Pediatric
Orthopedic Surgery
Epiphysiodesis
| Developmental dysplasia of | 443 | Slipped upper femoral epiphysis: Osteotomy | 462 |
| --- | --- | --- | --- |
| the hip: Closed reduction | 446 | Tendo-Achilles lengthening | 464 |
| Developmental dysplasia of the hip: Open reduction | 449 | Congenital talipes equinovarus correction | 469 |
| Developmental dysplasia of the | |
| Surgical treatment of Perthes disease | 473 |
| hip: Pelvic osteotomy 452 Principles of surgery in cerebral palsy | 476 |
| Developmental dysplasia of the Guided growth: Temporary hip: Proximal femoral osteotomy 456 hemiepiphysiodesis | 479 |
| Slipped upper femoral epiphysis: Viva questions | 481 | --- | --- | Pinning | 459 |
Epiphysiodesis
Preoperative planning
Epiphysiodesis involves destruction of the physis to allow equalisation of leg length discrepancy (LLD) in children. As most growth occurs around the knee , the distal femoral and/or the proximal tibial and fibular physes are targeted depending on the predicted remaining growth.
Indications
1. Predicted true LLD 2–5 cm at maturity
2. May be used to treat LLD greater than 7 cm through lengthening of the short limb and epiphysiodesis of the long limb
Contraindications
3. Apparent LLD
4. LLD less than 1.5 cm
5. Localised infection
6. Tumour
7. Closed physis
Consent and risks
1. Neurovascular injury : Less than 1%
2. Infection : Less than 1%
3. Fracture : Less than 1%
4. Angular deformity : Less than 1%
5. Residual LLD : 80% patients within 1 cm
Operative planning
Various methods exist to determine the LLD at maturity and to guide the timing and type of epiphysiodesis (distal femoral and/or proximal tibial):
8. Green-Anderson growth remaining method : Estimates growth potential in the distal femoral and proximal tibial physes at various skeletal ages separately for girls and boys.
9. Moseley straight-line graph : A logarithmic representation of the Green-Anderson method.
10. Menelaus arithmetic method : Assumes growth of 10 mm/year from distal femur and
6 mm/year from the proximal tibia and that girls reach maturity at 14 years and boys at 16 years.
11. Eastwood-Cole method : A graphic representation of the arithmetic method but takes into account non-linear changes in LLD. Bone age is more reliable than chronological age in determining growth remaining and can be calculated using the Greulich and Pyle method. This involves comparison of a left hand and wrist radiograph with a known standard.
Anaesthesia and positioning
General anaesthesia is used, together with intravenous antibiotic prophylaxis. The patient is positioned supine with the knee slightly flexed over a small sandbag. A pneumatic thigh tourniquet is used. An image intensifier is required and a gonadal shield should be appropriately placed.
Surgical technique
Landmarks
The image intensifier is used to mark the orientation of the physis in the frontal plane and the midpoint of the physis in the lateral plane.
Approach
A 1–2 cm longitudinal incision is centred over the midpoint of physis medially and laterally. A larger incision is made laterally to identify and protect the common peroneal nerve if performing proximal fibular epiphysiodesis.
Dissection
Sharp dissection is continued down to bone.
Procedure
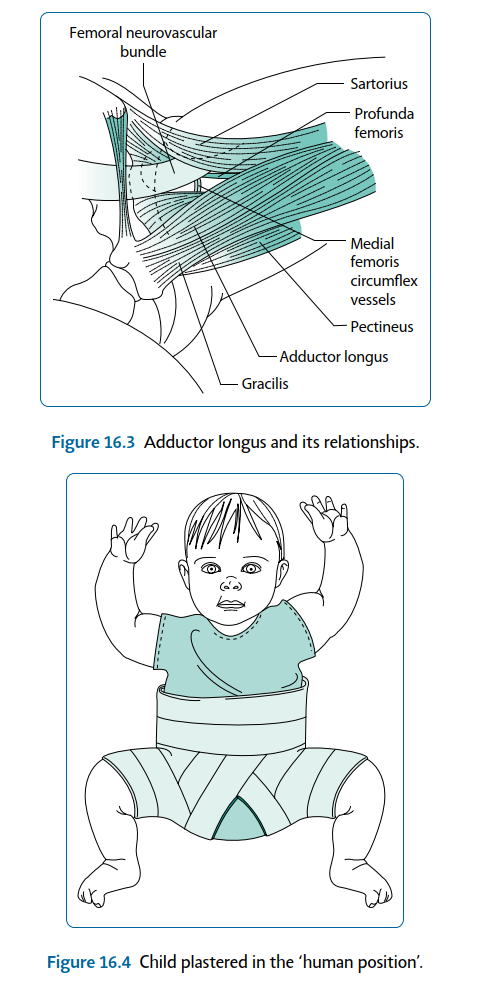
Physeal cartilage is removed using a 4.5 mm diameter drill under image guidance: A single entry point is made in the lateral cortex in line with the physis on the frontal view and at its midpoint on the lateral view. This minimises weakening of the cortex and the risk of subsequent fracture. The drill is advanced transversely along the line of the physis in the frontal view until the tip reaches its midpoint (Figure 16.1). 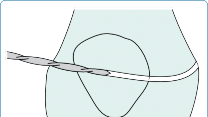

Figure 16.1 The trajectory of the drill should be checked periodically using the image intensifier to ensure obliteration of the physis. Using the same entry point each time, the drill is tilted 30° first anteriorly then posteriorly and advanced to the halfway mark to remove a fan-shaped area of physeal cartilage (Figure 16.2). This technique is then repeated on the medial side. The swarf should be 

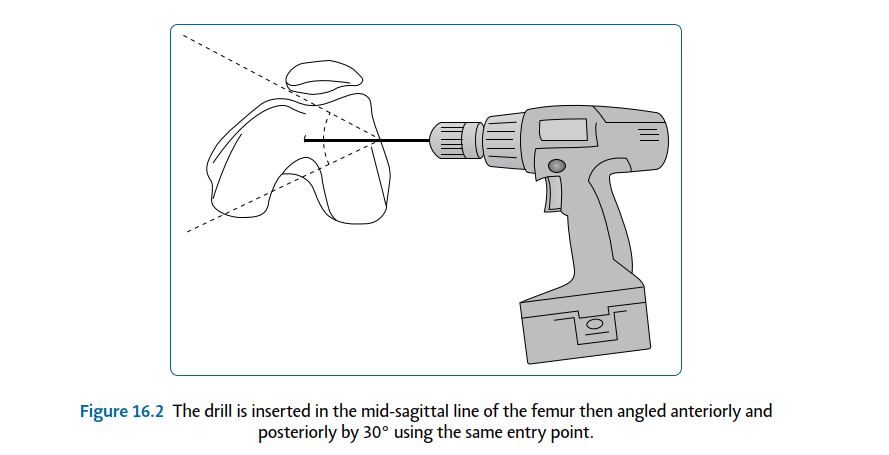
Figure 16.2 The drill is inserted in the mid-sagittal line of the femur then angled anteriorly and posteriorly by 30° using the same entry point.
inspected to ensure removal of physeal cartilage. Further curettage of the epiphyseal surface is performed to remove any remaining physeal cartilage.
Closure
A layered closure is used with absorbable subcuticular material to skin.
Postoperative instructions
12. Mobilise full weightbearing with crutches for comfort for up to 2 weeks
13. Radiographs at 3 months then periodically until maturity to assess physeal closure and leg lengths
Recommended
Scientific References
-
Atar D, Lehman WB, Grant AD et al. Percutaneous epiphysiodesis. _J Bone Joint Surg Br_. 1991;73:173. Eastwood DM, Cole WG. A graphic method for timing the correction of leg-length discrepancy. _J Bone_
_Joint Surg Br. 1995;77:743–747._
Menelaus MB. Correction of leg length discrepancy by epiphyseal arrest. _J Bone Joint Surg Br_.
1966;48:336–339.
Snyder M, Harcke HT, Bowen JR et al. Evaluation of physeal behaviour in response to epiphysiodesis with the use of serial magnetic resonance imaging. _J Bone Joint Surg Am_. 1994;76:224–229.
[Developmental dysplasia of the hip: Closed reduction](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark16)
Preoperative planning
Although often combined with an arthrogram and soft tissue releases, technically this remains a closed procedure as the capsule is not opened. Adductor and psoas releases are performed via an open medial approach, the technical details of which are provided in the section ‘Developmental dysplasia of the hip: Open reduction’ (p. 449).
The optimum timing of reduction is subject to debate: Waiting for the capital femoral epiphysis to appear reduces the risk of avascular necrosis although, conversely, early reduction suggests a better long-term outcome.
