Orthopedic Sport Review | Dr Hutaif Sports Medicine Rev -...
Updated: Feb 2026
60 Views
Key Medical Takeaway
We review everything you need to understand about Orthopedic Mcqs Sport 0019. The question of a 54-year-old man’s shoulder arthroscopy reveals double-row rotator cuff repair techniques demonstrate superior results in reducing the retear rate compared to single-row methods for small and medium-sized tears. This is due to a stronger initial repair construct. Studies show no significant difference in time to healing, functional outcomes, or postsurgical pain scores.
Score: 0%
Orthopedic Mcqs Sport 0019
QUESTION 1
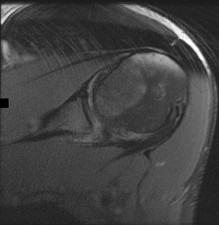
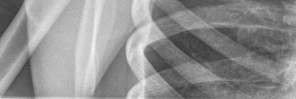
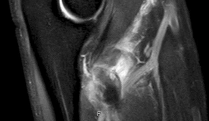
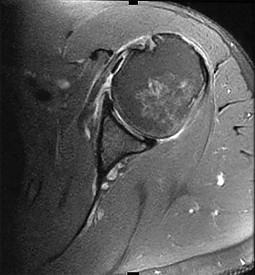
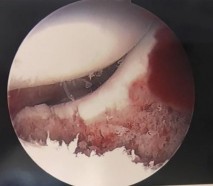
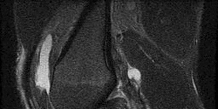
Figures 1 and 2 are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared with traditional arthroscopic techniques when evaluating which outcome? ---
1
Time to healing
2
Retear rate
3
Functional outcome scores
4
Postsurgical pain scores
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the two techniques.
QUESTION 2
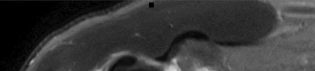
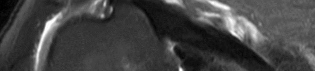
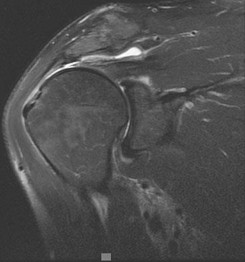
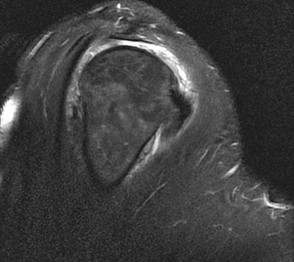
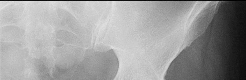
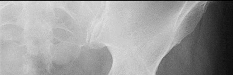
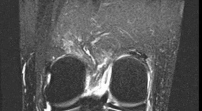
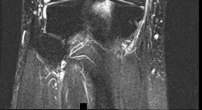
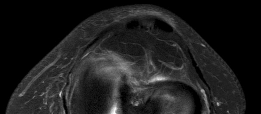
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario? ---
1
Recurrent instability
2
Degenerative joint disease
3
Shoulder stiffness
4
Axillary nerve injury
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
QUESTION 3
Figure 1 is the MRI scan of a 19-year-old man who has an acute anterior shoulder dislocation. The bony fragment occupies 10% of the glenoid articular surface. What is the most appropriate treatment? ---
1
Open structural iliac crest graft
2
Open reduction and internal fixation
3
Arthroscopic coracoid transfer
4
Arthroscopic repair incorporating the bone lesion
The MRI scan shows a bony Bankart lesion involving <20% of the glenoid joint surface. A recent series reported high success rates after arthroscopic treatment when the defect is incorporated into the repair. Anterior bony deficiencies occupying >25% to >30% of the glenoid joint surface treated with soft-tissue repair only are associated with high recurrence rates. In these patients, an open or arthroscopic coracoid transfer or structural iliac crest graft should be considered. Open reduction and internal fixation has been reported for treatment of large acute glenoid rim fractures but is not recommended for recurrent anterior shoulder instability in the setting of a 10% glenoid rim fracture.
QUESTION 4
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate
external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
1
Calcified transverse scapular ligament
2
Parsonage-Turner syndrome
3
Spinoglenoid notch cyst
4
Quadrilateral space syndrome
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
QUESTION 5
A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment
consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
1
Anterior and superior acromioclavicular joint ligaments
2
Posterior and superior acromioclavicular joint ligaments
3
Conoid ligament
4
Trapezoid ligament
The posterior and superior acromioclavicular ligaments provide the most restraint to posterior translation of the acromioclavicular joint and must be preserved during a Mumford procedure. Anterior and superior acromioclavicular joint ligaments are the opposite of the preferred response and prevent anterior translation of the clavicle. Injuries to the conoid and trapezoid ligaments are more pronounced with grade III or higher acromioclavicular separations, with superior migration of the clavicle relative to the acromion.
QUESTION 6
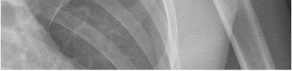
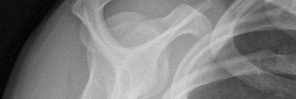
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
1
axillary nerve.
2
musculocutaneous nerve.
3
median nerve.
4
radial nerve.
---
--- DISCUSSION:
The patient has undergone a Latarjet procedure as shown in the radiographs. After harvesting the coracoid graft, care must be taken to not place too much tension on or dissect excessively near the musculocutaneous nerve. The nerve is encountered 5 cm distal to the coracoid as it enters the conjoint tendon. The lateral antebrachial cutaneous nerve is the terminal branch of the musculocutaneous nerve and; therefore, injury can cause decreased sensation in the lateral forearm.
QUESTION 7
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.The most substantial functional deficit that may develop if no surgical treatment is provided is
1
elbow flexion strength.
2
elbow supination strength.
3
lack of terminal extension at the elbow.
4
decrease of elbow pronation strength.
This patient had an eccentric muscle contraction (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors
have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
QUESTION 8
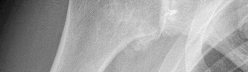
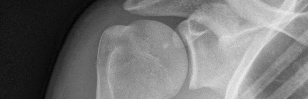
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient? --- ---
1
Range of motion
2
Infraspinatus strength
3
Activity level
4
Quality of the subscapularis
The radiographs show severe osteoarthritis of the shoulder. The best surgical option would be an arthroplasty. The major determining factor for which type of arthroplasty to choose is the integrity of the rotator cuff tendons.
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
QUESTION 9
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain? ---
1
Forward elevation in the scapular plane
2
External rotation and abduction
3
Flexion, adduction, and internal rotation
4
Flexion and abduction
This patient has a mechanism of injury and MRI scan consistent with a posterior labral tear and posterior instability. Flexion, adduction, and internal rotation produce a net posterior vector on the glenohumeral joint and should reproduce this patient's symptoms. Pain or instability with the arm elevated in the scapular plane describes an impingement sign. Pain or instability with the arm in external rotation and abduction describes the apprehension sign. Pain or instability with the arm in flexion and abduction is a _nonspecific finding._
QUESTION 10
A 13-year-old right-hand dominant pitcher was treated for Little League shoulder. What finding increases his risk of recurrence?
1
Hyperlaxity
2
Rotator cuff weakness
3
Increased height
4
Glenohumeral internal rotation deficit
Little League shoulder is a physeal injury increasingly seen in young throwers. The primary treatment is refraining from throwing with rehabilitation, followed by a throwing program. The risk of recurrence is approximately 7%. The risk of recurrence is three times higher in athletes with glenohumeral internal rotation deficit. Hyperlaxity,
rotator cuff weakness, and increased height have not been shown to correlate with recurrent symptoms.
QUESTION 11
Figures 1 and 2 are the MR arthrogram images of a 20-year-old right-hand dominant collegiate basketball player who sustained an initial shoulder dislocation 1 year ago. In the month prior to presentation, he dislocated his shoulder two more times. Each time it occurred when going up for a rebound and an opponent grabbed the ball from behind him, hyperextending his shoulder. Physical examination demonstrates full range of motion, absence of atrophy, a positive apprehension sign and relocation test, and a positive Kim test. What is the best next step? --- ---
1
Anterior labral repair
2
Anterior labral repair and remplissage
3
Posterior labral repair and rotator interval closure
4
Anterior and posterior labral repair
The mechanism of injury/dislocation is most consistent with anterior glenohumeral joint instability. The axial cuts of the MR arthrogram reveals an anteroinferior labral tear, as well as a posterior labral tear. A Hill-Sachs lesion is also consistent with anterior glenohumeral joint instability. At the time of examination under anesthesia, this patient exhibited 2+ anterior and 2+ posterior glenohumeral joint instability. Patients with pan-labral tears and 270° tears can be challenging to diagnose, because patients can report anterior or posterior shoulder instability alone. The
physical examination and advanced imaging in these patients are crucial in directing appropriate treatment.
