Orthopedic Shoulder And Review | Dr Hutaif Shoulder & E -...
Updated: Feb 2026
41 Views
Key Medical Takeaway
For anyone wondering about Orthopedic MCQS online Shoulder and Elbow 017, Shoulder arthroplasty RTSA (Reverse Total Shoulder Arthroplasty) is a surgical solution for complex shoulder conditions like irreparable rotator cuff tears or severe arthritis. Orthopedic care addresses various musculoskeletal challenges, from treating specific elbow fractures involving the anteromedial coronoid facet to managing long-term joint damage. Treatment aims to restore function and prevent debilitating progressive arthritis.
Score: 0%
Orthopedic MCQS online Shoulder and Elbow 017
QUESTION 1
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_ CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
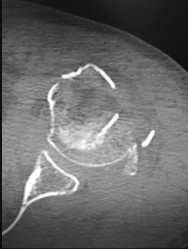
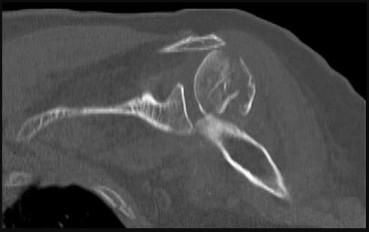
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b. **Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?
1
Lateral ulnar collateral ligament
2
Radial collateral ligament
3
Posterior medial collateral ligament (MCL)
4
Anterior MCL
_
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
QUESTION 2
of 100
Figures 5a through 5d are the radiographs of a 55-year-old healthy woman who fell down a flight of steps while sleepwalking. When the surgeon replace the radial head, the elbow dislocates posteriorly at 60 degrees of flexion as it is brought out from full flexion. What is the best next step?
1
Only repair the lateral collateral ligament (LCL)
2
Do nothing further and place the elbow in 90 degrees of flexion
3
Repair the posterior band of the medial collateral ligament (MCL)
4
Repair the coronoid and reassess for stability
The coronoid is important for elbow stability because it moves into extension. Repairing the LCL alone after radial head replacement in “terrible triad” injuries may suffice if there is a type 1 coronoid fracture or an anterior capsular avulsion. For more extensive coronoid injuries, live dynamic examination of stability is needed to determine whether repair of the coronoid is needed. For this patient, doing nothing further will lead to immediate postsurgical instability, and repairing the LCL complex alone will not lead to stability. The posterior band of the MCL will not add to stability. The next step to attain stability is to repair the coronoid and reexamine the elbow for stability.
RECOMMENDED READINGS
3. [Papatheodorou LK, Rubright JH, Heim KA, Weiser RW, Sotereanos DG. Terrible triad injuries of the elbow: does the coronoid always need to be fixed? Clin Orthop Relat Res. 2014 Jul;472(7):2084-91. doi: 10.1007/s11999-014-3471-7. PubMed PMID: 24474322](http://www.ncbi.nlm.nih.gov/pubmed/24474322)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24474322)
4. Reichel LM, Milam GS, Hillin CD, Reitman CA. Osteology of the coronoid process with clinical correlation to coronoid fractures in terrible triad injuries. J Shoulder Elbow Surg. 2013 Mar;22(3):323-
[8/. doi: 10.1016/j.jse.2012.10.038. Epub 2013 Jan 16. ](http://www.ncbi.nlm.nih.gov/pubmed/23333172)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23333172)
5. [Dodds SD, Fishler T. Terrible triad of the elbow. Orthop Clin North Am. 2013 Jan;44(1):47-58. doi: 10.1016/j.ocl.2012.08.006. PubMed PMID: 23174325.](http://www.ncbi.nlm.nih.gov/pubmed/23174325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23174325)
QUESTION 3
of 100
A 70-year-old man has a 1-year history of progressive right shoulder pain, motion loss, and weakness associated with rotator cuff arthropathy. He has failed nonsurgical treatment. During the informed consent process, the patient is counseled regarding his treatment options, and the surgeon recommends that he undergo a right reverse total shoulder arthroplasty (rTSA). The patient must be informed about the complications associated with this type of procedure, the most common of which is
1
infection.
2
prosthetic joint instability.
3
neurologic injury.
4
scapular notching.
rTSA originally was used to address rotator cuff arthropathy. Current indications have expanded to include massive rotator cuff tears without arthritis, failed shoulder arthroplasty, 3- and 4-part proximal humerus fractures, and glenohumeral arthrosis associated with severe/uncorrectable glenoid retroversion. rTSA volume has increased, leading to identification of problems specific to the procedure. Some of the common complications include neurologic injury, periprosthetic fracture, hematoma, infection, scapular notching, prosthetic joint instability, baseplate failure, and acromial fracture. A meta-analysis performed by Bohsali and associates involving rTSA
demonstrated these complications in decreasing order of frequency: scapular notching, hematoma formation, glenoid dissociation such as baseplate failure or aseptic loosening, glenohumeral dislocation, acromial and/or scapular spine fracture, infection, loosening or dissociation of the humeral component, and nerve injury.
RECOMMENDED READINGS
6. [Cheung E, Willis M, Walker M, Clark R, Frankle MA. Complications in reverse total shoulder arthroplasty. J Am Acad Orthop Surg. 2011 Jul;19(7):439-49. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/21724923)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21724923)
7. [Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. ](http://www.ncbi.nlm.nih.gov/pubmed/17015609)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17015609)
QUESTION 4
of 100
A 24-year-old right-hand-dominant professional baseball pitcher has valgus extension overload (VEO) syndrome of the right elbow, as seen in Figure 7. Which letter in the figure corresponds to the typical area of osteophyte formation in this condition?
1
A
2
B
3
C
4
D
VEO most commonly is seen in throwers for whom valgus stress across the elbow causes impingement of the posteromedial olecranon tip against the medial wall of the olecranon fossa. With repeated impingement, a bony osteophyte may grow on the olecranon at the site of impingement in this posteromedial region of the olecranon. Bony growth within the olecranon
fossa also has been seen. The distinction between this condition and ulnar collateral ligament injury is difficult to make, but VEO often can be distinguished from UCL injury by determining the exact location of pain a patient experiences. With VEO, the pain typically occurs with direct palpation of the posterior medial tip of the olecranon. The valgus extension overload provocative test also aids in diagnosis. A supervised physical therapy program and arthroscopic surgical decompression when nonsurgical treatment is unsuccessful are typical treatments for this condition.
Locations C and D represent the origin and insertion, respectively, of the elbow medial collateral ligament (MCL) structure, and, although associated MCL pathology can exist in the setting of VEO syndrome, osteophyte formation is not typical in these areas. Location A is the radial head, and although the radiocapitellar joint is a known secondary stabilizer of elbow valgus stress, osteophyte formation in this area is less likely in this clinical scenario.
RECOMMENDED READINGS
8. [Reddy AS, Kvitne RS, Yocum LA, Elattrache NS, Glousman RE, Jobe FW. Arthroscopy of the elbow: a long-term clinical review. Arthroscopy. 2000 Sep;16(6):588-94. ](http://www.ncbi.nlm.nih.gov/pubmed/10976118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976118)
9. [Andrews JR, Craven WM. Lesions of the posterior compartment of the elbow. Clin Sports Med. 1991 Jul;10(3):637-52. Review. PubMed PMID: 1868565.](http://www.ncbi.nlm.nih.gov/pubmed/1868565)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1868565)
10. [Wilson FD, Andrews JR, Blackburn TA, McCluskey G. Valgus extension overload in the pitching elbow. Am J Sports Med. 1983 Mar-Apr;11(2):83-8. ](http://www.ncbi.nlm.nih.gov/pubmed/6846685)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/6846685)
QUESTION 5
of 100
In rotator cuff tear arthropathy with pseudoparalysis, forward elevation of the humerus away from the body is prohibited because of
1
deltoid atony.
2
loss of the glenoid concavity.
3
loss of the humeral head depression of the biceps tendon.
4
loss of compressive force on the humeral head.
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with this condition, so no atony is present. Glenoid concavity can be lost over time, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
RECOMMENDED READINGS
11. [Drake GN, O'Connor DP, Edwards TB. Indications for reverse total shoulder arthroplasty in rotator cuff disease. Clin Orthop Relat Res. 2010 Jun;468(6):1526-33. doi: 10.1007/s11999-009-1188-9. Review. PubMed PMID: 20049573.](http://www.ncbi.nlm.nih.gov/pubmed/20049573)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20049573)
12. [Walker M, Brooks J, Willis M, Frankle M. How reverse shoulder arthroplasty works. Clin Orthop Relat Res. 2011 Sep;469(9):2440-51. doi: 10.1007/s11999-011-1892-0. Review.](http://www.ncbi.nlm.nih.gov/pubmed/21484471)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21484471)
CLINICAL SITUATION FOR QUESTIONS 9 AND 10
A 19-year-old, right-hand-dominant collegiate baseball pitcher reports a 4-month history of right shoulder pain after a throwing activity. He localizes the pain primarily to the posterior aspect of his shoulder and describes the type of pain as an aching sensation. He has been involved with strength and conditioning with his team, but denies any specific therapy other than the application of ice after throwing and use of occasional over-the-counter anti-inflammatory drugs, neither of which has provided relief. He denies any specific traumatic event or previous history of shoulder problems. His pitching coach has noted a slight decrease in his throwing velocity during the last 2 months.
QUESTION 6
of 100
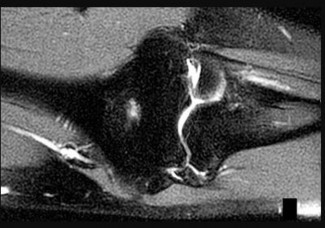
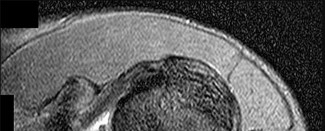
The patient fails nonsurgical treatment and undergoes shoulder arthroscopy. At the time of surgery, the area marked by the asterisk in Figure 9 is visualized from the posterolateral portal. This anatomic structure impinges on which other structure during late cocking of the throwing phase?
1
Biceps tendon
2
Posterior band of the inferior glenohumeral ligament
3
Hill-Sachs lesion
4
Undersurface of the supraspinatus and infraspinatus tendons
- Undersurface of the supraspinatus and infraspinatus tendons_
QUESTION 7
of 100
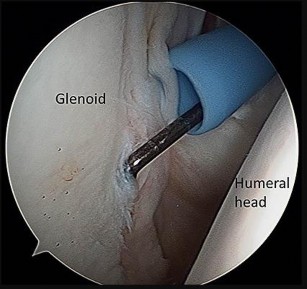
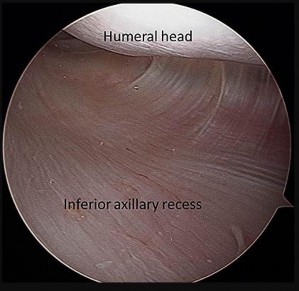
Which image seen during arthroscopic treatment is most likely associated with this patient’s condition?
A b c d
1
Figure 10a
2
Figure 10b
3
Figure 10c
4
Figure 10d
This patient’s clinical presentation is consistent with internal impingement accompanied by glenohumeral internal rotation deficit (GIRD). Although throwers may have increased external rotation, their overall arc of motion should be the same as on the nonthrowing side. In comparison, patients with GIRD experience a marked decrease in arc of motion, particularly in internal rotation.
Internal impingement represents a spectrum of findings that can include superior and posterior labral tears, undersurface (articular-sided) tearing of the posterior supraspinatus, posterior glenoid wear, and scar formation of the posterior capsule. Myers and associates demonstrated internal impingement is associated with GIRD, although the latter by itself may be asymptomatic and perhaps a sports-specific adaptation. However, posterior capsular tightness can lead to posterosuperior translation of the humerus during throwing, leading to these injuries. Internal impingement is common among overhead throwing athletes and occurs during the late cocking and early acceleration phases of throwing. Humeral migration during the abducted/externally rotated throwing position results in abutment of the greater tuberosity against the posterosuperior glenoid labrum, which impinges the rotator cuff (Paley and associates).