_Indications_
- 14. 6- to 18-month-old child with developmental dysplasia of the hip (DDH) [View Source / PubMed]
- 15. Failed treatment with Pavlik harness _Contraindications_ This is contraindicated in a child less than 6 months or older than 18 months. _Consent and risks_ [View Source / PubMed]
- 1. Application of spica plaster in the human position; subsequent care must be explained to parents [View Source / PubMed]
- 2. _Avascular necrosis : 5%–10%_ [View Source / PubMed]
- 1. _Re-dislocation : Less than 5%_ [View Source / PubMed]
- 2. _Further surgery : 20%_ [View Source / PubMed]
- 3. _Neurovascular injury and infection : Less than 1% (if arthrogram and soft tissue releases performed)_ [View Source / PubMed]
- 4. _Risk of conversion to open reduction : 10%–20%; greater risk for high-riding dislocation_ _Operative planning_ Imaging studies are requested depending on the expected presence of the ossific nucleus: [View Source / PubMed]
- 16. Dynamic ultrasound if less than 6 months of age to determine alpha and beta angles, reducibility and capsular laxity. [View Source / PubMed]
- 17. Plain anteroposterior (AP) pelvis and frog lateral radiographs if older than 6 months. Note any delayed appearance of ossific nucleus, Shenton, Hilgenreiner and Perkins lines, acetabular index and Tonnis grade. _Anaesthesia and positioning_ General anaesthesia is used. The patient is positioned supine at the end of a radiolucent table, to allow image intensifier access. The surgeon stands between flexed, abducted and externally rotated hips. Surgical technique Examination under anaesthesia (EUA) and arthrogram are first performed to assess reduction and the need for adductor longus, gracilis and psoas release. _Landmarks_ [The landmark is the adductor longus muscle – palpable in the child’s groin (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark31)Figure 16.3). _Procedure_ A 22G spinal needle is introduced beneath the palpable adductor longus tendon in the groin and advanced cranially towards the ipsilateral scapular until the tip is felt to traverse the hip capsule. The position is confirmed with image intensifier before instilling 0.5 mL of diluted contrast. The hip is reduced with a combination of flexion, abduction and anterior displacement without excessive force. Soft tissue releases should be considered if this does not occur easily. If the head appears to stand out from the acetabulum on the arthrogram, this suggests a block to reduction such as an infolded labrum. A conversion to open reduction may therefore be required. The stability is assessed within the safe zones of flexion and abduction. Typically, a stable position is 90° of flexion and 30°–50° of abduction. Extreme positions increase the risk of avascular necrosis and must be avoided.  Figure 16.4 Child plastered in the ‘human position’. [A well-padded spica plaster is carefully applied in the human position before final radiographic confirmation of reduction (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark32)Figure 16.4). Postoperative instructions [View Source / PubMed]
- 18. Plaster check prior to discharge [View Source / PubMed]
- 19. Limited slice computed tomography (CT) at 2/52 to confirm maintenance of reduction [View Source / PubMed]
- 20. Convert to abduction brace at 10/52 [View Source / PubMed]
- 21. Wean out of brace after further 6/52; depending on acetabular development, night-time bracing may continue for up to 1 year Recommended references Kalamchi A, MacEwen GD. Avascular necrosis following treatment of congenital dislocation of the hip. _J Bone Joint Surg Am. 1980;62:87688._ Malvitz TA, Weinstein SL. Closed reduction for congenital dislocation of the hip. Functional and radiographic results after an average of thirty years. _J Bone Joint Surg Am_. 1994;12:177792. Ramsey PL, Lasser S, MacEwen GD. Congenital dislocation of the hip: Use of the Pavlik harness in the child in the first six months of life. _J Bone Joint Surg Am_. 1978;58:1000–1004. Severin E. Contribution to knowledge of congenital dislocation of the hip joint: Late results of closed reduction and arthrographic studies of recent cases. _Acta Chir Scand Suppl_. 1941;63:142. Tennant SJ, Eastwood DM, Calder P, Hashemi-Nejad A, Catterall A. A protocol for the use of closed reduction in children with developmental dysplasia of the hip incorporating open psoas and adductor releases and a short-leg cast: Mid-term outcomes in 113 hips. _Bone Joint J_. 2016;98–B**(** 11**)** : 1548–1553. [Developmental dysplasia of the hip: Open reduction](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark18) Preoperative planning Open reduction deals directly with soft tissue obstruction facilitating relocation of the hip without excessive force. _Indications_ [View Source / PubMed]
- 22. Children 6–18 months with obstruction to closed reduction (psoas tendon, contracted capsule, ligamentum teres, transverse acetabular ligament and inverted limbus), an unstable safe zone, previous failed closed or open reduction [View Source / PubMed]
- 23. Children presenting over 18 months _Contraindications_ The procedure is contraindicated in children less than 6 months old. _Consent and risks_ [View Source / PubMed]
- 1. Application of spica plaster; subsequent care must be explained to parents [View Source / PubMed]
- 2. _Neurovascular injury : Less than 1%_ [View Source / PubMed]
- 3. _Infection : Less than 1%_ [View Source / PubMed]
- 4. _Avascular necrosis : 5%_ [View Source / PubMed]
- 5. _Re-dislocation : 1%_ [View Source / PubMed]
- 6. _Further surgery for dysplasia or LLD : 10%–15%_ _Operative planning_ Planning should include radiographs as per closed reduction. _Anaesthesia and positioning_ General anaesthesia with intravenous antibiotics is used. The patient is positioned supine at the end of a radiolucent table. The surgeon stands between the patient’s legs for a medial approach or on the operative side for an anterior approach. An image intensifier is required. Surgical technique A medial approach is used if the patient is less than 12 months old; an anterior approach, via a bikini incision, is preferred if the child is older. Medial approach _Landmarks_ The adductor longus tendon is a landmark – palpable in the groin, approximately 2 cm lateral to the labia/scrotum. _Incision_ A 2.5 cm, vertical skin crease incision is centred on the palpable tendon of adductor longus. _Superficial dissection_ _Structures at risk_ [View Source / PubMed]
- 1. Anterior and posterior divisions of obturator nerve The fascia overlying the tendons of adductor longus and gracilis is opened along their length and fractional lengthening tenotomies are performed. Adductor magnus and brevis are exposed with blunt dissection. Branches of the obturator nerve are identified on the superficial surface of the adductor brevis and are protected. _Deep dissection_ _Structure at risk_ [View Source / PubMed]
- 1. Medial circumflex femoral artery The plane between the adductor magnus and brevis is dissected to access the lesser trochanter. A psoas tenotomy is performed under direct vision avoiding the medial femoral circumflex vessels which pass over the medial surface of the psoas tendon distally. A medial arthrotomy is made above the vessels, and the acetabular attachment of the ligamentum teres is divided and used as a traction aid to relocate the femoral head. It is then sutured to the anterior inferior capsule. Anterior approach _Landmarks_ [View Source / PubMed]
- 24. Anterior superior iliac spine (ASIS) [View Source / PubMed]
- 25. Pubic tubercle _Incision_ The line of the inguinal ligament is marked between the ASIS and the pubic tubercle. A second line is then dropped vertically downwards from the ASIS. Next, a 5 cm bikini line incision is marked 2 cm inferior and parallel to the inguinal ligament, one-third of it medial and two-thirds lateral to the vertical line. _Superficial dissection_ _Structure at risk_ [View Source / PubMed]
- 1. Lateral cutaneous nerve of the thigh The interval between sartorius and tensor fascia lata is developed to reach the rectus femoris and gluteus medius. _Deep dissection_ [The interval between the rectus femoris and gluteus medius is dissected and the straight head of the rectus femoris is detached from the anterior capsule. It may then be retracted medially to allow psoas tenotomy and L-shaped anterior arthrotomy (see](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark34)[Figure ](#bookmark34)16.5).  Figure 16.5 Anterior approach to the right hip. _Procedure_ Obstructions to reduction are removed as necessary; pulvinar is extracted, the transverse ligament is released and the ligamentum teres excised if obstructive. Adductor releases are performed, via a separate groin incision, to facilitate reduction as required. The redundant capsule is tightened with capsulorrhaphy following reduction. Using the image intensifier, the position of maximum stability is identified; the hip is placed in 30° of internal rotation, flexion and abduction and then each of these positions is removed in sequence to determine positioning in plaster and the need for future surgery. Femoral osteotomy or an acetabular procedure may be undertaken concomitantly if severe dysplasia is present in an older child. _Closure_ [View Source / PubMed]
- 26. Layered closure ensuring reconstruction of rectus femoris. [View Source / PubMed]
- 27. Skin is closed with absorbable subcuticular material followed by a waterproof dressing. A well-padded spica plaster is carefully applied in the stable safe zone of flexion and abduction before final radiographic confirmation of reduction. This should be in greater than 90° of flexion without forced flexion and abducted between 30° and 60°. Postoperative instructions [View Source / PubMed]
- 28. Plaster check prior to discharge [View Source / PubMed]
- 29. Limited slice CT at 2 weeks to confirm maintenance of reduction [View Source / PubMed]
- 30. Spica removal at 10 weeks and mobilisation allowed [View Source / PubMed]
- 31. Follow-up at 3 months with radiographs Recommended references Ferguson AB Jr. Primary open reduction of congenital dislocation of the hip using a median adductor approach. _J Bone Joint Surg Am_. 1973;55:671–681. Morcuende JA, Meyer MD, Dolan LA et al. Long term outcome after open reduction through an anteromedial approach for congenital dislocation of the hip. _J Bone Joint Surg Am_. 1997;79:810–817. Wright J, Tudor F, Luff T, Hashemi-Nejad A. Surveillance after treatment of children with developmental dysplasia of the hip: Current UK practice and the proposed Stanmore protocol. _J Pediatr Orthop B_. 2013 Nov;22**(** 6**)** :509–515. Zadeh HG, Catterall A, Hashemi-Nejad A et al. Test of stability as an aid to decide the need for osteotomy in association with open reduction in developmental dysplasia of the hip. A long term review. _J Bone Joint Surg Br_ 2000;82:17–27. [Developmental dysplasia of the hip: Pelvic osteotomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark20) Various techniques exist for pelvic osteotomy in DDH, and an account of them all is beyond the scope of this chapter. Therefore, only the Salter and Pemberton types are described further. Salter osteotomy Preoperative planning _Indications_ [View Source / PubMed]
