INTRODUCTION TO KNEE DISLOCATIONS AND ASSOCIATED INJURIES
Knee dislocations are catastrophic, high-energy injuries that severely compromise the structural integrity and neurovascular viability of the lower extremity. While historically considered rare, the true incidence is likely underestimated due to spontaneous reductions occurring prior to clinical evaluation. A true knee dislocation implies the disruption of at least two, and often three or four, of the primary knee ligaments (Anterior Cruciate Ligament [ACL], Posterior Cruciate Ligament [PCL], Medial Collateral Ligament [MCL], and Lateral Collateral Ligament [LCL]/Posterolateral Corner [PLC]).
Beyond the gross ligamentous incompetence, associated osteochondral and meniscal injuries are ubiquitous. The intercondylar eminences are frequently fractured, and fractures of the distal femur or proximal tibia are present in approximately 16% of all knee dislocations.
Biomechanics of Ligamentous Failure
Although a complete dislocation of the tibiofemoral joint rarely occurs without the disruption of both cruciate ligaments, specific injury vectors can result in isolated cruciate sparing. In straight anterior or posterior dislocations, a deceptive degree of coronal stability may be retained. This occurs because the femoral condyles can be stripped cleanly out of their capsular and collateral ligament attachments, slipping back inside this soft-tissue envelope upon reduction.
The morphological patterns of ligamentous tearing dictate the surgical approach:
* Anterior Cruciate Ligament (ACL): Midsubstance tears occur in approximately 50% of knee dislocations. This is followed in frequency by avulsions at the femoral attachment, and least commonly, the tibial attachment.
* Posterior Cruciate Ligament (PCL): In stark contrast to the ACL, the PCL is torn directly from its femoral attachment in nearly 75% of knee dislocations, followed by midsubstance ruptures and tibial avulsions.
Clinical Pearl: In cases of clean ligamentous avulsion fractures (particularly of the cruciates or collateral origins), primary anatomical repair with suture anchors or transosseous tunnels may be viable if addressed in the acute setting, negating the immediate need for allograft reconstruction.
VASCULAR ASSESSMENT AND TREATMENT ALGORITHM
The most critical, limb-threatening complication of a knee dislocation is injury to the popliteal artery. Due to its rigid tethering proximally at the adductor hiatus and distally at the soleal arch, the popliteal artery is highly susceptible to traction, intimal tearing, and complete transection during tibiofemoral displacement.
The Ischemic Cascade and Amputation Risk
Time is tissue. Procrastination with a nonsurgical approach or the false expectation that collateral genicular circulation will provide sufficient peripheral perfusion invites disaster. The amputation rates correlate directly with the duration of ischemia:
* < 6 Hours: ~6% amputation rate.
* 6 to 8 Hours: ~11% amputation rate.
* > 8 Hours: ~86% amputation rate.
* Untreated Vascular Injury: >90% amputation rate.
Evidence-Based Vascular Algorithm
Based on the modified Howells et al. (2011) treatment algorithm, the management of a known or suspected knee dislocation must proceed systematically:
- Immediate Closed Reduction: Perform an immediate, gentle longitudinal traction-countertraction reduction.
- Physical Examination: Assess distal pulses and calculate the Ankle-Brachial Pressure Index (ABPI).
- Stratification based on Perfusion:
- Distal Pulses Present & ABPI > 0.9: Admit for 24-hour observation with serial pulse examinations. Consider duplex ultrasound or CT angiography prior to any planned ligamentous reconstruction.
- Distal Pulses Asymmetric, ABPI < 0.9, or Clinical Concern: Mandates immediate advanced imaging via CT Angiogram or conventional Angiogram.
- Distal Pulses Absent / Hard Signs of Vascular Injury (Ischemia, Expanding Hematoma, Pulsatile Hemorrhage): Immediate vascular surgery consultation. Proceed directly to the operating room for exploration and repair, with on-table angiography.