Pain is often posterior, but symptoms can be vague. Patients may have examination findings consistent with rotator cuff weakness and superior labrum anterior to posterior (SLAP)/biceps involvement. Radiograph findings can be negative, although a Bennett lesion involving hypertrophy and mineralization of the posterior capsular injury may be seen (Wright and Paletta). A CT scan may show glenoid retroversion (Crockett and associates), while MR imaging should be reviewed for a possible partial articular-sided rotator cuff tear, SLAP tear, or increased signal in the posterosuperior labrum or greater tuberosity.
Treatment of this condition should be the focus on therapy, and most cases can be treated nonsurgically. Stretching aimed at the posterior capsule (ie, sleeper stretch) has been reported as effective (Tyler and associates, Litner and associates). Burkhart and associates also demonstrated posterior capsular stretching can help prevent throwing injuries. Because cuff pathology may be present, physical therapy also should include rotator strengthening, scapular stabilization, and addressing of issues related to throwing mechanics (Drakos and associates). Kibler and associates published a comprehensive rehabilitation guideline. Surgical intervention is reserved for those who fail 6 months of nonsurgical treatment and is directed by intra-articular pathology (debridement vs repair of the rotator cuff and labrum) (Braun and associates).
RECOMMENDED READINGS
13. [Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20. Review. PubMed PMID: 12671624. ](http://www.ncbi.nlm.nih.gov/pubmed/12671624)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12671624)
14. [Braun S, Kokmeyer D, Millett PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009 Apr;91(4):966-78. doi: 10.2106/JBJS.H.01341. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/19339585)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19339585)
15. [Crockett HC, Gross LB, Wilk KE, Schwartz ML, Reed J, O'Mara J, Reilly MT, Dugas JR, Meister K, Lyman S, Andrews JR. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002 Jan-Feb;30(1):20-6. ](http://www.ncbi.nlm.nih.gov/pubmed/11798991)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11798991)
16. [Drakos MC, Rudzki JR, Allen AA, Potter HG, Altchek DW. Internal impingement of the shoulder in the overhead athlete. J Bone Joint Surg Am. 2009 Nov;91(11):2719-28. doi: 10.2106/JBJS.I.00409. Review. PubMed PMID: 19884449.](http://www.ncbi.nlm.nih.gov/pubmed/19884449)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884449)
17. [Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/11888148)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11888148)
18. [Lintner D, Mayol M, Uzodinma O, Jones R, Labossiere D. Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med. 2007 Apr;35(4):617-21. Epub 2007 Feb 9. PubMed PMID: 17293473. ](http://www.ncbi.nlm.nih.gov/pubmed/17293473)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17293473)
19. [Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006 Mar;34(3):385-91. Epub 2005 Nov 22. PubMed PMID: 16303877. ](http://www.ncbi.nlm.nih.gov/pubmed/16303877)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16303877)
20. [Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS. Arthroscopic findings in the overhand throwing athlete: evidence for posterior internal impingement of the rotator cuff. Arthroscopy. 2000 Jan-Feb;16(1):35-40. PubMed PMID: 10627343. ](http://www.ncbi.nlm.nih.gov/pubmed/10627343)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627343)
21. [Tyler TF, Nicholas SJ, Lee SJ, Mullaney M, McHugh MP. Correction of posterior shoulder tightness is associated with symptom resolution in patients with internal impingement. Am J Sports Med. 2010 Jan;38(1):114-9. doi: 10.1177/0363546509346050. Epub 2009 Dec 4. ](http://www.ncbi.nlm.nih.gov/pubmed/19966099)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19966099)
22. [Wright RW, Paletta GA Jr. Prevalence of the Bennett lesion of the shoulder in major league pitchers. Am J Sports Med. 2004 Jan-Feb;32(1):121-4. PubMed PMID: 14754734. ](http://www.ncbi.nlm.nih.gov/pubmed/14754734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14754734)
QUESTION 8
of 100
Which organism is most likely responsible for a periprosthetic shoulder infection?
1
A gram-positive aerotolerant anaerobic _Bacillus_
2
A gram-negative anaerobic _Bacillus_
3
Aerobic gram-positive _cocci_ in clusters
4
Aerobic gram-positive _cocci_ in pairs
_Propionibacterium acnes (P. acnes) has emerged as the most likely cause of infection associated with shoulder arthroplasty. A gram-positive, aerotolerant anaerobic rod that lives in the skin, not on the skin, it is more difficult to diagnose and treat than more conventional organisms. As an anaerobe, it does not create pus, but rather a turbid fluid, and is associated with humeral stem loosening when a clinically significant infection is present. P. acnes remains sensitive to most antibiotics, and, although some resistance to clindamycin has been reported, highly resistant strains have not yet evolved._
_P. acnes often remains a diagnostic challenge. Conventional tests measuring C-reactive protein, sedimentation rate, Interleukin-6, and white cell counts are not highly accurate. Even aspiration and culture of the affected joint is not reliable. Cultures should be kept at least 2 weeks to avoid false-negative results with slow-growing organisms. Some investigators have advocated diagnostic arthroscopy with biopsy as another diagnostic alternative._
Treatment of shoulder replacements infected with _P. acnes_ is evolving. For shoulders associated with low clinical suspicion for infection but an unexpected positive culture result, treatment can be 1-stage reconstruction without an extended course of intravenous antibiotics. Most commonly, an infected shoulder arthroplasty is treated with a 2-stage reconstruction similar to that seen in the setting of hip and knee arthroplasty.
RECOMMENDED READINGS
23. Kelly JD 2nd, Hobgood ER. Positive culture rate in revision shoulder arthroplasty. Clin Orthop Relat Res. 2009 Sep;467(9):2343-8. doi: 10.1007/s11999-009-0875-x. Epub 2009 May 12. PubMed PMID:
[19434469/. ](http://www.ncbi.nlm.nih.gov/pubmed/19434469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19434469)
24. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
25. Grosso MJ, Sabesan VJ, Ho JC, Ricchetti ET, Iannotti JP. Reinfection rates after 1-stage revision shoulder arthroplasty for patients with unexpected positive intraoperative cultures. J Shoulder Elbow Surg. 2012 Jun;21(6):754-8. doi: 10.1016/j.jse.2011.08.052. Epub 2012 Feb 3. PubMed PMID:
[22305921/. ](http://www.ncbi.nlm.nih.gov/pubmed/22305921)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22305921)
26. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861.](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
QUESTION 9
of 100
For humeral shaft fractures, the characteristic most associated with radial nerve palsy is
1
open fracture.
2
distal one-third humeral shaft fracture.
3
proximal one-third humeral shaft fracture.
4
closed, comminuted humeral shaft fracture.
Open fractures are not associated with a higher incidence of radial nerve palsy than closed fractures. Comminution has not been associated with an increase in radial nerve palsy. Transverse and spiral fractures are associated with a higher incidence of radial nerve palsy than comminuted fractures. Proximal humerus fractures have an incidence of only 1.8%. Distal one-third humeral shaft fractures are associated with the highest incidence of radial nerve palsy at 23.6%.
RECOMMENDED READINGS
27. [Shao YC, Harwood P, Grotz MR, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus: a systematic review. J Bone Joint Surg Br. 2005 Dec;87(12):1647-52. Review. PubMed PMID: 16326879. ](http://www.ncbi.nlm.nih.gov/pubmed/16326879)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16326879)
28. [Ring D, Chin K, Jupiter JB. Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am. 2004 Jan;29(1):144-7. PubMed PMID: 14751118. ](http://www.ncbi.nlm.nih.gov/pubmed/14751118)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14751118)
RESPONSES FOR QUESTIONS 13 THROUGH 17
1. Isolated posterior instability with a posterior labral tear
2. Multidirectional instability
3. Anterior shoulder subluxation
4. Thoracic outlet syndrome
5. Superior labrum anterior to posterior (SLAP) tear
6. Proximal humeral physeal injury
For each clinical scenario described below, please select the most likely diagnosis listed above.
QUESTION 10
of 100
An 18-year-old female collegiate swimmer has a 1-year history of posterior shoulder pain and popping and a bilateral 2-cm sulcus sign.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Multidirectional instability_
QUESTION 11
of 100
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Anterior shoulder subluxation_
QUESTION 12
of 100
A 21-year-old collegiate baseball player experiences posterior shoulder pain in the lead shoulder while batting.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Isolated posterior instability with a posterior labral tear_
QUESTION 13
of 100
A 23-year-old professional baseball pitcher experiences worsening pain in the throwing shoulder. Examination reveals increased external rotation, decreased internal rotation, and loss of total arc of motion in the throwing arm compared to the opposite side.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Superior labrum anterior to posterior (SLAP) tear_
QUESTION 14
of 100
A 14-year-old Little League pitcher who plays in 2 leagues concurrently has pain in his throwing shoulder while pitching but not at rest.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
Multidirectional shoulder instability can be diagnosed by demonstrating instability in at least 2 planes. The sulcus sign is often present with a prominent depression below the acromion when traction is applied to the arm. The mechanism of anterior shoulder dislocation or subluxation is most commonly a combination of abduction, external rotation, and a posteriorly directed force applied to the arm. Among baseball players, the lead shoulder is susceptible to posterior capsulolabral lesions termed “batter’s shoulder.” SLAP tears are common among overhead
athletes and can cause symptoms similar to impingement as well as a glenohumeral internal rotation deficit, which may predispose players to labral tears. Little League shoulder is an overuse injury typically seen in baseball pitchers who are around 14 years of age. It is an osteochondrosis of the proximal humeral epiphysis attributable to overuse from throwing.
RECOMMENDED READINGS
1. [Kang RW, Mahony GT, Harris TC, Dines JS. Posterior instability caused by batter's shoulder. Clin Sports Med. 2013 Oct;32(4):797-802. doi: 10.1016/j.csm.2013.07.012. Epub 2013 Aug 22. Review. PubMed PMID: 24079435. ](http://www.ncbi.nlm.nih.gov/pubmed/24079435)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24079435)
2. [Carson WG Jr, Gasser SI. Little Leaguer's shoulder. A report of 23 cases. Am J Sports Med. 1998 Jul-Aug;26(4):575-80. PubMed PMID: 9689382. ](http://www.ncbi.nlm.nih.gov/pubmed/9689382)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9689382)
3. [Ren H, Bicknell RT. From the unstable painful shoulder to multidirectional instability in the young athlete. Clin Sports Med. 2013 Oct;32(4):815-23. doi: 10.1016/j.csm.2013.07.014. Review. PubMed PMID: 24079437. ](http://www.ncbi.nlm.nih.gov/pubmed/24079437)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24079437)
4. [Werner BC, Brockmeier SF, Miller MD. Etiology, Diagnosis, and Management of Failed SLAP Repair. J Am Acad Orthop Surg. 2014 Sep;22(9):554-565. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/25157037)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25157037)
QUESTION 15
of 100
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
1
Inflammatory elbow arthritis
2
A presurgical flexion-extension elbow arc of approximately 50 degrees
3
Retained distal humerus hardware on presurgical radiographs
4
Evidence of presurgical elbow instability
End-stage posttraumatic or inflammatory elbow arthritis in active, high-demand patients remains difficult to treat. Traditional total elbow arthroplasty is discouraged in this demographic secondary to the concerns about implant longevity. The soft-tissue interposition arthroplasty does not necessitate the same activity and weight restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in
Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51 degrees to 97 degrees after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior surgery was not deemed a contraindication.