- 32. Acetabular dysplasia; acetabulum faces anterolaterally causing deficient anterior coverage in extension and deficient superior coverage in adduction [View Source / PubMed]
- 33. Congruent hip [View Source / PubMed]
- 34. 18 months to 6 years (as it requires flexibility of symphysis pubis) _Contraindications_ [View Source / PubMed]
- 35. Bilateral DDH (uncovers contralateral hip) [View Source / PubMed]
- 36. Congruent reduction not achievable on EUA arthrogram _Consent and risks_ [View Source / PubMed]
- 1. _Overall risks : Less than 5%_ [View Source / PubMed]
- 2. _Neurovascular injury : 1%_ [View Source / PubMed]
- 3. Limited weightbearing/crutches [View Source / PubMed]
- 4. _Infection : Less than 1%_ [View Source / PubMed]
- 5. _LLD : Gains 1 cm with Salter osteotomy_ [View Source / PubMed]
- 6. Triradiate cartilage growth arrest (Pemberton osteotomy) [View Source / PubMed]
- 7. Failure of graft [View Source / PubMed]
- 8. Hardware breakage [View Source / PubMed]
- 9. Residual dysplasia (retroversion) [View Source / PubMed]
- 10. _Secondary degeneration : Lateralisation of joint increases joint reaction force (Salter)_ [View Source / PubMed]
- 11. Further surgery (removal of hardware, salvage procedures) _Operative planning_ Congruency confirmed with EUA arthrogram. _Anaesthesia and positioning_ General anaesthesia is used, together with intravenous antibiotics. The patient is positioned supine with an ipsilateral sandbag in a position suitable for image intensifier access. Surgical technique Anterosuperior coverage is achieved at the expense of posterior coverage by flexing the acetabular fragment. Typically, the lateral centre edge angle will increase by 10°. It is performed via an anterior approach (see ‘Developmental dysplasia of the hip: Open reduction’, p. 449) extending the bikini incision proximally over the iliac crest to allow splitting of the iliac apophysis and subperiosteal exposure of the ilium to reach the sciatic notch. _Procedure_ _Structures at risk_ [View Source / PubMed]
- 1. _Sciatic nerve : Rang retractors are placed in the sciatic notch keeping them closely applied to bone to protect the nerve_ [View Source / PubMed]
- 2. Devascularization/denervation of abductors An osteotomy is performed between the sciatic notch and midway between the ASIS and anterior inferior iliac spine (AIIS) using a Gigli saw. This should appear to be parallel to the acetabular surface on AP images. Hinging on the symphysis pubis, the acetabulum is rotated anteriorly and laterally to gain coverage while avoiding retroversion. [A wedge of bone from the iliac wing is inserted perpendicular to the weightbearing axis. The ‘winking sign’ should be noted on an image intensifier (foreshortening of ipsilateral obturator foramen) and the position held with two threaded Schantz pins across the osteotomy. Image guidance is used to advance the pins proximodistally beginning just proximal to the ASIS and aiming for the triradiate cartilage (](#bookmark36)Figures 16.6 [and ](#bookmark37)16.7).   Figure 16.6 Salter osteotomy.   Figure 16.7 Radiograph showing left Salter osteotomy and ‘winking sign’. _Closure_ [View Source / PubMed]
- 37. Layered closure ensuring repair of the iliac apophysis [View Source / PubMed]
- 38. Absorbable subcuticular material to skin Postoperative instructions Plaster spica for those under 6 years of age. Limited weightbearing with crutches for 6–8 weeks if over 6 years of age. Pemberton osteotomy Preoperative planning _Indications_ [View Source / PubMed]
- 39. Double diameter dysplastic acetabulum [View Source / PubMed]
- 40. Congruent hip [View Source / PubMed]
- 41. Open triradiate cartilage [View Source / PubMed]
- 42. Close to normal range of motion [View Source / PubMed]
- 43. No degeneration [View Source / PubMed]
- 44. Normal proximal femoral morphology [View Source / PubMed]
- 45. Paralytic hip disorders/Ehlers-Danlos syndrome (posterior coverage is maintained, conferring stability) _Contraindications_ [View Source / PubMed]
- 46. Poor range of motion (flexion, abduction and internal rotation will be further diminished) [View Source / PubMed]
- 47. Closed triradiate cartilage [View Source / PubMed]
- 48. Congruent reduction not achievable [View Source / PubMed]
- 49. Centre of rotation of head and acetabulum coincide For consent and risks/preoperative preparation/anaesthesia and positioning, see ‘Salter osteotomy’ (p. 452). Surgical technique [The Pemberton osteotomy reduces the volume of a large-diameter acetabulum making the centre of rotation of both femoral head and socket coincident. The acetabulum is displaced forwards and laterally hinging on the triradiate cartilage (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark38)[Figure ](#bookmark38)16.8). The autograft is stable and fixation is therefore not required. The approach and exposure are performed as per the Salter osteotomy.    Figure 16.8 Pemberton osteotomy. _Procedure_ The osteotomy is made 10–15 mm superior to the AIIS passing a curved osteotome posteriorly to reach the ilioischial and iliopubic limb of the triradiate cartilage (midway between sciatic notch and posterior acetabular rim). The acetabulum is hinged on the triradiate to improve coverage. Corticocancellous graft is harvested from the iliac wing and inserted into the osteotomy site. Posterior stability negates the need for internal fixation. _Closure_ This is the same as per Salter osteotomy. Postoperative instructions Instructions are the same as per Salter osteotomy. Recommended references Colemann SS. The incomplete pericapsular (Pemberton) and innominate (Salter) osteotomies. _Clin Orthop_. 1974;98:116–123. Pemberton PA. Pericapsular osteotomy of the ilium for treatment of congenital subluxation and dislocation of the hip. _J Bone Joint Surg Am_. 1965;47:65–86. Salter RB. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. _J Bone Joint Surg Br_. 1961;43:518–539. Thomas SR, Wedge JH, Salter RB. Outcome at forty five years after open reduction and innominate osteotomy for late presenting developmental dysplasia of the hip. _J Bone Joint Surg Am_. 2007;89:2341–2350. [Developmental dysplasia of the hip: Proximal femoral](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark22)[ osteotomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark22) The varus derotation osteotomy (VDRO) is the most common type performed for DDH. Preoperative planning _Indications_ [View Source / PubMed]
- 50. Persistent dysplasia following DDH (coxa valga, anteversion) [View Source / PubMed]
- 51. Congruent reduction in abduction and internal rotation [View Source / PubMed]
- 52. Reasonable sphericity (lateral portion of head intact) _Contraindications_ [View Source / PubMed]
- 53. Limited range of motion (abduction and internal rotation) [View Source / PubMed]
- 54. Active infection [View Source / PubMed]
- 55. Pelvic procedure more appropriate (centre-edge angle [CEA] <15°) [View Source / PubMed]
- 56. Previous avascular necrosis is a relative contraindication with less predictable results [View Source / PubMed]
- 57. Be aware that VDRO will compound an existing negative LLD _Consent and risks_ [View Source / PubMed]
- 1. Plaster spica if under 6 years [View Source / PubMed]
- 2. Limited weightbearing with crutches if over 6 years [View Source / PubMed]
- 3. Bleeding [View Source / PubMed]
- 4. Neurovascular damage: 1% [View Source / PubMed]
- 5. _Infection : Less than 1%_ [View Source / PubMed]
- 6. _Delayed/non-union : 1%–5% (greater risk with increasing age)_ [View Source / PubMed]
- 7. _Failure of hardware : Less than 1%_ [View Source / PubMed]
- 8. Incomplete correction [View Source / PubMed]
- 9. _LLD : Inevitable with closing wedge varus osteotomy_ [View Source / PubMed]
- 10. Joint degeneration [View Source / PubMed]
- 11. Further surgery (removal of hardware, complex arthroplasty) _Operative planning_ An EUA and arthrogram is performed to confirm adequate range of motion and concentric reduction; greater than 15° abduction is required for a varus femoral osteotomy. The type of fixation device and degree of fixed angle are decided (e.g. blade plate/Coventry pin and plate; 90° or 130° angle). _Anaesthesia and positioning_ [View Source / PubMed]
- 58. General anaesthesia [View Source / PubMed]
- 59. Supine with ipsilateral buttock sandbag [View Source / PubMed]
- 60. Intravenous antibiotic prophylaxis [View Source / PubMed]
- 61. Image intensifier Surgical technique A lateral approach to the subtrochanteric region of the proximal femur is used to avoid compromise to the vascular supply to the femoral head. _Landmarks_ The predicted trajectory of the chosen device along the femoral neck is planned and marked using the image intensifier. _Incision_ A 10 cm longitudinal wound is used, running along the lateral aspect of the proximal femur from the metaphyseal flare of the greater trochanter to the proximal femoral diaphysis. _Superficial dissection_ The longitudinal incision is continued through superficial fat and the fascia lata, in line with the skin incision. _Deep dissection_ _Structures at risk_ [View Source / PubMed]
- 1. Perforating branches of profunda femoris artery: These should be identified and cauterised where necessary. The posterior insertion of vastus lateralis is detached from the posterior intermuscular septum and reflected anteriorly to expose the lateral surface of proximal femur. The periosteum is incised longitudinally and elevated at the site of the predicted osteotomy. _Procedure_ Beginning from the lateral cortex just inferior to the flare of the greater trochanter, a guide wire is passed up the femoral neck, under image control, without breaching the physis. The trajectory should aim to restore a normal neck-shaft angle of 130°. The wire is measured and over-drilled before insertion of the cannulated lag screw. Under image guidance, the proximal osteotomy is made perpendicular to the shaft in the subtrochanteric region using an oscillating saw. The second osteotomy is made beginning at the same entry point on the lateral cortex with the saw tilted inferiorly creating a medially based wedge with a lateral apex. The medial cortex is then completed using an osteotome. A guide wire is inserted transversely into the anterolateral cortex distal to the future position of the plate. [The leg is adducted to close the varus osteotomy, and the guide wire is used as a joystick to externally rotate the distal shaft into a satisfactory position on fluoroscopy (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark40)[Figure ](#bookmark40)16.9). Congruent alignment of the lateral cortices should be checked to ensure seating of the plate. The plate is applied over the lag screw, and the distal shaft is reduced onto the plate and held with a Hey-Groves clamp while maintaining correct orientation. Four bicortical screws are inserted to fix the plate before removal of the guide wire. The degree of correction and position of hardware are confirmed with imaging.  Figure 16.9 Stages in varus derotation osteotomy. (a) Valgus, anteverted proximal femur. (b) Screw placed under image guidance. (c) Medially based closing wedge osteotomy performed from lateral side. (d) Varus producing osteotomy closed and held with plate following derotation. _Closure_ [View Source / PubMed]
