BIOMECHANICAL RATIONALE FOR MENISCAL PRESERVATION
The paradigm of meniscal surgery has shifted dramatically from routine total meniscectomy to aggressive meniscal preservation. The menisci serve critical biomechanical functions within the knee, including load transmission, shock absorption, joint stability, proprioception, and articular cartilage lubrication.
The lateral meniscus bears approximately 70% of the weight in the lateral compartment, whereas the medial meniscus bears 50% of the weight in the medial compartment. Consequently, partial or total lateral meniscectomies historically yield significantly worse long-term clinical outcomes than their medial counterparts. Fairbanks changes (radiographic signs of osteoarthritis) are noted to be seven times more frequent following partial or total meniscectomy compared to successful meniscal repair. Joint deterioration is further accelerated in the presence of concomitant pathologies, such as grade II or III anterior cruciate ligament (ACL) instability, tibiofemoral malalignment, or pre-existing femoral and tibial chondromalacia. Therefore, the overarching goal of modern operative orthopaedics is to preserve as much functional meniscal tissue as possible.
PARTIAL EXCISION OF THE DISCOID MENISCUS
A discoid meniscus is a congenital morphological variant, most commonly affecting the lateral meniscus, characterized by a thickened, disc-like shape that covers a larger-than-normal area of the tibial plateau. Because of its abnormal microarchitecture and poor peripheral vascularity, it is highly susceptible to tearing.
The primary surgical objective of partial excision of a symptomatic torn discoid meniscus is to resect the central anomalous portion, leaving a balanced, stable peripheral rim approximately the width of a normal lateral meniscus (6 to 8 mm). However, the exact width of the preserved rim is ultimately dictated by the location and extent of the tear within the meniscal body.
Diagnostic Arthroscopy and Identification
Surgical Pitfall: During systematic diagnostic arthroscopy of the lateral compartment, a discoid lateral meniscus may be easily missed. Because the tibial plateau may be completely covered by the anomalous meniscus, the lateral compartment may falsely appear to be devoid of a lateral meniscus altogether.
If the free inner edge of the meniscus is not immediately visualized, the surgeon must maintain a high index of suspicion for a discoid variant. Careful exploration should be focused more centrally in the lateral compartment, or medially near the intercondylar eminence, to locate the displaced or continuous meniscal edge.
Surgical Setup and Instrumentation
- Pediatric and Small Patients: In young patients with small knees, utilize a 2.7-mm arthroscope and appropriately sized small-joint instruments to prevent iatrogenic chondral damage.
- Adult Patients: In older individuals or those with standard-sized joints, utilize a medial midpatellar portal for the arthroscope to achieve a superior panoramic view of the lateral compartment. Standard anteromedial and anterolateral portals are established for instrumentation.
Step-by-Step Surgical Technique
- Visualization and Planning: With direct vision of the discoid meniscus, carefully plan the resection trajectory. The goal is to ensure that a healthy peripheral meniscal rim of approximately 6 to 8 mm in width remains.
- Positioning: Place the operative knee in a "figure-four" position to open the lateral compartment and apply a varus stress.
- Central Resection: Introduce a rotary basket forceps through the working portal to initiate the central resection of the discoid tissue.
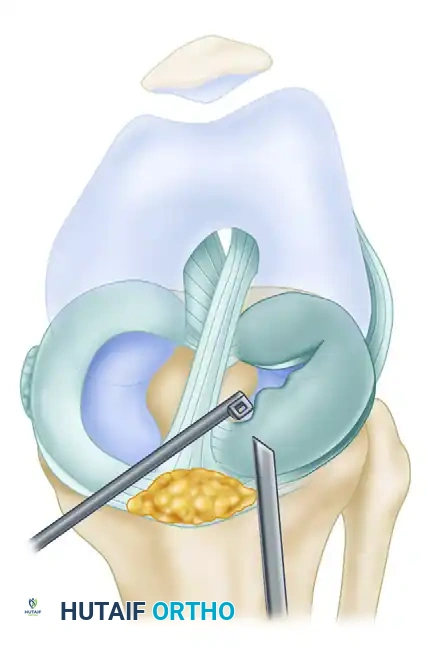
Figure 51-20A: The anterior portion of the discoid lateral meniscus is systematically removed using a rotary basket forceps.