QUESTION 12
A 23-year-old student complains of recurrent left shoulder instability. He first dislocated his shoulder in high school while playing lacrosse and was managed with physical therapy. A second dislocation occurred one year later while skiing. He has since sustained two more dislocations and says that his shoulder feels “loose.” Examination reveals grade II anterior load and shift, positive apprehension and relocation tests, and normal rotator cuff strength. An MRI arthrogram is ordered and surgical treatment is recommended. What factor would most strongly represent an indication for a procedure including bone augmentation (e.g. Latarjet) rather than a soft-tissue-only stabilization (isolated labral repair/capsulorrhaphy)?
1
Patient’s intention to resume lacrosse and other contact sports after surgery
2
Presence of a 270° labral tear
3
2-cm “on-track” Hill-Sachs lesion
4
Anterior bony loss measuring 30% of inferior glenoid width
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Barring other factors or concomitant pathology, however, there is no persuasive literature to suggest routine use of bone augmentation for contact athletes. Extensive labral involvement (here specifically implying posterior labral involvement, as well) will require a more extensive repair but does not, in and of itself, suggest the necessity for
glenoid bone augmentation. A large Hill-Sachs lesion may be an indication for glenoid augmentation, primarily if it is in a location/orientation that engages the anterior glenoid rim. These are referred to as “off-track” lesions. Of these choices, the strongest indication for a Latarjet coracoid transfer or similar bone augmentation (other options include iliac crest autograft or distal tibial allograft) is high-grade glenoid bone loss. Classically, this is performed through an open approach, although arthroscopic techniques are increasing in popularity. Although the critical amount of bone loss is debated, most surgeons and studies suggest a cut-off of approximately 20% to 25%, above
which isolated soft-tissue stabilization alone is less likely to be successful in the long-term.
QUESTION 13
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. The athlete undergoes repair of the injury, and postsurgical radiographs are shown in Figures 1 and
1
At his first postsurgical visit, he reports no pain but describes weakness in his hand and decreased sensation over his lateral forearm. Upon examination, he has decreased 2-point discrimination over the lateral forearm and an inability to actively extend his thumb and fingers at the metacarpophalangeal joints. He can extend at the finger interphalangeal joints. He can extend his wrist weakly, and it deviates radially as he extends. His distal sensation is intact. Considering his examination findings, which two nerves are injured?




2
PIN and radial nerve
3
PIN and lateral antebrachial cutaneous nerve (LABCN)
4
Median nerve and LABCN
5
Radial nerve and LABCN
This patient had an eccentric muscle contraction (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the
elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
---
QUESTION 14
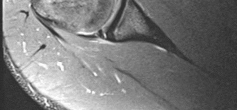
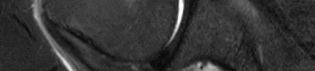
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
1
Subscapularis tear
2
Supraspinatus tear
3
Superior labral anterior-posterior (SLAP) tear
4
Bankart tear
The axial MRI scan reveals a subluxated biceps tendon. In the study by Koh and associates, 85% of patients with a biceps subluxation on MRI were found to have a subscapularis tear at the time of arthroscopy. These are not always obvious on the MRI, and close inspection of the leading edge/upper border of the subscapularis tendon at the time of arthroscopy is necessary. Although supraspinatus tears, SLAP tears, and Bankart tears can all occur in conjunction with a biceps subluxation, none have been shown to be strongly correlated with this pathology, nor as
specific to this pathology.
QUESTION 15
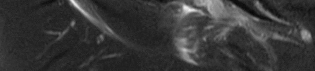
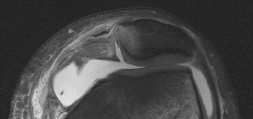
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness? ---
---
1
Axillary nerve injury
2
Cervical radiculopathy involving the C6 nerve root
3
Massive rotator cuff tear with loss of the transverse force couple
4
Long head of the biceps tendon rupture with loss of superior stabilizing effect
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation, and loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction. Active shoulder elevation <90 degrees in the presence of full passive motion is termed pseudoparalysis. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve. This patient's sensory examination suggests that the axillary nerve is intact. Cervical radiculopathy is less common after shoulder dislocation but has been reported. Conflicting evidence exists regarding the contribution of the long head of the biceps tendon to glenohumeral stability. One study reported minimal electromyographic activity in the biceps during ten basic shoulder motions.
QUESTION 16
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out
with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. Which type of contraction of the involved muscle most likely resulted in this lineman's injury?
1
Eccentric
2
Concentric
3
Isometric
4
Isokinetic
This patient had an eccentric muscle contraction (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
QUESTION 17
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan? --- ---
1
Arthroscopic infraspinatus tenodesis
2
Arthroscopic posterior labral repair
3
Arthroscopic capsular shift and rotator interval closure
4
Posterior glenoid opening-wedge osteotomy
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
QUESTION 18
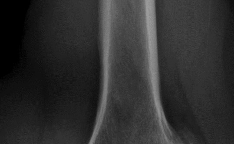
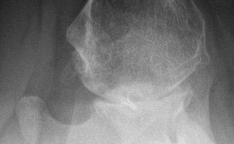
Figure 1 is the radiograph of an 11-year-old baseball pitcher who has had right shoulder pain for the past 3 months. He has full range of motion and normal strength in both external rotation and abduction,
although all tests cause him discomfort over the lateral and anterior shoulder. What is the most likely basis for his injury? ---
1
Increased external rotation with an associated decrease in internal rotation
2
Excessive pitch counts
3
Use of breaking pitches such as sliders and curve balls
4
Congenital humeral cyst
The radiograph reveals a widened lateral physis at the proximal humerus, consistent with a physeal stress fracture or “Little Leaguer’s shoulder.” Numerous studies have established that children and adolescents are particularly prone to such overuse injuries. With regard to baseball participation, a major contributor is over-pitching, i.e., excessive numbers of pitches, excessive innings pitched, and insufficient rest days. Altered range of rotational motion, a gradual adaptation to the increased stresses of throwing, can predispose to long-term injury, especially internal impingement and labral pathology. A unicameral or aneurysmal bone cyst can often occur in the proximal humerus, but has a distinct radiographic appearance and would predispose to fracture. There is evidence that breaking pitches place increased stresses on the elbow and shoulder, but it remains controversial whether such
throws should be avoided at certain ages.
QUESTION 19
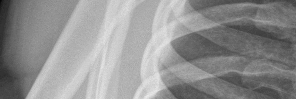
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation? --- ---
1
Arthroscopic Bankart procedure
2
Physical therapy
3
SAWA shoulder brace
4
Latarjet procedure
The patient has recurrent instability and is at a high rate of further dislocations due to his young age. Therefore, therapy and bracing are unlikely to decrease his dislocation rate. The radiographs are normal, and there is no Hill-Sachs lesion or bony Bankart lesion. His instability severity index score is 3, and; therefore, a bony procedure such as Latarjet is not necessary. Furthermore, the rate of complication following a Latarjet procedure, especially nerve
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
QUESTION 20
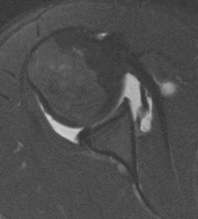
Figures 1 and 2 are the right shoulder MRI scans of a 22-year-old right-handed professional male volleyball player with 4 months of right shoulder pain. The pain began insidiously and is exacerbated by overhead activities and hitting during games. He has maintained a daily program of shoulder stretching and strengthening exercises but has experienced a steady decline in function to the point of not being able to participate in volleyball. Examination reveals some mild atrophy at the posterior shoulder, full forward elevation, mild weakness of external rotation on the right shoulder, negative empty-can testing, positive O’Brien’s and negative apprehension. Surgical intervention would aim to resolve pathology related to which nerve? ---
1
Lower subscapular nerve
2
Suprascapular nerve at the spinoglenoid notch
3
Suprascapular nerve at the suprascapular notch
4
Axillary nerve
This athlete has a symptomatic posterior-superior labral tear, spinoglenoid notch cysts, and subsequent suprascapular nerve compression, as evidenced by the atrophy of the infraspinatus muscle on sagittal T1 MRI. The cyst is located at the spinoglenoid notch and is compressing the suprascapular nerve after it has innervated the supraspinatus but before innervation of the infraspinatus; hence, the atrophy of infraspinatus on examination and imaging. Compression of the suprascapular nerve at the suprascapular notch would lead to weakness and atrophy of both the supraspinatus and infraspinatus. The lower subscapular nerve innervates the teres major, as well as, with the upper subscapular nerve, the _subscapularis. The teres minor is innervated by the axillary nerve._
QUESTION 21
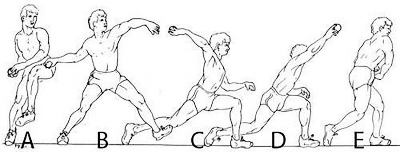
A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. Which phase of the throwing cycle shown in Figure 1 will most likely reproduce his symptoms? ---
1
A
2
B
3
C
4
D
This patient is experiencing soreness over his medial (ulnar) collateral ligament. Valgus overload is likely to reproduce his symptoms and is most pronounced during the late cocking phase of the throwing cycle. In windup, very little elbow torque is required. In early cocking, the arm is getting loaded, and maximum valgus is not yet achieved at the elbow. In acceleration and deceleration, more force is _generated at the level of the shoulder joint._
QUESTION 22
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. --- ---
Which of the four muscles of the rotator cuff provides the most resistance to this patient's direction of instability?
