Introduction & Epidemiology
Fracture management represents a cornerstone of orthopedic practice, demanding a comprehensive understanding of injury mechanisms, anatomical considerations, and therapeutic principles. Accurate and swift diagnosis is paramount, directly influencing patient outcomes, minimizing morbidity, and preventing long-term disability. The global incidence of fractures is substantial, with estimates suggesting millions of new fractures annually, imposing a significant socioeconomic burden. The etiology ranges from low-energy falls in osteoporotic individuals to high-energy polytrauma sustained in motor vehicle collisions or industrial accidents. Understanding the "point of impact" and the vector of applied forces is not merely an academic exercise; it is a critical diagnostic tool that informs the potential fracture pattern, associated soft tissue injuries, and guides both immediate resuscitative efforts and definitive surgical planning. This detailed understanding allows for a more targeted clinical assessment, optimization of imaging modalities, and anticipatory management of potential complications.
Surgical Anatomy & Biomechanics
A thorough understanding of surgical anatomy and bone biomechanics is indispensable for diagnosing and treating fractures. Bone is a dynamic, anisotropic, and viscoelastic material, capable of resisting significant loads, yet susceptible to failure when stresses exceed its intrinsic strength. The pattern of bone failure—and thus the fracture configuration—is directly dictated by the magnitude, direction, and rate of applied forces, as well as the inherent properties of the bone itself (e.g., cortical thickness, cancellous bone density, pre-existing pathology).
Biomechanical Principles of Fracture Patterns
- Tension: Forces pulling bone apart. Pure tension fractures are rare in long bones but are seen in avulsion injuries where a ligament or tendon pulls a bone fragment away (e.g., patella fracture from quadriceps contraction, medial malleolus avulsion).
- Compression: Forces pushing bone together. This typically results in oblique or transverse fractures in long bones, or impaction and comminution in cancellous bone (e.g., vertebral compression fractures, pilon fractures).
- Bending: A combination of tension on the convex side and compression on the concave side. This often leads to transverse fractures with a triangular butterfly fragment on the compressive side if the force continues.
- Torsion (Twisting): Rotational forces. This commonly produces spiral fractures, characteristic of low-energy rotational injuries. The length and pitch of the spiral indicate the energy involved and the fixation challenges.
- Shear: Forces applied parallel to the surface, causing displacement. Shear forces contribute to oblique fractures and often result in significant displacement when combined with other forces.
The "point of impact" is crucial. A direct blow typically results in a transverse or comminuted fracture at the point of impact. An indirect force, such as a fall onto an outstretched hand (FOOSH), can cause a fracture remote from the point of impact, like a distal radius fracture or even a supracondylar humerus fracture in children, exhibiting bending and compressive forces.
Critical Surgical Anatomy
Specific anatomical considerations are paramount in fracture management:
- Vascularity: Understanding the blood supply to bone (e.g., nutrient artery, periosteal supply) and surrounding soft tissues is critical for preserving bone viability and promoting healing. Fractures that disrupt major vascular bundles (e.g., popliteal artery with distal femur/proximal tibia fractures, brachial artery with supracondylar humerus fractures) constitute orthopedic emergencies.
- Nerve Proximity: Major nerves (e.g., radial nerve with humeral shaft fractures, peroneal nerve with fibular head fractures) can be directly injured at the time of trauma or entrapped during reduction or fixation.
- Muscle Compartments: Awareness of fascial compartments is vital to recognize and manage compartment syndrome, particularly in the tibia, forearm, and foot.
- Joint Surfaces: Intra-articular fractures demand meticulous anatomical reduction to restore joint congruity and prevent post-traumatic arthritis.
- Soft Tissue Envelope: The condition of the surrounding soft tissues (skin, muscle, subcutaneous tissue) directly impacts surgical approach, choice of fixation, and risk of complications like infection and wound dehiscence. Respecting internervous planes during surgical approaches minimizes iatrogenic muscle and nerve damage.
Indications & Contraindications
The decision between operative and non-operative management for fractures hinges on a comprehensive assessment of the fracture pattern, patient factors, and the presence of associated injuries. The goal is to achieve stable anatomical or functional reduction, facilitate healing, restore function, and prevent complications.
How to diagnose a fracture
The diagnostic process begins with a high index of suspicion based on the mechanism of injury and clinical presentation.
1 History
A detailed history is the cornerstone of fracture diagnosis, especially following a traumatic incident. Key points include:
1.
