A 56-year-old male is referred to your office by his primary physician, with concern for metastatic disease. He has lytic lesions found throughout his skeleton, including in the left iliac crest and proximal femur. The iliac crest lesion is biopsied for diagnosis confirmation. Histology image is shown in Figure 8–15.
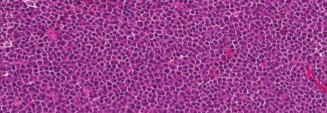
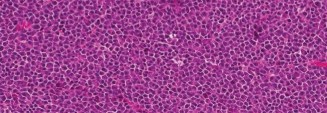
Figure 8–15
What is the correct diagnosis?
- Ewing sarcoma
- Metastatic prostate cancer
- Metastatic renal cell carcinoma
- Multiple myeloma
Discussion
The correct answer is (D). This slide shows typical features of multiple myeloma. On histopathologic examination, multiple myeloma consists of sheets of pleomorphic plasma cells with eccentric nuclei and abundant eosinophilic cytoplasm. The loose chromatin within the nucleus is arranged in the periphery, in a “clock-faced” pattern. Metastatic carcinomas have the appearance of the primary organ and can often be recognized in bone by the presence of glands, not seen in this slide. Ewing sarcoma is a small, round blue cell tumor, in which the cells have very little cytoplasm, as opposed to the abundant cytoplasm is myeloma cells.
Which immunohistochemistry stain is diagnostic for multiple myeloma?
- CD-99
- S-100
- CD-28
- Keratin
Discussion
The correct answer is (C). CD-28 is the immunohistochemistry stain associated with multiple myeloma. Ewing sarcoma is associated with CD-99 positivity, S-100 is a marker for malignant nerve sheath tumors and melanocytes, and keratin staining is nonspecific for many carcinomas.
The patient has a lytic lesion in the left proximal femur which is shown in Figure 8–16. He has pain with weight bearing and resultant ambulatory dysfunction. What would you recommend at this time regarding this finding?
- Prophylactic fixation of femur with long cephalomedullary device
- Prophylactic fixation of femur with dynamic hip screw construct
- Cytotoxic chemotherapy in combination with dexamethasone
- Bisphosphonate therapy
 🔍 Click to enlarge
🔍 Click to enlargeClinical Radiograph / Orthopedic Image
Figure 8–16
Discussion
The correct answer is (A). The patient’s lytic lesion represents an impending pathologic fracture of the proximal femur, and he meets the criteria for undergoing prophylactic stabilization with a long cephalomedullary device. This is preferred to a dynamic hip screw because it provides stabilization to the entire femur, so that if a second lesion were to develop in the future in the same bone, it would not require any further surgery. If there were involvement of the femoral head, an arthroplasty procedure would be more appropriate. While multiple myeloma lesions are also treated with chemotherapy, bisphosphonates, and radiation, these treatment strategies should not replace surgical fixation of an impending fracture.
Objectives: Did you learn...?
Histology of myeloma?
Treatment of myeloma bone disease?