1
Subscapularis
2
Supraspinatus
3
Infraspinatus
4
Teres minor
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is
indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate.
QUESTION 23
A 47-year-old man who is an avid tennis player and laborer has had one year of shoulder pain and weakness. His pain occurs at night and radiates to the deltoid laterally. The patient denies any anterior based pain. He reports no prior surgeries and has been managed with steroid injections and physical therapy. On examination, he has full passive motion with significant weakness with external rotation. His neurologic examination is unremarkable. MRI evaluation reveals a posterior-superior rotator cuff tear with Goutallier grade 4 fatty infiltrate in the supraspinatus and infraspinatus with retraction beyond the glenoid. He is concerned about the lack of rotation of his arm and reports that this disability creates significant disability with his occupation as a mason. What is the best next step?
1
Shoulder scope and subacromial decompression
2
Tendon transfer
3
Total shoulder arthroplasty
4
Reverse total shoulder arthroplasty
In younger active patients, tendon transfer is considered a preferable treatment option. The patient has failed a course of nonoperative management. Subacromial decompression may offer pain relief but may not be advisable in a patient with rotator cuff deficient shoulder. A total shoulder arthroplasty requires functionality of the supraspinatus and infraspinatus. A reverse total shoulder is an option to alleviate pain and perhaps improve forward flexion height and strength; however, reverse arthroplasty would not improve external rotation in this patient, and there is concern for longevity of the implant in younger _patient populations._
QUESTION 24
Figures 1 and 2 are the MRI scans of a 35-year-old right-hand dominant man who has right elbow pain after trying to lift a large television at home. An examination reveals ecchymosis, an abnormal hook
test, and altered biceps muscle contour. What treatment is most likely to result in a satisfactory and predictable outcome? --- ---
1
Period of immobilization followed by physical therapy
2
Local corticosteroid injection
3
Surgical repair
4
Platelet-rich plasma (PRP)
Figures 1 and 2 show a full thickness distal biceps tendon rupture with proximal retraction. Edema is seen along the course of the distal biceps tendon, and the axial cut demonstrates the absence of tendon at the radial tuberosity. The sagittal cut demonstrates the stump of the proximally retracted biceps tendon. The biceps muscle contour is abnormal in appearance, demonstrating the classic “popeye” deformity. Nonsurgical treatment options result in predictable loss of supination and elbow flexion strength that is not desirable. A local corticosteroid injection would not improve strength, and there is no evidence to support the use of a PRP injection.
QUESTION 25
Figure 1 is the T2 coronal MRI scan(Massive atraumatic rotator cuff tear) of a 52-year-old woman with
a 6-month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
1
Tear size
2
Pain scale score
3
Strength deficit
4
Patient expectations
The MRI reveals a large full thickness supraspinatus tear. A large, prospective study showed that physical therapy can be effective in the treatment of atraumatic full-thickness rotator cuff tears. Patient expectations regarding the role of rehabilitation were the strongest predictor of surgery. Other factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator
cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
QUESTION 26
A 17-year-old high school football linebacker sustains an injury while making a tackle. His initial symptoms
are right shoulder pain, bilateral biceps weakness, and right arm numbness. The symptoms only last a few minutes, and he continues to play in the game. He tells his parents after the game, and they bring him to your office for evaluation the next day. He no longer has any symptoms, and his examination findings and cervical spine radiographs are normal. What is the best next step?
1
Allow him to continue playing football
2
Order an EMG
3
Observe and if symptoms are negative for one week, then a return to football
4
Order a cervical MRI scan
The football player had bilateral weakness indicating that the injury was more significant than a stinger. Stingers present with unilateral symptoms, and if they resolve, an athlete can return to sports. However, bilateral symptoms indicate cervical spine pathology, such as spinal stenosis, and warrant an MRI scan of the cervical spine. Despite the patient being able to continue playing in the game and having symptom resolution, a cervical MRI scan should be performed prior to return to sports.
QUESTION 27
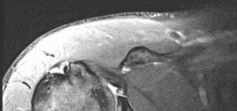
Figure 1 is the MR image of a 43-year-old man who has left shoulder pain and weakness after a fall. An examination reveals active forward elevation at 120° and positive Yergason and lift-off test examination findings. Arthroscopy reveals that the articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment at this time? ---
1
Rotator cuff repair and biceps tenodesis
2
Rotator cuff repair and loose body removal
3
Latissimus dorsi transfer
4
Bankart repair
The MR image shows medial subluxation of the biceps tendon, which can be confused with an articular loose body. In the clinical scenario of biceps instability/subluxation, the rationale regarding tenodesis is to address the painful dislocation and subluxation of the biceps tendon from the bicipital groove. Biceps tendon subluxation is most frequently associated with subscapularis tendon pathology, which is indicated by the MRI and by a positive lift-off test. The MR image does not show a loose body or Bankart lesion. Patients with irreparable rotator cuff tears with a severe external rotation deficit and a deficient teres minor _may experience a better functional result with latissimus dorsi transfer._
QUESTION 28
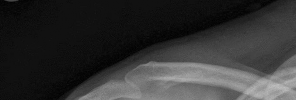
Figure 1 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snowboarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in ---
1
nonunion.
2
osteonecrosis.
3
altered rotator cuff mechanics.
4
normal shoulder function.
Humerus fractures account for 11% of all fractures among snowboarders and are the second-most-common upper-extremity fracture after radius fractures (48%). Surgical fixation is recommended for fractures with residual displacement >5 mm, or >3 mm in active patients involved in frequent overhead activity. Malunion can result in a mechanical block to shoulder abduction or external rotation and altered rotator cuff mechanics, causing weakness. A rich arterial network provides a favorable healing environment for greater tuberosity fractures. Consequently, nonunion and osteonecrosis are uncommon.
QUESTION 29
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement?
1
Age <20
2
Tonnis grade 2
3
Prominence of the femoral head in cam impingement
4
The patient is a professional athlete
A systematic review of case studies looking at the results of surgical treatment for femoroacetabular impingement shows good results for most patients, with the exception of those with preoperative radiographs showing osteoarthritis or Outerbridge grade III or grade IV cartilage damage noted intraoperatively. Both Byrd and Jones and Philippon and associates have shown good surgical results for this condition among professional athletes. Likewise, Fabricant and associates demonstrated good surgical results among adolescent patients with an average age of 17.6 years.