- Contouring the Anterior Rim: Continue to resect the bulk of the central tissue, moving anteriorly.
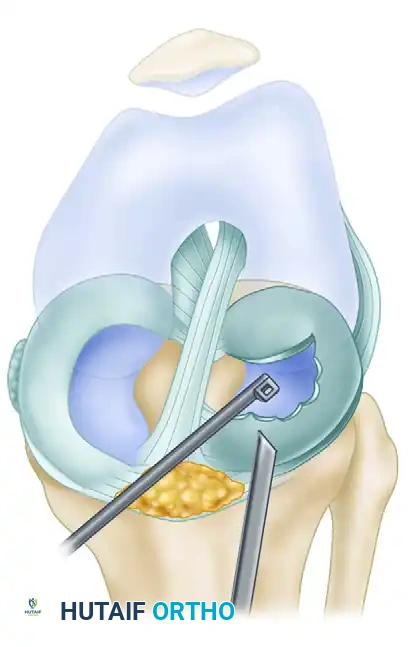
Figure 51-20B: Further contouring of the anterior meniscal rim is achieved with a 90-degree rotary basket forceps.
- Posterior Resection: Once the central bulk has been resected, place arthroscopic scissors through the anterolateral portal. Make a posterior, radially directed cut extending outward to the planned 8-mm mark of the peripheral meniscal tissue.
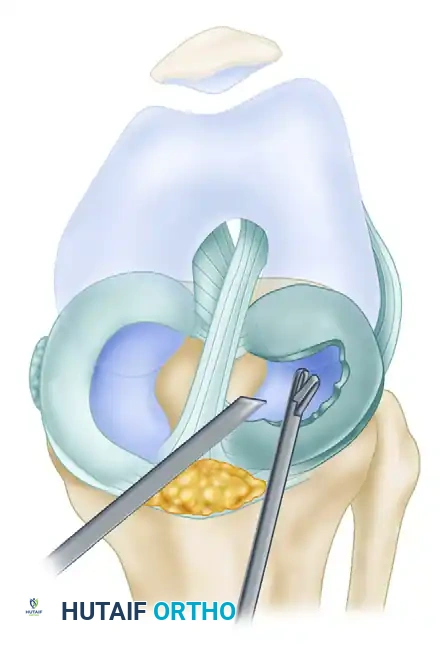
Figure 51-20C: The posterior discoid fragment is carefully excised and removed with basket forceps.
- Anterior Semicircular Cut: From a lateral peripatellar portal, introduce a curved arthroscopic knife into the outer extent of the radial cut. Direct the incision anteriorly in a semicircular manner, meticulously preserving the 6 to 8 mm peripheral rim. Complete the cut by alternating the knife or scissors to the medial portal as needed for optimal trajectory.
- Final Balancing: Ensure the remaining rim is balanced and stable. Note that the thickness of the inner edge of a reshaped discoid meniscus is inherently much greater than the inner edge following a routine partial meniscectomy.
- Joint Lavage: Thoroughly lavage and suction the joint to remove all microscopic meniscal debris, which can act as a mechanical irritant postoperatively.
BALANCING MENISCAL RESECTIONS
When performing any partial meniscectomy, achieving a smoothly contoured, balanced rim is critical to prevent focal stress risers that can lead to propagation of new tears. The resection strategy varies based on the tear morphology.
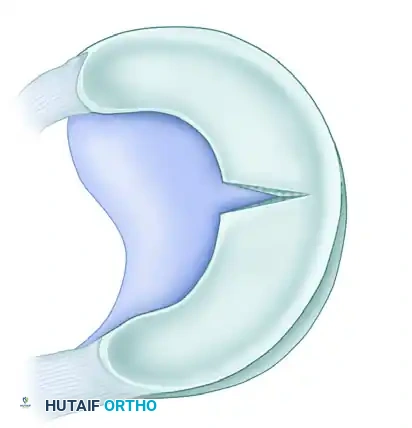
Figure 51-19A: Balancing a meniscal resection in the presence of a radial tear.

Detail: Radial tear contouring requires a smooth transition zone to dissipate hoop stresses.

Figure 51-19B: Balancing a meniscal resection in the presence of a longitudinal tear.
Detail: Longitudinal tear resection requires excision of the unstable inner leaf while preserving the stable peripheral rim.