RECOMMENDED READINGS
5. [Larson AN, Morrey BF. Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am. 2008 Dec;90(12):2714-23. doi: 10.2106/JBJS.G.00768. PubMed PMID: 19047718.](http://www.ncbi.nlm.nih.gov/pubmed/19047718)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19047718)
6. [Nolla J, Ring D, Lozano-Calderon S, Jupiter JB. Interposition arthroplasty of the elbow with hinged external fixation for post-traumatic arthritis. J Shoulder Elbow Surg. 2008 May-Jun;17(3):459-64. doi: 10.1016/j.jse.2007.11.008. Epub 2008 Mar 14. PubMed PMID: 18342545. ](http://www.ncbi.nlm.nih.gov/pubmed/18342545)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18342545)
QUESTION 16
of 100
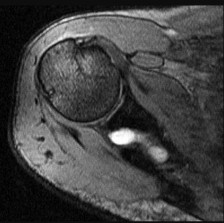
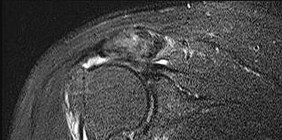
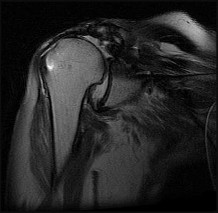
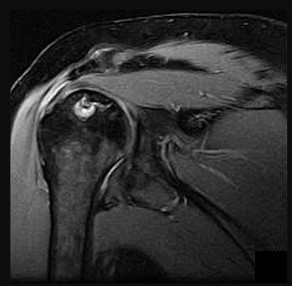
Left shoulder MR imaging results are shown in Figure 19 for a 22-year-old, right-hand-dominant collegiate athlete who reports a 6-month history of weakness in his right arm that first was noticed during weight training. He reports the weakness seems worse now than several months ago. He denies any specific traumatic event, has altered his weight-lifting activities, and has tried over-the-counter ibuprofen without experiencing any benefit. Upon examination of the bilateral upper extremities, there is no appreciable deformity or atrophy. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but there is weakness in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. He has normal sensation and pulses to the upper extremity. A standard radiographic shoulder series yields unremarkable results. What is the best surgical option?
1
Arthroscopic labral debridement and biceps tenodesis
2
Shoulder arthroscopy with undersurface cuff debridement and acromioplasty
3
Cyst decompression at the spinoglenoid notch with possible labral repair
4
Cyst decompression at the suprascapular notch with possible labral repair
This patient’s clinical and MR imaging findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
RECOMMENDED READINGS
7. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677.](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
8. [Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):600-4. PubMed PMID: 12469086.](http://www.ncbi.nlm.nih.gov/pubmed/12469086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12469086)
9. [Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL. Suprascapular neuropathy. Results of non-operative treatment. J Bone Joint Surg Am. 1997 Aug;79(8):1159-65. PubMed PMID: 9278075.](http://www.ncbi.nlm.nih.gov/pubmed/9278075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9278075)
10. [Chen AL, Ong BC, Rose DJ. Arthroscopic management of spinoglenoid cysts associated with SLAP lesions and suprascapular neuropathy. Arthroscopy. 2003 Jul-Aug;19(6):E15-21. PubMed PMID: 12861219. ](http://www.ncbi.nlm.nih.gov/pubmed/12861219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12861219)
11. [Cummins CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000 Mar;82(3):415-24. Review. PubMed PMID: 10724234.](http://www.ncbi.nlm.nih.gov/pubmed/10724234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10724234)
QUESTION 17
of 100
A 65-year-old patient undergoes revision total shoulder arthroplasty. Intraoperative culture results held for 5 days are negative. Five days after surgery, this afebrile patient experiences increasing pain, modest redness, and decreased motion. His postsurgical erythrocyte sedimentation rate is 25 mm/h (reference range, 0-20 mm/h), and his white blood cell level is normal. What is the best next step?
1
Additional imaging
2
Anti-inflammatory medications
3
Physical therapy
4
Ask microbiology to hold the intraoperative cultures for 2 weeks
_Propionibacterium acnes is increasingly recognized as a pathogen in shoulder surgery of all types and a cause of postsurgical shoulder pain. Its presentation often is characterized by pain and only minimally elevated laboratory study results and low-grade clinical findings. Cultures should be held for 2 weeks to identify this organism._
RECOMMENDED READINGS
12. Hudek R, Sommer F, Kerwat M, Abdelkawi AF, Loos F, Gohlke F. Propionibacterium acnes in shoulder surgery: true infection, contamination, or commensal of the deep tissue? J Shoulder Elbow Surg. 2014 Dec;23(12):1763-71. doi: 10.1016/j.jse.2014.05.024. Epub 2014 Aug 29. PubMed PMID:
[25179369/. ](http://www.ncbi.nlm.nih.gov/pubmed/25179369)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25179369)
13. [Matsen FA 3rd, Butler-Wu S, Carofino BC, Jette JL, Bertelsen A, Bumgarner R. Origin of propionibacterium in surgical wounds and evidence-based approach for culturing propionibacterium from surgical sites. J Bone Joint Surg Am. 2013 Dec 4;95(23):e1811-7. doi: 10.2106/JBJS.L.01733. PubMed PMID: 24306704. ](http://www.ncbi.nlm.nih.gov/pubmed/24306704)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24306704)
14. [Sethi PM, Sabetta JR, Stuek SJ, Horine SV, Vadasdi KB, Greene RT, Cunningham JG, Miller SR. Presence of Propionibacterium acnes in primary shoulder arthroscopy: results of aspiration and tissue cultures. J Shoulder Elbow Surg. 2015 May;24(5):796-803. doi: 10.1016/j.jse.2014.09.042. Epub 2014 Dec 4. PubMed PMID: 25483906. ](http://www.ncbi.nlm.nih.gov/pubmed/25483906)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25483906)
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the radiographs of a 45-year-old man following acute trauma.
QUESTION 18
of 100
Which radiographic finding indicates likely radial head replacement?
1
2 or fewer fragments of the radial head
2
Age younger than 21 years
3
Wrist pain and asymmetry of the ipsilateral distal radioulnar joint
4
Anteromedial coronoid comminution
- Wrist pain and asymmetry of the ipsilateral distal radioulnar joint_
QUESTION 19
of 100
Following radial head replacement, the elbow exhibits persistent laxity to valgus stress in extension. What is the best next step to regain stability?
1
Posterior capsular repair
2
Anterior capsular repair
3
Fixation of the type I coronoid fracture
4
Repair of the medial collateral ligament (MCL)
Longitudinal forearm instability is an indication for radial head replacement to prevent proximal migration of the radial shaft. Radial head replacement is indicated in radial head fractures involving 3 or more fragments. Younger age is not a contraindication or indication for radial head replacement. Anteromedial coronoid facet fractures usually are associated with a posteromedial rotatory mechanism that does not increase or decrease risk for radial head fractures necessitating replacement.
Following restoration of the radial head, a lateral collateral ligament repair would be the next step to restore stability if necessary. MCL repair would restore medial stability if stability persisted following restoration of posterolateral laxity. Repair of type I coronoid fractures does not substantially affect stability. Application of a hinged external fixator can restore stability in severe cases but is usually reserved for refractory instability after ligament repair has been performed and instability persists.
Anterior and posterior capsular repair do not significantly affect instability. MCL repair is generally the next step to obtain stability, with application of a hinged external fixator as a last step to maintain joint congruity.
RECOMMENDED READINGS
15. [Morrey BF, Tanaka S, An KN. Valgus stability of the elbow. A definition of primary and secondary constraints. Clin Orthop Relat Res. 1991 Apr;(265):187-95. ](http://www.ncbi.nlm.nih.gov/pubmed/2009657)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2009657)
16. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222. PubMed PMID:
[19487524/. ](http://www.ncbi.nlm.nih.gov/pubmed/19487524)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487524)
17. [Beingessner DM, Stacpoole RA, Dunning CE, Johnson JA, King GJ. The effect of suture fixation of type I coronoid fractures on the kinematics and stability of the elbow with and without medial collateral ligament repair. J Shoulder Elbow Surg. 2007 Mar-Apr;16(2):213-7.](http://www.ncbi.nlm.nih.gov/pubmed/17399625)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17399625)
18. [Bryce CD, Armstrong AD. Anatomy and biomechanics of the elbow. Orthop Clin North Am. 2008 Apr;39(2):141-54, v. doi: 10.1016/j.ocl.2007.12.001. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/18374805)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18374805)
QUESTION 20
of 100
A 45-year-old woman has a 3-month history of left shoulder pain. Her symptoms have failed to improve despite receiving an injection and participating in 2 months of physical therapy focusing on rotator cuff strengthening. An examination reveals no weakness, atrophy, or scapular winging. She has anterior and posterior shoulder tenderness and full symmetric forward elevation and abduction, but internal rotation on the left is decreased. She has pain with internal rotation in 90 degrees of forward elevation and an increased distance between the antecubital fossa and coracoid process with cross-chest adduction when compared to the contralateral side. Radiographs reveal a type II acromion. What is the most appropriate next step?
1
MR imaging
2
MRI arthrogram
3
Posterior capsular stretching exercises
4
Arthroscopic subacromial decompression and acromioplasty
This patient demonstrates symptoms consistent with posterior capsular tightness with loss of internal rotation. This can be evaluated by comparing internal rotation to the contralateral side with the arm in 90 degrees of abduction or by reaching behind the back. Treatment consists of posterior capsular stretching such as the sleeper stretch. MR imaging or MRI arthrogram findings would most likely be unremarkable and not change the initial treatment plan. Arthroscopic surgery would be indicated for failure of nonsurgical treatment, including a dedicated stretching program. Surgery would consist of arthroscopic release of the tight posterior capsule.
RECOMMENDED READINGS
19. [Kinsella SD, Thomas SJ, Huffman GR, Kelly JD 4th. The thrower's shoulder. Orthop Clin North Am. 2014 Jul;45(3):387-401. doi: 10.1016/j.ocl.2014.04.003. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24975765)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24975765)
20. [Bach HG, Goldberg BA. Posterior capsular contracture of the shoulder. J Am Acad Orthop Surg. 2006 May;14(5):265-77. Review. PubMed PMID: 16675620.](http://www.ncbi.nlm.nih.gov/pubmed/16675620)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16675620)
QUESTION 21
of 100
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes a sedated reduction in the emergency department without complications. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, he has persistent pain at rest and forward elevation and external rotation weakness. He has no abnormal sensation. What is the best next step?
1
Physical therapy with electrical stimulation and iontophoresis
2
Corticosteroid injection
3
MR imaging of the shoulder
4
Electromyography (EMG) of the arm
For a patient in his mid 50s who has shoulder instability and persistent weakness, MR imaging is indicated to evaluate rotator cuff integrity. EMG is not indicated because this patient has no evidence of deltoid functional abnormality. Corticosteroid injections and physical therapy modalities do not address the concern about his potential for a rotator cuff tear.
RECOMMENDED READINGS
21. [Gombera MM, Sekiya JK. Rotator cuff tear and glenohumeral instability: a systematic review. Clin Orthop Relat Res. 2014 Aug;472(8):2448-56. doi: 10.1007/s11999-013-3290-2. Review. Erratum in: Clin Orthop Relat Res. 2015 Feb;473(2):751. Gomberawalla, M Mustafa ](http://www.ncbi.nlm.nih.gov/pubmed/24043432)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24043432)
22. [Paxton ES, Dodson CC, Lazarus MD. Shoulder instability in older patients. Orthop Clin North Am. 2014 Jul;45(3):377-85. doi: 10.1016/j.ocl.2014.04.002. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24975764)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24975764)
QUESTION 22
of 100
A right-hand-dominant 45-year-old man sustained an injury to the anterior aspect of his right elbow during sudden elbow flexion while trying to lift a heavy load 3 days ago. He reports the sensation of a sudden, sharp pain at the time of injury, which has since subsided. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made, and, after having a discussion with the patient, surgical treatment is chosen. During surgical reattachment, what is the relationship of the distal biceps tendon within the antecubital fossa to the median nerve and recurrent radial artery before the tendon attaches to the bicipital tuberosity?