Surgical Warning: If popliteal artery repair is required, extensive concurrent ligamentous reconstruction is strictly contraindicated. The orthopedic surgeon may place a few well-positioned sutures in the capsular structures during the vascular exposure, but definitive reconstruction must be delayed. Ligamentous reconstruction can be safely performed up to 2 weeks post-vascular repair, provided the vascular surgeon clears the use of a tourniquet.
INDICATIONS FOR IMMEDIATE VERSUS DELAYED ORTHOPEDIC SURGERY
Historically, knee dislocations were treated with closed reduction and prolonged plaster immobilization due to the sheer complexity of the soft-tissue damage and the lack of advanced reconstructive techniques. Today, modern evidence overwhelmingly supports early ligament repair or reconstruction combined with aggressive rehabilitation, particularly in young, active patients.
Indications for Immediate Orthopedic Intervention
While most multiligament reconstructions are performed on a delayed-acute basis (10 to 14 days), certain scenarios demand immediate surgical intervention:
1. Irreducible Dislocation: Occasionally, the medial capsule and MCL are invaginated and trapped within the joint during a posterolateral dislocation.
* Pathognomonic Sign: A dimpling, puckering, or deep furrow along the medial joint line, combined with a slightly nonanatomical reduction on post-reduction radiographs.
2. Vascular Injury: Requiring immediate revascularization (as detailed above).
3. Open Knee Dislocations: Requiring emergent irrigation and debridement.
4. Compartment Syndrome: Requiring emergent four-compartment fasciotomies of the leg.
Post-Reduction Immobilization
Once an anatomical closed reduction is achieved (and confirmed via orthogonal radiographs), the knee must be immobilized in its most stable position.
* Positioning: 30 to 45 degrees of knee flexion is optimal. This specific arc of flexion relaxes the posterior capsule, the posteromedial corner (PMC), and the posterolateral corner (PLC), while critically removing tension from the popliteal vessels.
* Immobilization Method: Utilize a posterior plaster splint or a hinged knee brace locked in flexion.
* Contraindications: Circumferential casts must be strictly avoided to allow for continuous monitoring of neurovascular status and evolving compartment swelling. Transarticular pinning (olecranization of the patella) is obsolete and should be avoided due to the high risk of articular cartilage damage and pin-tract infection. If splinting fails to maintain a concentric reduction, a spanning external fixator is the treatment of choice.
SURGICAL TIMING AND GRAFT SELECTION
A meta-analysis of knee dislocations confirms that operative reconstruction yields significantly better functional outcomes, higher stability scores, and a lower risk of arthrofibrosis compared to nonoperative management.
Timing of Reconstruction
Current treatment paradigms focus on the early reconstruction of the cruciate ligaments combined with the repair or reconstruction of collateral structures.
* Early Intervention (10 to 14 Days): Preferred for severe injury patterns, including ACL/PCL/PLC, PCL/PLC, and grade III distal tears of the MCL combined with cruciate injuries. Operating within this window allows for the primary repair of avulsed collateral structures before tissue retraction and scarring occur.
* Delayed Intervention: Can be considered for isolated ACL/PCL injuries with intact collateral ligaments, or when the posterior oblique ligament (POL) remains intact in the setting of medial-sided injuries.
Graft Selection in the Multiligament Knee
The choice of graft depends on the specific structures injured, the timing of surgery, and surgeon experience. In the setting of a multiligament-injured knee, allografts are generally preferred to minimize surgical time, reduce donor-site morbidity, and avoid further trauma to an already compromised extremity.
- ACL Reconstruction: Bone-Patellar Tendon-Bone (BTB) allograft or autograft.
- PCL Reconstruction: Achilles tendon allograft (allows for a robust bone block at the femoral footprint and ample soft tissue for tibial fixation).
- Posterolateral Corner (PLC): Tibialis anterior or posterior allograft.