- 62. Layered absorbable closure of vastus lateralis then fascia lata [View Source / PubMed]
- 63. Subcuticular absorbable material to skin Postoperative instructions [View Source / PubMed]
- 64. Mobilise partial weightbearing [View Source / PubMed]
- 65. Increase weightbearing status at 6–8 weeks after union confirmed clinically and radiographically Recommended references Blockey NJ. Derotation osteotomy in the management of congenital dislocation of the hip. _J Bone Joint Surg Br_. 1984;66:485–490. Kasser JR, Bowen JR, MacEwen GD. Varus derotation osteotomy in the treatment of persistent dysplasia in congenital dysplasia of the hip. _J Bone Joint Surg Br_. 1985;67:195–202. Williamson DM, Benson MKD. Late femoral osteotomy in congenital dislocation of the hip. _J Bone Joint Surg Br_. 1988;70:614–618. [Slipped upper femoral epiphysis: Pinning](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark24) Manoeuvres to reduce the epiphysis are associated with a high incidence of avascular necrosis (40%); pinning _in situ_ therefore aims to prevent further displacement, promote physeal closure and minimise future secondary degeneration. Slips are described as stable if weightbearing is possible or unstable if weightbearing is not possible even with crutches. Preoperative planning _Indications_ [View Source / PubMed]
- 66. Grades I—II slip (Southwick angle <60°) [View Source / PubMed]
- 67. Bilateral pinning is performed if there is [View Source / PubMed]
- 1. Evidence of bilateral slip [View Source / PubMed]
- 2. Endocrinopathy [View Source / PubMed]
- 3. Younger end of age spectrum (10 years – girls, 12 years – boys) _Contraindications_ [View Source / PubMed]
- 68. Advanced avascular necrosis [View Source / PubMed]
- 69. Active infection _Consent and risks_ [View Source / PubMed]
- 1. Limited weightbearing/crutches [View Source / PubMed]
- 2. Avascular necrosis: 0%–5% but higher if unstable slip [View Source / PubMed]
- 3. _Chondrolysis : 10% (greater risk for African Caribbeans, females and poor technique)_ [View Source / PubMed]
- 4. _Fracture : Less than 1%_ [View Source / PubMed]
- 5. _Infection : Less than 1%_ [View Source / PubMed]
- 1. Failure of hardware [View Source / PubMed]
- 2. Further slip (associated with inadequate screw advancement) [View Source / PubMed]
- 3. _LLD : 1.5 cm difference on average_ [View Source / PubMed]
- 4. Joint degeneration [View Source / PubMed]
- 5. Further surgery (removal of hardware/osteotomy/arthrodesis/complex arthroplasty) _Operative planning_ [View Source / PubMed]
- 70. [An AP and Billings lateral of both hips – it is bilateral in 25% of cases (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark42)**[Figures** ](#bookmark42) ## 16.10 [and](#bookmark43)16.11) 71. Endocrine workup if at younger end of age spectrum _Anaesthesia and positioning_ [View Source / PubMed]
- 72. General anaesthesia is used. [View Source / PubMed]
- 73. Patient is positioned supine on a radiolucent table; care is taken when transferring, preparing and draping the unstable hip to prevent further displacement. [View Source / PubMed]
- 74. Intravenous antibiotic prophylaxis is given. [View Source / PubMed]
- 75. Image intensifier. Surgical technique An aspiration of the hip is first performed under image guidance for pain relief and to decompress the retinacular vessels. 25°    Figure 16.10 Patient positioning for Billings lateral radiograph. The hip is abducted, externally rotated and elevated 25° on a foam wedge.  _Landmarks_ Figure 16.11 Billings lateral radiograph showing slip. The image intensifier is used to delineate the joint and proximal femur. _Incision_ As pinning is performed percutaneously, the planned trajectory of the screw is marked in two planes using the image intensifier bearing in mind the course of important neurovascular structures. The entry point of the screw should not be distal to the lesser trochanter as this creates stress risers and increases the incidence of fracture. Preoperative marking also limits the number of guide wire passes necessary to achieve a satisfactory screw position, further decreasing the chance of guide wire misplacement and minimising the risk of fracture. Because the epiphysis is relatively posterior and inferior to the neck, a more anterior entry point is required. Optimal screw position should avoid the posterior neck and posterior superior epiphysis to preserve the blood supply to the femoral head and minimise the risk of avascular necrosis. _Dissection_ Tissues are dissected bluntly down to bone. _Procedure_ A guide wire is passed under image intensifier control to avoid malposition and joint penetration. After measuring and over-drilling the wire, a partially threaded 6.5–7.5 mm diameter cannulated screw is inserted. A reverse cutting thread is used for easier subsequent removal. Despite an increase in shear strength across the physis using multiple screws, the use of a single screw diminishes the risk of chondrolysis and avoids the disproportionate complication rate of multiple screws. The passage of guide wire, drill and screw should be performed under image guidance to avoid joint penetration. The screw tip should reach the centre of the epiphysis, 5 mm from the articular surface with a minimum of three to four threads crossing the physis to provide adequate fixation. At completion, live screening of the hip is performed to ensure solid fixation of the epiphysis and confirm screw position. _Closure_ Subcuticular absorbable material is used to close the stab incision. Postoperative instructions Range-of-motion exercises are begun on the first postoperative day. Mobilisation is then: [View Source / PubMed]
- 76. Fully weightbearing with crutches for 2–3 weeks if slip is stable [View Source / PubMed]
- 77. Partial weightbearing until healed if unstable Assessment is carried out at 6–8 weeks for clinical and radiological evidence of union and to ensure that there has not been any further slip. Sporting activities are prohibited until physeal closure occurs. Following physeal closure, screw removal is recommended. Recommended references Givon U, Bowen JR. Chronic slipped femoral epiphysis: Treatment by pinning _in situ_. _J Pediatr Orthop B_. 1999;8:216–222. Loder RT, Aronson DD, Dobbs MB et al. Slipped capital femoral epiphysis. _Instr Course Lect_. 2001;50:555–570. Loder RT, Richards BS, Shapiro PS et al. Acute slipped capital femoral epiphysis. The importance of physeal stability. _J Bone Joint Surg Am_. 1993;75:1134–1140. Phillips SA, Griffiths WEG, Clarke NMP. The timing and reduction of the acute unstable slipped upper femoral epiphysis. _J Bone Joint Surg Br_. 2001;83:1046–1049. [Slipped upper femoral epiphysis: Osteotomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark15) An open reduction with osteotomy serves to restore the head-neck angle with subsequent improvement in hip biomechanics. This aims to provide good future function, minimise or delay the onset of painful secondary degeneration, and normalise proximal femoral anatomy for future hip replacement. Osteotomy can be performed at various levels (intracapsular and extracapsular neck, intertrochanteric and subtrochanteric) with greater correction achievable at the site of deformity (more proximally). Although these proximal osteotomies have been associated with a greater risk of avascular necrosis, a Dunn or Fish cuneiform osteotomy performed with meticulous technique, as described later, can achieve excellent results. Preoperative planning _Indications_ [View Source / PubMed]
- 78. Slip greater than 60° [View Source / PubMed]
- 79. Chronic/acute on chronic or unstable slip [View Source / PubMed]
- 80. Open physis _Contraindications_ Closed physis is a contraindication (Southwick intertrochanteric osteotomy may be more appropriate). _Consent and risks_ [View Source / PubMed]
- 1. _Avascular necrosis : 10%–48%_ [View Source / PubMed]
- 2. _Chondrolysis : 10%–12%_ [View Source / PubMed]
- 3. _Infection : Less than 1%_ [View Source / PubMed]
- 4. Slip progression [View Source / PubMed]
- 5. _LLD : 1–2 cm shortening_ [View Source / PubMed]
- 6. Further surgery (removal of hardware/complex arthroplasty) _Preoperative preparation_ Preoperative AP and lateral radiographs are used to confirm the degree of slip and plan orientation of the osteotomy. Slings and springs are used preoperatively for 3 weeks if acute or acute on chronic. _Anaesthesia and positioning_ [View Source / PubMed]
- 81. General anaesthesia [View Source / PubMed]
- 82. Intravenous antibiotic prophylaxis [View Source / PubMed]
- 83. Supine on radiolucent table [View Source / PubMed]
- 84. Image intensifier Surgical technique _Landmarks and approach_ The osteotomy is performed via an anterior approach (see ‘Developmental dysplasia of the hip: Open reduction’, p. 449). Particular care must be taken not to disturb the posterior capsule or forcefully manipulate the slip to preserve vascularity to the femoral head. _Procedure_ Following longitudinal capsulotomy, the epiphysis must be correctly identified as the anteriorly displaced neck may be mistaken for it. Two osteotomies are required: [View Source / PubMed]
- 85. First, an osteotomy is performed perpendicular to the neck at the level of the physis taking more anteriorly to create a wedge. The aim is to leave a convex surface for later reduction and shorten the neck by 3–4 mm. Over-shortening will lead to instability. Care must also be taken to avoid driving instruments into the posterior capsule, compromising the blood supply. [View Source / PubMed]
- 86. Second, an osteotomy is made in the long axis of the neck to remove the bony beak on the side of the slip, again taking care not to breach the posterior capsule. Any remaining callus is carefully removed with a spoon from the posterior capsule. Shortening the neck, removing the beak and elevating the posterior capsule allows tension-free reduction of the epiphysis. The epiphysis is reduced onto the neck by placing the leg in flexion, abduction and internal rotation. If insufficient bone has been removed, the epiphysis will not reduce easily, and posterior structures will be placed under tension increasing the risk of avascular necrosis. Shortening and wedging of the neck should cause the epiphysis to overlap the neck anteriorly giving a mushroom appearance. Restoration of the Shenton line and a valgus head-neck angle of 20° should be ensured using the image intensifier. While an assistant maintains position, a lateral stab incision is made according to the predicted trajectory of cannulated screw followed by blunt dissection down to the lateral cortex of the proximal femur. A guide wire is then advanced across the osteotomy to hold the epiphysis. Images are checked in two planes to confirm a satisfactory position before definitive screw insertion. Similar to pinning _in situ,_ the entry point should not be below the lesser trochanter, and screw tips should be 5 mm short of the articular surface. Dynamic screening allows confirmation of both a solid fixation and satisfactory positioning of hardware. _Closure_ [View Source / PubMed]