Activity at incident:
What was the patient doing (e.g., sport, driving, working at height)? This helps estimate energy transfer and likely mechanisms.
2.
Nature of incident:
Was it a direct kick, a fall, a twisting injury? This directly correlates with the biomechanical forces applied.
3.
Magnitude of applied forces:
Quantifying the energy involved (e.g., fall height, speed of vehicle, type of impact) is critical. Trivial violence might suggest a pathological fracture. Severe violence necessitates exclusion of multiple injuries and consideration of polytrauma protocols.
4.
Point of impact and direction of applied forces:
This directly predicts the fracture pattern, potential associated soft tissue injuries, and guides the subsequent clinical and radiological examination. For example, a direct anterior impact to the knee suggests patellar or tibial plateau injury, whereas a rotational force might indicate a spiral tibial shaft fracture.
*
Note on original text: "In reducing a fracture, one of the principle methods employed is to redup" - This likely refers to the principle of "reduction," where understanding the original deforming forces helps reverse them to achieve anatomical alignment.
Clinical examination
A systematic clinical examination follows ATLS principles, prioritizing the primary survey (Airway, Breathing, Circulation, Disability, Exposure) for poly-traumatized patients.
*
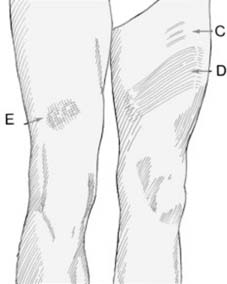
Inspection:
Deformity, swelling, ecchymosis, open wounds (grade according to Gustilo-Anderson classification if applicable).
*
Palpation:
Tenderness, crepitus, abnormal motion.
*
Neurovascular assessment:
Meticulous evaluation of distal pulses, capillary refill, and sensory/motor function. Document pre-reduction neurological status.
*
Associated injuries:
Assess adjacent joints, spinal column, and other body systems. For severe trauma, consider abdominal, thoracic, and head injuries.
Radiological and other visualisation techniques
Imaging confirms the diagnosis, characterizes the fracture, and informs treatment.
*
Plain Radiographs:
Standard anteroposterior and lateral views, often with oblique projections. Obtain orthogonal views, and include the joint above and below the suspected fracture site. Stress views can assess ligamentous stability.
*
Computed Tomography (CT):
Essential for complex intra-articular fractures (e.g., tibial plateau, pilon, acetabular, calcaneal), spinal fractures, and pelvic ring injuries. CT provides detailed 3D information, aiding pre-operative planning.
*

*
Magnetic Resonance Imaging (MRI):
Indicated for occult fractures not seen on X-ray (e.g., scaphoid, osteochondral lesions, stress fractures), evaluation of soft tissue injuries (ligaments, tendons, menisci), and assessment of bone marrow edema.
*
*
Ultrasound:
Useful for evaluating soft tissue injuries, guiding aspirations, and assessing vascular integrity in some settings.
*
Angiography:
Performed when vascular injury is suspected, typically after clinical or Doppler examination.
*

Diagnostic pitfalls
- Missed fractures: Overlooking subtle fractures, especially in polytrauma or non-displaced fractures. Common sites include the scaphoid, radial head, occult hip fractures, and posterior column acetabular fractures.
- Growth plate injuries: Salter-Harris classifications must be understood in pediatric patients.
- Pathological fractures: Fractures through abnormal bone (e.g., tumor, osteoporosis) may occur with trivial trauma.
- Associated injuries: Focusing solely on the obvious fracture while missing critical ligamentous, neurovascular, or visceral injuries.
Treatment of fractures
Resuscitation and fluid replacement
In the poly-traumatized patient, immediate resuscitation following ATLS guidelines is paramount. This includes airway management, breathing support, control of hemorrhage, and aggressive fluid resuscitation.
*
Initial fluid management:
Crystalloids (e.g., Lactated Ringer's solution) are typically used for initial volume expansion.
*
Blood products:
In cases of significant blood loss, early transfusion of packed red blood cells, fresh frozen plasma, and platelets in a balanced ratio (e.g., 1:1:1) is crucial, guided by massive transfusion protocols.
Complications of transfusion
Transfusion carries risks, including allergic reactions, febrile non-hemolytic transfusion reactions, transfusion-related acute lung injury (TRALI), transfusion-associated circulatory overload (TACO), acute hemolytic reactions, and transmissible infections.
Persisting circulatory impairment
Persistent hypotension and inadequate tissue perfusion necessitate ongoing resuscitation, search for occult bleeding sources (e.g., pelvic fracture, intra-abdominal hemorrhage), and potential surgical intervention for source control.
