OVERGROWTH (MACRODACTYLY): PATHOLOGY AND PRINCIPLES
Macrodactyly is an exceptionally rare congenital anomaly characterized by the profound, disproportionate enlargement of a digit or multiple digits. According to seminal epidemiological data by Flatt, macrodactyly was identified in only 19 of 1,476 patients presenting with congenital hand anomalies, representing an incidence of merely 0.9%. The condition exhibits a strong predilection for the index finger, followed by the middle finger and thumb, corresponding primarily to the median nerve distribution.
Unlike many congenital hand differences, macrodactyly does not demonstrate a clear Mendelian inheritance pattern. The precise etiology remains elusive, though contemporary orthopedic consensus strongly suspects the interplay of three primary factors:
1. Abnormal Nerve Supply: Hypertrophy of the digital nerves and excessive neural input.
2. Abnormal Blood Supply: Localized hypervascularity driving tissue hypertrophy.
3. Abnormal Humoral Mechanisms: Localized dysregulation of growth factors.
While some authors have historically postulated that macrodactyly represents a localized, aborted variant of neurofibromatosis (NF), the classic systemic manifestations of NF (e.g., café-au-lait spots, Lisch nodules) are typically absent in isolated macrodactyly patients. However, it is well-documented that a subset of patients with confirmed neurofibromatosis will develop secondary macrodactyly.
Clinical Presentation and Classification
Macrodactyly most commonly presents as an isolated condition, though syndactyly is a recognized associated anomaly in approximately 10% of cases. Involvement of both the hands and the feet has been documented by Keret, Ger, and Marks. Involvement is overwhelmingly unilateral, with multiple digits affected two to three times more frequently than a single digit.

Fig. 76-53 A and B, Macrodactyly of the index finger and thumb, demonstrating characteristic volar and distal soft-tissue hypertrophy.
Barsky’s classic taxonomy divides true macrodactyly into two distinct clinical entities based on growth velocity:
* Static Macrodactyly: The deformity is present at birth or early infancy. The digit is diffusely enlarged but grows in proportion to the child's normal digital growth.
* Progressive Macrodactyly: The digit may appear relatively normal or only slightly enlarged during infancy but begins to enlarge rapidly and disproportionately during early childhood. This aggressive form is frequently associated with severe angular deformities, rendering the finger "banana-shaped."
Clinical Pearl: In both static and progressive forms, the overgrowth is rarely symmetric. The distal and palmar (volar) tissues typically exhibit significantly more hypertrophy than the dorsal and proximal tissues. This volar-dominant overgrowth is the primary biomechanical driver of the characteristic dorsal extension and lateral angular deformities seen as the child grows.
Pathoanatomy and Late Complications
The pathoanatomy of macrodactyly involves the hypertrophy of all tissue layers—skin, subcutaneous fat, nerves, and bone—though some authors have noted relative sparing of the tendons and major blood vessels. The skin becomes markedly thickened, and the nails are often grossly hypertrophied. The phalanges are universally involved, and the metacarpals may also demonstrate enlargement.
The digital nerves innervating the affected territory are characteristically tortuous, thickened, and infiltrated with fibrofatty tissue. In a rare variant termed the hyperostotic variety by Kelikian, osteocartilaginous deposits form around the interphalangeal joints, which Schuind et al. suggested may have a traumatic etiology.
As the patient matures, the enlarged digit progressively loses range of motion due to joint incongruity and massive soft-tissue impingement. Later in life, the sheer volume of fibrofatty tissue within the rigid confines of the carpal canal frequently precipitates carpal tunnel syndrome, presenting with classic paresthesias and hypesthesias. Furthermore, the insensate, bulky digit is highly susceptible to trauma, often leading to recalcitrant trophic ulcers.