QUESTION 30
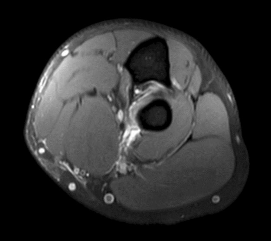
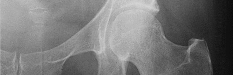
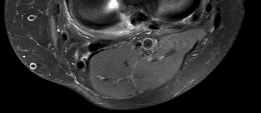
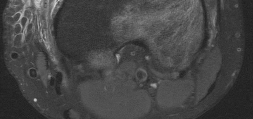
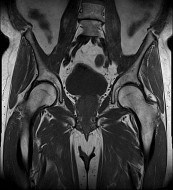
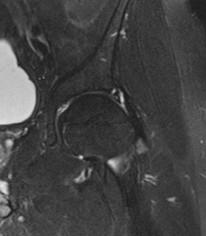
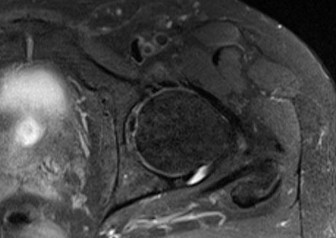
Figure 1 is the axial cut MRI scan of a 35-year-old woman who has had posteriorly based right hip pain
for 3 months. Examination demonstrates full and symmetric range of motion between the right and left hips, negative impingement test, but reproduction of her pain with passive extension of the right hip. Which muscle is indicated by the arrow? ---
1
Piriformis
2
Obturator internus
3
Superior gemellus
4
Quadratus femoris
This patient has ischiofemoral impingement, in which there is abnormal contact between the lesser trochanter and the lateral border of the ischium. Patients typically present with posteriorly based hip pain and do not respond to intra-articular diagnostic injections. Examination can demonstrate pain with long strides, pain with palpation over the area, as well as reproduction of symptoms with the patient in the contralateral decubitus position and taking the affected hip into passive extension (ischiofemoral impingement test). MRI demonstrates a narrowed ischiofemoral space, as well as increased signal within the quadratus femoris muscle. The diagnosis can be confirmed with a diagnostic injection into this area. Treatment is typically nonsurgical, with surgical intervention consisting of resection of the lesser _trochanter reserved for refractory cases._
---
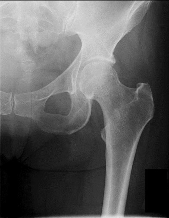
QUESTION 31
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intraoperatively, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
1
Debridement of the labral tear plus bony resection of the pincer lesion
2
Debridement of the labral tear and no bony resection of the pincer lesion
3
Femoral neck osteoplasty plus labral repair using suture anchor
4
Resection of the bony pincer lesion plus labral repair using suture anchor
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
QUESTION 32
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What is the most likely diagnosis for the source of this patient's pain? ---
1
Cam-type femoroacetabular impingement
2
Pincer-type femoroacetabular impingement
3
Hip flexor strain
4
Athletic pubalgia
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
---
QUESTION 33
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
1
Femoroacetabular impingement (FAI)
2
Osteoarthritis of the sacroiliac joint
3
Intra-articular loose body
4
Trochanteric bursitis
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
QUESTION 34
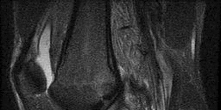
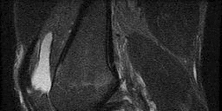
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step? ---
1
Hip arthroscopy with labrum repair
2
MRI arthrogram
3
Percutaneous screw fixation
4
CT scan with fine cuts
An osteoid osteoma is a benign bone tumor. Osteoid osteomas tend to be small—typically <1.5 cm. Regardless of their size, they cause a large amount of reactive bone to form around them, and they make a new type of abnormal bone material called osteoid bone. This osteoid bone, along with the tumor
cells, forms the nidus of the tumor, which is easily identified on CT scans.
QUESTION 35
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain? ---
1
Diagnostic arthroscopy of the hip
2
Hip bone scan
3
Hip MRI arthrogram
4
Hip ultrasonography
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
QUESTION 36
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. Images from an MRI scan of this patient's left hip are shown in Figures 3 through
1
What is the most likely cause of his acute pain?


2
Significant cartilage loss on the acetabulum
3
Labral tear
4
Femoral neck stress fracture
5
Tendinopathy of the rectus femoris
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of long-
standing groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a
periacetabular osteotomy can develop a more retroverted acetabulum as well.
QUESTION 37
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What examination findings are most consistent with the pathology seen in the radiographs? ---
1
Pain with resisted hip flexion
2
Pain with a half sit-up, plus tenderness at the pubic ramus
3
Pain with a combination of hip flexion, adduction, and internal rotation
4
Tenderness to palpation at the greater trochanter
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
QUESTION 38
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. Further workup confirms an anterosuperior tear of the acetabular labrum and prominence of the acetabulum. What is the most likely location of a chondral injury associated with these findings? ---
1
Posterosuperior acetabulum
2
Posteroinferior acetabulum
3
Femoral head above the fovea
4
Femoral head below the fovea
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
QUESTION 39
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1
Prior arthroscopy
2
Current smoking history
3
BMI of 22
4
Age of 40
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved
compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO _but does not influence technique._
QUESTION 40
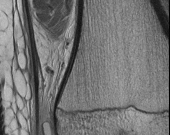
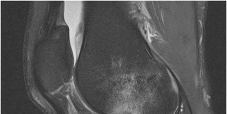
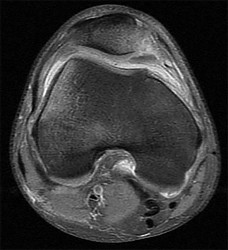
A football player injures his knee when he is tackled and falls awkwardly. He does not note any discreet “pop,” but pain prevents him from returning to the game. An effusion is noted the following day and an MRI scan is ordered. Selected images are shown in Figures 1 through
1
Based on these images, physical examination findings likely include



2
positive Lachman test, normal posterior drawer, positive pivot shift.
normal Lachman test, positive posterior drawer, positive pivot shift.
5
normal Lachman test, positive posterior drawer, negative pivot shift.
The images provided reveal a posterior cruciate ligament (PCL) disruption with an intact anterior cruciate ligament (ACL). Common diagnostic findings for a PCL tear include a positive posterior drawer test, positive reverse pivot shift, positive quadriceps active test, and positive posterior sag. A positive Lachman test, which would indicate a torn ACL, would not be expected to be positive. A false-positive result for a Lachman test can arise with a torn PCL because of the overall increased anterior-posterior translation; _this must be avoided by careful attention to initial resting position and station of the knee._
QUESTION 41
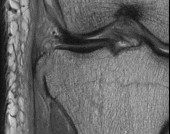
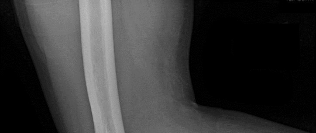
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured? --- ---
1
Lateral collateral ligament
2
Tibial spine
3
Medial meniscus
4
Anterior cruciate ligament (ACL)
This is a rupture of the anterolateral ligament complex and a portion of the IT band. This injury is highly correlated with a complete ACL injury. In the MRI, the curvilinear or elliptic bone fragment (Segond fracture) projected parallel to the lateral aspect of the tibial plateau, the lateral capsular sign, is seen. The lateral capsular sign is also associated with ACL tears. Thus, this is an MRI showing a complete ACL _tear._
QUESTION 42
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect? --- --- --- ---
1
Microfracture
2
Autologous chondrocyte implantation
3
Osteochondral allograft transfer
4
Dejour trochleoplasty
The images show a full-thickness cartilage defect with significant bony involvement >4 cm2. Microfracture should be considered for lesions <2 cm2 without an underlying osseous defect. Autologous chondrocyte implantation, although used for lesions between 1 and 10 cm2, should be restricted for defects with minimal (<8 mm depth) bone loss. Osteochondral allograft transfer with the mosaicplasty technique (transfer of multiple plugs) would be well-suited for this large defect with significant osseous involvement. Dejour trochleoplasty is performed for patellar instability to correct trochlear dysplasia and _would not be indicated in this case._
QUESTION 43
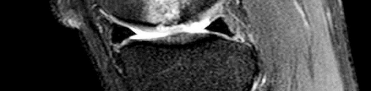
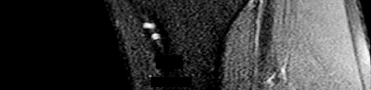
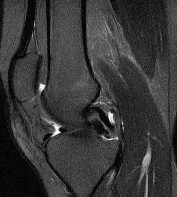
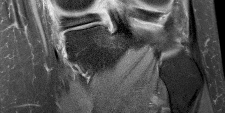
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time? --- --- ---
1
Lateral meniscus repair
2
Corticosteroid injection and physical therapy
3
Medial meniscus repair
4
Unloader brace
The MRI scan shows a posterior horn medial meniscus root avulsion with bony edema at the tibial root insertion. The radiograph shows no significant degenerative changes. If left untreated, posterior meniscal
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more _appropriate in the older patient with pre-existing advanced degenerative changes._
QUESTION 44
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings. What do Figures 1 and 2 reveal? ---
1
Medial femoral condyle physeal widening
2
An osseous or osteochondral loose fragment
3
Osgood-Schlatter disease
4
A patella nondisplaced fracture
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence and the need for reconstruction.
QUESTION 45
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by ---
1
accessory incisions.
2
use of tapered drill bits.
3
use of oscillating drills.
4
greater knee extension.
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases,
the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
QUESTION 46
Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgical option? --- ---
1
Revision ACL with bone-patellar tendon-bone (BTB) allograft and meniscal transplant
2
Distal femoral osteotomy
3
Pure sagittal osteotomy
4
Closing wedge and slope neutralizing high-tibial osteoto
Lateral closing wedge (LCW) and medial opening wedge (MOW) high-tibial osteotomies (HTOs) can both correct varus knee alignment and stabilize the ACL–deficient knee. Increasingly, HTO is being proposed as a singular or concomitant procedure with ACL reconstruction for restoring knee stability and as a more reliable slope correction. LCW HTO demonstrates more reliable slope correction than does MOW HTO. Revision ACL with BTB allograft and meniscal transplant will not help early arthritis in varus alignment. Distal femoral osteotomy is usually considered for valgus knee. Pure sagittal osteotomy _would not help the patient’s medial knee pain, arthritis, and malalignment._
QUESTION 47
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1
Hamstring autograft
2
Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3
Revision ACL reconstruction and posteromedial corner reconstruction
4
Revision ACL reconstruction and posterolateral corner reconstruction
This patient underwent an ACL reconstruction that has now failed. Based on his examination, he also has a posterolateral corner injury. Because this concomitant injury was not treated, the patient had undue strain on his graft, resulting in ultimate failure. Hamstring grafts are as effective as other graft types for ACL reconstruction. The medial meniscus provides secondary stabilization to the knee; however, this patient has a missed lateral ligamentous injury, and meniscus tears do not result in the development of a varus thrust. An unrecognized PCL tear likely results in mild-to-moderate medial and patellofemoral osteoarthritis without significant lateral laxity and thrust.
