Score: 0%
Orthopedic MCQS Trauma 0018
A 32-year-old man has a closed mid-shaft spiral humeral fracture after a fall. After a discussion of his treatment options, he wants to proceed with surgical management. When counseling him about open reduction internal fixation (ORIF) versus intramedullary nailing (IMN), what is the primary difference in outcomes between the two procedures?
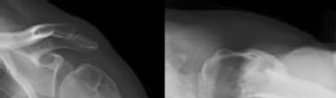
Figure 1 is the radiograph of a 49-year-old man who sustained a closed injury to his
left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---



left shoulder in a motor vehicle collision. He underwent uncomplicated ORIF (see Figure 2), but at his first post-operative visit he had persistent pain and deformity (see Figure 3). What is the primary factor contributing to this complication?
---
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
A pathognomonic radiographic feature of this injury is a
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What is the typical intra-operative patient position for treatment of this injury?
---

Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What is the typical intra-operative patient position for treatment of this injury?
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
The surgical exposure that provides optimal visualization to treat this injury is
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
The surgical exposure that provides optimal visualization to treat this injury is
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---

Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function.
What type of screws should be available for stabilization of this injury?
---
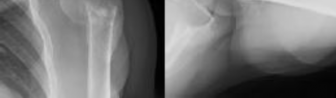
Figures 1 and 2 are the radiographs of a 46-year-old man with left shoulder pain and
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
limited range of motion two years after a proximal humerus fracture, which was treated non-operatively. He has forward elevation to 100 degrees with pain at the terminal arc of motion. A subsequent MRI reveals no soft tissue abnormality. After a failed course of non-operative treatment, what is the most appropriate surgical treatment?
---
Figures 1 and 2 are the radiographs of a 44-year-old man who comes to the
emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure


emergency department after a fall from a ladder with pain and a closed injury to his left shoulder. He undergoes open reduction internal fixation (ORIF) of his left proximal humerus fracture. A postoperative radiograph is shown in Figure
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---


Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
What represents the best indication for surgical management of the humeral shaft fracture in this patient?
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---


Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
After a discussion with the patient, surgery is chosen for the right humerus. A posterior triceps-reflecting approach is selected. What structure marks the most proximal extent of the humerus that can be exposed through this approach?
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
Postoperative radiographs are shown in Figures 3 and




Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
Postoperative radiographs are shown in Figures 3 and
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
The working length of the plate is best described as the length
---
---


Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity.
The working length of the plate is best described as the length
---
---
What is the best treatment option for complex proximal humerus fractures in the
low-demand patient population?

low-demand patient population?
**CLINICAL SITUATION**
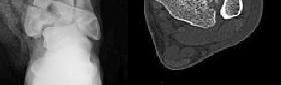
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
Three years following surgery, which parameter will most likely predict a poor clinical outcome and failure to return to work?
---
---

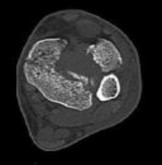
Figure 1 is the radiograph and Figure 2 is the CT image of a 45-year-old woman who fell about 20 feet off her balcony. These images show an isolated, open injury with a 3-cm open medial wound.
Three years following surgery, which parameter will most likely predict a poor clinical outcome and failure to return to work?
---
---
**CLINICAL SITUATION**
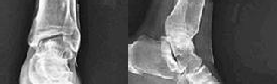
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after
---
---


Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---


Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic instability best assessed intra-operatively?
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---

Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Our understanding of malreduction of the syndesmosis has changed over the years based on changes in technique and imaging. Our current understanding is that malreduction of the syndesmosis
---

Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Our understanding of malreduction of the syndesmosis has changed over the years based on changes in technique and imaging. Our current understanding is that malreduction of the syndesmosis
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---

Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
What is the morphology of the posterior malleolar fracture component?
---
---


Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
What is the morphology of the posterior malleolar fracture component?
---
---
**CLINICAL SITUATION**
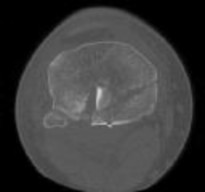
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---








Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---


Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---



Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
This knee injury is best described as a
---
---
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---



Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Initial surgical management should consist of
---
---
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---






Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
Figures 4 through 8 are the axial and coronal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be
---
---
---
---
---
---
---
---
**CLINICAL SITUATION**
Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
---



Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal.
The surgical approach for definitive reduction and stabilization of this pattern is
---
---
---
**CLINICAL SITUATION**
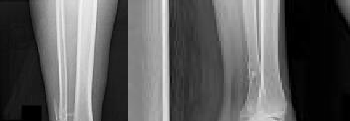
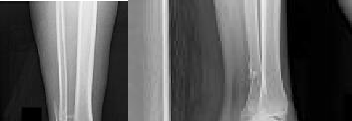
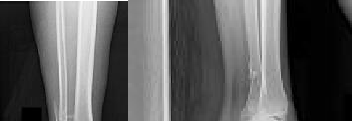
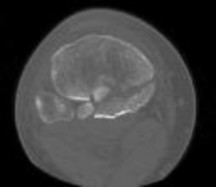
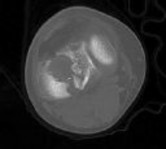
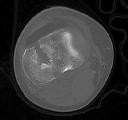
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
What is the best next step in the patient’s evaluation?
---




Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
What is the best next step in the patient’s evaluation?
---
**CLINICAL SITUATION**
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Based on the radiographs shown in Figures 1 and 2, her tibia is a
---
---
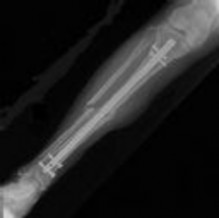
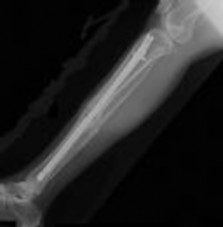
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Based on the radiographs shown in Figures 1 and 2, her tibia is a
---
---
Suprapatellar intramedullary nailing for tibia fractures when compared to
infrapatellar nailing is associated with
infrapatellar nailing is associated with
**CLINICAL SITUATION**
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Assuming her workup is negative for any other causes, what is the best treatment option?
---


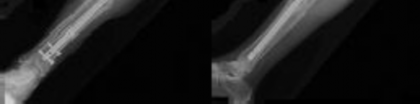
Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities.
Assuming her workup is negative for any other causes, what is the best treatment option?
---
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?
---

---
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
A 58-year-old man has a painful, warm, erythematous and fluctuant area over his left olecranon. An aspiration would be most likely to reveal
A 65-year-old woman with type II diabetes mellitus (most recent Hgb A1C was 8.2) has had 3 days of left knee pain. Physical examination of the left knee reveals erythema, warmth and a large effusion. Range of motion is painful and limited to 30 degrees of flexion. She is found to be hypotensive and not responding to volume resuscitation. She requires phenylephrine to maintain Mean Arterial Pressure (MAP) of 70. ESR and CRP are elevated and Lactate is 3.1 mmol/L. What is the next best intervention for this patient’s treatment?
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?
---
---



---
---
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---

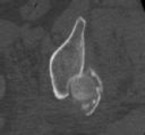

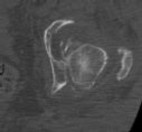

Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
Which factors will lead a surgeon to pursue fracture fixation and acute total hip arthroplasty instead of fixation alone?
---

Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
Which factors will lead a surgeon to pursue fracture fixation and acute total hip arthroplasty instead of fixation alone?
---
**CLINICAL SITUATION**
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---

Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
In this patient, what other potential injury can be associated with this fracture pattern and is commonly overlooked?
---