Head injuries
Co-existing head injuries require immediate neurological assessment (Glasgow Coma Scale) and neurosurgical consultation. Orthopedic management must be coordinated to avoid exacerbating intracranial pressure.
Glasgow Coma Scale
The GCS is a standardized neurological assessment tool, evaluating eye opening, verbal response, and motor response. It is crucial for initial assessment, monitoring, and prognostication in trauma patients.
*
Trauma complications
Beyond immediate hemorrhage and organ injury, trauma patients are at high risk for systemic complications, including acute respiratory distress syndrome (ARDS), sepsis, multiple organ dysfunction syndrome (MODS), deep vein thrombosis (DVT), and pulmonary embolism (PE). Prophylaxis for DVT/PE is standard.
Trauma scoring
Trauma scoring systems aid in prognostication, resource allocation, and quality improvement.
*
Injury Severity Score (ISS):
An anatomical scoring system based on the Abbreviated Injury Scale (AIS).
*
Revised Trauma Score (RTS):
A physiological scoring system incorporating GCS, systolic blood pressure, and respiratory rate.
*
TRISS (Trauma and Injury Severity Score):
Combines ISS, RTS, patient age, and mechanism of injury to predict survival.
General principles of treatment
The overarching goals of fracture treatment are:
1.
Reduction:
Restore anatomical alignment and length.
2.
Immobilization/Fixation:
Maintain reduction to allow bone healing.
3.
Rehabilitation:
Restore function and prevent stiffness.
*

Damage control orthopaedics (DCO)
DCO is a staged surgical approach for severely injured polytrauma patients, aiming to stabilize fractures and control hemorrhage in the acute phase, followed by definitive fixation once the patient is physiologically optimized. This strategy avoids the "second hit" phenomenon associated with prolonged early definitive surgery. Initial stabilization often involves external fixation, followed by conversion to definitive internal fixation later.
Mangled Extremity Severity Score (MESS)
The MESS is a scoring system used to assess the severity of extremity trauma and predict the likelihood of amputation. It considers skeletal/soft tissue injury, limb ischemia, shock, and age. While a high MESS score suggests amputation, it is not an absolute indication, and limb salvage decisions are complex and multifactorial.
*

Suspected child abuse
Fractures in pediatric patients, particularly those with unusual patterns, inconsistent history, or multiple injuries in varying stages of healing, mandate a high index of suspicion for child abuse. A multidisciplinary approach involving social services is essential.
*

| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Absolute Indications |
-
Open Fractures (Gustilo-Anderson Type I-III):
Requires urgent debridement and stabilization to prevent infection.
- Neurovascular Compromise: Fracture causing acute nerve or vascular impairment requiring reduction and stabilization. - Compartment Syndrome (Impending/Actual): Requires fasciotomy and often fracture stabilization. - Polytrauma with Associated Life-Threatening Injuries: Damage control orthopaedics (DCO) principles apply, often with external fixation. - Irreducible Fractures: Fractures that cannot be anatomically reduced by closed means due to soft tissue interposition, muscle spasm, or anatomical blockage. - Pathological Fractures: Often require stabilization and biopsy/resection, especially impending fractures. - Intra-articular Displaced Fractures: Displacement >1-2mm often requires ORIF to restore joint congruity and prevent post-traumatic arthritis. - Certain Unstable Fractures: Specific fracture patterns with a high propensity for displacement or nonunion (e.g., femoral neck, unstable pelvic ring, bilateral forearm fractures, both bone leg fractures with significant displacement). |
-
Non-Displaced or Minimally Displaced Stable Fractures:
Fractures where anatomical alignment is maintained and stability is inherent (e.g., stable distal fibula, non-displaced wrist fractures, stable vertebral compression fractures).
- Fractures in Patients with Significant Comorbidities: When the risks of surgery outweigh the potential benefits (e.g., severe cardiopulmonary disease, sepsis, end-stage malignancy) and functional outcome is less critical than survival. - Certain Pediatric Fractures: High remodeling potential in children allows for greater tolerance of angulation and displacement in specific fracture patterns (e.g., buckle fractures, greenstick fractures, some physeal injuries). - Contraindications to Anesthesia/Surgery: Severe medical comorbidities precluding safe surgical intervention. - Extremely Poor Soft Tissue Envelope: In cases where surgical incision would severely compromise tissue viability and increase infection risk, non-operative measures or external fixation might be preferred as a temporizing or definitive measure. - Patient Refusal: After informed discussion of risks and benefits. |
| Relative Indications |
-
Fractures with Expected Malunion/Nonunion:
High-risk fractures for poor healing or malalignment with non-operative treatment (e.g., proximal humerus, tibial shaft, scaphoid).