- 87. Layered closure including capsular repair with absorbable material [View Source / PubMed]
- 88. Subcuticular absorbable material to skin Postoperative instructions [View Source / PubMed]
- 89. Bed rest with slings and springs for 5 days [View Source / PubMed]
- 90. Mobilise 15 kg weightbearing 8 weeks; increase weightbearing status at 8 weeks, after confirming union clinically and radiographically Recommended references Dunn DM, Angel JC. Replacement of the femoral head by open operation in severe adolescent slipping of the upper femoral epiphysis. _J Bone Joint Surg Br_. 1978;60:394–403. Fish JB. Cuneiform osteotomy of the femoral neck in the treatment of slipped capital femoral epiphysis. _J Bone Joint Surg Am_. 1984;66:1153–1168. Loder RT. Unstable slipped capital femoral epiphysis. _J Pediatr Orthop_. 2001;21:694–699. Vanhegan IS, Cashman JP, Buddhdev P, Hashemi-Nejad A. Outcomes following subcapital osteotomy for severe slipped upper femoral epiphysis. _Bone Joint J_. 2015;97–B**(** 12**)** :1718–1725. [Tendo-Achilles lengthening](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark17) Preoperative planning Various methods for tendo-Achilles lengthening (TAL) exist and may be used in conjunction with other procedures. Percutaneous methods such as the Hoke and DAMP (distal anterior, medial proximal; also called a White slide) technique and open methods such as the Baker and Vulpius techniques are described ([Figures ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark46)16.12 [through ](#bookmark48)16.14). The choice depends on the cause, the individual patient and the surgeon’s preference.   Figure 16.14 Two techniques of gastrocnemius recession: (a) Baker slide and (b) Vulpius technique. _Indications_ [View Source / PubMed]
- 91. Fixed equinus deformity is defined as an inability to dorsiflex the ankle sufficiently to allow heel contact without compensation in the remainder of the limb or spine. Often, this correlates with dorsiflexion less than 5° and is seen in various conditions such as cerebral palsy, congenital talipes equinovarus (CTEV), congenital vertical talus, Charcot-Marie-Tooth (CMT), pes planus and intractable toe walkers. [View Source / PubMed]
- 92. Failure of conservative treatment. [View Source / PubMed]
- 93. To achieve stump coverage during Chopart’s amputation for congenital malformation of the foot. _Contraindications_ [View Source / PubMed]
- 94. Rigid bony deformity. [View Source / PubMed]
- 95. Pseudoequinus: A false clinical appearance of equinus caused by plantarflexion of the mid- and forefoot (plantaris deformity). [View Source / PubMed]
- 96. Medical co-morbidity is not a contraindication as percutaneous techniques can be performed under local anaesthesia. _Consent and risks_ [View Source / PubMed]
- 97. The most predictable outcome following TAL is in patients with spastic hemiplegia. The least predictable scenario is seen with percutaneous procedures in patients with diplegia. The two most frequently encountered problems are over-lengthening and recurrence. The former tends to occur following percutaneous procedures on the conjoined tendon, whereas recurrence is associated with recession of the gastrocnemius or soleus aponeurosis. [View Source / PubMed]
- 98. _Neurovascular damage : The sural nerve in particular is at risk._ [View Source / PubMed]
- 99. _Percutaneous techniques : 1%._ [View Source / PubMed]
- 100. _Open techniques : 5%._ [View Source / PubMed]
- 101. Plaster immobilisation/limited mobility. [View Source / PubMed]
- 102. Complete tendon rupture (percutaneous). [View Source / PubMed]
- 103. Wound problems/infection (open): 1%. [View Source / PubMed]
- 104. _Recurrence(Baker and Vulpius): Less than 5%._ [View Source / PubMed]
- 105. _Over-lengthening leading to crouchedgait : More likely following percutaneous procedures and associated with uncontrolled lengthening in an older child._ [View Source / PubMed]
- 106. _Repeat lengthening : More likely in a younger child and patients with hemiplegia._ [View Source / PubMed]
- 107. _Further surgery(hamstring, psoas or selective gastrocnemius lengthening most often required in patients with diplegia)._ _Preoperative assessment_ Silverskiold test under anaesthetic differentiates between pure gastrocnemius tightness (increased ankle dorsiflexion with knee flexion) and combined tightness of gastrocnemius and soleus (limited dorsiflexion in knee flexion and extension). _Anaesthesia and positioning_ [View Source / PubMed]
- 108. General anaesthesia or local anaesthesia for percutaneous techniques [View Source / PubMed]
- 109. Prone for open or supine for percutaneous techniques [View Source / PubMed]
- 110. High pneumatic thigh tourniquet Surgical technique _Percutaneous techniques_ Both Hoke and DAMP procedures are used to treat combined gastrocnemius-soleus tightness. The advantages are improved healing and the option of local anaesthesia. However, these techniques are associated with an increased incidence of over-lengthening and inadvertent complete tenotomy. _Hoke technique_ _Structures at risk_ [View Source / PubMed]
- 1. Tibial nerve – at risk proximally [View Source / PubMed]
- 2. Sural nerve – laterally [View Source / PubMed]
- 3. Flexor hallucis longus muscle – distally [Three points are marked on the tendo-Achilles at 1 cm, 3 cm and 6 cm from its calcaneal insertion. A number 15 blade scalpel is inserted longitudinally in the midline of the tendon at each marked level and then turned through 90° in the desired direction to perform the hemisection while the ankle is dorsiflexed to control the correction. The hemisections are performed on the medial half proximally and distally and the lateral half in the middle incision (see](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark46)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark46)16.12). _DAMP technique_ Two 1.5 cm skin incisions are made postero-medially, one 2 cm from the calcaneal insertion and another 5 cm proximal to it. The anterior two-thirds of the tendon is divided distally and the medial half to two-thirds proximally. (This is because of the 90° rotation of tendon fibres in the distal third of the leg.) [The tendon is divided progressively while tensioning the tendo-Achilles until it yields 5°–10° of dorsiflexion. The medial fibres slide over the lateral fibres, giving length in continuity with a thinned portion of tendon distally and a square cut proximally (see](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark47)Figure 16.13). Open techniques These have the advantage of controlled lengthening but carry a greater risk of recurrence. _Incision_ _Structures at risk_ [View Source / PubMed]
- 1. Sural nerve [View Source / PubMed]
- 2. Short saphenous vein A 7 cm longitudinal incision is made, 10 cm proximal to the calcaneal insertion positioned 1 cm medial to the midline to avoid the sural nerve. _Dissection_ The sural nerve and short saphenous vein are retracted if encountered or may be avoided altogether by raising a full-thickness lateral flap. The paratenon is incised longitudinally in the midline to avoid the skin incision, and the medial and lateral edges of the gastrocnemius aponeurosis are exposed. Baker slide procedure Although considered a selective gastrocnemius lengthening, fibres of the soleus aponeurosis are also incised distally. However, this does not lead to over-lengthening as seen in procedures on the conjoined tendon owing to controlled lengthening and inherent stability. [The medial and lateral thirds of the aponeurosis are incised transversely 12 cm above the calcaneal insertion. A similar incision is then performed across the middle third at least 3 cm proximally to allow side-to-side contact after lengthening. A tongue and groove pattern is created by joining the proximal and distal cuts with two longitudinal incisions (see](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark48)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark48)16.14). Dorsiflexion of the ankle allows slide-lengthening of the aponeurosis and reveals any remaining fibres that require incision. The underlying muscle fibres of soleus are revealed as the aponeurosis is lengthened. Further lengthening should not be performed once 10° of dorsiflexion is achieved on the table, and 3/0 absorbable sutures are placed across the longitudinal portions of the aponeurosis. Vulpius procedure [This is used to treat combined gastrocnemius-soleus tightness when plaster immobilisation is not desirable. Instead of a tongue and groove lengthening, an inverted ‘V’ incision is made in the aponeurosis of both the gastrocnemius and the soleus (see](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark48)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark48)16.14). _Closure_ [View Source / PubMed]
- 111. Tension-free layered closure with buried knots to avoid skin irritation [View Source / PubMed]
- 112. Subcuticular absorbable material to skin With the exception of the Vulpius technique, a below-knee plaster is applied in a plantigrade position. A dorsiflexed position must be avoided to prevent a calcaneus deformity. Postoperative instructions Mobilise weightbearing as tolerated in cast for 4 weeks if used. Convert to night-time splint at 4 weeks and continue for 6 months. Use guided physiotherapy to maintain position and prevent recurrence. Recommended references Baker LD. Surgical needs of the cerebral palsy patient. _J Bone Joint Surg Am_. 1956;38:313–323. Borton DC, Walker K, Pirpiris M et al. Isolated calf lengthening in cerebral palsy. _J Bone Joint Surg Br_. 2001;83:364–370. Graham HK, Fixsen JA. Lengthening of the calcaneal tendon in spastic hemiplegia by the white slide technique. _J Bone Joint Surg Br_. 1988;70:472–475. [Congenital talipes equinovarus correction](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark19) Ponseti technique Preoperative planning _Indications_ Flexible CTEV _Contraindications_ [View Source / PubMed]
- 113. Rigid clubfoot [View Source / PubMed]
- 114. Age over 7 years is a relative contraindication as results are notably worse _Consent and risks_ [View Source / PubMed]
- 1. Neurovascular injury (any open procedure) [View Source / PubMed]
