INTRODUCTION TO PARONYCHIA
Paronychia, colloquially referred to in its advanced stages as a “runaround” infection, represents the most frequently encountered bacterial infection of the hand. It is characterized by an acute or chronic inflammatory process involving the soft tissue folds surrounding the fingernail, specifically the eponychium and paronychium. Acute paronychia is typically a localized, purulent bacterial infection, whereas chronic paronychia is increasingly recognized as a multifactorial inflammatory dermatosis often exacerbated by environmental exposure and secondary fungal colonization.
For the practicing orthopedic surgeon and hand specialist, mastering the surgical management of paronychia requires a profound understanding of perionychial anatomy, precise surgical technique to avoid iatrogenic nail dystrophy, and the clinical acumen to differentiate bacterial abscesses from viral etiologies that strictly contraindicate surgical intervention.
SURGICAL ANATOMY OF THE PERIONYCHIUM
A rigorous understanding of the nail unit's anatomy is paramount before undertaking any surgical intervention in this region. The perionychium comprises the nail bed and the surrounding soft tissues (paronychium, eponychium, and hyponychium).
- Nail Plate: The keratinized structure providing dorsal protection to the distal phalanx.
- Eponychium: The proximal soft tissue fold overlying the base of the nail plate.
- Paronychium: The lateral soft tissue folds bordering the nail plate.
- Germinal Matrix (Ventral Floor): Located proximally beneath the eponychium, extending to the lunula. It is responsible for generating approximately 90% of the nail plate's volume. Iatrogenic injury to the germinal matrix will result in permanent nail ridging or absent nail growth.
- Sterile Matrix (Nail Bed): Extends from the lunula to the hyponychium. It provides adherence for the nail plate and contributes slightly to its thickness.
- Dorsal Roof: The undersurface of the eponychial fold, which imparts the smooth dorsal sheen to the growing nail plate.
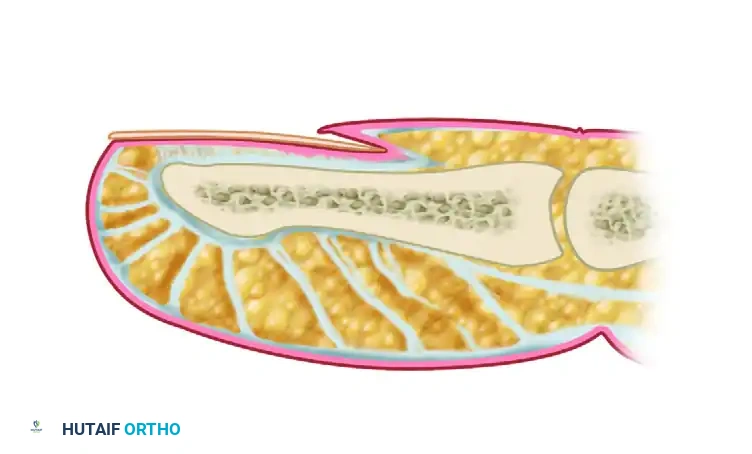
FIGURE 78-1: Diagram of the nail and nail bed anatomy. A, Nail plate. B, Eponychium. C, Dorsal roof of the nail fold. D, Ventral floor of the nail fold (germinal matrix). E, Nail bed (sterile matrix).
PATHOPHYSIOLOGY AND MICROBIOLOGY
Acute paronychia is almost universally precipitated by minor local trauma—such as a hangnail, aggressive manicuring, nail-biting (onychophagia), or a puncture wound—which compromises the protective seal between the nail plate and the eponychium.
This mechanical breach facilitates the inoculation of pathogenic bacteria into the closed perionychial space. Staphylococcus aureus is the most common causative organism, followed by Streptococcus pyogenes. In patients with a history of nail-biting or finger-sucking, mixed infections involving oral flora, including anaerobic bacteria (e.g., Bacteroides, Fusobacterium) and Eikenella corrodens, must be anticipated.
The "Runaround" Infection
The infection typically originates at one corner of the horny nail fold. If left untreated, the purulent exudate dissects along the path of least resistance. It travels proximally under the eponychium or beneath the proximal nail plate, migrating toward the contralateral paronychial fold. This circumferential spread around the base of the nail is classically termed a "runaround" infection.
CLINICAL EVALUATION AND DIFFERENTIAL DIAGNOSIS
Patients typically present with acute onset of throbbing pain, erythema, edema, and localized tenderness along the lateral or proximal nail folds. As the infection progresses, a visible collection of purulence (fluctuance) may become apparent beneath the eponychium or the lateral nail fold.
🚨 SURGICAL WARNING: Herpetic Whitlow
The most critical differential diagnosis is Herpetic Whitlow, an infection caused by Herpes Simplex Virus (HSV) type 1 or 2. Misdiagnosing herpetic whitlow as a bacterial paronychia and proceeding with surgical incision and drainage is a severe clinical error that can lead to viral dissemination, secondary bacterial superinfection, and delayed healing.
