HY 2026
00:00
Start Quiz
Question 901
High Yield
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
Most authors recommend an initial trial of nonsurgical management in the treatment of adult-acquired flatfoot deformity such as posterior tibial tendon dysfunction. Chao and associates found that there is high patient satisfaction with ankle-foot orthoses and UCBL-type inserts in elderly patients with a relatively sedentary lifestyle. Alternatively, there was a higher dissatisfaction rate in young active patients, those with balance and ambulation difficulties (Parkinson's, severe arthritis of the hip or knee), and patients with inflammatory systemic disorders. Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Question 902
High Yield
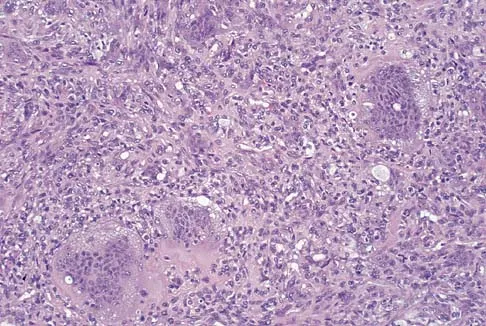
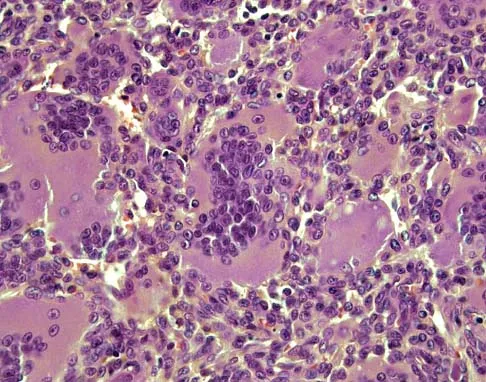
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?

Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 903
High Yield
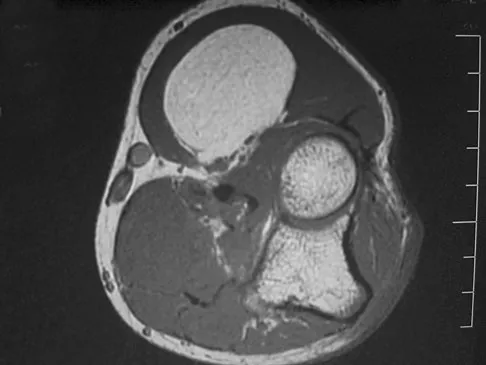
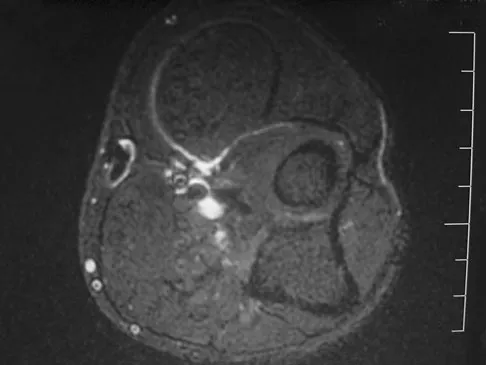
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of

