs. If indicated, a radial styloidectomy can be performed at this point. G. Excised distal pole of the scaphoid.
RADIAL STYLOIDECTOMY
If indicated, an oblique radial styloidectomy can be performed at this point using an osteotome.In this situation, the distal pole may be too large to excise and a radial styloidectomy can accomplish the same purpose.The styloidectomy should be large enough so that the arthritic distal pole no longer touches the radius in radial deviation but not so large as to disrupt the origin of the radioscapholunate ligament, as this may preclude later proximal row carpectomy.
WOUND CLOSURE

TECH FIG 2 • An incision over the dorsoradial aspect of the wrist may be used when prior surgery has been performed.
PEARLS AND PITFALLS

P.367
POSTOPERATIVE CARE
Patients are immobilized for 2 weeks in a well-padded volar splint. The splint and sutures are removed 2 weeks after the procedure.A removable orthosis is applied and the patient is instructed on active and passive ROM exercises.Once active and passive ROM has been achieved, strength exercises are started (usually at 4 weeks postoperatively).Regaining full ROM and strength typically takes about 3 months.Pain relief is noticeable within 2 to 4 weeks of surgery.
OUTCOMES
Review of outcomes in the literature suggest that both ROM and grip strength improve postoperatively.3,4,5Pain relief can be expected if the proper indications for surgery are followed.All patients have some degree of DISI preoperatively, and this pattern of deformity may worsen after excision of the distal pole of the scaphoid. DISI deformities that are severe can result in both loss ofmotion and pain. This problem is not well documented in the literature but certainly exists.5In the patient undergoing multiple procedures, outcomes of distal pole excision are better than attempting another bone graft and internal fixation, where the failure rate can approach 50%.1
COMPLICATIONS
The presence of midcarpal arthritis undiagnosed before distal pole excision can lead to persistent pain. Resection of too large a distal pole (>50%) can result in collapse of the scaphoid.If the procedure is performed in a very loose-jointed individual, the DISI pattern may significantly worsen, leading to persistent pain.
REFERENCES
- Bishop AT. Vascularized bone grafts. In: Green DG, Hotchkiss R, Pederson W, eds. Green's Operative Hand Surgery. New York: Churchill Livingstone, 1999.
- Chang MA, Bishop AT, Moran SL, et al. The outcomes and complications of 1,2 intercompartmental supraretinacular artery pedicled vascularized bone grafting of scaphoid nonunions. J Hand Surg Am 2006;31(3):387-396.
- Dias JJ, Wildin CJ, Bhowal B, et al. Should acute scaphoid fractures be fixed? A randomized controlled trial. J Bone Joint Surg Am 2005;87(10):2160-2168.
- Drac P, Manak P, Pieranova L. Distal scaphoid resection arthroplasty for scaphoid nonunion with radioscaphoid arthritis. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2006;150: 143-145.
- Duckworth AD, Jenkins PJ, Aitken SA, et al. Scaphoid fracture epidemiology. J Trauma Acute Care Surg 2012;72(2):E41-E45.
- Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5(5):508-513.
- Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg 1999;33:423-426.
- Kerluke L, McCabe SJ. Nonunion of the scaphoid: a critical analysis of recent natural history studies. J Hand Surg Am 1993;18:1-3.
- Kuschner SH, Lane CS, Brien WW, et al. Scaphoid fractures and scaphoid nonunion. Diagnosis and treatment. Orthop Rev 1994; 23:861-871.
- Lindström G, Nyström A. Natural history of scaphoid non-union, with special reference to “asymptomatic” cases. J Hand Surg Br 1992;17:697-700.
- Malerich MM, Clifford J, Eaton B, et al. Distal scaphoid resection arthroplasty for the treatment ofdegenerative arthritis secondary to scaphoid nonunion. J Hand Surg Am 1999;24:1196-1205.
- Merrell GA, Wolfe SW, Slade JF III. Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am 2002;27(4):685-691.
- Peimer CA, Medige J, Eckert BS, et al. Reactive synovitis after silicone arthroplasty. J Hand Surg Am 1986;11:624-638.
- Ruby LK, Stinson J, Belsky MR. The natural history of scaphoid non-union: a review of 55 cases. J Bone Joint Surg Am 1985;67: 428-432.
- Ruch DS, Papadonikolakis A. Resection of the scaphoid distal pole for symptomatic scaphoid nonunion after failed previous surgical treatment. J Hand Surg Am 2006;31:588-593.
- Smith BS, Cooney WP. Revision of failed bone grafting for nonunion of the scaphoid. Treatment options and results. Clin Orthop Relat Res 1996;(327):98-109.
- Taleisnik J, Kelly PJ. The extraosseous and intraosseous blood supply of the scaphoid bone. J Bone Joint Surg Am 1966;48:1125-1137.
- Trumble TE, Salas P, Barthel T, et al. Management of scaphoid nonunions. J Am Acad Orthop Surg 2003;11:380-391.