1
The tendon travels lateral (radial) to the median nerve and posterior (deep) to the recurrent radial artery
2
The tendon travels lateral (radial) to the median nerve and anterior (superficial) to the recurrent radial artery
3
The tendon travels medial (ulnar) to the median nerve and posterior (deep) to the recurrent radial artery
4
The tendon travels medial (ulnar) to the median nerve and anterior (superficial) to the recurrent radial artery
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
RECOMMENDED READINGS
23. Leslie BM, Ranger H. Biceps tendon and triceps tendon ruptures. In: Baker CL, Plancher KD, eds. _Operative treatment of elbow injuries_. New York: Springer-Verlag; 2002:110-122.
24. [Eames MH, Bain GI, Fogg QA, van Riet RP. Distal biceps tendon anatomy: a cadaveric study. J Bone Joint Surg Am. 2007 May;89(5):1044-9. PubMed PMID: 17473142. ](http://www.ncbi.nlm.nih.gov/pubmed/17473142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17473142)
QUESTION 23
of 100
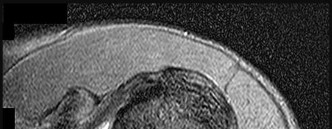
Figure 26 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder and loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
1
no difference in terminal range of motion.
2
a lower functional outcome score.
3
a clinically significant reduction in passive forward flexion and external rotation.
4
a higher retear rate of the rotator cuff repair.

Historically, orthopaedic surgeons considered early range-of-motion programs following rotator cuff surgery secondary to concerns about potential postsurgical stiffness. Although this may have been a primary open repair concern, arthroscopic surgery appears to substantially decrease this risk. More recently, investigators are reporting similar results in terms of range of motion, retear rate, and functional outcome scores among patients who undergo early and delayed rehabilitation programs.
RECOMMENDED READINGS
25. [Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010 Oct;19(7):1034-9. doi: 10.1016/j.jse.2010.04.006. Epub 2010 Jul 24. ](http://www.ncbi.nlm.nih.gov/pubmed/20655763)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20655763)
26. [Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012 Nov;21(11):1450-5. doi: 10.1016/j.jse.2012.01.025. Epub 2012 May 2. ](http://www.ncbi.nlm.nih.gov/pubmed/22554876)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22554876)
27. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
28. [Chan K, MacDermid JC, Hoppe DJ, Ayeni OR, Bhandari M, Foote CJ, Athwal GS. Delayed versus early motion after arthroscopic rotator cuff repair: a meta-analysis. J Shoulder Elbow Surg. 2014 Nov;23(11):1631-9. doi: 10.1016/j.jse.2014.05.021. Epub 2014 Aug 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25127908)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25127908)
QUESTION 24
of 100
A 44-year-old right-hand-dominant mechanic has left lateral elbow pain. He was injured at work 6 months ago when he sustained a hyperextension injury to his left arm when a tire fell off of a truck. He experienced immediate left lateral elbow pain and swelling. Initial radiograph findings in the emergency department were normal. He was given a sling, which he continues to use. He tried to do physical therapy, but he stopped after 1 visit because he said it made his pain worse. He denies any numbness or tingling but has not been able to return to work. He was given an injection in the region of the lateral epicondyle 1 month ago, which did not improve his symptoms. Upon examination, he is maximally tender to palpation about 5 cm distal to the lateral epicondyle. Active range of motion is limited by pain. He has lateral elbow pain with resisted wrist extension and resisted middle finger extension. Which test would most likely confirm a diagnosis?
1
MR imaging
2
Electromyography (EMG)
3
Bone scan
4
Lidocaine injection test
This patient’s symptoms are most consistent with radial tunnel syndrome. This diagnosis should be considered in the differential of lateral elbow pain and can often be confused with lateral epicondylitis. The patient’s symptoms did not improve with a lateral elbow injection, and his pain is located in the region of the radial tunnel. A diagnostic injection can help confirm the diagnosis. MR imaging would be helpful to rule out a ligamentous or tendon injury, which is less likely based upon the history and examination. EMG findings will most likely be normal for patients with radial tunnel syndrome. A bone scan would help to confirm complex regional pain syndrome, which is less likely in this scenario because the patient does not have hyperesthesia, loss of motion, or skin changes.
RECOMMENDED READINGS
29. [Naam NH, Nemani S. Radial tunnel syndrome. Orthop Clin North Am. 2012 Oct;43(4):529-36. doi: 10.1016/j.ocl.2012.07.022. Review. PubMed PMID: 23026469.](http://www.ncbi.nlm.nih.gov/pubmed/23026469)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23026469)
30. [Knutsen EJ, Calfee RP, Chen RE, Goldfarb CA, Park KW, Osei DA. Factors associated with failure of nonoperative treatment in lateral epicondylitis. Am J Sports Med. 2015 Sep;43(9):2133-7. doi: 10.1177/0363546515590220. Epub 2015 Jun 29. PubMed PMID: 26122386. ](http://www.ncbi.nlm.nih.gov/pubmed/26122386)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/26122386)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26122386)
CLINICAL SITUATION FOR QUESTIONS 28 THROUGH 31
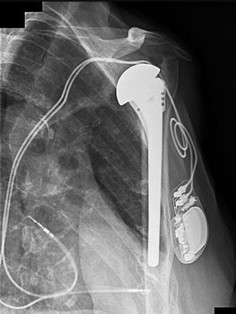
Figure 28 is the radiograph of a 78-year-old patient with a painful uncemented hemiarthroplasty of 6 months duration. Complete blood count and erythrocyte sedimentation rate findings are negative, and trauma is not a factor.
QUESTION 25
of 100
The radiograph shows components that are
1
subluxed.
2
fractured.
3
loose and potentially infected.
4
normal.
- loose and potentially infected._
.
QUESTION 26
of 100
The next step in this patient’s workup should be
1
aspiration.
2
observation.
3
physical therapy.
4
revision to total shoulder arthroplasty.
- aspiration.
QUESTION 27
of 100
If aspiration findings are negative or equivocal, the diagnosis can be established with
1
arthroscopy.
2
a bone scan.
3
a serum white blood cell level.
4
a C-reactive protein level.
- arthroscopy._
QUESTION 28
of 100
If the culture results are positive, which treatment will most likely resolve the infection?
1
Arthroscopic debridement
2
Intravenous antibiotics
3
Single-stage revision
4
Double-stage revision
Osteolysis of this magnitude is uncommon in the setting of an uncemented hemiarthroplasty. Further workup for infection is indicated, such as aspiration under fluoroscopy or ultrasound. Infection needs to be ruled out before proceeding. Observation and physical therapy are not indicated. Arthroscopy has been shown in several studies to have greater sensitivity and specificity than aspiration and can be especially effective to obtain cultures of slow-growing organisms such as Propionibacterium acnes. Blood tests are unreliable, and a bone scan would not reliably differentiate between loosening and infection. Arthroscopic debridement would not be reliable for treatment. Intravenous antibiotics can be used for suppression, but the best results in terms of resolving the infection would be achieved with 2-stage revision.
RECOMMENDED READINGS
31. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
32. Hersch JC, Dines DM. Arthroscopy for failed shoulder arthroplasty. Arthroscopy. 2000 Sep;16(6):606-
[12/. PubMed PMID: 10976121. ](http://www.ncbi.nlm.nih.gov/pubmed/10976121)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976121)
33. [Foruria AM, Fox TJ, Sperling JW, Cofield RH. Clinical meaning of unexpected positive cultures (UPC) in revision shoulder arthroplasty. J Shoulder Elbow Surg. 2013 May;22(5):620-7. doi: 10.1016/j.jse.2012.07.017. Epub 2012 Sep 13. PubMed PMID: 22981448. ](http://www.ncbi.nlm.nih.gov/pubmed/22981448)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22981448)
QUESTION 29
of 100
Figures 32a through 32c are the radiograph and CT scans of a 75-year-old smoker with hypertension who sustained a ground-level fall without loss of consciousness with impact to her
left upper extremity 1 week ago. She states that she lived independently at home with her husband prior to her fall. What is the most appropriate next step?
1
Hemiarthroplasty
2
Initial sling immobilization with subsequent physical therapy
3
Open reduction and internal fixation
4
Reverse total shoulder arthroplasty (rTSA)
The radiographs and CT scans indicate a 4-part left proximal humerus fracture with tuberosity comminution. Based upon her preinjury level of activity and current imaging studies, nonsurgical management is not the correct option to restore her ability to perform activities of daily living, including hygiene care. There has been enthusiasm among surgeons regarding the use of the reverse shoulder prosthesis as the primary mode of surgical treatment of certain 3- and 4-part proximal humerus fractures. The main attribute of this implant is its ability to achieve functional shoulder forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Nevertheless, repair and union of the greater tuberosity fragment during rTSA demonstrate improved external rotation, clinical outcomes, and patient satisfaction than outcomes achieved after tuberosity resection, nonunion, or resorption. Based upon this patient’s age and imaging findings, an rTSA would provide pain relief and improved function with complication rates similar to those associated with hemiarthroplasty. Open reduction with internal fixation would not be a viable option because of the high probability for a dysvascular head, increased risk for nonunion, and potential for revision surgery, including arthroplasty. Hemiarthroplasty for 4-part proximal humerus fractures remains a viable option for patients younger than 70 years of age with minimal tuberosity comminution and an intact rotator cuff who can comply with a postsurgical rehabilitation program. Most studies indicate significant pain relief with this modality with significant variation in functional outcomes. In this clinical scenario, the patient’s injury may not be best served with hemiarthroplasty because of uncertainty regarding functional outcome.
RECOMMENDED READINGS
34. [Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/25630370)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25630370)
35. [Bufquin T, Hersan A, Hubert L, Massin P. Reverse shoulder arthroplasty for the treatment of three- and four-part fractures of the proximal humerus in the elderly: a prospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br. 2007 Apr;89(4):516-20. ](http://www.ncbi.nlm.nih.gov/pubmed/17463122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17463122)
36. [Cuff DJ, Pupello DR. Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. J Bone Joint Surg Am. 2013 Nov 20;95(22):2050-5. doi: 10.2106/JBJS.L.01637. PubMed PMID: 24257664.](http://www.ncbi.nlm.nih.gov/pubmed/24257664)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24257664)
37. [Boyle MJ, Youn SM, Frampton CM, Ball CM. Functional outcomes of reverse shoulder arthroplasty compared with hemiarthroplasty for acute proximal humeral fractures. J Shoulder Elbow Surg. 2013 Jan;22(1):32-7. doi: 10.1016/j.jse.2012.03.006. Epub 2012 May 29. ](http://www.ncbi.nlm.nih.gov/pubmed/22652065)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22652065)
QUESTION 30
of 100
What is the role of the long head of the biceps brachii tendon in providing stability to the humeral head?
1
It provides no stability to the humeral head
2
Its stabilizing function is greatest with the shoulder forward elevated 120 degrees
3
It decreases superior translation of the humeral head only
4
It decreases anterior, inferior, and superior translation of the humeral head
Cadaveric studies have been performed to evaluate the biomechanical role of the long head of the biceps brachii tendon in providing shoulder stability. A study performed by Pagnani and associates assessed the impact of contraction of the long head of the biceps brachii on glenohumeral translation. Sequential 50-N anterior, posterior, superior, and inferior forces and a 22-N joint compressive load were applied to the shoulders. A constant force to the tendon of the long head of the biceps brachii was applied. The shoulders were tested in 7 positions of glenohumeral elevation and rotation. Application of a force to the long head of the biceps brachii resulted in statistically significant decreases in humeral head translation. The influence of the long head of the biceps was more pronounced at middle and lower elevation angles. When the shoulder was placed in 45 degrees of elevation and neutral rotation, application of a 55-N force to the biceps tendon reduced anterior translation by 10.4 mm, inferior translation by 5.3 mm, and superior translation by 1.2 mm.