- 2. Complete Achilles tenotomy [View Source / PubMed]
- 3. Plaster impingement/skin ulceration [View Source / PubMed]
- 4. Infection (open procedures) [View Source / PubMed]
- 5. Stiffness [View Source / PubMed]
- 6. Recurrent deformity: Long-term splintage required [View Source / PubMed]
- 7. Deformity due to incorrect or incomplete correction, overcorrection or recurrence, e.g. cavus, rocker-bottom, longitudinal breach, flattening and lateral rotation of talus [View Source / PubMed]
- 8. 1 cm limb shortening, 2 cm decreased calf girth and smaller shoe by one or half sizes are common sequelae Do not expect a completely normal foot; although the Ponseti technique yields good clinical results, foot malformations still exist and can be seen radiographically. _Operative planning_ The deformity can be graded using various methods. Dimeglio suggests a 20-point scoring system with four grades of severity which correlates with an increasing resistance to correction. The Pirani score helps to predict the need for Achilles tenotomy and is based upon the severity of deformity in the midfoot and hindfoot with a total maximum score of 6\. Eighty-five per cent of patients with scores over 5 will require tenotomy. _Anaesthesia and positioning_ No anaesthesia or sedation required unless the patient is extremely uncooperative. An assistant is essential. Surgical technique Casting is performed weekly, correcting all three components of the deformity in a predetermined sequence prior to additional operative procedures. At least three toe-to-groin casts are required over a period of 7–10 weeks depending on the severity of deformity. _Castings_ [View Source / PubMed]
- 1. _Cavus : Caused by a relative pronation of the forefoot due to a plantarflexed first ray. The first ray is elevated with pressure beneath the first metatarsal head to supinate the forefoot and align it with the varus hindfoot. Forced pronation of the foot is avoided as this will worsen the cavus._ [View Source / PubMed]
- 2. _Varus and adductus : Correction of the abnormally internally rotated calcaneus is achieved by external rotation using the lateral talar head as the fulcrum. The cuboid and anterior calcaneus are displaced laterally by applying medial pressure to the navicular anterior to the ankle and pushing the posterior calcaneus medially by lateral pressure posterior to the ankle, ensuring the talar head does not externally rotate. In severe cases, the navicular may not fully reduce although abduction of the cuneiforms more distally will allow correction and the navicular-cuneiform joints will remodel. Once the calcaneocuboid alignment is restored with the anterior calcaneus lateralised, correction of varus can be achieved. The cast must be toe to groin with the knee in_ 90° of flexion to maintain abduction and external rotation. This will also treat any associated internal tibial torsion if present. Midfoot pronation must again be avoided to prevent cavus deformity and a midfoot breach. [View Source / PubMed]
- 3. _Equinus : With the hindfoot varus corrected, serial casts are applied in a progressively dorsiflexed position. This usually requires two to three casts to achieve 15° of dorsiflexion and 60° of external rotation. Dorsiflexion is achieved via pressure beneath the midfoot rather than the metatarsals to avoid rocker-bottom feet._ _Additional procedures_ _Tendo-Achilles lengthening : If dorsiflexion of 15° is not achieved, then a percutaneous tenotomy under local anaesthesia is indicated. This is preferable to posterior ankle and subtalar capsulotomy as contraction of scar tissue in this region will lead to progressive loss of dorsiflexion._ Lateral transfer of the tibialis anterior tendon to the lateral cuneiform may be required for persistent supination. Postoperative care and instructions The final cast is left _in situ_ for 3 weeks and then assessment made for residual equinus; 90% of patients will require Achilles tenotomy. Denis Browne boots are worn full time for 2–3 months then at night only for 2–4 years or until age 7 years. These maintain 15° of dorsiflexion (to avoid equinus) and 60° external rotation (to prevent varus, adductus and in-toeing). High-top shoes are worn during the day to maintain position. Periodic evaluation should be performed by an experienced clinician to assess the relationship between the hindfoot and forefoot, the attitude of the heel and range of ankle motion. Anteroposterior and lateral radiographs should also be obtained. Extensive soft tissue release via the Cincinnati incision Preoperative planning _Indications_ [View Source / PubMed]
- 4. Failed Ponseti treatment: 50% may relapse at an average age of 2.5 years. Remanipulation and casting with or without Achilles tenotomy followed by splintage may be successful although extensive soft tissue releases are required in resistant cases. [View Source / PubMed]
- 5. Rigid clubfoot. [View Source / PubMed]
- 6. Walking on lateral border of foot/internally rotated gait. [View Source / PubMed]
- 7. Posteriorly placed lateral malleolus (a reflection of uncorrected internal calcaneal rotation). [View Source / PubMed]
- 8. Parallelism of talus and calcaneus on AP and lateral radiographs. _Contraindications_ Contraindications include previous releases via alternative incisions. _Consent and risks_ [View Source / PubMed]
- 1. Neurovascular damage (see later) [View Source / PubMed]
- 2. Plaster immobilisation/impaired mobility/long-term splintage [View Source / PubMed]
- 3. Residual deformity [View Source / PubMed]
- 4. Recurrence and further surgery [View Source / PubMed]
- 5. Wound irritation over the Achilles tendon, particularly rubbing on shoes [View Source / PubMed]
- 6. Avascular necrosis of the talus [View Source / PubMed]
- 7. Arthritis of the hindfoot and midfoot [View Source / PubMed]
- 8. Ankle and subtalar stiffness _Preoperative assessment_ [View Source / PubMed]
- 9. AP and lateral radiographs required for assessing the talocalcaneal angle [View Source / PubMed]
- 10. Dimeglio and Pirani scores _Anaesthesia and positioning_ General anaesthesia is used with addition of an intravenous prophylactic antibiotic. The patient is positioned prone with a high thigh tourniquet. Surgical technique _Landmarks_ The base of the first metatarsal, medial malleolus and lateral malleolus is palpable. _Incision (the Cincinnati incision)_ An 8–9 cm extensile, transverse incision across the posterior ankle (at the level of the tibio-talar joint) is created. This begins at the base of the first metatarsal, curves below the medial malleolus, rises slightly to traverse the Achilles tendon and continues over the lateral malleolus to terminate distal and medial to the sinus tarsi. _Superficial dissection_ _Structures at risk_ [View Source / PubMed]
- 1. Sural nerve laterally [View Source / PubMed]
- 2. Superficial venous structures below the lateral malleolus The proximal subcutaneous flap is raised off underlying tissues for around 3 cm to allow proximal visualisation. _Deep dissection_ _Structures at risk_ [View Source / PubMed]
- 1. Posterior tibial nerve and vessels [View Source / PubMed]
- 2. Deep tibiotalar portion of the deltoid ligament [View Source / PubMed]
- 3. Medial and lateral plantar nerves This begins laterally with incision of the calcaneofibular ligament and superior peroneal ligament to allow dissection of the peronei off the calcaneus without damaging them. The lateral talocalcaneal ligament and lateral capsule of subtalar joint are then released. The posterior tibial neurovascular bundle is retracted anteriorly to allow further release of the posterior ankle and subtalar capsule and the posterior talofibular ligament. Subsequent posterior retraction of the tibial neurovascular bundle allows division of the superficial tibiocalcaneal part of deltoid. The deep portion of the tibiotalar portion of the deltoid ligament is left intact to prevent excessive subtalar translation and flat foot deformity. The tibialis posterior tendon sheath is opened along its length from above the medial malleolus to the navicular to allow Z-lengthening of the tendon at least 2.5 cm proximal to the medial malleolus. The nearby posterior tibial neurovascular bundle is protected to avoid its transection. Dissection continues medially, into the arch of the foot, to release the lacinate ligament, the plantar aponeurosis and small plantar muscles, including abductor hallucis. Beneath the navicular, the master knot of Henry (intersection of the flexor hallucis longus [FHL] and flexor digitorum longus [FDL]) is taken down, taking care not to damage the medial and lateral plantar nerves on either side of it. The sheaths of the FDL and FHL are opened and tendon Z-lengthening performed to prevent flexion contracture of the toes when the ankle is dorsiflexed. This is done sufficiently proximally to allow the lengthened portions to be covered by tendon sheath. Conjoint lengthening is an alternative if the tendons are too small to perform Z-lengthening. This step may be unnecessary as toe contractures will often stretch out over time. The talonavicular joint is freed to mobilise the navicular laterally and release all of its attachments; keeping hold of it via the distal end of tibialis posterior tendon will avoid handling the articular cartilage. The dorsal talonavicular ligament and the spring ligament can then be released. Release of the bifurcate ligament and the talocalcaneal interosseous ligament will allow external rotation of the anterior calcaneus. Finally, the quadratus plantae is stripped off the calcaneus to release the long plantar ligament, the plantar calcaneocuboid ligament and inferior medial capsule of the calcaneocuboid joint without damaging the peroneus longus tendon. The extensive soft tissue releases should result in the plane of the foot being at 90° to the bimalleolar axis with the talus beneath the tibia and slight hindfoot valgus. If the mortise is not fully reduced, tibiofibular ligament release then tibiofibular syndesmosis release can be carried out if the talus is too wide anteriorly. Stabilisation with K-wires is the final stage, one passing along the medial column to hold the talonavicular joint and one across the lateral column to hold the calcaneocuboid joint. _Closure_ Tendon sheaths over all over-lengthened tendons are closed. The medial and lateral extensions of the Cincinnati incision are closed, without tension, using absorbable sutures to the subcutaneous and subcuticular layers. The posterior, central portion of the wound is left open to heal by secondary intention. If blanching of wound edges following tourniquet release is noted, position in less dorsiflexion. Apply plaster of Paris from the toes to the mid-thigh with a neutral or slightly plantarflexed foot and the knee flexed to 90°. Postoperative care and instructions The cast is changed at 10 days after surgery, to inspect the wound. It is removed, along with the K-wires, at 6 weeks. Denis Browne boots are prescribed for the next 12–18 months. Physiotherapy (for mobility, to promote tarsal growth and preserve cartilage) is continued for at least 6 months. Recommended references Crawford AH, Marxen JL, Osterfield DL. The Cincinnati incision: A comprehensive approach for surgical procedures of the foot and ankle in childhood. _J Bone Joint Surg Am_. 