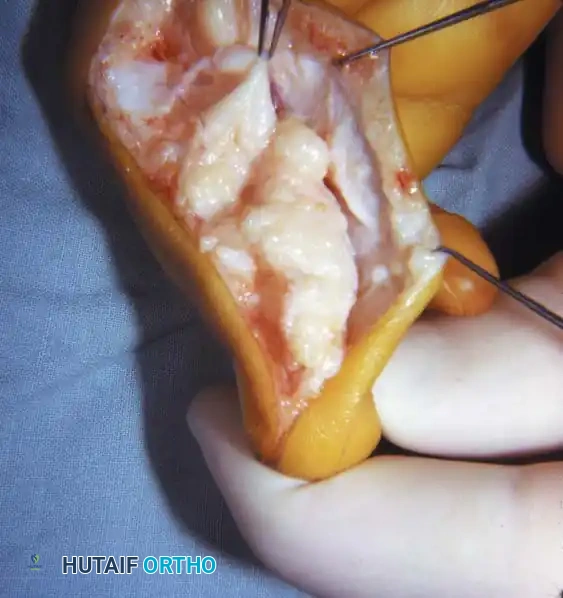
Fig. 76-54 A, Recurrent macrodactyly in a 6-year-old child 2 years after a debulking procedure of the ring finger and amputation of the long finger. B, Intraoperative photograph demonstrating gross enlargement and fibrofatty infiltration of the digital nerve. C, Wound closure after secondary debulking.
SURGICAL INDICATIONS AND PREOPERATIVE PLANNING
There are absolutely no satisfactory nonsurgical methods for controlling macrodactyly. Attempts to restrict growth via compressive elastic wrapping have universally failed and risk ischemic injury.
Indications for Surgical Intervention:
1. Progressive, disproportionate enlargement interfering with hand function.
2. Severe angular deformity (angulation).
3. Development of compressive neuropathies (e.g., Carpal Tunnel Syndrome).
4. Intractable causalgia or trophic ulceration.
Surgical management is highly complex and fraught with a high recurrence rate. The primary goal is to achieve a functional, sensate, and cosmetically acceptable digit. In severe, unmanageable cases in adults, ray amputation remains a definitive salvage procedure, though it is considered a last resort.
Surgical Warning: Flap necrosis is the most devastating acute complication in macrodactyly surgery. The hypertrophic skin has a tenuous, unpredictable vascular supply. Careful attention to flap design is mandatory. Operating on only one side of the finger at a time is a strict rule to minimize the risk of catastrophic circulatory disturbance.

Intraoperative visualization of the massive fibrofatty proliferation surrounding the neurovascular bundles, necessitating meticulous micro-dissection to preserve viability while achieving adequate debulking.
SURGICAL TECHNIQUES
Complex Reconstruction and Pollicization (Technique 76-30)
In cases of severe multi-digit involvement where the thumb is deficient or functionally compromised by massive overgrowth, pollicization of the most functional adjacent digit combined with fillet-type amputations of excessive digits may be indicated.
Step-by-Step Procedure:
* Preoperative Design: Before inflation of the tourniquet, meticulously plan the incisions. Design flaps to allow pollicization of the chosen digit, fillet-type amputations of the non-salvageable excessive digits, and wide exposure of the neurovascular bundles.
* Preparation: Exsanguinate the limb and inflate the pneumatic tourniquet.
* Neurovascular Dissection: Make the planned incisions. Carefully dissect the common neurovascular bundles to the middle digit within each web space. Ligate the vascular bifurcations leading to each adjacent digit that is slated for amputation.
* Nerve Preservation: Dissect the common digital nerves proximally to the thenar level before any division. It is critical to meticulously preserve the digital nerves and dorsal venous outflow to the digit selected for pollicization.
* Tendon Management: Dissect out the flexor and extensor tendons to the pollicized digit. If anomalous bifurcations exist, divide the abnormal insertions tethering them to neighboring tendons.
* Amputation of Excess Digits: Amputate the designated extra digits, including their respective metacarpals and articulating carpal bones. Crucial Step: Preserve the extensor tendons of the excised digits; these will be utilized later to reinforce thumb extension or abduction.
* Metacarpal Shortening: Shorten the metacarpal of the pollicized digit via an osteotomy just proximal to the metacarpal neck. Discard the remaining proximal shaft.
* Positioning and Fixation: Rotate the metacarpal head into 120 degrees of flexion and 90 degrees of pronation. Secure it in this functional opposition position using two intraosseous sutures or a stout Kirschner wire.
* Intrinsic Transfer: Suture the available intrinsic muscles to the lateral bands of the extensor mechanism of the pollicized digit to augment active adduction and abduction.
* Web Space Reconstruction: Utilize the fillet flaps harvested from the amputated digits to reconstruct a deep, functional first web space.
* Closure: Excise any redundant skin to allow tension-free closure over the shortened, pollicized digit.