A cadaveric study by Kumar and associates assessed the role of the tendon of the long head of the biceps in the stabilization of the head of the humerus. Upward migration of the humeral head was measured by noting any reduction in the acromiohumeral distance in radiographs of the shoulder.
There was a statistically significant decrease in the acromiohumeral interval on tensing the short head of biceps, but there was no significant change in the interval on tensing either the long head or both heads of the biceps brachii. Complete transection of the tendon of the long head while both heads were tensed caused a significant upward migration of the head of the humerus. This study concluded that 1 of the important functions of the long head of the biceps is to stabilize the humeral head in the glenoid during powerful elbow flexion and forearm supination. Additionally, transection of the intra-articular segment of this tendon in surgical procedures of the shoulder may produce instability and dysfunction.
RECOMMENDED READINGS
38. [Pagnani MJ, Deng XH, Warren RF, Torzilli PA, O'Brien SJ. Role of the long head of the biceps brachii in glenohumeral stability: a biomechanical study in cadavera. J Shoulder Elbow Surg. 1996 Jul-Aug;5(4):255-62. PubMed PMID: 8872922. ](http://www.ncbi.nlm.nih.gov/pubmed/8872922)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8872922)
39. [Kumar VP, Satku K, Balasubramaniam P. The role of the long head of biceps brachii in the stabilization of the head of the humerus. Clin Orthop Relat Res. 1989 Jul;(244):172-5. ](http://www.ncbi.nlm.nih.gov/pubmed/2743659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2743659)
QUESTION 31
of 100
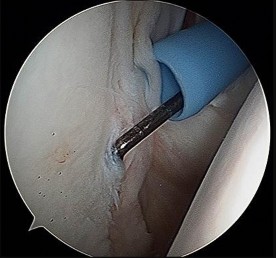
An arthroscopic image taken from the posterior portal with the patient in the lateral decubitus position is shown in Figure 34. The most appropriate treatment of this abnormality is
1
anterior labral repair with suture anchors.
2
superior labral repair with suture anchors.
3
biceps tenotomy.
4
no treatment.
The image reveals a cordlike middle glenohumeral ligament known as a Buford complex. This is a normal variant and does not necessitate treatment. The superior labrum and anterior inferior labrum are intact, and repair is not required. The biceps tendon also appears normal, making a biceps tenotomy unnecessary.
RECOMMENDED READINGS
40. [Farmer KW, Wright TW. Shoulder arthroscopy: the basics. J Hand Surg Am. 2015 Apr;40(4):817-21. doi: 10.1016/j.jhsa.2015.01.002. Epub 2015 Feb 26. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/25726045)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25726045)
41. [Keener JD, Brophy RH. Superior labral tears of the shoulder: pathogenesis, evaluation, and treatment. J Am Acad Orthop Surg. 2009 Oct;17(10):627-37. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/19794220)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19794220)
CLINICAL SITUATION FOR QUESTIONS 35 THROUGH 38
A 43-year-old right-hand-dominant man has acute right distal anterior arm pain and swelling after attempting to move his sofa. Upon examination, you find ecchymosis in the antecubital fossa with moderate swelling. He expresses pain and weakness with resisted supination of the forearm and flexion of the elbow. He is distally neurovascularly intact.
QUESTION 32
of 100
The surgeon orders MR imaging to confirm the diagnosis. How should the patient position his arm to increase study sensitivity?
1
Extended elbow, abducted shoulder, and supinated forearm
2
Extended elbow, adducted shoulder, and pronated forearm
3
Flexed elbow, abducted shoulder, and pronated forearm
4
Flexed elbow, abducted shoulder, and supinated forearm
- Flexed elbow, abducted shoulder, and supinated forearm_
QUESTION 33
of 100
If the patient chooses nonsurgical treatment, which functional loss should he anticipate?
1
10% loss of flexion strength
2
40% loss of supination strength
3
60% loss of flexion strength
4
80% loss of supination strength
- 40% loss of supination strength_
QUESTION 34
of 100
The patient elects surgical intervention. You proceed with an anterior single-incision primary repair. When comparing single- and double-incision approach complication rates, the single-incision approach is associated with
1
a lower risk for forearm synostosis.
2
a higher incidence of lateral antebrachial cutaneous nerve palsy.
3
improved objective outcome scores.
4
stronger isometric forearm supination strength.
- a higher incidence of lateral antebrachial cutaneous nerve palsy._
QUESTION 35
of 100
If surgical intervention is delayed for 3 months and intraoperatively the surgeon finds that primary repair can be performed but hyperflexion of the elbow to 90 degrees is necessary, what is the likely long-term consequence?
1
30% loss of elbow flexion strength
2
60-degree elbow flexion contracture
3
Inability to pronate the forearm past neutral
4
No significant loss of elbow range of motion
This patient classically depicts an acute complete distal biceps rupture. This injury typically results from an eccentric load applied to a flexed elbow. This occurs most often among middle-aged men. Often, a clinical examination is adequate to confirm the diagnosis. When needed, standardized MR imaging at the point at which the injured arm is flexed at the elbow and abducted at the shoulder with the forearm in supination can increase sensitivity for diagnosis of a complete tear.
Patients who do not undergo surgical repair have an approximate 40% loss of supination strength and 30% loss of elbow flexion strength. Some patients describe persistent painful cramping and difficulty with repetitive activities such as using a screwdriver. Others may be able to modify their activities and tolerate the functional loss.
Studies comparing single anterior repair to double-incision posterior repair have reported similar success rates for pain and function. Grewal and associates performed a prospective randomized clinical trial comparing single- vs double-incision distal biceps tendon repairs and reported that both techniques can provide equally successful results. However, the anterior single-incision approach resulted in a statistically significant higher incidence of transient lateral antebrachial nerve palsy (19/47 vs 3/43).
Studies have shown that primary repair may be possible for patients with subacute or chronic distal biceps tears. This may obviate the need for an additional interposition allograft reconstruction. Morrey and associates performed primary repair on 19 chronic distal biceps ruptures by hyperflexing the elbow to anatomically reattach the tendon to the biceps tuberosity. Surprisingly,
this did not lead to any significant loss of elbow range of motion or flexion contracture. Elbow flexion strength was improved.
RECOMMENDED READINGS
42. [Schmidt CC, Jarrett CD, Brown BT. The distal biceps tendon. J Hand Surg Am. 2013 Apr;38(4):811-21; quiz 821. doi: 10.1016/j.jhsa.2013.01.042. Epub 2013 Mar 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/23474326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23474326)
43. [Giuffrè BM, Moss MJ. Optimal positioning for MRI of the distal biceps brachii tendon: flexed abducted supinated view. AJR Am J Roentgenol. 2004 Apr;182(4):944-6. ](http://www.ncbi.nlm.nih.gov/pubmed/15039168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15039168)
44. [Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus nonoperative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. ](http://www.ncbi.nlm.nih.gov/pubmed/3972865)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3972865)
45. [Nesterenko S, Domire ZJ, Morrey BF, Sanchez-Sotelo J. Elbow strength and endurance in patients with a ruptured distal biceps tendon. J Shoulder Elbow Surg. 2010 Mar;19(2):184-9. doi: 10.1016/j.jse.2009.06.001. Epub 2009 Aug 6. PubMed PMID: 19664936. ](http://www.ncbi.nlm.nih.gov/pubmed/19664936)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19664936)
46. [Grewal R, Athwal GS, MacDermid JC, Faber KJ, Drosdowech DS, El-Hawary R, King GJ. Single versus double-incision technique for the repair of acute distal biceps tendon ruptures: a randomized clinical trial. J Bone Joint Surg Am. 2012 Jul 3;94(13):1166-74. doi: 10.2106/JBJS.K.00436. PubMed PMID: 22760383. ](http://www.ncbi.nlm.nih.gov/pubmed/22760383)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22760383)
47. [Morrey ME, Abdel MP, Sanchez-Sotelo J, Morrey BF. Primary repair of retracted distal biceps tendon ruptures in extreme flexion. J Shoulder Elbow Surg. 2014 May;23(5):679-85. doi: 10.1016/j.jse.2013.12.030. PubMed PMID: 24745316. ](http://www.ncbi.nlm.nih.gov/pubmed/24745316)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24745316)
QUESTION 36
of 100
Figures 39a and 39b are the radiographs of a 60-year-old woman with elbow pain at the extremes of motion; occasional locking; flexion/extension, 30-130; pronation/supination, 60/70; and no pain on forearm rotation. She injured her elbow as a teenager and had surgery at that time. What is the best next step?
1
Debridement, capsular excision, and loose body removal
2
Unconstrained total elbow arthroplasty (TEA)
3
Radial head excision
4
Elbow arthrodesis
This patient appears to have sustained a lateral condyle fracture as a young adult. She was treated with surgical repair and now has posttraumatic arthritis. The best treatment, especially in the setting of mechanical symptoms, is debridement with capsular excision to regain motion and loose body removal. Radial head excision is not indicated because she has no pronation/supination loss or pain with forearm rotation. Elbow arthrodesis is severely limiting because of an associated inability to perform activities of daily living. Unconstrained TEA is more effectively used as a salvage for an older person who has failed debridement and has mid arc motion pain. Unconstrained elbow arthroplasty mandates near-normal elbow bony architecture and intact and normal collateral ligaments, both of which may be compromised in this case.
RECOMMENDED READINGS
48. [Papatheodorou LK, Baratz ME, Sotereanos DG. Elbow arthritis: current concepts. J Hand Surg Am. 2013 Mar;38(3):605-13. doi: 10.1016/j.jhsa.2012.12.037. Epub 2013 Feb 5. Review. PubMed PMID: 23391361. ](http://www.ncbi.nlm.nih.gov/pubmed/23391361)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23391361)
49. [Ring D. Instability after total elbow arthroplasty. Hand Clin. 2008 Feb;24(1):105-12. doi: 10.1016/j.hcl.2007.11.002. Review. PubMed PMID: 18299024. ](http://www.ncbi.nlm.nih.gov/pubmed/18299024)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18299024)
QUESTION 37
of 100
A 26-year-old recreational athlete sustained an initial dislocation 1 year ago and was treated nonsurgically. He recently sustained a second dislocation and is scheduled for surgical repair. Plain radiographs and MR images reveal no bony defect. What is the difference in recurrence rate after open and arthroscopic repair?
1
Recurrence after open surgery is twice that of arthroscopic repair
2
Recurrence after arthroscopic surgery is twice that of open repair
3
Recurrence after arthroscopic repair generally occurs at an earlier time than after open repair
4
There is no difference in recurrence after open and arthroscopic repair
Traditionally, recurrence rates associated with open stabilization procedures have been lower than rates associated with arthroscopic repair. Recent studies show that for patients without significant bone loss, however, the recurrence rate is the same for open and arthroscopic surgeries.
