INTRODUCTION TO NEOPLASTIC CONDITIONS OF THE HAND
The evaluation and management of osseous and synovial neoplasms in the hand demand a rigorous, evidence-based approach. While the majority of hand tumors are benign, their anatomical proximity to critical neurovascular structures, tendons, and articular surfaces makes surgical intervention highly complex. The primary goals of operative orthopaedics in this domain are complete eradication of the lesion, preservation of biomechanical function, and minimization of recurrence.
This masterclass delineates the pathophysiology, clinical presentation, and step-by-step surgical management of four distinct entities: Osteochondroma, Synovial Chondromatosis, Giant Cell Tumor (GCT) of bone, and Aneurysmal Bone Cyst (ABC).
OSTEOCHONDROMA OF THE HAND
Osteochondromas (exostoses) are the most common benign bone tumors overall but are paradoxically rare in the hand and carpus. When they do occur in the upper extremity, they are occasionally seen on a phalanx or metacarpal.
Pathophysiology and Biomechanics
An osteochondroma represents a developmental hamartoma rather than a true neoplasm. It originates from an aberrant focus of physeal cartilage that separates from the epiphyseal plate and grows outward through the metaphyseal cortex. The lesion consists of mature trabecular bone continuous with the medullary cavity of the host bone, capped by hyaline cartilage. Growth typically ceases upon skeletal maturity. In the hand, the biomechanical consequence of this exophytic growth is often mechanical impingement on the extensor or flexor mechanisms, leading to restricted range of motion (ROM) or tendon attrition.