* Tendon Transfer (Optional): If augmented wrist extension is required, divide the flexor digitorum sublimis (FDS) muscle at the level of the A1 pulley of the pollicized digit, route it dorsally, and transfer it to the dorsal base of the second metacarpal.
* Tourniquet Deflation: Deflate the tourniquet prior to final closure to rigorously check the viability of the remaining digits and flaps. Achieve meticulous hemostasis.
* Immobilization: Apply a bulky, non-compressive dressing reinforced with a long-arm posterior splint. Position the elbow at 90 degrees, the wrist in neutral or slight extension, and the newly reconstructed thumb in wide abduction.
Staged Soft-Tissue Debulking (Tsuge Technique 76-31)
For progressively enlarging digits, staged debulking is the workhorse procedure. The objective is to excise as much excess fibrofatty tissue as possible. Tsuge proposed that disproportionate growth is driven by excessive neural input and advocated for aggressive neural management during debulking.
Surgical Warning: Debulking must be strictly limited to one half of the digit per stage. Attempting circumferential debulking in a single setting will almost certainly result in venous congestion, arterial insufficiency, and digital necrosis. The second stage is performed a minimum of 3 months later.
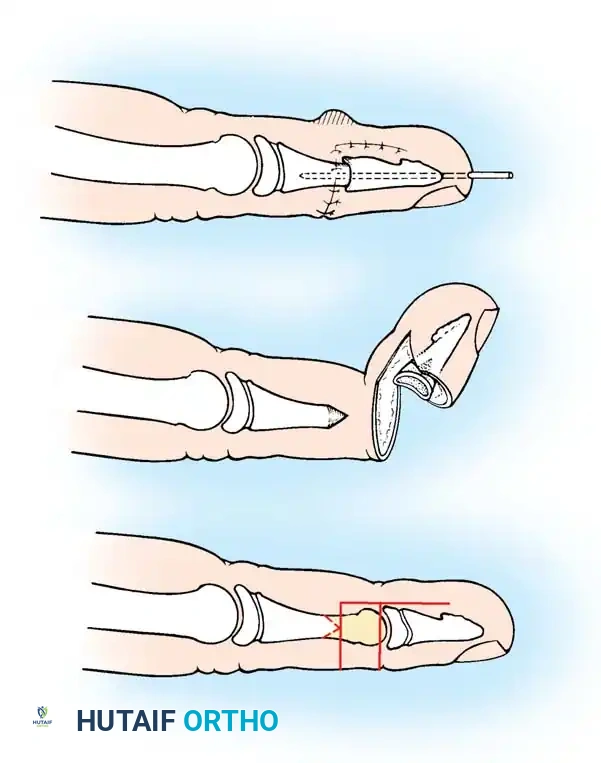
Fig. 76-55 Digital shortening for macrodactyly (Tsuge). A, Matching sections (shaded areas) of the volar half of the distal phalanx and dorsal half of the middle phalanx are removed. B, The distal phalanx is reduced onto the middle phalanx, preserving the dorsal skin bridge while removing excess soft tissue. C, Soft-tissue closure is completed.
Step-by-Step Procedure:
* Approach: Under tourniquet control, utilize a midlateral incision extending the entire length of the involved digit on the side chosen for the first stage.
* Neurovascular Identification: Identify and carefully dissect out the hypertrophied digital nerve and artery.
* Tissue Excision: Radically excise all excessive fibrofatty adipose tissue from the volar and lateral aspects of the exposed half of the digit.
* Nerve Management (Tsuge vs. Kelikian):
* Tsuge Method: If the digital nerve is grossly enlarged, Tsuge recommends stripping and excising one-half of the nerve fascicles. He argued that complete excision of the enlarged nerve is the most effective way to halt progressive overgrowth, noting that children tolerate the resulting sensory deficit surprisingly well.
* Kelikian Method: If the nerve is excessively tortuous rather than diffusely thickened, resect the tortuous segment entirely and perform a primary end-to-end epineural repair.
* Bony Resection (If Shortening is Required): Resect matching sections of the volar half of the distal phalanx and the dorsal half of the middle phalanx (Fig. 76-55A). Reduce the fragments to shorten the digit while maintaining joint stability (Fig. 76-55B).
* Closure: Excise redundant, hypertrophic skin. Close the incision meticulously (Fig. 76-55C). If skin viability is questionable, some authors recommend excising the native skin entirely and replacing it with a full-thickness skin graft.