QUESTION 48
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior
knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
1
Physical therapy with a focus on quadriceps strengthening
2
Physical therapy and delayed posterior cruciate ligament (PCL) reconstruction
3
PCL reconstruction
4
PCL and posterolateral corner reconstruction
This patient has likely sustained an isolated PCL injury. The examination is consistent with a grade II injury to the PCL. In this scenario, the best initial option is nonsurgical treatment and return to play as symptoms subside and strength improves. Physical therapy with a focus on quadriceps strengthening and delayed PCL reconstruction is not the answer because this patient can likely be treated without surgery. The absence of valgus laxity and negative dial testing findings suggest that an injury to the posteromedial and posterolateral corners has not occurred. Initial nonsurgical treatment is indicated for this patient. If he completes rehabilitation and experiences persistent disability with anterior and/or medial knee discomfort or senses the knee is "loose," PCL reconstruction should be considered at that time.
QUESTION 49
An otherwise healthy 31-year-old man has had right knee pain for the past 9 months. His former physician
administered a cortisone injection and ordered 6 months of physical therapy. The patient later had an arthroscopy with debridement of the right knee by another physician and completed another course of physical therapy. The patient received minimal relief from these treatments and still is not able to walk longer distances or go on hikes. On examination, he is a healthy appearing male with a body mass index of 24 kg/m2. He has a small effusion, minimal quadriceps atrophy, no tenderness about the knee, full range of motion, stable to varus and valgus stress at 30° of flexion, a grade 1 Lachman test, and a normal posterior drawer. Figures 1 through 4 are his arthroscopic views, radiograph and MRI scan from his prior surgical procedure. What is the next most appropriate step in treatment? --- --- --- ---
1
Bracing with physical therapy focusing on quadriceps/vastus medialis obliquus (VMO) and hamstring strengthening
2
Osteotomy
3
Osteochondral allograft to femoral condyle
4
Arthroscopy with femoral condyle microfracture
The patient has a symptomatic cartilage lesion of his medial femoral condyle, which has not responded to nonsurgical measures, and he failed a prior arthroscopy with debridement. Based on his examination and imaging, he is ligamentously stable, has normal mechanical alignment, and has intact menisci, making him a candidate for a cartilage restoration procedure. The accompanying MRI also indicates subchondral bone involvement with increased T2 signal underlying the cartilage defect. Osteochondral allograft is the only choice that addresses both the cartilage defect, as well as compromised subchondral bone. Depending on lesion size, osteochondral autograft transfer may also be considered, but this is not presented as an answer choice.Given the radiographic finding of neutral mechanical alignment, bracing would be less effective, and the patient has already tried extensive physical therapy. Lack of malalignment also excludes tibial osteotomy as a preferred answer choice. Microfracture is best for small cartilage lesions without _significant bone marrow involvement._
QUESTION 50
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of
flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. What is the most appropriate next step in treatment?
1
Repeat corticosteroid injection
2
Trial of a medial unloader brace
3
MRI scan of the knee to evaluate for recurrent medial meniscus tear
4
Referral to pain management
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO _but does not influence technique._
QUESTION 51
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the next diagnostic step?
1
Repeat radiographs while the patient is weight bearing
2
Ultrasonography of the lower extremity and calf
3
Stress radiographs
4
CT scan
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a _cylindrical or long-leg cast._
QUESTION 52
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an ---
1
anterolateral bundle that is tight in flexion and a posteromedial bundle that is tight in extension.
2
anterolateral bundle that is tight in extension and a posteromedial bundle that is tight in flexion.
3
anteromedial bundle that is tight in flexion and a posterolateral bundle that is tight in extension.
4
anteromedial bundle that is tight in extension and a posterolateral bundle that is tight in flexion.
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
QUESTION 53
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis? --- --- --- --- ---
1
Symmetric knee pathology
2
Excessive joint laxity
3
Recurrent patella instability
4
Extra-articular manifestations
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
QUESTION 54
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion
between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the most likely area of injury?
1
Femoral attachment of the medial collateral ligament
2
Tibial attachment of the medial collateral ligament
3
Hypertrophic zone of the growth plate
4
Proliferative zone of the growth plate
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast.
QUESTION 55
A 20-year-old healthy female endurance athlete has lower leg pain and dorsal foot paresthesias after
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
**Baseline**
**1 Minute**
**5 Minutes**
---|---|---|---
**Anterior**
7
32
25
**Lateral**
8
29
23
**Superficial Posterior**
12
25
17
**Deep Posterior**
14
22
16
The patient decides to pursue surgical intervention. Which compartments should be released?
1
Anterior and lateral
2
Anterior, lateral, and deep posterior
3
Anterior, lateral and superficial posterior
4
Lateral and superficial posterior
The diagnostic criteria for chronic exertional compartment syndrome is pressure >15 mm Hg at rest, or
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible _for the patient's symptoms and falls below current thresholds for diagnosis._
QUESTION 56
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. Knee range of motion is between 0° and 70°. What is the most appropriate treatment option? ---
1
Open reduction and internal fixation of the lateral condyle
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibial plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated versus nonaccelerated rehabilitation programs have demonstrated no significant differences in long-term results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
QUESTION 57
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal? --- --- --- ---
1
Posterior cruciate ligament (PCL) tear, isolated
2
PCL tear and medial meniscus tear
3
Anterior cruciate ligament (ACL) tear, isolated
4
ACL tear and medial meniscus tear
The MRI scans show that edema is noted on the femoral insertion of the ACL consistent with a high-grade or complete ACL tear. The ACL is not visualized on the sagittal view, although the torn meniscus can be seen in the notch. On the coronal image, there is an empty lateral wall sign indicating proximal
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly _indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear._
QUESTION 58
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience ---
1
increased laxity.
2
increased risk for graft failure.
3
no differences in long-term results.
4
lower Knee Injury and Osteoarthritis Outcome Score (KOOS).
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibial plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated versus nonaccelerated rehabilitation programs have demonstrated no significant differences in long-term results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft _failures, or KOOS scores._
QUESTION 59
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment? ---
1
Arthroscopic or open reduction and internal fixation
2
Arthroscopic loose body removal
3
Activity restriction for up to 9 months
4
Subchondral drilling
OCD is an acquired lesion of the subchondral bone. Patients with OCD initially report nonspecific pain and variable amounts of swelling. Initial radiographs help identify the lesion and establish the status of the physes. An MRI scan is useful for assessing the potential for the lesion to heal with nonsurgical treatment. Nonsurgical treatment is appropriate for small, stable lesions in patients with open physes and focuses on activity restriction for 3 to 9 months. Surgical treatment is necessary for unstable or detached lesions. Stable lesions with intact articular cartilage can be treated with subchondral drilling to stimulate vascular ingrowth, with radiographic healing at an average of 4.4 months. Fixation is indicated for unstable or hinged lesions, and stabilization of the fragment can be achieved using a variety of implants through an arthroscopic or open approach. The fragment should be salvaged and the normal articular _surface restored whenever possible._
QUESTION 60
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Based on the pathology noted, which finding may be found on plain knee radiographs? --- --- --- --- ---
1
Shallow trochlear groove
2
Squaring of the lateral femoral condyle
3
Deepening of the sulcus terminalis
4
Medial joint space narrowing
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
QUESTION 61
A 9-year-old girl, who is an avid soccer player, has intermittent spontaneous snapping in her left knee that has worsened. There is no reported trauma or prior surgeries to her knee. Despite working with her trainer, she has developed anterior-based knee pain and lacks full extension. Her knee skin is unremarkable, but there is fullness to palpation on the lateral aspect of her knee. Her range of motion demonstrates a lack of 15° of terminal extension and ligamentous examination is unremarkable. Considering possible surgical treatments for this patient, what is the most appropriate surgical treatment?