- Medial/Posteromedial Corner (PMC): Tibialis or Achilles tendon allograft.
- Artificial Ligaments: Synthetic scaffolds are currently under renewed investigation for multiligament reconstructions, showing comparable subjective and objective outcomes at mid-term follow-up, though they remain secondary to biologic grafts in standard practice.
SURGICAL APPROACHES AND TECHNIQUES
The operative treatment of a dislocated knee begins with a comprehensive Examination Under Anesthesia (EUA) to confirm the preoperative MRI findings and identify all incompetent structures.
The Role of Arthroscopy
Arthroscopy is invaluable for the evaluation and treatment of concomitant meniscal and chondral injuries, which must be addressed prior to ligamentous reconstruction. However, arthroscopy in the acute multiligament knee must be strictly limited.
Surgical Pitfall: Prolonged arthroscopy with high pump pressures in an acutely dislocated knee with capsular disruption will lead to massive fluid extravasation into the calf and thigh, precipitating an iatrogenic compartment syndrome. Use gravity flow or low-pressure settings, and transition to open procedures swiftly.
Incisions and Exposures
The surgical approach is dictated by the specific injury pattern. Maintaining wide skin bridges (greater than 7 cm) is absolute to prevent catastrophic skin necrosis between incisions.
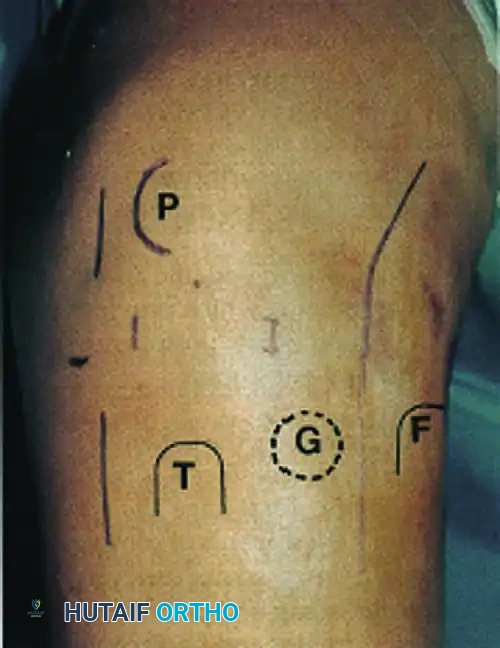
Above: Skin incisions for open lateral or posterolateral reconstruction combined with arthroscopic reconstruction of anterior and posterior cruciate ligaments. F, Fibular head; G, Gerdy tubercle; P, patella; T, tibial tubercle.
- Medial Utility Incision: A curved medial incision allows comprehensive exposure of the medial collateral ligament, the posteromedial corner, and the medial meniscus.
- Posterior L-Shaped Incision (Burks and Schaffer): Utilized for the direct exposure of the tibial insertion of the PCL. This is essential for the repair of PCL avulsion fractures or for performing an open tibial inlay PCL reconstruction.
- Lateral/Posterolateral Incision: A straight lateral incision provides access to the IT band, LCL, popliteus tendon, and the fibular head for PLC reconstruction. Careful identification and neurolysis of the common peroneal nerve are mandatory during this approach.
- Midline Incision: A single, expansile straight midline incision can be utilized to access all structures by developing full-thickness medial and lateral fasciocutaneous flaps, though this requires extensive dissection.
Suggested Surgical Sequence
- Examination under anesthesia.
- Diagnostic arthroscopy (low pressure) and management of meniscal/chondral pathology.
- Preparation of allograft tissues.
- Drilling of femoral and tibial tunnels for the PCL and ACL.
- Open exposure of the medial and/or lateral sides.
- Fixation of the PCL graft.
- Fixation of the ACL graft.
- Reconstruction and tensioning of the PLC and/or PMC.
- Final assessment of stability and layered closure.