- Patient Preference/Functional Demand: Higher demand patients often benefit from operative stabilization for earlier mobilization and return to function. - Open Reduction is More Reliable: When closed reduction is unlikely to achieve or maintain acceptable alignment. - Fractures with Associated Ligamentous Instability: When combined injury dictates surgical repair or reconstruction. - Floating Joints: Fractures above and below a single joint (e.g., ipsilateral femoral and tibial shaft fractures – "floating knee"). |
-
Acceptable Angulation/Shortening:
When residual deformity after closed reduction is within functionally acceptable limits for the patient's age and activity level.
- Stable Periarticular Fractures: Fractures near a joint but not extending into it, without significant displacement or instability. - Contraindications to Specific Fixation Techniques: Allergies to implant materials, local skin infections precluding internal fixation. - Resource Limitations: In austere environments where surgical capabilities are limited, acceptable non-operative management may be the only option. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing surgical outcomes, minimizing complications, and ensuring efficient operative time. This phase integrates diagnostic information, patient-specific factors, and surgeon expertise.
Imaging Review and Fracture Characterization
- Comprehensive Radiological Review: Detailed analysis of plain radiographs (AP, lateral, obliques) to characterize fracture pattern (e.g., simple, wedge, complex comminuted), location, displacement, angulation, and rotation. For complex fractures, CT scans with 3D reconstructions are indispensable for understanding articular involvement, comminution, and fragment orientation. MRI may be reviewed for soft tissue injuries.
- Fracture Classification: Apply established classification systems (e.g., AO/OTA, Gustilo-Anderson for open fractures, Salter-Harris for pediatric physeal injuries) to communicate fracture characteristics concisely and guide treatment algorithms.
- Soft Tissue Assessment: Evaluate the soft tissue envelope for swelling, blistering, open wounds, and ecchymosis. This dictates timing of surgery (e.g., delay for "fracture blisters" to resolve) and choice of incision.
Implant Selection and Templating
- Implant Choice: Based on fracture pattern, bone quality, patient age, activity level, and surgeon preference. Options include intramedullary nails, plates and screws (locking, non-locking, compression, neutralization, bridging), external fixators, wires, and screws.
- Pre-operative Templating: Using X-ray templates or digital planning software, plan the length and size of implants, trajectory of screws, and estimated angles. This helps anticipate technical challenges and ensures appropriate implant availability. For intramedullary nailing, measure nail length and diameter. For plates, estimate plate length and contour.
- Surgical Approach Planning: Identify the optimal surgical approach, considering internervous planes, neurovascular structures, and potential for future soft tissue coverage. Plan the incision location and length.
Patient Preparation and Positioning
- Pre-operative Assessment: Optimize patient comorbidities (e.g., diabetes control, cardiac risk stratification). Administer pre-operative antibiotics within 60 minutes of incision.
- Anesthesia: Discuss anesthesia options (general, regional) with the patient and anesthesia team.
-
Patient Positioning:
Critical for adequate surgical exposure, ease of reduction, and safety.
- Supine: Common for lower extremity fractures (e.g., tibia, femur, ankle), pelvis, and some upper extremity fractures (e.g., distal radius). Often requires a fracture table for traction and fluoroscopy.
- Lateral Decubitus: Used for proximal humerus, some femoral shaft, and hip fractures.
- Prone: For posterior approaches to the spine, calcaneus, and some posterior knee fractures.
- Beach Chair/Semi-Fowler: For shoulder girdle and proximal humerus fractures.
- Maintaining Physiological Homeostasis: Ensure appropriate padding to prevent pressure sores or nerve palsies. Monitor vital signs and maintain normothermia. Prepare for blood loss and transfusion if indicated.
- Fluoroscopy: Position C-arm for optimal views (AP/lateral, oblique) without compromising sterile field or surgical access. Confirm proper setup and function pre-incision.
Detailed Surgical Approach / Technique
The surgical management of fractures aims to achieve stable anatomical reduction and fixation, facilitating bone union and early functional recovery while minimizing iatrogenic damage. The specific technique varies widely depending on the fracture type, location, and soft tissue involvement, but general principles apply. The "point of impact" and the resulting fracture morphology heavily influence the chosen approach and reduction strategy.