RECOMMENDED READINGS
50. [Chalmers PN, Mascarenhas R, Leroux T, Sayegh ET, Verma NN, Cole BJ, Romeo AA. Do arthroscopic and open stabilization techniques restore equivalent stability to the shoulder in the setting of anterior glenohumeral instability? a systematic review of overlapping meta-analyses. Arthroscopy. 2015 Feb;31(2):355-63. doi: 10.1016/j.arthro.2014.07.008. Epub 2014 Sep 10. Review. PubMed PMID: 25217207. ](http://www.ncbi.nlm.nih.gov/pubmed/25217207)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25217207)
51. [Harris JD, Gupta AK, Mall NA, Abrams GD, McCormick FM, Cole BJ, Bach BR Jr, Romeo AA, Verma NN. Long-term outcomes after Bankart shoulder stabilization. Arthroscopy. 2013 May;29(5):920-33. doi: 10.1016/j.arthro.2012.11.010. Epub 2013 Feb 5. Review. PubMed PMID: 23395467. ](http://www.ncbi.nlm.nih.gov/pubmed/23395467)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23395467)
CLINICAL SITUATION FOR QUESTIONS 41 THROUGH 43
Figures 41a and 41b are the radiographs of a 69-year-old, left-hand-dominant retired man with left shoulder pain. The pain has been present for several years, although he cannot pinpoint the exact time at which it started. He worked in construction but retired 3 years ago. He now reports pain interfering with activities around the house but declines recent trauma or prior shoulder surgery. He has tried different nonsteroidal anti-inflammatory drugs prescribed by his primary care physician, but these do not provide complete relief. Upon examination, he demonstrates pain and crepitus with active and passive shoulder motion. Motion is restricted, but he can actively forward flex to 100 degrees and external rotate to 30 degrees. Rotator cuff testing reveals 5/5 strength bilaterally. He has normal neurovascular examination findings.
QUESTION 38
of 100
After discussing his diagnosis along with surgical and nonsurgical treatment options, the patient wishes to proceed with surgical intervention. He has done some online research and has questions about which procedure will produce the best outcome. Based on the current literature, what is the optimal next procedure?
1
Arthroscopic glenohumeral debridement with biceps tenotomy
2
Hemiarthroplasty
3
Total shoulder arthroplasty (TSA)
4
Reverse TSA (rTSA)
- Total shoulder arthroplasty (TSA)_
QUESTION 39
of 100
During the patient’s presurgical history and physical visit, he tells the nurse that he has a history of rheumatoid arthritis for which management by his primary care physician is required. With this new information in hand, which finding is most commonly seen on imaging during presurgical planning?
1
Glenoid medicalization
2
Posterior glenoid wear
3
Posterior subluxation of the humeral head
4
Inferior osteophytes at the humeral head
- Glenoid medialization_
QUESTION 40
of 100
Following a successful shoulder arthroplasty and hospital discharge, the patient returns for his 1-month follow-up. His staples were removed at his 2-week visit. At today’s visit his wound appears benign, and he denies drainage or fevers. He reports he was doing well until last week, at which time he reached out to close the car door, which resulted in new anterior shoulder pain. His postsurgical radiograph is shown in Figure 43. What is the most likely cause of this new finding?
1
Supraspinatus tear
2
Subscapularis tear
3
Glenoid component loosening
4
Infection
The examination and radiograph findings are consistent with glenohumeral osteoarthritis, which is now interfering with this patient’s daily activities.
Regarding surgical treatment for glenohumeral arthritis, several studies have shown that TSA is associated with better functional outcomes than hemiarthroplasty. A recent meta-analysis comparing outcomes between TSA and hemiarthroplasty revealed better function after TSA regarding pain, University of California-Los Angeles Shoulder Scores, and postsurgical forward elevation at a minimum of 2 years (Bryant and associates). In addition, Gartsman and associates showed that TSA resulted in better pain relief, function, strength, and patient satisfaction than hemiarthroplasty at 3-year follow-up. The patient in this scenario exhibits good rotator cuff strength on examination; therefore, arthroscopy with debridement or rTSA used in the setting of a massive cuff tear would not be the best answer.
Several studies have similarly shown good results with TSA in the setting of inflammatory and rheumatoid arthritis (Thomas and associates, Jolles and associates). Posterior glenoid wear is a common pattern in osteoarthritis (OA) and not a contraindication (Walch and associates). However, patients with a brachial plexus root avulsion or preganglionic injury resulting in a flail arm are not candidates for TSA because of the poor prognosis for recovery of motor and sensory deficits.
Inflammatory arthritis seen in patients with rheumatoid disease characteristically results in concentric glenoid wear and not the eccentric posterior erosion seen in OA. This concentric wear results in medialization of the glenohumeral joint line. This wear pattern can lead to severe erosion, making it difficult to achieve glenoid resurfacing. Eccentric posterior glenoid wear would lead to posterior humeral head subluxation, which is not as common in inflammatory arthritis. In addition, inferior humeral head osteophytes are seen in OA. Walch and associates have developed and published a classification system describing glenoid wear.
During TSA, exposure to the glenohumeral joint involves subscapularis management, tendon peel, or lesser tuberosity osteotomy. As a result, early postsurgical rehabilitation limits passive external rotation and active internal rotation, typically for 6 weeks, to protect the subscapularis repair. The patient in this scenario likely contracted his subscapularis, resulting in rupture of his repair. Upon clinical examination, internal rotation weakness, increased passive external rotation, and abnormal belly press or lift-off test results can be expected. One study revealed that rupture of the subscapularis was seen in all anterior dislocations following TSA (Wirth and associates).
RECOMMENDED READINGS
52. [Bryant D, Litchfield R, Sandow M, Gartsman GM, Guyatt G, Kirkley A. A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder. A systematic review and meta-analysis. J Bone Joint Surg Am. 2005 Sep;87(9):1947-56. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/16140808)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16140808)
53. [Gartsman GM, Roddey TS, Hammerman SM. Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am. 2000 Jan;82(1):26-34. PubMed PMID: 10653081.](http://www.ncbi.nlm.nih.gov/pubmed/10653081)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10653081)
54. [Norris TR, Iannotti JP. Functional outcome after shoulder arthroplasty for primary osteoarthritis: a multicenter study. J Shoulder Elbow Surg. 2002 Mar-Apr;11(2):130-5. ](http://www.ncbi.nlm.nih.gov/pubmed/11988723)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11988723)
55. [Thomas S, Price AJ, Sankey RA, Thomas M. Shoulder hemiarthroplasty in patients with juvenile idiopathic arthritis. J Bone Joint Surg Br. 2005 May;87(5):672-6. ](http://www.ncbi.nlm.nih.gov/pubmed/15855370)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15855370)
56. [Jolles BM, Grosso P, Bogoch ER. Shoulder arthroplasty for patients with juvenile idiopathic arthritis. J Arthroplasty. 2007 Sep;22(6):876-83. PubMed PMID: 17826280.](http://www.ncbi.nlm.nih.gov/pubmed/17826280)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17826280)
57. [Walch G, Badet R, Boulahia A, Khoury A. Morphologic study of the glenoid in primary glenohumeral osteoarthritis. J Arthroplasty. 1999 Sep;14(6):756-60. ](http://www.ncbi.nlm.nih.gov/pubmed/10512449)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10512449)
58. [Iannotti JP, Norris TR. Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am. 2003 Feb;85-A(2):251-8 ](http://www.ncbi.nlm.nih.gov/pubmed/12571302)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/12571302)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12571302)
59. [Miller BS, Joseph TA, Noonan TJ, Horan MP, Hawkins RJ. Rupture of the subscapularis tendon after shoulder arthroplasty: diagnosis, treatment, and outcome. J Shoulder Elbow Surg. 2005 Sep-Oct;14(5):492-6. PubMed PMID: 16194740.](http://www.ncbi.nlm.nih.gov/pubmed/16194740)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16194740)
60. [Wirth MA, Rockwood CA Jr. Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am. 1996 Apr;78(4):603-16. Review. PubMed PMID: 8609143. ](http://www.ncbi.nlm.nih.gov/pubmed/8609143)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8609143)
QUESTION 41
of 100
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis. The surgery is uncomplicated. What is the most common indication for future revision?
1
Infection
2
Periprosthetic fracture
3
Glenoid component loosening
4
Rotator cuff tearing
The most common reason for revision surgery is loosening of an implant. In most studies that distinguish glenoid from humeral loosening, it appears the glenoid is the problem. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening vs 7% for infection and 7% for rotator cuff tearing.
RECOMMENDED READINGS
61. [Matsen FA 3rd, Li N, Gao H, Yuan S, Russ SM, Sampson PD. Factors Affecting Length of Stay, Readmission, and Revision After Shoulder Arthroplasty: A Population-Based Study. J Bone Joint Surg Am. 2015 Aug 5;97(15):1255-63. doi: 10.2106/JBJS.N.01107. Erratum in: J Bone Joint Surg Am. 2015 Sep 2;97(17):e60. PubMed PMID: 26246260.](http://www.ncbi.nlm.nih.gov/pubmed/26246260)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26246260)
62. [Dillon MT, Ake CF, Burke MF, Singh A, Yian EH, Paxton EW, Navarro RA. The Kaiser Permanente shoulder arthroplasty registry: results from 6,336 primary shoulder arthroplasties. Acta Orthop. 2015 Jun;86(3):286-92. Epub 2015 Mar 2. PubMed PMID: 25727949. ](http://www.ncbi.nlm.nih.gov/pubmed/25727949)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25727949)
QUESTION 42
of 100
A 68-year-old right-hand-dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
1
Improved longevity in comparison to the linked prosthesis
2
A significantly larger flexion-extension arc
3
A higher incidence of postsurgical instability
4
Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
RECOMMENDED READINGS
63. [Kudo H, Iwano K. Total elbow arthroplasty with a non-constrained surface-replacement prosthesis in patients who have rheumatoid arthritis. A long-term follow-up study. J Bone Joint Surg Am. 1990 Mar;72(3):355-62. PubMed PMID: 2312530.](http://www.ncbi.nlm.nih.gov/pubmed/2312530)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2312530)
64. [Plaschke HC, Thillemann TM, Brorson S, Olsen BS. Implant survival after total elbow arthroplasty: a retrospective study of 324 procedures performed from 1980 to 2008. J Shoulder Elbow Surg. 2014 Jun;23(6):829-36. doi: 10.1016/j.jse.2014.02.001. Epub 2014 Apr 22. ](http://www.ncbi.nlm.nih.gov/pubmed/24766794)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24766794)
65. [Dos Remedios C, Chantelot C, Giraud F, Migaud H, Fontaine C. Results with Kudo elbow prostheses in non-traumatic indications : a study of 36 cases. Acta Orthop Belg. 2005 Jun;71(3):273-88. PubMed PMID: 16035700. ](http://www.ncbi.nlm.nih.gov/pubmed/16035700)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16035700)
QUESTION 43
of 100
Figures 46a and 46b are the radiographs of a 60-year-old man with gradual onset of right shoulder pain and motion loss 1 year after undergoing an uncomplicated right total shoulder arthroplasty
(TSA) for end-stage osteoarthritis. He denies trauma to his right shoulder and constitutional symptoms, but admits to difficulty performing activities of daily living. His surgical wound site is benign. He demonstrates active and passive forward flexion to 90 degrees, abduction to 60 degrees, external rotation to 30 degrees, and internal rotation to the lumbosacral junction. His rotator cuff strength is graded as normal and symmetrical to his unaffected left shoulder. Based upon the current evaluation, what is the most appropriate next step?
1
Revision TSA
2
Infection workup
3
CT scan of the shoulder
4
Observation and physical therapy
This patient’s radiographs do not reveal prosthetic loosening, osteolysis, instability, or rotator cuff deficiency. History and examination findings suggest a possible indolent infectious process, and it is incumbent upon the treating surgeon to obtain screening laboratory studies (complete blood count with differential, erythrocyte sedimentation rate, and C-reactive protein) and proceed with obtaining cultures (via joint aspiration or arthroscopic soft-tissue biopsy) to rule out an infectious process. Cultures should be held for 2 weeks to evaluate for the possibility of a Propionibacterium acnes infection, which is the predominant organism elicited from painful and stiff TSAs for which revision is required. Immediate revision TSA is not indicated in this scenario because the components appear well fixed and positioned. Observation and therapy in the setting of deterioration of a previously well-functioning TSA also are not appropriate.