1982;84:1355–1358. Dimeglio A, Benshahel H, Souchet P et al. Classification of clubfoot. _J Pediatr Orthop B_. 1995;4:129–136. McKay DW. New concept of and approach to clubfoot treatment: section II – Correction of the clubfoot. _J Pediatr Orthop. 1983;3:10–21._ Pirani J, Outerbridge HK, Sawatzky B et al. A reliable method of clinically evaluating a virgin clubfoot. _21st World Congress of SICOT , Sydney, Australia, 18–23 April 1999._ Ponseti I. _Congenital Clubfoot: Fundamentals of Treatment_. New York, NY: Oxford University Press, 1996. [Surgical treatment of Perthes disease](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark21) Perthes disease occurs as a result of a temporary cessation in the blood supply to the femoral head leading to avascular necrosis. It is commonly seen between the ages of 4 and 8 years although should be suspected from 2 to 12 years of age. Although more common in boys by a factor of four, it may be more severe in girls. Presenting symptoms comprise hip or referred knee pain, stiffness, limping and a short leg. The disease progresses through the four phases of ischaemia (causing collapse and sclerosis), fragmentation, reossification and remodelling, which take place over a 4-year period. However, development of the hip is frequently abnormal leading to incongruency, altered biomechanics and accelerated secondary degeneration. Prognosis is dependent on age and severity of disease at presentation, and treatment falls into the three broad categories of observation, containment and salvage, depending also on the phase of disease. Preoperative planning _Indications_ The type of treatment largely depends upon the capacity to remodel and therefore age. Below the age of 6 years, there is high potential for remodelling, and therapy therefore tends to be conservative. Above 8 years, further remodelling is limited and treatment is more aggressive in order to correct deformity and extend the longevity of the native hip. Between the ages of 6 and 8 years, the indications for either a conservative approach or containment procedures depend upon bone age and remodelling potential, the presence of ‘at-risk’ signs for the viability of the femoral head and whether the hip is congruent or containable. The surgical options for containable hips are a varus osteotomy of the proximal femur and/or a Salter-type pelvic osteotomy. [Salvage procedures are indicated if hinge abduction occurs (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark51)[Figure ](#bookmark51)16.15), where the overgrown and uncontained anterolateral portion of the femoral head abuts the lateral rim of the acetabulum. In this situation valgus extension osteotomy (VGEO) of the proximal femur is indicated, which will medialize the centre of rotation of the hip and make it congruent in the weightbearing position. The medial column must be of sufficient height after reossification and a better outcome is expected in younger patients where the   Figure 16.15 Hip arthrogram showing hinge abduction, where dye pools medially in abduction. triradiate cartilage remains open. This will allow deformity correction, a better functional range of movement, improvement of leg length and abductor function. _Contraindications_ Containment procedures are contraindicated if hips are not congruent or containable. _Consent and risks_ The natural history of the disease must be explained to the child and parents. It should be emphasised that the aim is to improve symptoms and to achieve a spherical and contained femoral head to maximise and prolong native joint function. However, secondary degenerative changes may continue to occur at an unpredictable and accelerated rate ultimately leading to total joint arthroplasty or arthrodesis. [View Source / PubMed]
- 1. An older presentation, particularly in girls, is associated with a worse outcome. [View Source / PubMed]
- 2. Stiffness/contractures. [View Source / PubMed]
- 3. Other risks pertain to the type of procedure being performed. See the relevant sections on DDH for the risks associated with pelvic and femoral osteotomies. _Operative planning_ Various classification systems exist to guide treatment and predict the prognosis of Perthes disease. Catterall grouped patients as I-IV, although large intra- and inter-observer error has been shown with this method. The Herring classification correlates with prognosis according to the degree of collapse of the lateral capital femoral epiphysis during the fragmentation phase using the AP radiograph of the pelvis. The Stulberg classification (1–5) is made during the reossification phase and predicts the end result of Perthes disease dependent on the relative shapes of the femoral head and acetabulum. Increasing grade correlates with the likelihood of secondary osteoarthritis with Stulberg 5 hips likely to require total hip replacement before age 50 years. Head at-risk signs include Gage’s sign (a lytic ‘rat bite’ at the periphery of the physis), calcification lateral to the epiphysis, lateral subluxation of the femoral head and horizontal inclination of the physis. [Arthrography will determine the congruency of the hip in various positions and whether an appropriate range of movement is possible to perform the relevant femoral osteotomy (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark51)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark51)16.15). Significant abduction is required for a varus osteotomy and adduction for a valgus osteotomy. _Anaesthesia and positioning_ [View Source / PubMed]
- 1. General anaesthesia [View Source / PubMed]
- 2. Supine [View Source / PubMed]
- 3. Intravenous prophylactic antibiotics Surgical technique [View Source / PubMed]
- 4. For varus osteotomy, the technique as described in the section ‘Developmental dysplasia of the hip: Proximal femoral osteotomy’ (p. 456) is used, employing the derotation component if required. [View Source / PubMed]
- 5. For valgus osteotomy, a similar technique is used as for varus osteotomy, the difference being the orientation of the osteotomy to give a laterally based wedge to achieve the desired realignment. [View Source / PubMed]
- 6. Pelvic osteotomy (see ‘Salter osteotomy’, p. 452). Postoperative instructions Instructions are as per the type of procedure performed. Regular periodic clinical and radiographic review is required to determine the presence of deterioration and the need for further surgery. Recommended references Bankes MJK, Catterall A, Hashemi-Nejad A. Valgus extension osteotomy for ‘hinge abduction’ in Perthes disease: Results at maturity and factors influencing the radiological outcome. _J Bone Joint Surg Br_. 2000;82:548–554. Catterall A. The natural history of Perthes disease. _J Bone Joint Surg Br_. 1971;53:37–53. Coates CJ, Paterson JMH, Catterall A et al. Femoral osteotomy in Perthes disease. Results at maturity. _J Bone Joint Surg Br_. 1990;72:581–585. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease. Part I: Classification of radiographs with use of the modified lateral pillar and Stulberg classifications. _J Bone Joint Surg Am_. 2004;86:2103–2120. Herring JA, Kim HT, Browne R. Legg-Calvé-Perthes disease. Part II: Prospective multicentre study of the effect of treatment on outcome. _J Bone Joint Surg Am_. 2004;86:2121–2134. [Principles of surgery in cerebral palsy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark23) Preoperative planning Cerebral palsy results from an insult to the immature brain and its effects are variable. It may be classified anatomically (hemiplegic, diplegic or total body involvement) or physiologically (spastic, athetoid, ataxic or mixed). The spastic form is most common; a combination of muscle weakness and spasticity leads to a progressive sequence of dynamic deformity, fixed contractures, bony deformity and joint subluxation or dislocation. Depending on the severity, intervention may be indicated at any point during this continuum to optimise energy consumption during gait, to perform activities of daily living, to facilitate standing or seated transfer and to maintain hygiene. Maximum function requires a straight spine over a level pelvis, congruent, mobile hips, mobile knees and plantigrade feet. Cerebral palsy is typically treated in one of three phases: [View Source / PubMed]
- 7. Dynamic contractures: Casting and/or botulinum toxin (BTX) injection [View Source / PubMed]
- 8. Fixed contractures: Muscle balancing techniques such as releases, lengthening and transfers [View Source / PubMed]
- 9. Bony deformity and joint incongruence: Osteotomies Decisions around timing of surgery are difficult. Allowing maturation will improve certainty about the gait pattern and reduce the risk of recurrent deformity at the price of an increased chance of fixed deformities and multilevel operations being required. Surgery in the younger child may be less technically demanding but can lead to repeat surgery year on year. In addition, single-level operations may reveal further problems: a common example is a crouched gait occurring after Achilles tendon release due to unrecognised, concomitant tight hamstrings. Throughout all stages, physiotherapy helps to reduce fixed deformity and occupational therapy can adapt equipment to accommodate existing deformity. Surgical techniques in muscle contractures _Botulinum toxin A injections_ BTX A inhibits the release of acetylcholine from the nerve terminal at the neuromuscular junction, causing decreased muscle activity in a dose-dependent manner. It may be administered under local or general anaesthesia or sedation. It should be placed deep to the muscle fascia in a dose appropriate for the patient and the number of injection sites required. The injection volume must be sufficient to allow diffusion to endplate zones which may be scattered, particularly in the sartorius and gracilis. Localise injection sites using palpation and anatomical knowledge; accuracy is improved with electrical stimulation or ultrasound guidance. Combine injection with casting, orthoses and guided physiotherapy to maximise the benefits. _Contraindications_ [View Source / PubMed]
- 10. Myasthenia gravis [View Source / PubMed]
- 11. Aminoglycoside antibiosis [View Source / PubMed]
- 12. Non-depolarizing muscle relaxants [View Source / PubMed]
- 13. Pseudobulbar palsy [View Source / PubMed]
- 14. Gastro-oesophageal reflux or frequent chest infections _Consent and risks_ [View Source / PubMed]
- 1. _Local : Pain, temporary weakness in adjacent muscles_ [View Source / PubMed]