Explanation
An intramuscular lipoma is a benign soft-tissue lesion that can grow and has a small risk of progressing to a liposarcoma. Radiographs usually show a globular radiolucent mass adjacent to higher-density muscle tissue shadows. When the patient has symptoms and reports an increase in size of the mass, the treatment of choice after appropriate radiographic analysis is complete excision of the mass with marginal resection. Sampling error is a problem with fatty lesions and core or incisional biopsies are frequently unnecessary, especially if an MRI scan of the lesion shows signal intensity that matches subcutaneous fat on all sequences. Damron TA: What to do with deep lipomatous tumors. Instr Course Lect 2004;53:651-655. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 904
High Yield
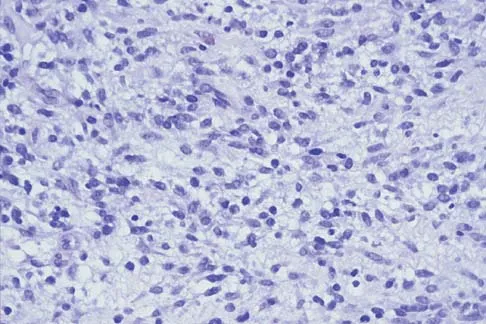
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 905
High Yield
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
Highly cross-linked polyethylene has gained widespread acceptance for joint arthroplasty components because of reported experimental and early clinical accounts of significant reductions in wear. Cross-linking is increased by imparting additional energy into the polymer (above that conventionally used for sterilization). The thermal treatments after cross-linking stabilize the material against oxidative degradation by quenching free radicals and also reduce the elastic modulus. One disadvantage of the increased cross-linking is a reduction in toughness that makes the polyethylene more susceptible to crack initiation and propagation. The reduced toughness raises concerns for gross component fracture and fracture at stress concentrations that can arise with the locking mechanisms used to secure polyethylene inserts into metallic backings. Nonconsolidated polyethylene particles have been associated with increased subsurface density secondary to oxidative degradation in conventional polyethylene implants. The quenching of free radicals by thermal treatment in highly cross-linked polyethylene should prevent this problem. Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
Question 906
High Yield
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Progressive hip subluxation occurs in up to 50% of children with spastic quadriparesis. The subluxation is the result of chronic muscle hypertonicity, especially in the adductor muscle group. In time, the constant muscle tension will lead to dislocation, dysplastic changes in the acetabulum, and erosive changes in the cartilage of the femoral head. Many of these children will experience pain. Two recent studies have shown that early soft-tissue releases can successfully prevent progressive subluxation in children who are younger than age 4 years and who have a Reimers index (migration index) of less than 40%. Botulinum toxin A injections may reduce tone in the adductors for 4 to 6 months, but it is difficult to inject into the iliopsoas. Additionally, there are no long-term studies documenting the efficacy of botulinum toxin A to treat progressive hip subluxation in patients who have spastic quadriparesis. In general, proximal femoral osteotomy, combined with soft-tissue release as necessary, is indicated in older children (older than age 4 years) with progressive subluxation. Although selective dorsal rhizotomy has been used in nonambulatory patients, outcomes are less well documented than in ambulatory patients. There are no studies documenting the effect of selective dorsal rhizotomy on progressive hip subluxation in nonambulatory children. Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
Question 907
High Yield
A metal-on-metal bearing used for total hip arthroplasty shows which of the following properties?

Explanation
Activity levels do not affect cobalt and chromium ion levels, which are the bulk of serum ion levels. The majority of ions are produced in the run-in period in the first several years. A gradual reduction in ion levels occurs thereafter. The kidneys are responsible for the bulk of clearance from the serum, and to date there is no relationship of cancer to ion levels in the serum.
Question 908
High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 909
High Yield
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?


Explanation
The blood supply to the adult capitellum and lateral trochlea comes from posterior vessels arising from the radial recurrent, radial collateral, and interosseous recurrent arteries. These arteries penetrate the distal humerus posterior and superior to the capitellum.
Question 910
High Yield
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?





Explanation
The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461. Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416. Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Question 911
High Yield
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?

Explanation
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
Question 912
High Yield
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?

Explanation
The figure shows a supracondylar process, which is a normal anatomic variant. An osteochondroma tends to occur more toward the end of bones, and the medullary space of the underlying bone extends into the base of the osteochondroma. The presence of a supracondylar process is usually asymptomatic. However, the ligament of Struthers that always extends from the supracondylar process to the medial epicondyle can result in median nerve entrapment secondary to trauma. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Question 913
High Yield
Soft-tissue sarcomas most commonly metastasize to the

Explanation
The most common location for soft-tissue tumors to metastasize is the lungs. Depending on the grade of the sarcoma, metastases develop in as many as 50% of patients with soft-tissue sarcomas. Tumor grade is considered the most significant prognostic factor in predicting risk of metastases, with high-grade lesions at greatest risk. Staging CT of the chest should be performed once the diagnosis of a soft-tissue sarcoma is suspected or confirmed. Regular surveillance of patients treated for soft-tissue sarcomas includes follow-up CT scans at regular intervals. Intra-abdominal metastases are uncommon but may occur, particularly in patients with myxoid liposarcoma. Regional metastases are relatively uncommon and occur in approximately 5% of all patients with soft-tissue sarcoma. The incidence of regional nodal metastases is higher for synovial sarcoma and epithelioid sarcomas than other soft-tissue sarcomas. Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 914
High Yield
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
The most predictable positive outcome from spinal surgery due to a cauda equina syndrome is early surgical intervention before any significant neurologic deficit develops. Meta-analysis studies demonstrate that surgical intervention more than 48 hours after the onset of cauda equina syndrome show an increased risk for poor outcomes. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Question 915
High Yield
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
Evidence implicates an association, albeit unexplained, between Clostridium septicum infection and malignancy, particularly hematologic or intestinal malignancy. The malignancy is often at an advanced stage, compromising survival of the patients. A bowel portal of entry is postulated for most patients. In the absence of an external source in the patient with clostridial myonecrosis or sepsis, the cecum or distal ileum should be considered a likely site of infection. Increased awareness of this association between Clostridium septicum and malignancy, and aggressive surgical treatment, may result in improvement in the present 50% to 70% mortality rate. Other organisms associated with malignancy include group Clostridium streptococci that are occasionally associated with upper gastrointestinal malignancies. Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Question 916
High Yield
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?