1. Incision and Soft Tissue Management
-
Approach Selection:
Based on pre-operative planning, selecting an approach that provides adequate exposure of the fracture while respecting soft tissue viability and internervous planes. Examples:
- Anterolateral/Lateral approaches for tibial shaft fractures (e.g., Henry approach).
- Deltopectoral approach for proximal humerus.
- Direct lateral/Posterolateral approaches for femoral shaft and hip.
- Incision: Design the incision to allow for extensibility, avoid neurovascular structures, and preserve adequate skin bridges for perfusion, especially in polytrauma or open fractures.
- Dissection: Careful, atraumatic dissection through subcutaneous tissue, fascia, and muscle layers. Identify and protect neurovascular bundles. Use blunt dissection where possible. Preserve periosteal attachments to maintain vascularity to the bone fragments, particularly for biological fixation strategies.
- Wound Protection: Use appropriate retractors and moist sponges to protect soft tissues from drying and iatrogenic injury.
2. Reduction Techniques
The goal of reduction is to restore anatomical alignment, length, and rotation. The technique chosen depends on the fracture pattern and surgeon preference. Understanding the mechanism of injury (point of impact, direction of forces) guides the reduction maneuvers to reverse the deforming forces.
-
Closed Reduction with Indirect Techniques:
- Traction and Counter-Traction: Applying longitudinal pull to overcome muscle spasm and restore length. Often performed on a fracture table or with manual traction.
- Ligamentotaxis: Using intact ligaments and soft tissue attachments to indirectly pull and reduce articular fragments, commonly used in intra-articular fractures (e.g., distal radius, pilon).
- External Fixation: Can be used as a reduction aid, applying controlled distraction and compression to align fragments.
- Minimally Invasive Reduction: Using percutaneous clamps, joysticks, or limited incisions to manipulate fragments under fluoroscopic guidance, minimizing soft tissue stripping.
-
Open Reduction with Direct Techniques:
- Direct Manipulation: Using reduction clamps, bone hooks, or instruments to directly grasp and manipulate fragments into anatomical alignment.
- Leverage: Using bone levers or small osteotomes to elevate depressed fragments (e.g., tibial plateau).
- Temporary Fixation: K-wires or provisional clamps are often used to hold reduction while definitive fixation is applied.
3. Fixation Principles and Techniques
Once reduced, the fracture must be stabilized to allow healing. The choice of fixation depends on the desired stability (absolute vs. relative), fracture morphology, bone quality, and patient factors.
-
Absolute Stability (Anatomic Reduction with Compression):
- Lag Screw Principle: Achieves interfragmentary compression across a fracture line, typically for simple, oblique, or spiral fractures. The screw glides in the near cortex and purchases threads in the far cortex, pulling the fragments together.
- Compression Plating: Using dynamic compression plates (DCP) or limited contact DCP (LC-DCP) to apply axial compression across a transverse or short oblique fracture. Eccentric screw placement or a tension device can generate compression.
- Indications: Intra-articular fractures, simple diaphyseal fractures where anatomical reduction and direct bone healing are desired.
-
Relative Stability (Biologic Fixation with Bridging/Splinting):
- Intramedullary Nailing: Gold standard for many diaphyseal fractures of the femur and tibia. The nail acts as an internal splint, sharing load with the bone, allowing for micromotion at the fracture site (secondary bone healing with callus formation). Reamed vs. unreamed nailing. Locked with proximal and distal screws to control length and rotation.
- Bridging Plating: Used for comminuted diaphyseal fractures, especially with locking plates. The plate is applied to span the comminuted zone without directly compressing fragments. It maintains length and alignment while preserving the fracture hematoma and biological environment.
- External Fixation: Provides rigid immobilization without extensive soft tissue dissection. Used for open fractures, provisional stabilization in polytrauma (DCO), highly contaminated wounds, or when internal fixation is contraindicated.
- Indications: Comminuted diaphyseal fractures, open fractures, metaphyseal fractures where precise anatomical reduction of all fragments is not critical but alignment and length are.
-
Other Fixation Methods:
- Tension Band Wiring: Converts distractive forces into compressive forces, typically used for fractures where muscle pull creates tension (e.g., olecranon, patella, medial malleolus).
- K-wires/Pins: Used for temporary fixation, small fragment fixation, or in pediatric fractures.
- Screws Alone: For specific fractures (e.g., malleolar fractures, scaphoid, condylar fractures).