RECOMMENDED READINGS
66. [Pottinger P, Butler-Wu S, Neradilek MB, Merritt A, Bertelsen A, Jette JL, Warme WJ, Matsen FA 3rd. Prognostic factors for bacterial cultures positive for Propionibacterium acnes and other organisms in a large series of revision shoulder arthroplasties performed for stiffness, pain, or loosening. J Bone Joint Surg Am. 2012 Nov 21;94(22):2075-83. doi: 10.2106/JBJS.K.00861. ](http://www.ncbi.nlm.nih.gov/pubmed/23172325)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23172325)
67. Dodson CC, Craig EV, Cordasco FA, Dines DM, Dines JS, Dicarlo E, Brause BD, Warren RF. Propionibacterium acnes infection after shoulder arthroplasty: a diagnostic challenge. J Shoulder Elbow Surg. 2010 Mar;19(2):303-7. doi: 10.1016/j.jse.2009.07.065. Epub 2009 Nov 1. PubMed PMID:
[19884021/. ](http://www.ncbi.nlm.nih.gov/pubmed/19884021)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884021)
68. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
CLINICAL SITUATION FOR QUESTIONS 47 AND 48
A 42-year-old mechanic has right medial elbow pain that is worse with use at work. He denies any injury to the arm. He has no significant medical history, but he smokes a pack of cigarettes each day. He has filed a Workers’ Compensation claim and has hired an attorney. He is still working his full job duty, but he expresses dissatisfaction with his employer. An examination reveals tenderness to palpation maximally anterior to the medial epicondyle. Pain is worse with resisted wrist flexion and resisted forearm pronation.
QUESTION 44
of 100
What is the most common coexisting pathology in this scenario?
1
Ulnar neuropathy at the cubital tunnel
2
Lateral epicondylitis
3
Triceps tendinosis
4
Posterolateral rotatory instability
- Ulnar neuropathy at the cubital tunnel_
QUESTION 45
of 100
The patient’s symptoms fail to improve after a 6-month course of nonsurgical treatment. His inability to return to his full job duties after surgery is most likely related to
1
poor job satisfaction.
2
his smoking habit.
3
representation by an attorney.
4
ligament instability.
This patient has typical signs and symptoms of medial epicondylitis. The most common coexisting pathology is ulnar nerve compression. Less commonly, patients may have other tendon issues
including lateral epicondylitis and triceps tendinosis. Posterolateral instability is most commonly a tennis elbow surgery complication or results from trauma with injury to the lateral ulnar collateral ligament. A patient’s ability to return to work is most commonly predicated upon his or her job satisfaction prior to sustaining a work-related injury.
RECOMMENDED READINGS
69. [Amin NH, Kumar NS, Schickendantz MS. Medial epicondylitis: evaluation and management. J Am Acad Orthop Surg. 2015 Jun;23(6):348-55. doi: 10.5435/JAAOS-D-14-00145. Review. PubMed PMID: 26001427. ](http://www.ncbi.nlm.nih.gov/pubmed/26001427)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26001427)
70. [Gruson KI, Huang K, Wanich T, Depalma AA. Workers' compensation and outcomes of upper extremity surgery. J Am Acad Orthop Surg. 2013 Feb;21(2):67-77. doi: 10.5435/JAAOS-21-02-67. Review. PubMed PMID: 23378370. ](http://www.ncbi.nlm.nih.gov/pubmed/23378370)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23378370)
QUESTION 46
of 100
Figure 49 is the radiograph of a 54-year-old man who has increasing weakness and numbness in his lateral arm. No prior surgery or injury is reported. What is the most appropriate next diagnostic test?
1
MR imaging of the shoulder
2
MR imaging of the cervical spine
3
Chest CT scan
4
Chest radiograph
The radiograph reveals a Charcot shoulder. The atraumatic dissolving of the humeral head is concerning for a neuropathic etiology and necessitates MR imaging of the cervical spine to evaluate for the presence of a syrinx.
RECOMMENDED READINGS
71. [Drvaric DM, Rooks MD, Bishop A, Jacobs LH. Neuropathic arthropathy of the shoulder. A case report. Orthopedics. 1988 Feb;11(2):301-4. PubMed PMID: 3357846. ](http://www.ncbi.nlm.nih.gov/pubmed/3357846)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3357846)
72. [Patel AY, Eagle KA, Vaishnava P. Cardiac Risk of Noncardiac Surgery. J Am Coll Cardiol. 2015 Nov 10;66(19):2140-8. doi: 10.1016/j.jacc.2015.09.026. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/26541926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26541926)
QUESTION 47
of 100
When a patient has acute or chronic anterior shoulder instability, a bony or glenoid reconstructive procedure should be considered in which clinical setting?
1
Associated humeral avulsion of the glenohumeral ligament (HAGL) lesion
HAGL lesions may be initially treated without surgery. Recurrent instability in the setting of a HAGL lesion may be treated with a soft-tissue repair. A nonengaging or nontracking Hill-Sachs lesion may be treated with an anterior soft-tissue (Bankart) repair. A tracking or engaging lesion may be treated with a bony glenoid procedure or a soft-tissue procedure plus remplissage. An ALPSA lesion may be treated with a soft-tissue procedure unless it is associated with a glenoid bony defect exceeding 25%. A glenoid bony defect exceeding 25% is associated with substantially higher recurrence than defects smaller than 20%, and consideration for bony glenoid reconstruction is advised.
RECOMMENDED READINGS
73. [Beran MC, Donaldson CT, Bishop JY. Treatment of chronic glenoid defects in the setting of recurrent anterior shoulder instability: a systematic review. J Shoulder Elbow Surg. 2010 Jul;19(5):769-80. doi: 10.1016/j.jse.2010.01.011. Epub 2010 Apr 14. Review. PubMed PMID: 20392650. ](http://www.ncbi.nlm.nih.gov/pubmed/20392650)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20392650)
74. [Boileau P, Villalba M, Héry JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006 Aug;88(8):1755-63. PubMed PMID: 16882898. ](http://www.ncbi.nlm.nih.gov/pubmed/16882898)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16882898)
QUESTION 48
of 100
Figure 51 is the MR image of a 23-year-old Minor League pitcher who has dominant elbow pain. He reports a pop while throwing and loss of velocity and control. He has failed nonsurgical treatment that included rest and physical therapy. What is the most common complication following surgical treatment of this injury?
1
Infection
2
Medial epicondyle fracture
3
Arthrofibrosis
4
Ulnar nerve irritation
This competitive thrower’s clinical picture and imaging findings are consistent with an ulnar collateral ligament (UCL) injury. For patients who fail nonsurgical treatment, UCL reconstruction is an accepted surgical solution. About 80% of overhead athletes return to at least the same level of competition. All of the responses are potential complications following UCL reconstruction, but ulnar neuritis is the most common, occurring in approximately 6% to 13% of patients.
RECOMMENDED READINGS
75. [Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008 Jun;36(6):1193-205. doi: 10.1177/0363546508319053. Review. PubMed PMID: 18490476. ](http://www.ncbi.nlm.nih.gov/pubmed/18490476)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18490476)
76. [Cain EL Jr, Andrews JR, Dugas JR, Wilk KE, McMichael CS, Walter JC 2nd, Riley RS, Arthur ST. Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: Results in 743 athletes with minimum 2-year follow-up. Am J Sports Med. 2010 Dec;38(12):2426-34. doi: 10.1177/0363546510378100. Epub 2010 Oct 7. PubMed PMID: 20929932. ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/20929932)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20929932)
77. Watson JN, McQueen P, Hutchinson MR. A systematic review of ulnar collateral ligament reconstruction techniques. Am J Sports Med. 2014 Oct;42(10):2510-6. doi: 10.1177/0363546513509051. Epub 2013 Nov 12. Review. PubMed PMID: 24220014.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24220014)
QUESTION 49
of 100
What most accurately describes treatment of displaced proximal humerus fractures involving the humeral neck for elderly patients?
1
Hemiarthroplasty provides better clinical outcome measures at 2 years
2
Early physiotherapy improves outcomes at 2 years
3
Complication rates are higher after surgical treatment than with a sling
4
Surgical treatment increases risk for future surgery
A Cochrane Review of the literature demonstrated no differences regarding inclusion of physical therapy and complication rates between surgical and nonsurgical treatment and outcomes. Surgery as initial treatment is associated with an increased risk for later surgery than nonsurgical initial treatment.
RECOMMENDED READINGS
78. [Handoll HH, Brorson S. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst Rev. 2015 Nov 11;11:CD000434. doi: 10.1002/14651858.CD000434.pub4. Review. PubMed PMID: 26560014.](http://www.ncbi.nlm.nih.gov/pubmed/26560014)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26560014)
79. [Cuff DJ, Pupello DR. Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. J Bone Joint Surg Am. 2013 Nov 20;95(22):2050-5. doi: 10.2106/JBJS.L.01637. PubMed PMID: 24257664. ](http://www.ncbi.nlm.nih.gov/pubmed/24257664)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24257664)
QUESTION 50
of 100
A 35-year-old high school volleyball coach has an acute 1-day history of right elbow pain and swelling in the antecubital fossa. He was moving equipment when his symptoms began. He describes considerable weakness with forearm supination and elbow flexion. Upon examination, he has a proximal “Popeye” deformity. In surgery, attention is first focused on identifying the ruptured tendon stump. During the anterior exposure, a nerve is appreciated just lateral of midline as it appears in between the brachialis and biceps stump. It continues distally under the cephalic vein and disappears distally down the forearm. This anatomic structure is the
1
radial nerve.
2
lateral antebrachial cutaneous nerve.
3
superficial branch of the radial nerve.
4
median nerve.
Injury to the lateral antebrachial cutaneous nerve is among the most common complications following repair of distal biceps ruptures. This nerve enters the antecubital fossa between the biceps and brachialis muscles. It usually emerges from beneath the lateral aspect of the biceps tendon at the level of the interepicondylar line. It then travels down the forearm more superficially beneath the cephalic vein. The ruptured biceps tendon may displace it further midline, distorting its normal course. The orthopaedic surgeon must maintain a heightened awareness to this nerve’s location during exposure to minimize risk for iatrogenic injury.
RECOMMENDED READINGS
80. Doyle JR. Forearm. In: Doye JR, Botte MJ, eds. _Surgical Anatomy of the Hand and Upper Extremity_. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:365-406.
81. [Jarrett CD, Brown BT, Schmidt CC. Anatomic distal biceps and triceps tendon repairs. Oper Tech Orthop. 2013; 23: 215-223. ](https://www.researchgate.net/publication/259141943_%20Anatomic_Distal_Biceps_and_Triceps_Tendon_Repairs)[https://www.researchgate.net/publication/259141943_](https://www.researchgate.net/publication/259141943_%20Anatomic_Distal_Biceps_and_Triceps_Tendon_Repairs)
Anatomic_Distal_Biceps_and_Triceps_Tendon_Repairs (Accessed June 9, 2016).
82. [Bourne MH, Wood MB, Carmichael SW. Locating the lateral antebrachial cutaneous nerve. J Hand Surg Am. 1987 Sep;12(5 Pt 1):697-9. PubMed PMID: 3655226. ](http://www.ncbi.nlm.nih.gov/pubmed/3655226)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3655226)
CLINICAL SITUATION FOR QUESTIONS 54 THROUGH 57
Figures 54a through 54f are the radiographs, CT scans, and arthroscopic images of a right-hand-dominant 18-year-old man who reports a history of right shoulder recurrent anterior instability. He sustained his first traumatic anterior dislocation after a fall while playing basketball 9 months ago. After closed reduction in the emergency department, he was initially treated with sling immobilization for 2 weeks followed by physical therapy for progression to full range of motion with rotator cuff strengthening. He subsequently has sustained 2 anterior dislocations during overhead activities, each necessitating closed reduction in the emergency department. Upon examination, anterior apprehension and relocation test findings are positive with the shoulder in the abducted and externally rotated position; posterior jerk test and sulcus test findings are negative, and he has no evidence of generalized ligamentous laxity. Imaging studies reveal less than 10% bone loss of the anterior glenoid along with a Hill-Sachs lesion.