Explanation
Several large clinical studies have shown that the most common problem after elastic nailing of a femoral shaft fracture is persistent pain and irritation at the nail insertion site. Unacceptable shortening and malunion are very rare in a 7-year-old patient. Rotational malalignment also is unusual. Osteonecrosis has been reported in solid antegrade nailing but not with elastic nailing of femoral shaft fractures in skeletally immature patients. Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777. Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
Question 917
High Yield
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6 degrees F (37 degrees C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Explanation
The patient is at risk for a pelvic vascular injury and major hemorrhage. This type of complication of pelvic trauma is highest in motorcyclists. Once it is recognized that the pelvic ring has opened, it is important to close that ring to tamponade any venous bleeding with a pelvic binder and to add a skeletal traction pin to the limb on the involved side. This will correct any translational displacement. The noninvasive pelvic binders or sheets are easy to apply and are very effective. They do not compromise future care and allow the surgeons access to the abdomen. External fixation or pelvic resuscitation clamps require a certain amount of skill to apply and are not always available. If the pelvic stabilization does not improve the hemodynamic parameters in 10 to 15 minutes, angiography is necessary.
Question 918
High Yield
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?
Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 919
High Yield
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 920
High Yield
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of

Explanation
The radiograph shows a type IIa Hangman's fracture, and the classic treatment is halo vest immobilization. Traction should be avoided in type IIa injuries because of the risk of overdistraction. A lesser form of immobilization such as a hard collar or a Minerva jacket can be used for nondisplaced (type I) fractures. Surgery generally is reserved for type III fractures (includes C2-3 facet dislocation), or extenuating circumstances such as multiple trauma or other fractures of the cervical spine that require surgical stabilization. Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 921
High Yield
Use of prophylactic knee bracing in contact sports participants results in which of the following?

Explanation
Several studies have looked at the effects of knee bracing, and it appears to be effective in prophylactically decreasing the incidence of medial collateral ligament sprains. Najibi and Albright reported that although evidence is not conclusive, bracing appears to help decrease the incidence of medial collateral ligament injuries. Albright and associates showed similar findings. Prophylactic knee braces have been associated with an increased incidence of ankle injuries. Albright JP, Powell JW, Smith W, et al: Medial collateral ligament knee sprains in college football: Effectiveness of preventive braces. Am J Sports Med 1994;22:12-18.
Question 922
High Yield
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
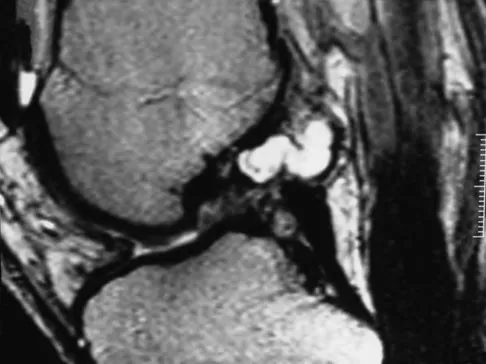
Explanation
Ganglia involving the cruciate ligaments have been recently reported as a cause of knee pain that interferes with knee flexion and extension. The symptoms are poorly localized in this patient and not along the medial joint line, making the diagnosis of a torn medial meniscus less likely. In addition, the MRI findings do not show a significant medial meniscal lesion. A Baker's cyst is usually posteromedial and extends posterior to the interval between the medial head of the gastrocnemius and semimembranosus. MRI scans show a fluid-filled lesion with an increased signal on T1- and T2-weighted images. A lipoma would be bright on the T1-weighted image only. Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Question 923
High Yield
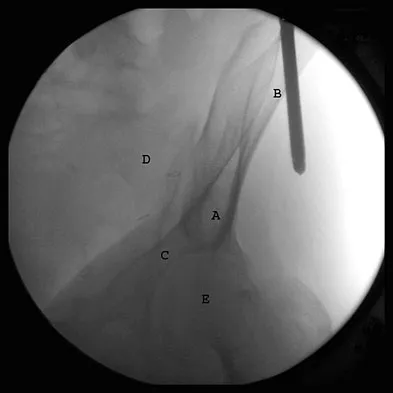
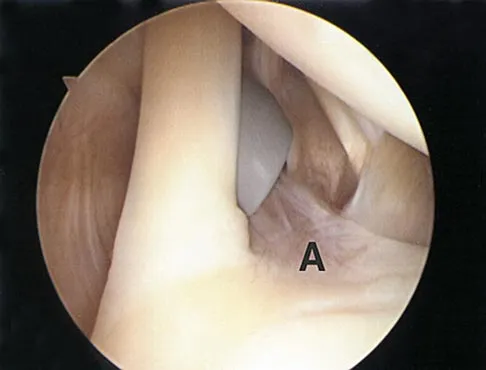
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 924
High Yield
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?