Clinical Pearls for Differentiating Herpetic Whitlow:
* Demographics: Disproportionately affects healthcare workers (dental hygienists, respiratory therapists) and immunocompromised patients. Also seen in children with herpetic gingivostomatitis.
* Presentation: Begins as a localized area of disproportionate pain and swelling, rapidly followed by the eruption of clear, coalescing vesicles.
* Systemic Signs: Lymphangitis and epitrochlear/axillary lymphadenopathy are frequently present.
* Diagnostics: Diagnosis is confirmed via viral cultures of vesicular fluid, a Tzanck smear (revealing multinucleated giant cells), or serum HSV antibody titers.
* Management: Strictly self-limited. Resolves over 3 to 4 weeks. Surgical treatment is absolutely contraindicated. Management consists of dry dressings to prevent transmission and, in severe cases, oral antivirals (e.g., acyclovir, valacyclovir).
INDICATIONS FOR SURGICAL INTERVENTION
Early, non-fluctuant paronychia (cellulitis phase) can often be managed conservatively with warm water or chlorhexidine soaks, elevation, and oral antistaphylococcal antibiotics.
Surgical Indications include:
1. Presence of a visible abscess or fluctuance.
2. Failure to improve after 48 hours of appropriate conservative management.
3. Extension of the infection beneath the nail plate (subungual abscess).
4. Development of a "runaround" infection.
OPERATIVE TECHNIQUES: INCISION AND DRAINAGE
The surgical approach is dictated by the extent of the abscess. The primary goal is to achieve complete evacuation of purulence while meticulously preserving the germinal matrix.
Preoperative Preparation
- Anesthesia: A digital block using 1% or 2% lidocaine without epinephrine is administered at the base of the digit. Ensure adequate time is allowed for the block to take full effect.
- Hemostasis: A sterile finger tourniquet (e.g., a Penrose drain or a commercial digital tourniquet) is applied to the base of the digit to provide a bloodless surgical field, which is critical for visualizing the delicate matrix tissues.
- Preparation: Standard surgical skin preparation with chlorhexidine or povidone-iodine.
Technique 1: Simple Unilateral Paronychia
If the abscess is confined to one lateral paronychial fold and has not extended beneath the nail plate or across the eponychium:
- Use a #11 or #15 scalpel blade.
- Make a longitudinal incision directly over the point of maximal fluctuance in the lateral fold.
- Crucial Biomechanical Step: Angle the blade away from the nail plate and nail bed during the incision. Directing the blade toward the nail bed risks lacerating the sterile or germinal matrix, which will inevitably cause a permanent longitudinal ridge or split in the growing nail.

FIGURE 78-2: Incision placement for a simple unilateral paronychia. Note the trajectory of the blade angled away from the nail bed to prevent iatrogenic matrix injury.
Technique 2: Complex or "Runaround" Paronychia
If the abscess has migrated to the opposite side, involves the entire eponychium, or extends under the proximal nail root, a more extensive approach is required.
- Bilateral Incisions: Make two longitudinal incisions at the junction of the lateral nail folds and the eponychium, extending proximally.
- Eponychial Elevation: Carefully elevate the eponychial fold proximally. This exposes the proximal third of the nail plate and the underlying abscess cavity. A Freer elevator or the blunt end of a scalpel handle can be used to gently separate the dorsal roof of the eponychium from the nail plate.
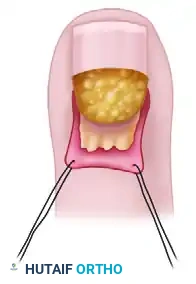
Elevation of the eponychial fold following bilateral incisions, exposing the proximal nail plate and the underlying purulent collection.
- Partial Nail Plate Excision: If purulence has tracked beneath the proximal nail plate, the proximal one-third of the nail must be excised to ensure adequate drainage.
- Insert the flat blade of straight Iris scissors or a small periosteal elevator beneath the proximal nail plate to separate it from the underlying germinal matrix.
- Cut across the nail plate transversely and remove the proximal portion. Do not disturb the distal two-thirds of the nail plate if it remains firmly adherent to the sterile matrix, as it provides protection to the sensitive nail bed during healing.
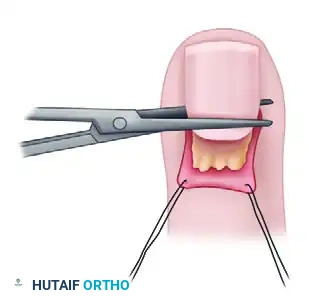
Excision of the proximal one-third of the nail plate using straight scissors. The instrument is carefully passed between the nail plate and the germinal matrix.