4. Intra-operative Assessment
- Fluoroscopy: Essential for confirming reduction, implant position, and stability. Obtain multiple views (AP, lateral, obliques) and assess length, alignment, and rotation.
- Stability Testing: Gently stress the fracture site to ensure adequate stability of the construct.
- Neurovascular Reassessment: Re-evaluate distal pulses and neurological function after fixation to ensure no iatrogenic injury or compromise.
5. Wound Closure
- Hemostasis: Achieve meticulous hemostasis to prevent hematoma formation, which can increase infection risk and compartment pressure.
- Irrigation: Copious irrigation of the surgical field, especially for open fractures.
- Layered Closure: Close muscle fascia, subcutaneous tissue, and skin in layers. Consider drains in select cases.
- Dressing: Apply a sterile dressing and appropriate splint or cast as indicated.
By adhering to these principles and adapting techniques based on the specific fracture characteristics and patient presentation, surgeons can optimize outcomes in fracture management.
Complications & Management
Fracture management, both operative and non-operative, carries inherent risks. A thorough understanding of potential complications and their timely management is crucial for minimizing morbidity and improving long-term outcomes.
| Complication | Incidence (Approximate) | Salvage Strategy / Management |
|
Fracture-Specific
| -
Non-Union:
5-15% (depending on bone, comminution, infection).
-
Malunion:
5-10%. |
|
Infection
| Operative: 1-5% for closed, 10-50% for open.
Non-operative: <1% for pin-site infection. |
Superficial:
Oral antibiotics, local wound care.
Deep/Hardware-related:
Surgical debridement, thorough irrigation, potentially hardware removal (if union achieved or nonunion with infection), intravenous antibiotics, culture-guided antibiotic therapy.
Osteomyelitis:
Staged debridement, bone sampling for culture, long-term targeted intravenous and oral antibiotics, reconstruction with bone grafts/flaps if necessary. Early detection and aggressive management are key. |
|
Nonunion
| 5-15% (higher in tibia, open fractures, poor biology, smoking, comorbidities). |
Hypertrophic:
Revision surgery with more stable fixation (e.g., IMN exchange, stronger plate), often with reaming to stimulate bone, without bone graft.
Atrophic:
Revision surgery with stable fixation, debridement of fibrous tissue, bone grafting (autograft/allograft), osteoinductive agents (e.g., BMP), potentially electrical or ultrasonic stimulation. Address underlying causes (infection, poor biology, micromotion, malnutrition). |
|
Malunion
| 5-10% (more common in conservative treatment, less common with operative but can occur). |
Minor/Asymptomatic:
Observation.
Symptomatic/Functional Impairment:
Corrective osteotomy and stable internal fixation to restore alignment and joint mechanics. Joint replacement if severe arthritis has developed. |
|
* | | |
|
| | |
| ** ** |
Operative Procedures:
|
Non-Operative Modalities:
|
|
Diagnosis
| | |
| | |
|
|
*Medical History:
Relevant past medical history, medications, allergies, surgical history, family history, social history (smoking, alcohol, recreational drugs, occupation). Specific attention to bleeding diatheses, diabetes, osteoporosis, and renal function. |
Fracture Classification:
Understand the fracture pattern (simple, comminuted, intra-articular), displacement, angulation, rotation, and soft tissue involvement. Evaluate stability based on morphology. |
|
Description | A break in the continuity of bone or cartilage. The mechanism of injury, often involving a "point of impact," directly dictates the fracture pattern. This guide focuses on diagnosis and management in an academic setting. |
|
Primary Diagnosis | The diagnosis of fractures and principles of treatment.
How to diagnose a fracture
*
1 History
In taking the history of a patient who may have a fracture, the following points may prove to be helpful, especially when there has been a traumatic incident.
1 What activity was being pursued at the time of the incident (e.g. taking part in a sport, driving a car, working at a height, etc.)?
2 What was the nature of the incident (e.g. a kick, a fall, a twisting injury, etc.)?
3 What was the magnitude of the applied forces? For example if a patient was injured in a fall, it is helpful to know how far he fell, if his fall was broken, the nature of the surface on which he landed, and how he landed; trivial violence may lead one to suspect a pathological fracture: severe violence makes the exclusion of multiple injuries particularly important.
4 What was the point of impact and the direction of the applied forces? In reducing a fracture, one of the principle methods employed is to redup |
|
Emergency Assessment:
| Trauma complications; Persisting circulatory impairment; Head injuries; Glasgow Coma Scale; Trauma scoring; Resuscitation and fluid replacement; Complications of transfusion. |