POSTOPERATIVE REHABILITATION PROTOCOL
Rehabilitation following a multiligament knee reconstruction is a delicate balance between protecting the healing grafts and preventing debilitating arthrofibrosis. Full recovery is a prolonged process, typically requiring 9 to 12 months.
The Harner et al. Multiligament Rehabilitation Protocol
The following phased approach is widely accepted for optimizing outcomes:
Phase I: Maximum Protection (Weeks 0 to 2)
* Knee immobilized in a hinged brace locked in full extension.
* Strict non-weight bearing or touch-down weight bearing.
* Passive extension must be symmetrical to the noninvolved side (Note: For isolated PCL reconstructions, limit extension to 0° to prevent graft stretching).
* Initiate quadriceps sets and straight leg raises immediately to prevent atrophy.
Phase II: Controlled Motion (Weeks 2 to 4)
* Unlock brace for range of motion exercises.
* Gradually add passive flexion up to 90 degrees.
* Utilize biofeedback and electrical stimulation as necessary to recruit quadriceps function.
Phase III: Early Strengthening (Weeks 4 to 8)
* Progress to partial weight bearing with the brace locked in extension during ambulation.
* Initiate limited arc open-chain quadriceps exercises (60° to 75°).
* Begin closed-chain exercises for quadriceps and hamstrings.
* Passive and active-assisted ROM stretching to increase flexion beyond 90 degrees.
Phase IV: Advanced Strengthening (Months 6 to 9)
* Weight bearing as tolerated; discontinue crutches.
* Discontinue the functional brace for daily activities.
* Initiate balance and proprioception exercises.
* Begin low-impact aerobics and progress to running once quadriceps strength reaches 80% of the contralateral limb.
Phase V: Return to Function (Months 9 to 12)
* Clearance for heavy manual work.
* Return to sports activities requiring changes in direction and pivoting is strictly delayed until 9 to 12 months postoperatively, contingent upon passing functional hop tests and isokinetic strength evaluations.
CLINICAL OUTCOMES AND COMPLICATIONS
Despite a profound understanding of knee biomechanics and advanced surgical techniques, the severe soft-tissue disruption inherent to knee dislocations often precludes the restoration of a "normal" knee.
Functional Expectations
Patients must be counseled preoperatively regarding realistic outcomes. In large-cohort studies utilizing the International Knee Documentation Committee (IKDC) scoring system:
* 0% of multiligament reconstructed knees were rated as "Normal."
* 39% were rated as "Nearly Normal."
* 40% were rated as "Abnormal."
* 21% were rated as "Severely Abnormal."
However, when compared to nonoperative management, surgical reconstruction consistently yields superior range of motion, higher functional scores, and a significantly lower incidence of late degenerative joint disease. This holds true even in low-demand patients or those suffering from ultra-low-velocity dislocations (e.g., morbidly obese patients), where surgical stabilization provides a more functional limb than conservative care.
Complications
- Arthrofibrosis (Knee Stiffness): The most common complication following multiligament reconstruction. Early, controlled mobilization is the primary defense. Manipulation under anesthesia or arthroscopic lysis of adhesions may be required if flexion fails to progress by 12 weeks.
- Graft Failure and Residual Laxity: Failure of one or more components of the reconstruction can occur due to unrecognized concomitant injuries (e.g., missed PLC injury leading to ACL graft failure), premature return to sport, or failure to correct preexisting malalignment.
- Note on Alignment: Preexisting varus alignment must be treated surgically (often with a concurrent High Tibial Osteotomy) to prevent a lateral thrust gait and subsequent failure of a PLC reconstruction. The same principle applies to valgus alignment in the setting of severe medial-sided injuries.
- Neurovascular Compromise: Late vascular occlusion or common peroneal nerve palsy (which occurs in up to 25% of posterolateral dislocations) requires vigilant postoperative monitoring and potential secondary interventions, such as nerve exploration or tendon transfers.