* Postoperative Care: Apply a bulky hand dressing. No rigid postoperative protection is strictly required unless bony work was performed.
* Staging: Schedule the debulking of the contralateral side of the digit for 3 months postoperatively.
Epiphysiodesis (Technique 76-32)
Physeal arrest is frequently recommended once the macrodactylous digit has reached the estimated normal adult length of the patient's gender. Various techniques exist: Clifford utilized drill holes across the physis, Jones advocated for complete physeal resection, and Wood popularized the use of a high-speed burr.
Step-by-Step Procedure:
* Approach: Under tourniquet control, make a midlateral incision spanning the entire length of the finger.
* Exposure: Retract the neurovascular bundles volarly and the extensor mechanism dorsally to expose the joints and physes.
* Ablation: Identify the physes of the proximal, middle, and distal phalanges. Perform a thorough epiphysiodesis of all three physes using a high-speed burr or a curette combined with electrocautery to ensure complete destruction of the germinal matrix of the growth plate.
* Closure: Irrigate the wounds, close the incision in layers, and apply a protective finger splint.
* Aftertreatment: Maintain the splint for 3 weeks to allow soft-tissue healing and prevent physeal fracture during the fusion process.
Digital Shortening (Barsky Technique 76-33)
When the digit is excessively long and angulated, closing wedge osteotomies or formal shortening arthrodeses are required. Barsky described a highly effective "pencil-cone" technique for shortening the digit at the distal interphalangeal (DIP) joint level.
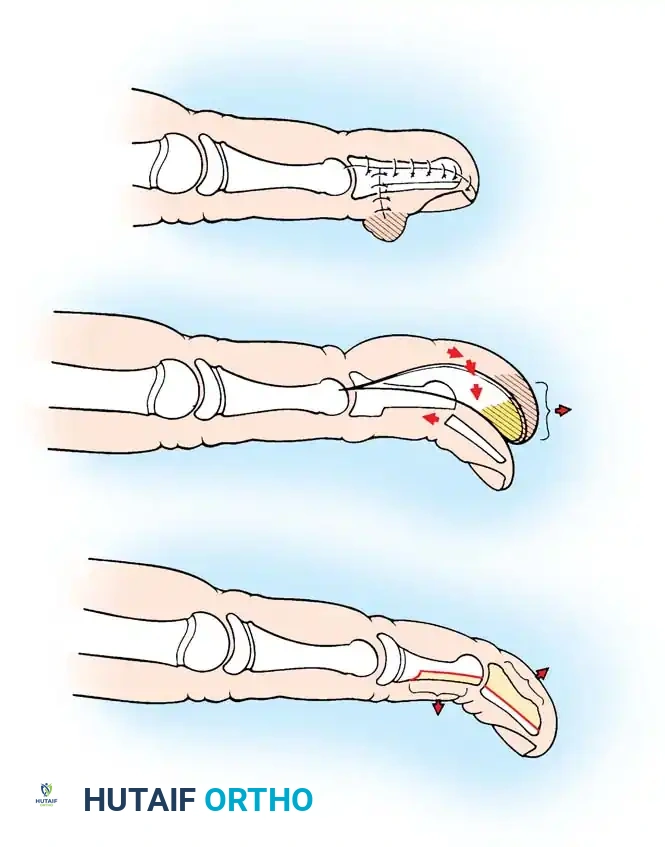
Fig. 76-56 Digital shortening for macrodactyly (Barsky). A, L-shaped midlateral and dorsal incisions allow removal of excess dorsal tissue, the distal half of the middle phalanx, and the proximal portion of the distal phalanx. B, Bone ends are prepared for a pencil-cone reduction. C, The distal phalanx is reduced onto the middle phalanx and secured with a Kirschner wire.
Step-by-Step Procedure:
* Incision: Under tourniquet control, make an L-shaped incision. Begin at the midlateral aspect of the proximal interphalangeal (PIP) joint and extend it distally to a level just proximal to the germinal matrix of the nail (Fig. 76-56A). Carry the distal limb of the incision transversely across the dorsum of the finger.
* Bone Resection: Expose the DIP joint. Resect the distal half of the middle phalanx and the proximal articular portion of the distal phalanx.