1
Arthroscopic lateral release with reconstruction of medial patellofemoral ligament
Microfracture versus stabilization of osteochondral lesion
Surgical intervention of discoid meniscus is based on symptomatic patients. Complete discoid menisci are typically stable but are expected to have >4.5 times incidence of surgical intervention. Saucerization of symptomatic discoid meniscus is associated with better results with younger patients with increases of poor outcomes in adult-aged patients. Meniscal transplant may be an option, although long-term results _are unknown._
QUESTION 62
Figure 1 is the radiograph of a 50-year old woman with lateral-sided left knee pain. She noticed the pain over the last few months and has had no new injury. She had a microfracture performed of her lateral femoral condyle 5 years ago. What is the likely cause of the finding noted on her radiograph? ---
1
Uncontained cartilage lesion
2
Removal of the subchondral plate
3
Removal of the calcified cartilage layer
4
Failure to remove the calcified cartilage layer
The radiograph reveals bony overgrowth of the microfracture site on the lateral femoral condyle. This occurs from violation of the subchondral plate during aggressive removal of the calcified cartilage layer during the microfracture. It is important during a microfracture to attempt to have a contained lesion and remove the calcified cartilage layer down to the subchondral plate, but avoid aggressively penetrating the _plate._
QUESTION 63
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. Treatment should include --- --- --- --- ---
1
anterior cruciate ligament reconstruction with lateral meniscus repair.
2
partial lateral meniscectomy with saucerization.
3
lateral meniscus transplant.
4
protected weight bearing with referral for genetic testing.
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
QUESTION 64
Figures 1 through 4 are selected sagittal MR images of an otherwise healthy 20-year-old collegiate football running back who was tackled during a game and has immediate onset of right knee pain. Video analysis of the injury shows that his flexed knee impacted the field. He is not able to return to play. On examination in the training room the following morning, he has a moderate effusion, no patellar instability, minimal joint line tenderness, and is stable to varus and valgus stress at 30° of knee flexion. A dial test is also negative. He has increased laxity in the anterior to posterior direction. What is the most appropriate next step in treatment? ---
1
Rehabilitation initially focused on closed chain quadriceps strengthening
2
Rehabilitation initially focused on hamstring strengthening
3
Anterior cruciate ligament (ACL) reconstruction using autograft tissue
4
Posterior cruciate ligament (PCL) reconstruction using autograft tissue
This athlete sustained an isolated PCL injury. The mechanism of injury is typical for a PCL injury. When a PCL injury is identified, one must rule out other ligamentous injuries to the knee. The patient has a stable examination to varus and valgus and a negative dial test, so the lateral collateral, medial collateral, and posterolateral corner (respectively) are intact. It is common to have increased anterior to posterior translation in isolated PCL injuries, even with an intact ACL, as the tibia will rest posterior to the medial femoral condyle. Treatment of isolated PCL injuries is typically nonoperative, with an initial focus on quadriceps strengthening. Hamstring strengthening and rehabilitation is added at a later time, as this places increased stress on the healing PCL. The images reveal an isolated PCL injury with intact menisci and ACL, ruling out ACL reconstruction using autograft tissue and PCL reconstruction using autograft tissue.
QUESTION 65
During anatomic medial patellofemoral ligament (MPFL) reconstruction, the surgeon notes that the graft
is becoming too tight with greater knee flexion. What is the most likely cause?
1
Femoral attachment placed too distal
2
Femoral attachment placed too proximal
3
Patellar attachment placed too distal
4
Patellar attachment placed too proximal
If the graft becomes tighter with knee flexion, the femoral attachment is too proximal. This error is referred to as “high and tight,” meaning that a high or proximal femoral attachment produces a graft that is too tight with knee flexion. If graft tension increases with increasing knee flexion, the result is loss of knee flexion or graft failure, increased contact forces resulting in patella femoral chondrosis, and possibly medial subluxation.
QUESTION 66
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that
has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is provided with a medial unloader brace that provides substantial pain relief, and he is able to work while wearing the brace. After 4 months, he returns to work and reports that while the brace enables him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace, and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
1
Valgus-producing high tibial osteotomy (VPHTO)
2
Repeat knee arthroscopy
3
Total knee arthroplasty (TKA)
4
Medial meniscus transplant
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO but does not influence technique.
QUESTION 67
Figures 1 and 2 are the T2-weighted MR images of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. Which treatment option is most likely to be associated with a favorable outcome? --- ---
1
Physical therapy
2
Meniscal repair
3
Menisectomy
4
Reconstruction
MR images reveal a posterior horn root tear of the medial meniscus. LaPrade and associates found that outcomes after posterior meniscal root repair significantly improved postoperatively and patient satisfaction was high, regardless of age or meniscal laterality. Patients aged <50 years had outcomes similar to those of patients ≥50 years, as did patients who underwent medial versus lateral root repair. In patients undergoing pullout fixation for posterior medial meniscus root tear, Chung and associates (in “Pullout Fixation of Posterior Medial Meniscus Root Tears”) found that patients with decreased meniscus extrusion at postoperative 1 year have more favorable clinical scores and radiographic findings at midterm follow-up than those with increased extrusion at 1 year. Krych and associates found that nonoperative treatment of medial meniscus posterior horn root tears is associated with poor clinical outcome, worsening arthritis, and a relatively high rate of arthroplasty at 5-year follow-up. Reconstruction would have no role _in the setting of a reparable meniscal root tear._
QUESTION 68
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"? ---
1
In extension with internal rotation/valgus force, the medial tibial plateau is subluxated; with flexion, the medial tibial plateau reduces.
2
In extension with internal rotation/valgus force, the medial tibial plateau is reduced; with flexion, the medial tibial plateau subluxates.
3
In extension with internal rotation/valgus force, the lateral tibial plateau is reduced; with flexion, the lateral plateau subluxates.
4
In extension with internal rotation/valgus force, the lateral tibial plateau is subluxated; with flexion, the lateral plateau reduces.
This patient sustained an isolated anterior cruciate ligament (ACL) injury based upon the mechanism described and examination findings. The finding that produces the “clunk” is the pivot-shift maneuver, which is positive in a knee with an incompetent ACL. With an ACL-deficient knee in full extension and internal rotation, the lateral tibial plateau subluxates anteriorly. As the knee is flexed, the lateral tibial plateau slides posteriorly into a reduced position, causing an audible clunk. Response D correctly describes the pathomechanics that result in the audible clunk heard during the pivot-shift maneuver. Responses A and B are incorrect because they describe the medial tibial plateau, which is not part of the pathomechanics of the pivot shift. Response C is incorrect because in extension, the lateral tibial plateau _is subluxated, not reduced._
QUESTION 69
Figure 1 is the MRI scan of a patient with recurrent knee instability, which persists after a period of nonsurgical treatment. Anatomic reconstruction of the torn ligament is recommended. What radiographic finding is the most important independent predictor of recurrent instability following surgery? ---
1
Tibial tubercle to trochlear groove (TT-TG) distance
2
Patella alta
3
Tibial slope
4
Trochlear dysplasia
The MR image is consistent with an episode of patellar instability with concomitant bruising of the medial patellar facet and lateral femoral condyle. The medial patellofemoral ligament appears torn and attenuated. Kita and associates reported that severe trochlear dysplasia is the most important predictor of residual patellofemoral instability after isolated medial patellofemoral ligament reconstruction. An increased TT-TG affected outcomes of patients with type D trochlear dysplasia (Dejour classification). Wagner and associates also found that high degrees of trochlear dysplasia correlate with poor clinical outcome due to graft overload in dysplastic situations. Other studies by Nelitz and associates and Matsushita and associates have also suggested that TT-TG distance did not reliably correlate with clinical outcome. Tibial slope would not affect recurrent patellar instability.
QUESTION 70
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common
source of surgical failure?
1
Graft choice
2
Tunnel position
3
Tibial fixation
4
Femoral fixation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause for technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. Although graft choice is an important factor when planning an ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position.
QUESTION 71
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment
overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
1
Patella infera (baja)
2
Patella alta
3
Recurrence of medial joint overload
4
Nonunion of the osteotomy
After HTO, particularly in patients who have been immobilized after a closing-wedge osteotomy, patella baja is a common finding. This can precipitate anterior knee pain or patellofemoral pain syndrome. Recurrence of medial joint overload is incorrect because the patient has no medial joint complaints. Nonunion is less likely with a closing-wedge osteotomy and likely will not result in anterior knee pain.
QUESTION 72
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a
football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What is the underlying cause of the pathology noted in the figures? --- --- --- --- ---
1
Genetic mutation
2
Recurrent trauma
3
Shallow intercondylar notch
4
Congenital abnormality
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment _of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair._
QUESTION 73
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks? ---
1
Resist anterior translation during knee flexion
2
Resist posterior translation during knee flexion
3
Resist rotatory loads during knee flexion
4
Resist rotatory loads during knee extension
The structure shown is the posterolateral bundle of the anterior cruciate ligament (ACL). This bundle is optimally positioned in the knee to resist rotatory forces during terminal knee extension. "Resist anterior translation during knee flexion" best describes the anteromedial bundle. "Resist rotatory loads during knee flexion" is unlikely because the posterolateral bundle is tightest during knee extension. The posterior cruciate ligament, not the ACL, functions to resist posterior translation.