Explanation
The osseous sites most frequently involved by giant cell tumor of bone are the distal femur, proximal tibia, and distal radius with approximately 10% of giant cell tumors involving the distal radius. The goals of treatment are to remove the tumor completely and to preserve maximum function of the extremity.
Question 925
High Yield
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
The goal of fluid replenishment should be to replace the sweat that has been lost. Sweat is mostly water, with a small concentration of salts and other electrolytes. Absorption is enhanced by solutions of low osmolality. Scientific research has also shown that adding carbohydrates to the drink improves athletic performance. Carbohydrates such as glucose and maltodextrins (glucose polymers) stimulate fluid absorption by the intestines. Fructose slows intestinal absorption of fluids. Drinks that are high in fructose, such as orange juice, can lead to gastrointestinal distress and osmotic diarrhea. Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
Question 926
High Yield
Which of the following is most commonly associated with an open clavicular fracture?

Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 927
High Yield
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of



Explanation
The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
Question 928
High Yield
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 929
High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 930
High Yield
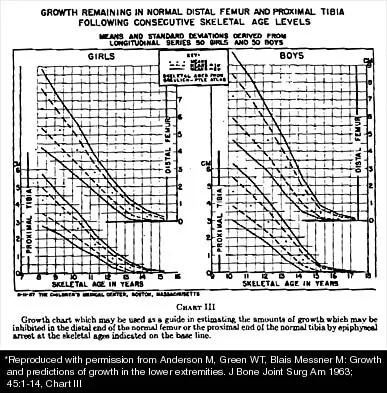
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 931
High Yield
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?

Explanation
The musculocutaneous nerve may be injured by retracting the conjoined tendon medially. This nerve enters the coracobrachialis 5 cm distal to its origin. Its sensory distribution is the radial forearm, and its motor supply is to the biceps and brachialis. Bach BR, O'Brien SJ, Warren RF, et al: An unusual neurologic complication of the Bristow procedure. J Bone Joint Surg Am 1988;70:458-460.
Question 932
High Yield
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 933
High Yield
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
The term 'spinal shock' applies to all phenomena surrounding physiologic or anatomic transection of the spinal cord that results in temporary loss or depression of all or most spinal reflex activity below the level of the injury. Hypotension and bradycardia caused by loss of sympathetic tone is a possible complication, depending on the level of the lesion. The mechanism of injury that causes spinal shock is usually traumatic in origin and occurs immediately, but spinal shock has been described with mechanisms of injury that progress over several hours. Spinal cord reflex arcs immediately above the level of injury also may be depressed severely on the basis of the Schiff-Sherrington phenomenon. The end of the spinal shock phase of spinal cord injury is signaled by the return of elicitable abnormal cutaneospinal or muscle spindle reflex arcs. Autonomic reflex arcs involving relay to secondary ganglionic neurons outside the spinal cord may be affected variably during spinal shock, and their return after spinal shock abates is variable. The returning spinal cord reflex arcs below the level of injury are irrevocably altered and are the substrate on which rehabilitation efforts are based.
Question 934
High Yield
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
All other factors being equal, a patient's age is the most important factor in determining outcome after peripheral nerve injury. Repair of a nerve laceration within the first 2 weeks is generally considered appropriate. Fascicular repair may be of benefit in larger proximal nerves to reapproximate appropriate nerve bundles; distally perineural or epineural repair is sufficient. Use of a fibrin tissue sealant for nerve repair does not result in improved outcomes over suture repair. Nerve conduits have shown promise in digital nerves but do not have proven benefit in larger caliber nerves. Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991. Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325. Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Question 935
High Yield
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 936
High Yield
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of

Explanation
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition. Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Question 937
High Yield
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?

Explanation
The most common deleterious side effect of ketamine is increased salivation and tracheobronchial secretions. For this reason, an antisialagogue agent should be given. While lack of sufficient respiratory depression is one of the major advantages of using ketamine, apnea can occur if the drug is given too rapidly intravenously. Emergence phenomena is common in adults but relatively rare in children. Furman JR: Sedation and analgesia in the child with a fracture, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 62-63. White PF, Way WL, Trevor AJ: Ketamine: Its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-136.
Question 938
High Yield
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
The mainstay of early treatment of open fractures includes irrigation and debridement. Prior to the development of antibiotics, this was traditionally accomplished with some form of detergent irrigation. Antibiotic irrigation has been in favor more recently but has mixed scientific results related to its use. Results of at least one major study show the use of a nonsterile liquid soap additive (castile soap) is at least as effective as the use of bacitracin with regards to the rate of postoperative infection and fracture healing, and shows a significant decrease in problems with soft-tissue healing.