Clinical Evaluation and Indications for Surgery
Patients typically present with a painless, slow-growing, hard mass. Pain usually indicates mechanical irritation of overlying soft tissues, bursa formation, or, rarely, a pathological fracture through the stalk.
Indications for Excisional Biopsy:
* Pain or neurovascular impingement.
* Mechanical block to joint motion.
* Progressive deformity (especially angular deformities in the pediatric population).
* Cosmetic concerns or interference with daily activities.
* Growth of the lesion after skeletal maturity (raises suspicion for malignant transformation to secondary chondrosarcoma, though exceedingly rare in the hand).
Clinical Pearl: Always evaluate the cartilage cap thickness on MRI if malignant transformation is suspected. A cap thicker than 1.5 cm to 2.0 cm in an adult is highly concerning for secondary chondrosarcoma.
Surgical Technique: Excisional Biopsy
1. Positioning and Preparation:
* The patient is positioned supine with the arm extended on a radiolucent hand table.
* A well-padded upper arm tourniquet is applied.
* Regional anesthesia (axillary or supraclavicular block) is preferred.
2. Surgical Approach:
* A longitudinal or lazy-S incision is made directly over the palpable mass, avoiding neurovascular bundles.
* For phalangeal lesions, a mid-axial or dorsal approach is utilized depending on the exostosis location.
* The extensor mechanism is carefully mobilized and retracted. If the lesion is volar, the flexor tendon sheath is identified and protected.
3. Resection:
* The periosteum overlying the osteochondroma is incised and elevated.
* Crucial Step: The resection must be extraperiosteal and include the entire cartilage cap and the overlying perichondrium to prevent recurrence.
* An osteotome or oscillating microsaw is used to resect the stalk flush with the normal cortical contour of the host bone.
* The medullary canal of the host bone may be sealed with bone wax if bleeding is excessive, though this is rarely necessary.
4. Closure and Postoperative Protocol:
* The wound is irrigated copiously.
* Soft tissues are closed in layers.
* A bulky soft dressing is applied, allowing for immediate active range of motion (AROM) to prevent tendon adhesions.
SYNOVIAL CHONDROMATOSIS
Synovial chondromatosis is an unusual, typically monoarticular mechanical condition characterized by benign, nodular cartilaginous metaplasia of the synovial membrane.
Pathophysiology
While it usually affects large joints such as the knee, hip, elbow, or shoulder, it can occasionally manifest in the proximal interphalangeal (PIP) joint and the wrist. The synovial lining undergoes metaplasia, producing osteocartilaginous loose bodies that vary in size from microscopic to 2 cm in diameter. These bodies may detach, float freely in the synovial fluid (which nourishes them), and eventually calcify or ossify.
Surgical Warning: Cartilaginous metaplasia from joint, tendon, or bursal synovial lining differentiates primary synovial chondromatosis from secondary loose bodies arising from degenerative arthritis, osteochondritis dissecans, or osteochondral fractures.
Diagnostic Imaging
- Plain Radiographs: Usually characteristic, portraying multiple, uniform, stippled, or ring-and-arc calcified loose bodies within the joint capsule.
- Advanced Imaging: Noncalcified cartilaginous bodies may be radiolucent on plain films. In such cases, arthrography or MRI with contrast enhancement is essential to detect the extent of synovial involvement and the presence of uncalcified bodies.
Surgical Technique: Arthrotomy and Synovectomy
1. Approach:
* Standard dorsal approaches to the wrist or PIP joint are utilized.
* For the wrist, a dorsal longitudinal incision is made, and the extensor retinaculum is opened (typically through the 3rd or 4th extensor compartment).
2. Joint Exploration and Loose Body Removal:
* A formal arthrotomy is performed.
* All loose bodies are systematically extracted. Copious irrigation with normal saline helps flush out microscopic cartilaginous fragments hidden in the recesses.
3. Synovectomy:
* A subtotal or total synovectomy is mandatory to address the underlying metaplastic tissue and reduce the risk of recurrence.
* Rongeurs and synovial resectors are used to meticulously clear the joint capsule.
4. Postoperative Protocol:
* Early mobilization is critical to prevent joint stiffness, particularly in the PIP joint.
* A dynamic splint may be employed if extensive capsular release was required.
ANEURYSMAL BONE CYST (ABC) OF THE HAND
Aneurysmal bone cysts are rare, expansile, osteolytic lesions consisting of blood-filled spaces separated by connective tissue septa containing fibroblasts, osteoclast-like giant cells, and reactive woven bone.
Clinical Presentation
ABCs can be primary or secondary (arising within a pre-existing lesion like a GCT or chondroblastoma). In the hand, they often present with rapid, insidious enlargement, dull aching, and occasionally a history of antecedent trauma.
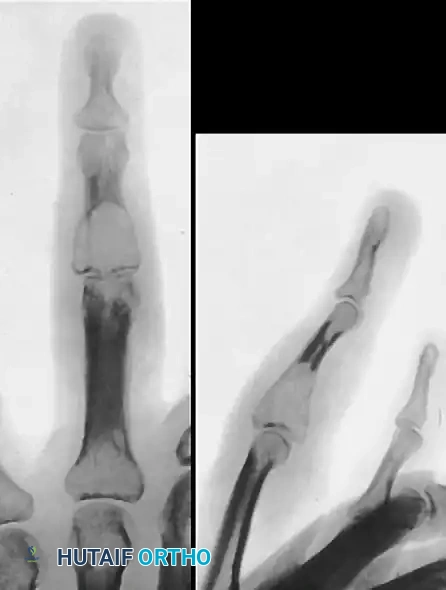
FIGURE 77-15 A 17-year-old boy was first seen with a swollen ring finger 1 year after the tip of the finger was crushed by a falling railroad tie. Immediate swelling occurred with drainage from split skin at the tip. The finger soon became asymptomatic as initial edema diminished, but insidious enlargement of the distal phalanx, dull aching, and clubbing of the nail were noted. A, Bulbous enlargement progressed over the next 12 months. B, Radiograph of destroyed expanded distal phalanx. C, Arteriogram shows arterial filling of the lesion. D, Venous phase with large venous channels.



FIGURE 77-16 Aneurysmal bone cyst in middle finger metacarpal in a skeletally immature patient.