QUESTION 74
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal
1
grade 2 pivot shift.
2
positive Thessaly test.
3
positive quadriceps active test.
4
positive dial test at 30°.
---
---
DISCUSSION:
The MRI scan clearly reveals bone bruises in the mid lateral femoral condyle and posterior tibial plateau. These MRI findings are commonly associated with acute anterior cruciate ligament injuries. Therefore, the preferred answer would be a positive pivot shift examination. A positive posterior drawer and positive quad active test are associated with posterior cruciate ligament injuries. A positive dial test would be suggestive of a posterolateral instability of the knee.
QUESTION 75
A 29-year-old recreational basketball player has developed pain to the distal aspect of her patella that
occurs during warm-ups and returns toward the end of the game. She reports no history of trauma, effusions, instability, and no mechanical symptoms. On examination, she is point tender at the inferior pole of the patella, lacks patella apprehension, and has a Q-angle of 15°. She has no ligamentous laxity. Radiographs are unremarkable. What is the best next step?
1
Therapy with an emphasis on eccentric exercises
2
Steroid injection
3
Platelet-rich plasma
4
Extracorporeal shock therapy
Patellar tendinopathy is a relatively common condition in athletes for which repetitive jumping is the norm, especially volleyball and basketball athletes. The prevalence has been reported to be up to 32% in professional basketball players. Initial management is nonoperative in nature with eccentric exercises providing the most reliable clinical results. The other selections have not demonstrated consistent longterm results.
QUESTION 76
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that
has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of
flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. What imaging study is most appropriate to determine treatment options for this patient?
1
Full-length weight-bearing radiographs of both legs
2
MRI scan of the left knee
3
CT scan of the left knee
4
Ultrasonography of the left leg
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an _indication for HTO but does not influence technique._
QUESTION 77
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. Stress radiographs show a 2-mm medial physeal widening with valgus stress. What is the best initial treatment strategy for this patient?
Crutch ambulation without immobilization and weight bearing as tolerated
4
Protected weight bearing with cast immobilization
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a _cylindrical or long-leg cast._
QUESTION 78
A 53-year-old man sustains a fall while skiing. He experiences immediate pain and deformity in his lower leg just above his ski boot top. Radiographs of his left lower leg are shown in Figures 1 and
1
After discussing operative management with the patient, you choose to proceed with an intramedullary nail. Where should blocking screws be placed to prevent the characteristic deformity of this fracture? 
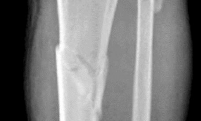  
 
2
Posterior and medial aspect of the proximal fragment
3
Anterior aspect of the proximal fragment and medial half of the distal fragment
4
Posterior and lateral aspect of the proximal fragment
5
Anterior and lateral aspect of the proximal fragment
The patient has sustained a proximal third tibia and fibula fracture, sometimes referred to as a "boot top" fracture when sustained while alpine skiing. These fractures frequently fall into apex anterior and valgus
angulation as shown in the radiographs. Great care needs to be taken during intramedullary nailing to avoid fixing the fracture in a malreduced position. The use of Poller blocking screws in the posterior and lateral aspects of the proximal fragment can help to avoid this complication (posterior screw prevents flexion deformity while lateral screw prevents valgus deformity). Additional technical pearls include starting with a more lateral entry point for the guidewire, placing a provisional unicortical plate prior to nailing to maintain the reduction, or using a suprapatellar entry nail to allow for fixation with the knee in _a semi-extended position._
QUESTION 79
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. If the patient chooses surgical reconstruction, he should be advised that, when compared with a transtibial technique, the tibial inlay technique has been shown to provide ---
1
stronger initial graft fixation.
2
more anatomic positioning of tibial fixation.
3
more natural knee kinematics during deep flexion.
4
more graft protection during cyclic loading.
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be
appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
QUESTION 80
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Left untreated, injury to this structure most likely will lead to degenerative changes in ---
1
medial and lateral compartments.
2
medial and patellofemoral compartments.
3
lateral and patellofemoral compartments.
4
the patellofemoral compartment only.
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal
Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for _vascular injury._
QUESTION 81
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings.Figures 3 and 4 are this patient's proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include --- ---
1
hinged knee bracing, protected weight bearing, and physical therapy.
2
anteromedialization of the tibial tubercle.
3
internal fixation and medial patellofemoral ligament (MPFL) reconstruction.
4
arthroscopic lateral retinacular release.
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair.
Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence _and the need for reconstruction._
QUESTION 82
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. This patient elects nonsurgical treatment and later experiences persistent instability. Examination reveals an asymmetric Dial test finding and a varus thrust during ambulation. Which osteotomy and correction appropriately addresses this chronic instability pattern? ---
1
Distal femoral/opening lateral wedge osteotomy
2
Distal femoral/closing lateral wedge osteotomy
3
High tibial osteotomy; opening medial wedge with increased tibial slope
4
High tibial osteotomy; closing lateral wedge with decreased tibial slope
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, one major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading. The scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag. Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used.
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
QUESTION 83
Augmentation of a Broström repair with the mobilized lateral portion of the extensor retinaculum (Gould
modification) is expected to produce
1
higher risk for iatrogenic nerve injury.
2
decreased ankle range of motion 6 weeks after surgery.
3
no significant biomechanical difference in initial ankle stability.
4
a significantly lower incidence of osteoarthritis on long-term follow-up.
Multiple biomechanical studies have investigated the contribution of the Gould modification with the Broström anatomic repair for chronic ankle instability. No studies to date have demonstrated a statistically significant difference in initial ankle stability with inclusion of the Gould modification or augmentation of the repair with a mobilized lateral portion of the extensor retinaculum. No clear association exists between the Broström-Gould repair technique and risk for nerve injury, postsurgical range of motion, or incidence of osteoarthritis on long-term follow-up.
QUESTION 84
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What is the most appropriate course of action for this patient’s condition?
1
Early mobilization and a guided proprioceptive and strengthening
2
Extended immobilization in a cast
3
Surgical intervention
4
Weight bearing as tolerated in an ankle brace for 6 weeks
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The
diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
QUESTION 85
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
1
Thompson test
2
External rotation stress test
3
Anterior drawer test
4
Squeeze test
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
QUESTION 86
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient
is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
1
Deltoid ligament
2
Calcaneofibular ligament
3
Anterior tibiofibular ligament
4
Posterior tibiofibular ligament
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization _and a guided rehabilitation program that emphasizes proprioceptive stability._
QUESTION 87
A 19-year old Division 1 offensive lineman sustains an ankle injury during a game. He has pain with weight-bearing and is unable to return to the game. Figures 1 through 5 are his radiographs taken the next day. What is the best next step? --- --- --- --- ---
1
Immobilization
2
Syndesmotic fixation
3
Physical therapy
4
Obtain an MRI scan
The radiographs reveal medial clear space widening and an oblique proximal fibula fracture (best seen on the lateral view overlapping the tibia). This is consistent with an unstable syndesmotic injury. Operative repair of the syndesmosis with reduction and fixation is warranted. Immobilization is the best option for a stable syndesmotic injury. Physical therapy and MRI are not warranted given the findings on the _radiographs._
QUESTION 88
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
1
Repeat radiographs
2
Full clearance to return to play
3
Bone scan
4
MRI scan
Ice hockey injuries demand a thorough assessment because they have the potential to be significant. In hockey players, bone injuries in the foot and ankle can be missed or improperly diagnosed through routine radiographic imaging. MRI can display bone injuries that are not found radiographically; this is because _some fractures and contusions involve the medial ankle and midfoot bones._
QUESTION 89
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness
but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
1
Return to full soccer activity
2
Start light aerobic activity
3
Obtain baseline neuropsychological testing
4
MRI scan of the brain
Mild traumatic brain injury is common in the adolescent child. Neuropsychological examination is widely used but, in this case, the patient is asymptomatic and has no baseline testing. There is a limited role for MRI in the recovery process of concussions. Furthermore, higher levels of physical/cognitive activity should be avoided due to their potential to increase total recovery time. In this scenario, a graduated return to activity is most appropriate thus, the next appropriate step is to start light aerobic activity.
QUESTION 90
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1
onset most often by age 30.
2
a temporary state of neuronal and axonal derangement.
3
manifestations of affect such as apathy, irritability, and suicidal ideation.
4
absence of gross pathological brain changes upon autopsy.
CTE is a neurodegenerative disease that occurs years or decades after recovery from acute or postacute effects of head trauma. The exact relationship between concussion and CTE is not entirely clear; however, early behavioral manifestations of CTE have been described by family and providers to include apathy, irritability, and suicidal ideation. For some patients, cognitive difficulty such as poor episodic memory and executive function may be the first signs of CTE. Onset most often occurs in midlife after athletes have completed their sports careers, with mean age of onset at 42 years. The effects on the brain are degenerative, leading to a permanent state of derangement. Autopsy findings demonstrate multiple gross pathological findings. The condition is more common among contact athletes.