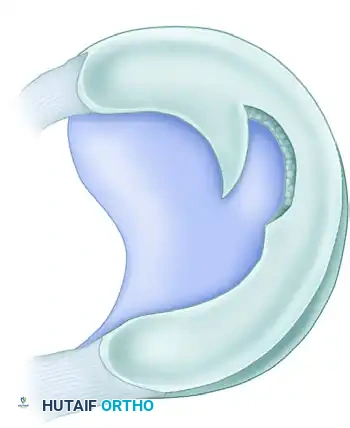
Figure 51-19C: Balancing a meniscal resection in the presence of a complex flap tear.
ARTHROSCOPIC MANAGEMENT OF MENISCAL CYSTS
Meniscal cysts typically develop secondary to chronic degenerative meniscal tears, most frequently involving the lateral meniscus. The cyst forms as synovial fluid is forced through a horizontal cleavage tear into the parameniscal soft tissues, acting as a one-way valve.
Surgical Decompression Technique
- Intraarticular Identification: The site of the cyst can usually be differentiated intraarticularly by probing the meniscal tear fragments.
- Opening the Split: Open the horizontal split in the meniscus using a small curved curet. Pass the curet directly through the meniscal body into the central portion of the parameniscal cyst.
- Decompression: Curette the cyst lining. Apply external digital palpation and pressure over the cyst on the lateral aspect of the knee to free up the cyst and decompress its mucinous contents directly into the joint.
- Evacuation: Utilize arthroscopic suction to thoroughly remove the extruded cyst contents.
- Meniscal Resection: Resect the unstable meniscal fragments associated with the horizontal cleavage tear, contouring the tissue back to a relatively stable, healthy meniscal rim.
Clinical Pearl: Good to excellent results are consistently reported with arthroscopic partial meniscectomy combined with intraarticular cyst decompression. If the cyst decompresses fully during the meniscectomy, no further treatment is required. If it does not spontaneously decompress, it can be percutaneously aspirated. Open excision of a meniscal cyst is rarely, if ever, indicated in modern practice.
ARTHROSCOPIC REPAIR OF TORN MENISCI
While partial meniscectomy yields functionally superior results compared to total meniscectomy, the ultimate long-term outcome remains suboptimal due to the loss of hoop stress distribution. Therefore, meniscal repair is the gold standard for amenable tears.
Currently, only 10% to 15% of all meniscal tears are deemed repairable. These are most frequently associated with acute anterior cruciate ligament (ACL) injuries.
Factors Influencing Meniscal Healing
- Peripheral Rim Width: Positive correlations with healing are strongly associated with a narrow peripheral meniscal rim (< 4 mm), placing the tear in the highly vascularized red-red or red-white zones.
- Chronicity: Repairs performed within 8 weeks of the initial injury demonstrate significantly higher healing rates.
- Tear Length: Tears greater than 4 cm in length have a higher failure rate. In a study by Cannon, repairs in tears > 4 cm failed to heal 58% of the time, independent of patient age.
- Biological Augmentation: The addition of an exogenous fibrin clot significantly increases healing rates. Henning noted that the healing rate in 950 lateral meniscal repairs increased from 59% to 90% with the addition of a fibrin clot.
Tear Classification and Repair Indications
Tears evaluated during arthroscopy can be categorized into four distinct treatment pathways:
- Tears that can be rasped and left alone: Peripheral tears of 7 mm or less heal without suture stabilization. These should be probed to ensure less than 3 mm of displacement. The tear and the adjacent meniscal synovium should be aggressively rasped to promote a localized inflammatory healing response.
- Tears that definitely can be repaired: Single vertical longitudinal tears located in the peripheral vascular portion (the red-red zone at the meniscosynovial junction, or the red-white zone within 3 mm of the junction). These tears are displaceable, > 1 cm long, and involve minimal damage to the meniscal body. Repair is generally highly successful in patients under 40 years of age.
- Tears that can be repaired under certain circumstances: Tears located 3 to 5 mm from the meniscosynovial junction. These must be evaluated with the surgical tourniquet deflated to accurately assess tissue vascularity. In young, active patients with minimal body damage, suture repair combined with healing enhancement (e.g., fibrin clot, trephination) is recommended.
- Tears that should be resected: Resection is mandatory for a meniscus with multiple complex tears, tears involving severe plastic deformation of the body, and tears located definitively in the avascular (white-white) zone.
