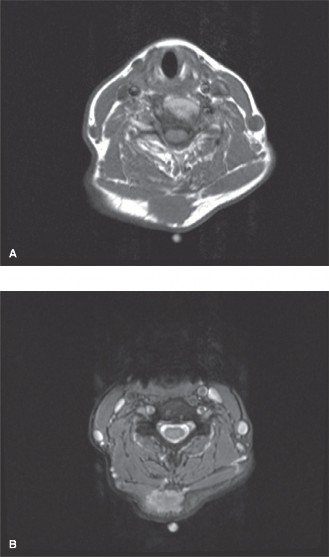
Discover the latest medical recommendations for Solving Complex Orthopedic Oncology Cases Schwannoma. Diagnosing a painless, slow-growing neck mass in orthopedic oncology cases, like a desmoid tumor or potentially a schwannoma, requires careful evaluation. Desmoid tumors are benign but locally aggressive fibrous neoplasms needing biopsy for definitive diagnosis; imaging alone is insufficient. Treatment typically involves surgical resection, sometimes followed by radiation, highlighting the complex management of such soft tissue lesions.
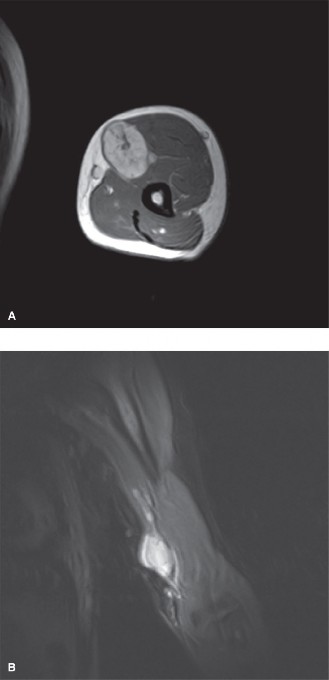
Differences between pre- and postoperative radiation treatment? **CASE 21** A 40-year-old male presents to your office with a chief complaint of pain and tingling down his left arm. He complains of some numbness at his fingertips. He notes that about 6 months ago, he noticed a growing lump in his upper arm. It has
[been growing slowly over time, and his symptoms have gotten worse. The area is relatively tender to palpation, and there is a positive Tinel sign with deep palpation of the mass, replicating his symptoms. MRI is shown in ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%208.%20Orthopaedic%20Oncology_Converted.html#bookmark33)[Figure ](file:///C:/Users/DELL/Desktop/hip/board/Chapter%208.%20Orthopaedic%20Oncology_Converted.html#bookmark33)8–26A [and ](#bookmark33)B.

## _Discussion_
The correct answer is (D). The history suggests a nerve tumor based on the neurologic symptoms and the Tinel sign. The MRI shows characteristic findings of Schwannoma as discussed below.
* **Which of the following are not characteristic MRI findings? [View Source / PubMed]
4. Infiltrative pattern eroding into neighboring bone
## _Discussion_
The correct answer is (D). Schwannoma is a benign soft-tissue tumor of Schwann cells. These tumors grow eccentrically from the nerve sheath and do not involve the nerve fibers themselves, therefore they can be surgically removed from the neighboring nerve, usually without causing any permanent nerve damage. Imaging studies reveal an oval mass which can often be seen to be continuous with a nerve fiber. A “split fat” sign is usually seen and can help make the diagnosis. These tumors demonstrate low signal intensity on T1 and high signal intensity on T2, with diffuse gadolinium enhancement. A central target may be seen on T1-weighted images, which is well demonstrated in this study. The tumor can produce peripheral nerve symptoms, and are generally firm and quite painful. Tapping the tumor with a finger can reproduce the nerve symptoms, which is called a Tinel sign. These tumors are benign and do not grow in an infiltrative pattern into neighboring bone.
* **Histologic examination performed on an incisional biopsy sample from the lesion reveals palisading and distinct Antoni A and Antoni B areas. What staining antibody could be used to support the diagnosis? [View Source / PubMed]
4. Schwann cells disintegrate with immunohistochemical staining, therefore no test is indicated
## _Discussion_
The correct answer is (B). Schwannomas and other nerve tumors strongly stain positive for the S100 antibody. Although S-100 is not diagnostic of schwannoma, in the setting of appropriate imaging and histology, it is supportive of the diagnosis. CD-28 is used to aid in the diagnosis of multiple myeloma, and CD-99 is associated with Ewing sarcoma. **Objectives: Did you learn...?**
Clinical and imaging features of schwannoma? Histological features of schwannoma? [View Source / PubMed]
 🔍 Click to enlarge
🔍 Click to enlarge