- 2. _General : Mild generalised weakness, urinary incontinence, constipation, dysphagia and aspiration pneumonia_ Parents and patients should be warned of its temporary effect of 12–16 weeks and the risk of recurrence and further procedures. Surgical technique _Muscle balancing techniques_ Adductor psoas and gracilis release is commonly indicated for the classic flexion adduction contracture and scissoring gait seen in cerebral palsy. Muscle imbalance combined with infrequent weightbearing causes structural changes at the hip (increased anteversion, posterolateralacetabulardysplasia) leadingtoposterolateralmigration, pelvicobliquityand scoliosis. This is more commonly seen in quadriplegic patients and releases are performed early (3–4 years) to prevent deterioration. Muscles should be released sequentially during the procedure and performed bilaterally to prevent a windswept deformity. Releases are also commonly combined with proximal varus femoral osteotomy at age 5 years. Hamstrings may be released proximally or distally to improve flexion contracture at the knee. Equinus deformity at the ankle is very common and is treated with tendo-Achilles release (see section ‘Tendo-Achilles Lengthening’, p. 464 for details). Knee and ankle releases are performed in a walking child between 4 and 6 years old. Another common problem is the thumb in hand deformity treated with adductor pollicis release and is performed in the older child. Tendon transfers such as tibialis anterior or tibialis posterior are often used in balancing the foot in combination with bony surgery. Osteotomy and joint containment _Hip containment_ Quadriplegic patients should be monitored regularly for hip subluxation and dislocation, which tends to occur between 18 months and 6 years. Hips at risk are those with limited abduction with uncovering of less than 50% on radiography. At-risk hips may be treated with adductor, psoas and hamstring release although a more aggressive approach may be considered. Subluxed hips (>50% uncovered) are treated with soft tissue releases and varus proximal femoral osteotomy. Early dislocated hips may be treated with open reduction; however, this may not be possible and poor conformity between the head and acetabulum may lead to early failure. A varus derotational osteotomy with soft tissue releases and/or shortening may be more appropriate. This can be combined with pelvic osteotomy. Late dislocations require either resurfacing or total joint arthroplasty; a large articulation is preferred to confer stability. Alternatively, a Girdlestone excision arthroplasty may be considered. _Triple arthrodesis of the ankle_ Various foot and ankle deformities are seen in cerebral palsy such as planovalgus, equinovalgus, equinovarus and calcaneovalgus. Triple arthrodesis is indicated for symptomatic degeneration and uncontrolled deformity. Despite frequent complications such as residual deformity, pseudarthrosis, pain and progressive intertarsal and tarsometatarsal arthritis, the response to surgery is good. _Scoliosis surgery_ Scoliosis is more common in quadriplegic and non-ambulatory diplegic patients. The risk of progression is related to age at presentation and hip problems. Curves are likely to reach 50° if present by age 5. Bracing is seldom preventive. Nutrition must be optimised preoperatively, and patients must be monitored closely postoperatively for respiratory complications. Indications for surgery are curves greater than 40° or progression greater than 10° per annum. Ambulatory patients receive posterior fusion, whereas non-ambulatory patients require additional anterior fusion and pelvic fixation. Recommended references Gage JR. _The Treatment of Gait Problems in Cerebral Palsy_. Cambridge, United Kingdom: Cambridge University Press, 2004. McCarthy JJ, D’andrea LP, Betz RR et al. Scoliosis in the child with cerebral palsy. _J Am Acad Orthop Surg_. 2006;14:367–375. Owers KL, Pyman J, Gargan MF et al. Bilateral hip surgery in severe cerebral palsy. _J Bone Joint Surg Br_. 2001;83:1161–1167. Ramachandran M, Eastwood DM. Botulinum toxin and its orthopaedic applications. _J Bone Joint Surg Br_. 2006;88:981–987. Skoff H, Woodbury DF. Management of the upper extremity in cerebral palsy. _J Bone Joint Surg Am_. 1985;67:500–503. [Guided growth: Temporary hemiepiphysiodesis](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark25) Preoperative planning Temporary hemiepiphysiodesis aims to produce a differential growth rate across a physis to allow correction of angular deformities. Several methods have been described to achieve this aim, including use of staples (Blount), percutaneous transphyseal screws (Metaizeau), or more recently the use of a two-hole tension band plate (e.g. 8-plate or Pediplate). This technique is most frequently used for coronal deformities about the knee, although use about other physes has been described. _Indications_ Coronal plane deformity with an abnormal periarticular angle leading to abnormal/ worsening mechanical axis alignment. Occasionally can be considered for correction of sagittal plane deformity (e.g. fixed knee flexion, as an alternative to capsular release). _Contraindications_ [View Source / PubMed]
- 15. Active infection [View Source / PubMed]
- 16. Untreated metabolic/nutritional cause for deformity ‘sick physis’ [View Source / PubMed]
- 17. Insufficient remaining growth [View Source / PubMed]
- 18. Non-compliance with follow-up [View Source / PubMed]
- 19. Partial growth arrest _Consent and Risks_ [View Source / PubMed]
- 1. Neurovascular injury [View Source / PubMed]
- 2. Infection [View Source / PubMed]
- 3. Fracture [View Source / PubMed]
- 4. Physeal injury/growth arrest [View Source / PubMed]
- 5. Over-/undercorrection [View Source / PubMed]
- 6. Implant failure _Operative planning_ Standardised long leg radiographs should be used for planning with leg lengths corrected using blocks and the patellae pointing forwards. Periarticular angles should be calculated to identify the location of the deformity. The tension band plate should be applied on the convexity of the deformity. Angular correction may be achieved at an average of 0.7° per month at the distal femoral physis and 0.5° per month at the proximal tibia. Surgical technique _Anaesthesia and positioning_ General anaesthesia is used with intravenous antibiotic prophylaxis. The patient is positioned supine on a radiolucent table with a thigh tourniquet. A sandbag or leg holder can be used to ensure the patella is pointing upwards. _Procedure_ An image intensifier is used to position a 3 cm incision centred at the level of the physis in the coronal and sagittal planes. Sharp dissection is performed down to, but not through the periosteum. The guide wire is placed approximately 1 cm into the physis and the position checked on AP and lateral radiographs, ensuring that a true lateral view is obtained. A suitably sized two-hole plate is passed down the guide wire and positioned, ensuring it is rotated to lie perpendicular to the physis on the lateral view. Two guide wires are placed through the centre of each hole to check the screw will not penetrate the physis or the joint. A cannulated drill is used to open the cortex and a screw is placed in each hole, either side of the physis. The guide wires are removed prior to final seating of the screws. _Closure_ A layered closure is used, using absorbable subcuticular material to skin. Postoperative instructions [View Source / PubMed]
- 20. Full weightbearing is permitted immediately with crutches for comfort. [View Source / PubMed]
- 21. Radiographs are performed at 3 months and then at regular intervals to monitor correction. [View Source / PubMed]
- 22. Implant removal is required once correction has been achieved to prevent overcorrection. Recommended references Ballal MS, Bruce CE, Nayagam S. Correcting genu varum and genu valgum in children by guided growth: Temporary hemiepiphysiodesis using tension band plates. _J Bone Joint Surg Br_. 2010;92(2):273–276. Blount WP, Clarke GR. Control of bone growth by epiphyseal stapling: A preliminary report. _J Bone Joint Surg [Am]_. 1949;31–A:464–478. Metaizeau JP, Wong-Chung J, Bertrand H, Pasquier P. Percutaneous epiphysiodesis using transphyseal screws (PETS). _J Pediatr Orthop_. 1998;18**(** 3**)** :363–369. Stevens PM. Guided growth for angular correction: A preliminary series using a tension band plate. _J Pediatr Orthop_. 2007;27:243–259. _[Viva questions_ ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/16.%20Paediatric%20Orthopaedic%20Surgery_Converted.html#bookmark26) [View Source / PubMed]
- 1. What are the clinical signs of hip instability in the newborn? [View Source / PubMed]
- 2. What are Hilgenreiner and Perkins lines, and what is their relevance? [View Source / PubMed]
- 3. What are the relative advantages and disadvantages of the anterior and medial approaches to the paediatric hip in developmental dysplasia of the hip? [View Source / PubMed]
- 4. Describe the Smith-Petersen approach to the paediatric hip? [View Source / PubMed]
- 5. What are the indications for varus proximal femoral osteotomy in developmental dysplasia of the hip? [View Source / PubMed]
- 6. How does a varus proximal femoral osteotomy affect range of hip movement and leg lengths? [View Source / PubMed]
- 7. What structures are at risk during a Salter pelvic osteotomy? [View Source / PubMed]
- 8. What are the indications and contraindications of the Pemberton pelvic osteotomy? [View Source / PubMed]
- 9. What is the ideal screw position when pinning a slipped upper femoral epiphysis? What risks are associated with this procedure? [View Source / PubMed]
- 10. What are the indications for prophylactic pinning of the contralateral hip in slipped upper femoral epiphysis? [View Source / PubMed]
- 11. How does the blood supply to the femoral head change throughout childhood? [View Source / PubMed]
- 12. What are the treatment options for avascular necrosis following slipped upper femoral epiphysis? [View Source / PubMed]
- 13. What is your approach to the treatment of Perthes disease in a 7-year-old child? [View Source / PubMed]
- 14. What classification systems do you know for grading the severity and predicting the prognosis of Perthes disease? [View Source / PubMed]
- 15. What are the component deformities of club foot, and which structures are tight? [View Source / PubMed]
- 16. Which structures are at risk during extensive soft tissue release of congenital talipes equinovarus via the Cincinnati approach? [View Source / PubMed]
- 17. How would you distinguish between a tight tendo-Achilles complex and gastrocnemius tightness? [View Source / PubMed]
- 18. What methods can you describe to determine when epiphysiodesis should be performed? [View Source / PubMed]
- 19. How much growth per year can be expected from each of the four main physes in the lower extremity in adolescence? [View Source / PubMed]
- 20. What is your approach to the orthopaedic assessment and treatment of the child with cerebral palsy? [View Source / PubMed]