Surgical Management
Because ABCs are highly vascular and expansile, surgical planning must account for potential intraoperative hemorrhage and the need for structural reconstruction.
1. Curettage and Bone Grafting:
* For contained lesions, a large cortical window is created.
* Aggressive intralesional curettage is performed. The cavity is cleared of all spongy, hemorrhagic tissue until healthy cortical bone is reached.
* High-speed burring extends the margin.
* The defect is packed with autologous cancellous bone graft (e.g., from the distal radius or iliac crest) or allograft.
2. En Bloc Resection:
* If the bone is entirely destroyed (as seen in the distal phalanx in Fig 77-15), or if the lesion is in an expendable bone, en bloc resection may be indicated.
* Reconstruction may involve structural bone grafting and internal fixation (K-wires or mini-plates).
GIANT CELL TUMOR (GCT) OF THE HAND
Giant cell tumors of bone are locally aggressive, osteolytic neoplasms. While they classically occur in the epiphyses of long bones (distal radius, proximal tibia), their presentation in the hand (metacarpals and phalanges) is unique and notoriously problematic.
Pathophysiology and Behavior
GCTs in the hand occur in a younger demographic compared to long bone GCTs and exhibit a higher rate of local recurrence. They are characterized by a proliferation of mononuclear stromal cells and multinucleated osteoclast-like giant cells.
Pitfall: This tumor should not be confused with an enchondroma or a giant cell reparative granuloma. A biopsy is strictly indicated to confirm the diagnosis before definitive resection.
Furthermore, GCTs have a tendency to metastasize (benign pulmonary implants) in about 2-3% of cases. Multicentric tumors have been reported, suggesting that a full bone survey (or whole-body MRI/bone scan) is indicated to discover remote sites of tumor when a giant cell tumor is suspected.
Classification
The Campanacci classification system helps guide treatment:
* Grade I: Latent, well-marginated, intact cortex.
* Grade II: Active, well-defined but without a sclerotic rim, cortical thinning, and expansion.
* Grade III: Aggressive, indistinct borders, cortical breakthrough, and soft tissue extension.
FIGURE 77-17 A, Giant cell tumor of head of fifth metacarpal. B, Pathological fracture caused by tumor.


Surgical Techniques for GCT
The treatment of GCT in the hand is highly debated, balancing the need for complete eradication against the desire for functional preservation. Poorly executed or marginal excisions have an unacceptably high tendency to recur.
1. Intralesional Curettage with Adjuvant Therapy (For Grade I and early Grade II)
- Cortical Window: A generous cortical window is created to allow full visualization of the tumor cavity.
- Aggressive Curettage: Meticulous curettage using variously angled curettes is performed.
- High-Speed Burring: The cavity walls are burred down to normal-appearing bone.
- Adjuvant Treatment: This is critical to kill microscopic disease. Options include:
- Phenol (89%) application followed by alcohol neutralization.
- Liquid nitrogen (Cryotherapy).
- Argon beam coagulation.
- Defect Filling: The cavity is filled with polymethylmethacrylate (PMMA) bone cement or bone graft. PMMA is advantageous as the heat of polymerization provides an additional thermal adjuvant effect, and it allows for immediate structural stability and easier radiographic detection of recurrence.
2. Wide Resection and Reconstruction (For Grade III or Recurrences)
Given the high recurrence rate of GCTs in the hand, wide en bloc resection is often required for advanced lesions or recurrences.
FIGURE 77-18 Giant cell tumor of middle phalanx. A, Before excision. B, Status 5 years after excision. Tumor has recurred, and proximal phalanx also has become involved. C, After fourth ray was amputated and fifth ray was transposed laterally.


Ray Amputation and Transposition:
As demonstrated in Figure 77-18, a recurrent GCT that has destroyed the joint and invaded adjacent bones necessitates radical management.
* Indications: Massive cortical destruction, soft tissue extension, or multi-bone involvement secondary to recurrence.
* Technique (Ray Amputation):
* A racquet-shaped incision is made around the base of the involved digit.
* The extensor and flexor tendons are transected under tension so they retract proximally.
* The digital nerves are identified, drawn distally, transected sharply, and allowed to retract deep into the soft tissues to prevent painful neuroma formation.
* The metacarpal is osteotomized at its base.
* Transposition (e.g., 5th to 4th ray): To close the gap and improve the cosmetic and functional outcome of the hand, the adjacent ray (e.g., the 5th metacarpal) can be osteotomized at its base and transposed to the base of the amputated ray (the 4th metacarpal). It is stabilized with K-wires or a plate.
* Postoperative Care: The hand is immobilized in a bulky dressing and volar splint in the intrinsic-plus position. Pin care is maintained until radiographic union of the transposition osteotomy is confirmed (typically 6-8 weeks).
Conclusion
The operative management of benign and locally aggressive bone tumors of the hand requires a nuanced understanding of tumor biology, meticulous surgical technique, and advanced reconstructive capabilities. From the straightforward excisional biopsy of an osteochondroma to the complex ray transposition required for a recurrent giant cell tumor, the orthopaedic surgeon must prioritize both oncologic clearance and the preservation of the intricate biomechanics of the human hand.