Surgical Warning regarding Radial Tears: Complete radial tears present a perplexing biomechanical problem. When they extend into the meniscal body, they completely disrupt the circumferential collagen fibers, destroying the meniscus's ability to dissipate hoop stresses. While radial tears near the posterior horn root can heal with repair, their biomechanical functionality remains in doubt. However, in young patients, the long-term results of a meticulous repair are still considered superior to a subtotal meniscectomy.
Biological Enhancement Techniques
Regardless of the suture technique utilized, biological enhancement is critical for success:
- Tear Débridement: The tear edges must be debrided of fibrous scar tissue.
- Synovial Abrasion: Local synovial, meniscal, and capsular abrasion (rasping) stimulates a proliferative fibroblastic healing response.
- Vascular Access Channels (Trephination): Using an 18-gauge spinal needle to penetrate the peripheral meniscus through to the vascular synovium creates channels that stimulate bleeding and cellular migration into the tear site.
- Fibrin Clot: Highly recommended for isolated meniscal repairs (without concomitant ACL reconstruction) to provide a chemotactic and mitogenic scaffold.
Arthroscopic Repair Techniques
Arthroscopic repair techniques are divided into four primary categories. The choice of technique depends heavily on the anatomical location of the tear.
1. Inside-Out Repair
Considered the gold standard for posterior horn and middle-third tears, as well as displaced bucket-handle tears. It utilizes double-lumen or single-lumen zone-specific cannulas to pass long flexible needles from the intraarticular space out through the joint capsule.
Safety Requirement: This technique is rendered safe only with the use of a dedicated accessory incision for capsular exposure and the placement of specialized retractors (e.g., a popliteal retractor) to protect the posterior neurovascular structures during needle retrieval.
2. Outside-In Repair
Described by Morgan, Casscells, and Johnson, this technique is most suitable for repairs of the anterior horn and the anterior portion of the middle third of the meniscus. Needles are passed from the outside of the knee, through the capsule, and into the meniscus, followed by suture shuttling.
3. All-Inside Repair
Rapidly evolving due to the development of advanced suture fixators with pre-tied, sliding-locking knots. These devices provide secure biomechanical fixation while decreasing the potential for the iatrogenic chondral injury seen with earlier rigid implants. They are best utilized for securing tears that are 2 to 4 mm from the peripheral attachment, particularly in the posterior horn.
4. Hybrid Repair
Complex tear patterns often require a combination of techniques. For example, if a large bucket-handle tear of the medial meniscus is suitable for repair:
- An initial stabilizing horizontal mattress suture can be inserted using an inside-out cannula technique at the midpoint of the tear near the posteromedial corner.
- Additional posterior sutures can be placed using an all-inside suture-based fixation device.
- The anterior extension of the tear is then secured using an outside-to-inside needle technique.
Concomitant Ligamentous Reconstruction
If a patient presents with an unstable knee caused by an anterior cruciate ligament (ACL) deficiency alongside a repairable meniscal lesion, the ligament reconstruction and the meniscal repair must be performed concurrently. The hemarthrosis and bone marrow elements released during the creation of ACL bone tunnels provide a highly favorable biological environment that significantly increases the healing rates of the repaired meniscus.
POSTOPERATIVE CARE AND REHABILITATION
Postoperative rehabilitation following meniscal surgery is dictated by whether a resection or a repair was performed.
Following Partial Meniscectomy / Discoid Excision:
Patients are generally allowed immediate weight-bearing as tolerated with crutches. Range of motion (ROM) exercises are initiated immediately to prevent arthrofibrosis. Return to sports is typically permitted once full, painless ROM and baseline quadriceps strength are restored (usually 4 to 6 weeks).
Following Meniscal Repair:
Rehabilitation must be carefully phased to protect the healing meniscal tissue from excessive shear and compressive forces.
- Weight-Bearing: Restricted to partial or non-weight-bearing in full extension for the first 4 to 6 weeks.
- Range of Motion: Flexion is typically limited to 90 degrees for the first 4 weeks to prevent excessive posterior translation and shear stress on the repaired posterior horn.
- Return to Play: Deep squatting, pivoting, and high-impact activities are strictly prohibited for a minimum of 4 to 6 months to ensure complete biological integration of the repair site.