* Pencil-Cone Preparation: Using a fine rongeur or burr, sharpen the distal end of the remaining middle phalanx into a conical "pencil point." Prepare the medullary canal of the remaining distal phalanx to receive this cone (Fig. 76-56B).
* Reduction and Fixation: Impale the distal phalanx onto the sharpened middle phalanx, effectively recessing and shortening the finger. Fix the arthrodesis rigidly with a longitudinal Kirschner wire (Fig. 76-56C).
* Soft Tissue Management: Excess volar soft tissue is typically left intact during this stage to protect the vascular supply and can be excised during a subsequent debulking stage.
* Closure: Close the dorsal and lateral incisions. Apply a protective finger splint.
Thumb Shortening (Millesi Technique 76-34)
Macrodactyly of the thumb presents a unique reconstructive challenge due to the critical importance of preserving the nail complex for pinch kinematics and aesthetics. Millesi described a complex step-cut shortening technique that preserves the distal interphalangeal joint equivalent.
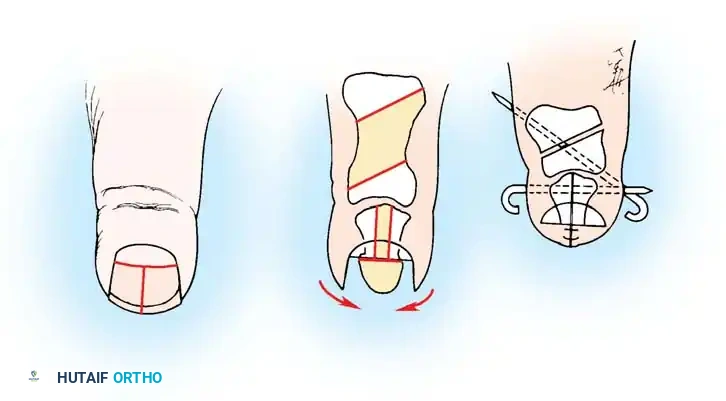
Fig. 76-57 Thumb reduction for macrodactyly (Millesi). A, Removal of the distal half of the nail and distal phalanx, meticulously preserving eponychial tissue. B, Reduction osteotomies performed through a dorsal incision. C, Remaining bone reduced and pinned.
Step-by-Step Procedure:
* Distal Ablation: Under tourniquet control, carefully excise the distal half of the nail plate, the underlying nail matrix, and the distal phalangeal tuft (Fig. 76-57A). Meticulously preserve the proximal eponychial fold.
* Dorsal Approach: Make a dorsal longitudinal incision overlying the proximal and distal phalanges.
* Phalangeal Resection: Remove the middle third of the distal phalanx along with the middle third of its overlying nail and matrix.
* Proximal Osteotomy: Remove the middle third of the proximal phalanx by executing parallel oblique osteotomies (Fig. 76-57B). This step-cut approach increases the surface area for bony union and controls rotation.
* Fixation: Reduce the shortened osseous segments and secure them with longitudinal or crossed Kirschner wires (Fig. 76-57C).
* Closure: Repair the remaining nail matrix meticulously with fine absorbable sutures (e.g., 6-0 chromic) to prevent nail dystrophy. Close the skin.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Aftertreatment:
For all osteotomy and arthrodesis procedures (Barsky, Millesi, Tsuge with bone resection), the digit is immobilized in a protective splint for a minimum of 3 weeks. Kirschner wires are typically removed in the clinic once radiographic evidence of clinical healing is observed at the osteotomy sites, usually between 4 to 6 weeks postoperatively. Aggressive occupational therapy is initiated immediately following K-wire removal to maximize interphalangeal and metacarpophalangeal joint mobility, which is notoriously stiff in these patients.
Complications:
1. Recurrence: The most common complication. Despite aggressive debulking and nerve resection, the fibrofatty tissue often proliferates, necessitating multiple revision surgeries throughout the child's growth period.
2. Flap Necrosis: A devastating complication resulting from overly aggressive single-stage debulking or poor flap design. If full-thickness necrosis occurs, it must be managed with aggressive debridement and full-thickness skin grafting or cross-finger flaps.
3. Neurovascular Injury: Inadvertent transection of the dominant digital artery during debulking can lead to digital ischemia.
4. Joint Stiffness: Inherent to the pathology but exacerbated by prolonged immobilization and extensive surgical scarring. Early, protected mobilization is critical.