Technique 3: Wound Packing and Drainage
Following thorough irrigation of the abscess cavity with sterile saline:
- The eponychial fold must be kept elevated to prevent premature closure and re-accumulation of purulence.
- Loosely pack the cavity under the eponychial fold with a small strip of iodoform gauze or plain fine-mesh gauze.
- The packing should be placed gently; tight packing can cause pressure necrosis of the delicate germinal matrix.

The wound is loosely packed with iodoform gauze placed beneath the elevated eponychial fold to facilitate continuous drainage for the first 48 hours.
MANAGEMENT OF CHRONIC PARONYCHIA
Chronic paronychia is defined as inflammation of the perionychium lasting longer than 6 weeks. Unlike acute paronychia, it is rarely a primary bacterial abscess. Current evidence suggests that in up to 45% of cases, chronic paronychia is primarily a contact dermatitis or inflammatory reaction related to environmental exposure (e.g., dishwashers, bartenders, cleaners exposed to harsh chemicals or chronic moisture). Secondary colonization with Candida albicans or mixed bacterial flora is common but is a consequence, rather than the primary cause, of the disease.
Clinical Presentation
Patients present with indurated, thickened, and erythematous eponychial folds. The cuticle is typically absent, leaving a gap between the proximal nail fold and the nail plate. The nail plate itself often becomes dystrophic, discolored, and transversely ridged.
Surgical Management: Eponychial Marsupialization
When prolonged conservative management (strict avoidance of moisture/irritants, topical corticosteroids, and topical antifungals) fails, surgical intervention is warranted.
Surgical Technique: Eponychial Marsupialization
1. Under digital block anesthesia and tourniquet control, a crescent-shaped incision is made dorsal to the eponychial fold.
2. The maximum width of the excised crescent should be approximately 3 to 5 mm, located 1 to 2 mm proximal to the distal edge of the eponychium.
3. The excision removes the thickened, fibrotic skin and subcutaneous tissue down to, but strictly avoiding, the germinal matrix.
4. If the nail plate is severely dystrophic, it may be removed entirely.
5. The wound is left open to heal by secondary intention. Epithelialization typically occurs over 2 to 3 weeks, resulting in a newly formed, healthy eponychial fold.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Optimal postoperative care is essential to prevent recurrence and ensure the return of normal digit function.
- Postoperative Day 0-2: The digit is dressed in a bulky, non-compressive dressing. The hand should be kept elevated above heart level to minimize edema and throbbing pain.
- Postoperative Day 2 (48 Hours): The initial dressing and the iodoform gauze packing are removed. This can be facilitated by soaking the hand in warm water or saline to minimize discomfort and tissue trauma during removal.
- Postoperative Day 3-10: The patient is instructed to perform warm water soaks (often mixed with mild antibacterial soap or chlorhexidine) for 15 minutes, 3 to 4 times daily. Following each soak, a light, dry dressing is applied.
- Rehabilitation: Active range of motion (AROM) exercises of the distal interphalangeal (DIP) joint are encouraged immediately following packing removal to prevent extensor tendon adhesions and joint stiffness.
- Antibiotics: Postoperative oral antibiotics are generally only required if there is associated severe cellulitis, lymphangitis, or if the patient is immunocompromised.
COMPLICATIONS AND PITFALLS
While incision and drainage of a paronychia is a common procedure, technical errors can lead to significant morbidity:
- Nail Dystrophy: The most common iatrogenic complication. Caused by directing the scalpel blade into the germinal or sterile matrix during incision, or by overly aggressive scraping of the matrix during debridement.
- Recurrence: Usually results from inadequate drainage, failure to remove the proximal nail plate in a runaround infection, or premature closure of the eponychial fold due to inadequate packing.
- Osteomyelitis: Prolonged, untreated paronychia can lead to contiguous spread of infection to the distal phalanx, necessitating bone debridement and prolonged intravenous antibiotics.
- Flexor Tenosynovitis: Rare, but aggressive infections can track volarly into the digital pulp (causing a felon) and subsequently into the flexor tendon sheath, representing a surgical emergency.
📚 Medical References
- paronychia, J Hand Surg 16A:314, 1991.
- Behr JT, Daluga DJ, Light TR, et al: Herpetic infections in the fi ngers of infants: report of fi ve cases, J Bone Joint Surg 69A:137, 1987.
- Belsole R, Fenske N: Cutaneous larva migrans in the upper extremity, J Hand Surg 5:178, 1980.
- Bhatty MA, Turner DP, Chamberlain ST: Mycobacterium marinum hand infection: case reports and review of literature, Br J Plast Surg 53:161, 2000.
- Birkinshaw R, O’Donnell J, Sammy I: Necrotizing fasciitis as a complication of steroid injection, J Acad Emerg Med 14:52, 1997.
- Blue ML, Payne WG, Mannari RI, et al: Mycobacterium kansasii causing