QUESTION 91
A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and loses
consciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain; numbness; or weakness, and she is moving all extremities without deficit. The athlete and coach want to go back to competition that day. How should they be advised?
1
Concussion precludes same-day return to play.
2
Order an urgent MRI scan; if findings are normal, she can return to competition.
3
Order neurocognitive testing; if findings are normal, she can return to competition.
4
If she is symptom-free after a 15-minute exertional test, she may return to competition.
The National Collegiate Athletic Association's (NCAA) 2011 revised health and safety guidelines regarding concussion management recommend no return to play on the same day of an injury. In particular, athletes sustaining a concussion should not return to play the same day as their injury. Before resuming exercise, athletes must be asymptomatic or returned to baseline symptoms at rest and have no
symptoms with cognitive effort. They must be off of medications that could mask or alter concussion symptoms. Neurocognitive testing can be a helpful tool in determining brain function even after all symptoms of concussion have resolved. With a comparison baseline test, this evaluation, in conjunction with a physician's examination, may reduce risk for second impact syndrome. The athlete's clinical neurologic examination findings (cognitive, cranial nerve, balance testing) must return to baseline before resuming exercise. Research has shown that among youth athletes, it may take longer for tested functions to return to baseline (compared with the recovery rate in adult athletes). Brain MRI scan has no role in evaluating athletes for return to play in this situation.
QUESTION 92
A collegiate lacrosse player is struck on the head by an opposing player’s stick. She is initially
unresponsive. She regains consciousness within 2 minutes but remains confused and uncooperative, complaining of head and neck pain. This is her second concussion of the calendar year. Initial management should consist of
1
calculation of Glasgow Coma Scale score.
2
evaluation with a sideline assessment tool, such as the SCAT-3.
3
urgent hospital transfer for CT scan.
4
stabilization of the cervical spine and placement of a collar
This patient has sustained a significant concussion or minor brain injury. Although all answer options reflect important steps in her management, the initial primary concern in any player who is confused or combative is protection of the cervical spine until formal clearance can be performed. This patient requires immediate immobilization, collar placement, and, ultimately, transportation to a hospital. Cervical immobilization should be achieved before transport, given her complaints of neck pain and inability to provide a reliable examination.
QUESTION 93
A 17-year-old high school football player sustains a neck injury in a game. During the initial on-field
assessment, the team physician removes the player’s helmet, and the athlete is log-rolled to the supine position while the physician manually stabilizes his cervical spine. An examination demonstrates tenderness to palpation over the cervical spine and neurologic deficits in bilateral upper and lower extremities. Shoulder pads prohibit proper placement of a hard cervical collar, and the athlete is immobilized on a spine board and transported to the emergency department via ambulance. Comprehensive evaluation in the emergency department reveals a bilateral facet dislocation of C5 on C6. The on-field intervention most likely to cause a neurologic injury is
1
failure to place a hard cervical collar.
2
helmet removal prior to examination.
3
transfer to a spine board prior to transport.
4
log-rolling the athlete to the supine position.
Complete immobilization of the cervical spine is critical for athletes with a suspected cervical spine or spinal cord injury. The spinal cord in the subaxial spine is especially sensitive to motion, and removal of protective gear such as the helmet and shoulder pads presents an unacceptable risk for progressive neurologic injury in the setting of a potentially unstable cervical spine injury. Removal of the face mask alone is typically performed to improve access to an athlete's airway. Protective equipment often prevents
proper placement of a hard cervical collar, and the spine board offers a variety of options for safe cervical spine immobilization of helmeted athletes without a hard cervical collar. The log-roll and lift-and-slide techniques allow for the safe transfer of an athlete to a spine board while maintaining appropriate manual stabilization of the cervical spine.
QUESTION 94
A coach of three football teams—the B team, junior varsity team, and varsity team—wants to study the
average times in the 40-yard dash for his players. Which test would help him determine if the mean 40-yard dash times for the athletes on one team are different from those on the other teams?
1
Independent 2-sample _t_ test
2
Analysis of variance (ANOVA)
3
Chi-square test
4
Fisher's exact test
Data collected in research studies fall into one of two categories—continuous or discrete. Continuous data can be displayed on a curve. Examples include height, weight, and time recorded in a 40-yard dash. Discrete data represent data that fall into specific categories such as gender or the presence or absence of a risk factor. ANOVA is used to determine statistical significance in mean values of continuous data when there are more than two independent samples. The 2-sample _t_ test compares mean values of continuous data between two independent groups. The Chi-square test and Fisher's exact tests are tests used to analyze discrete data.
QUESTION 95
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history
of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment? --- --- --- --- --- ---
The images illustrate a large unstable osteochondral lesion of the medial femoral condyle. Radiographs and MR images clearly show deep subchondral bone involvement. The appropriate choice of surgery is OCA transplantation, which is indicated for primary treatment of large cartilage lesions, osteochondral lesions, and salvage procedure from failed prior cartilage surgery. Correction of mechanical axis malalignment, ligamentous insufficiency, and meniscal deficiency should also be addressed. ACI alone or an arthroscopic microfracture procedure would not address the bone defect, leaving an uneven articular surface. Although an osteotomy may be a viable choice, a distal femoral varus osteotomy would increase the contact pressure in the medial compartment and worsen the situation. The histologic anatomy of articular cartilage is well described. The superficial layer or lamina splendens contains a small amount of proteoglycan with collagen fibrils arranged parallel to the articular surface. In contrast, the deep zone contains the largest-diameter collagen fibrils, oriented perpendicular to the joint surface, and the highest _concentration of proteoglycans._
QUESTION 96
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve? ---
1
Long thoracic nerve
2
Cranial nerve XI (spinal accessory nerve)
3
Suprascapular nerve
4
Axillary nerve
Figure 1 reveals medial scapular winging secondary to weakness of the serratus anterior, which is innervated by the long thoracic nerve. Damage to the long thoracic nerve can occur via repetitive stretching, compression, or iatrogenic injury during a surgical procedure. Lateral thoracic winging is caused by weakness of the trapezius, which is innervated by cranial nerve XI (spinal accessory nerve). The direction of scapular winging is judged by the upper medial border of the scapula. Observation of a period of at least 6 months with serratus anterior strengthening while the nerve recovers is the mainstay _of treatment for medial scapular winging._
QUESTION 97
A 16-year-old football player is participating in the second session of two-a-day preseason practices. He complains of dizziness and fatigue. He is brought to the sideline by the athletic trainer where examination
demonstrates confusion and disorientation. Ambient temperature is 82°F. What would be the next most appropriate step in his treatment?
1
Rapid cooling via ice bath, cold water and fans
2
Transportation via ambulance to a local emergency department
3
Rapid rehydration via oral and IV fluids
4
Immediate administration of acetaminophen or other anti-pyretics
Heat exhaustion and heat stroke reflect varying degrees of heat illness, with both marked by increased heat production with impaired heat dissipation. Heat exhaustion typically involves a core body temperature between 37°C (98.6°F) and 40°C (104°F) and usually presents with heavy sweating, as well as nausea; vomiting; headache; fainting; weakness; and cold or clammy skin. Fatigue, malaise, and dizziness may occur, but necessary to the diagnosis is normal mentation and stable neurologic status. Heat stroke is defined by a core body temperature >40°C (>104°F) and disturbances of the central nervous system, such as confusion, irritability, ataxia, and even coma. Heat exhaustion is a less urgent scenario and can usually be treated with rest, elevation, and rehydration. Heat stroke, confirmed here by the presence of mental status changes, is a more critical situation. The most important immediate step is rapid body cooling through whatever means are available, as this has been clearly shown to improve outcomes. Ideally, a whole body ice bath would be used, with ice towels, ice packs, cold water, and air fans all utilized if needed. Emergency department transportation and rehydration may be considered as well but are not as important as immediate lowering of body temperature. Anti-pyretics have no role in this process.
QUESTION 98
What is the most common complication after surgical management of chronic exertional compartment
syndrome (CECS) in the pediatric (≤18 years) population?
1
Recurrent CECS
2
Infection
3
Neurologic dysfunction
4
Hematoma or seroma formation
QUESTION 99
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%.
A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
1
Use of chest protectors
2
Time to initiation of chest compressions
3
Lower velocity of the puck at impact
4
Time to defibrillation
The hockey player is suffering from commotio cordis, in which a cardiac arrhythmia occurs after a sudden blunt impact to the chest. Treatment of commotio cordis is defibrillation. As the time to defibrillation increases, the likelihood of survival decreases. In animal models, chest protectors have not shown efficacy
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.