QUESTION 51
of 100
The likely detached ligamentous lesion is tightest when the position of the shoulder is
1
45-degree abduction, internal rotation.
2
45-degree abduction, external rotation.
3
90-degree abduction, external rotation.
4
90-degree abduction, internal rotation.
- 90-degree abduction, external rotation._
QUESTION 52
of 100
For patients who sustain their first anterior glenohumeral dislocation during sports activity, which associated injury is most commonly expected at the time of the initial dislocation?
1
Rotator cuff tear
2
Axillary nerve palsy
3
Greater tuberosity fracture
4
Biceps tendon rupture
- Axillary nerve palsy_
QUESTION 53
of 100
At the time of arthroscopy, the posterior humeral head Hill-Sachs lesion substantially engages with the glenoid; CT and arthroscopic findings reveal minimal glenoid bone loss. In addition to arthroscopic Bankart repair, arthroscopic Hill-Sachs remplissage with suture anchors is performed. In combined Bankart repair with Hill-Sachs remplissage vs Bankart repair alone, which complication is of highest potential concern?
1
Increase in shoulder external rotation of approximately 10 degrees vs the uninjured shoulder
2
Increased rate of recurrent dislocation
3
Loss of shoulder external rotation of approximately 10 degrees vs the uninjured shoulder
4
Lower rate of return to previous level of sports participation
- Loss of shoulder external rotation of approximately 10 degrees vs the uninjured shoulder_
QUESTION 54
of 100
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
1
axial loading of the glenohumeral joint.
2
isolated hyperabduction.
3
combined 45-degree abduction and external rotation.
4
combined hyperabduction and external rotation.
For patients with anterior shoulder instability, most commonly, a Bankart lesion, or detachment of the anteroinferior labrum with the attached inferior glenohumeral ligament from the glenoid rim is found. A medialized anteroinferior capsulolabral attachment (ALPSA lesion) is a common finding in shoulders with chronic anterior instability. The anterior band of the inferior glenohumeral ligament is tightest with the arm in 90 degrees of abduction with the shoulder externally rotated, creating a “hammock” that supports the humeral head. At 45 degrees of shoulder
abduction, the capsuloligamentous components of the shoulder are at their loosest, resulting in the most total superior-inferior translation.
During traumatic anterior glenohumeral dislocation, associated injuries commonly occur. In a prospective database of 3633 patients who sustained a traumatic anterior glenohumeral dislocation, 13.5% had a neurologic deficit following reduction, the majority of which were injuries to the axillary nerve. The injuries typically were sensory but not motor deficits and resolved spontaneously over time. These isolated axillary nerve injuries were more common in young, athletic patients. Associated rotator cuff tears and greater tuberosity fractures are commonly associated with shoulder dislocation as well and are more common in patients 60 years of age and older.
Large, engaging posterior humeral head Hill-Sachs lesions are associated with increased rates of recurrent shoulder instability. At the time of surgical arthroscopy, the Hill-Sachs lesion should be assessed for engagement with the glenoid. In the absence of significant glenoid bone loss, some patients with engaging Hill-Sachs defects may be suitable for combined Bankart repair and Hill-Sachs remplissage at the time of surgery. When these procedures are combined, patients have an approximate 10-degree decreased shoulder external rotation with the arm at the side and in abduction when compared to the contralateral, uninjured shoulder. Rates of recurrent dislocation and return to sport are comparable to those for patients undergoing Bankart repair alone.
Humeral avulsion of the glenohumeral ligaments (HAGL) has become a well-recognized cause of recurrent shoulder instability and is reported in 1% to 9% of patients. HAGL lesions can occur in isolation or, more commonly, may be associated with other abnormalities such as a tear of the rotator cuff, Bankart lesion, Hill-Sachs deformity, or labral tear. Recurrence of shoulder instability is more likely to occur if there is failure to identify a HAGL lesion. HAGL lesions can result from trauma in the setting of combined hyperabduction and external rotation. This is in contrast to a Bankart lesion, which is a result of trauma when the shoulder is hyperabducted without substantial associated rotation.
RECOMMENDED READINGS
1. [Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):675-85. PubMed PMID: 1456361. ](http://www.ncbi.nlm.nih.gov/pubmed/1456361)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1456361)
2. [Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am. 2012 Jan 4;94(1):18-26. doi: 10.2106/JBJS.J.01795. PubMed PMID: 22218378. ](http://www.ncbi.nlm.nih.gov/pubmed/22218378)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22218378)
3. [Visser CP, Coene LN, Brand R, Tavy DL. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999 Jul;81(4):679-85. PubMed PMID: 10463745. ](http://www.ncbi.nlm.nih.gov/pubmed/10463745)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10463745)
4. [Boileau P, O'Shea K, Vargas P, Pinedo M, Old J, Zumstein M. Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am. 2012 Apr 4;94(7):618-26. doi: 10.2106/JBJS.K.00101. PubMed PMID: 22488618. ](http://www.ncbi.nlm.nih.gov/pubmed/22488618)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22488618)
5. [Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007 Nov;35(11):1960-6. Epub 2007 Apr 9. Review. PubMed PMID: 17420506. ](http://www.ncbi.nlm.nih.gov/pubmed/17420506)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17420506)
QUESTION 55
of 100
A 71-year-old woman with a history of rheumatoid arthritis has right elbow pain. Her rheumatologist has referred her for failure of medical treatment. Figures 58a and 58b are her anteroposterior and lateral radiographs. What is the best next step?
1
An arthroscopic synovectomy, which will provide long-term pain relief
2
An interposition arthroplasty, which will be reliable for pain relief at the expense of a permanent 5-pound lifting restriction
3
Total elbow arthroplasty (TEA); the infection rate will be lower than if performed for posttraumatic arthritis
4
A TEA, which likely will provide better longevity than if performed for posttraumatic arthritis
This patient has symptoms and radiograph findings consistent with advanced inflammatory arthritis of the elbow. Although synovectomy has utility during earlier stages of disease, once bony changes occur, arthroscopic synovectomy is unlikely to provide long-term pain relief. Interposition arthroplasty is advocated in younger patients who may not be able to comply with the permanent 5- to 10-pound lifting restriction that accompanies a TEA, but it is less reliable for long-term pain relief. Infection after TEA remains a concern and is more common when this procedure is performed to address inflammatory arthritis and not posttraumatic sequelae. Persistent wound drainage after TEA is highly suggestive of a deep infection and is predictive of eventual component resection. However, TEA longevity is superior when performed to address inflammatory arthritis.
RECOMMENDED READINGS
1. [Horiuchi K, Momohara S, Tomatsu T, Inoue K, Toyama Y. Arthroscopic synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am. 2002 Mar;84-A(3):342-7. ](http://www.ncbi.nlm.nih.gov/pubmed/11886901)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11886901)
2. [Ljung P, Jonsson K, Larsson K, Rydholm U. Interposition arthroplasty of the elbow with rheumatoid arthritis. J Shoulder Elbow Surg. 1996 Mar-Apr;5(2 Pt 1):81-5. ](http://www.ncbi.nlm.nih.gov/pubmed/8742870)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8742870)
3. [Jeon IH, Morrey BF, Anakwenze OA, Tran NV. Incidence and implications of early postoperative wound complications after total elbow arthroplasty. J Shoulder Elbow Surg. 2011 Sep;20(6):857-65. doi: 10.1016/j.jse.2011.03.005. Epub 2011 Jun 8. PubMed PMID: 21641829. ](http://www.ncbi.nlm.nih.gov/pubmed/21641829)[View Abstract at ](http://www.ncbi.nlm.nih.gov/pubmed/21641829)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21641829)
QUESTION 56
of 100
Figure 59 is the MR image of a 17-year-old high school wrestler who has had multiple subluxation episodes of his right shoulder. Physical therapy has not controlled his symptoms, and he was unable to finish the wrestling season because of pain and instability. CT scanning is suggested. What is the advantage of a CT scan?
1
Bone loss is more reliably visualized than with MR imaging
2
Soft-tissue damage is more reliably imaged with a CT scan
3
Atrophy is better assessed using the Goutallier classification
4
Multidirectional instability can be ruled out
Most studies suggest that bone loss is most accurately imaged with a CT scan. Soft-tissue damage is more difficult to assess. Although the Goutallier classification for fatty infiltration is based on CT and not MR imaging findings, this is not relevant here. Multidirectional instability is a clinical, not imaging, diagnosis. CT’s substantial radiation dose can be especially harmful to young people
who presumably could live long enough to develop radiation-induced malignancies. Cost differences are minimal, and faster acquisition times are not clinically relevant. Breast and thyroid tissue exposure poses increased risk for radiation exposure for shoulder CT.
RECOMMENDED READINGS
4. [Jahnke AH Jr, Petersen SA, Neumann C, Steinbach L, Morgan F. A prospective comparison of computerized arthrotomography and magnetic resonance imaging of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):695-700; discussion 700-1. ](http://www.ncbi.nlm.nih.gov/pubmed/1456363)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1456363)
5. [Orchard JJ, Orchard JW, Grenfell T, Mitchell A. Ionising radiation: three game-changing studies for imaging in sports medicine. Br J Sports Med. 2014 Apr;48(8):677-8. doi: 10.1136/bjsports-2013-092499. Epub 2013 Jun 1. PubMed PMID: 23729176. ](http://www.ncbi.nlm.nih.gov/pubmed/23729176)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23729176)
6. [What are the Radiation Risks from CT? ](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)[http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-](http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm115329.htm)Rays/ucm115329.htm (Accessed August 25, 2016).
RESPONSES FOR QUESTIONS 60 THROUGH 66
1. Initial period of sling immobilization followed by physical therapy
2. Open reduction and internal fixation with or without bone grafting
3. Reverse total shoulder arthroplasty (rTSA)
4. Hemiarthroplasty
5. Unconstrained (TSA)
6. Closed reduction and Kirschner wire (K-wire) stabilization
Match the treatment listed above with the clinical scenario described below.
QUESTION 57
of 100
A 70-year-old woman with a 4-part proximal humerus fracture dislocation and history of failed rotator cuff repair
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Reverse total shoulder arthroplasty (rTSA)_
QUESTION 58
of 100
A 35-year-old man with a 2-part anterior proximal humerus fracture-dislocation
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Open reduction and internal fixation with or without bone grafting_
QUESTION 59
of 100
A 55-year-old man with a 4-part proximal humerus fracture with intra-articular comminution and a large greater tuberosity fragment
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Hemiarthroplasty_
QUESTION 60
of 100
A 37-year-old man with an irreducible posterior 2-part proximal humerus fracture dislocation
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Open reduction and internal fixation with or without bone grafting_
QUESTION 61
of 100
A 65-year-old woman with a nondisplaced surgical neck proximal humerus fracture
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Initial period of sling immobilization followed by physical therapy_
QUESTION 62
of 100
A 75-year-old man with a 4-part proximal humerus fracture and comminuted tuberosities
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Reverse total shoulder arthroplasty (rTSA)_
QUESTION 63
of 100
A 50-year-old woman with a 2-part surgical neck proximal humerus fracture and metaphyseal comminution
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
Proximal humerus fractures account for approximately 5% of all fractures, with incidence increasing to reflect an aging population and related osteoporosis. Treatment is dependent upon the mechanism of injury, the patient’s physiologic age and activity level, the fracture pattern, and rotator cuff integrity. Most of these injuries are nondisplaced or minimally displaced and are associated with a good overall prognosis with nonsurgical treatment and temporary impairment. A patient with a nondisplaced surgical neck fracture should be treated without surgery. K-wire stabilization, although technically difficult to achieve, is an option for compliant patients with 2-part, 3-part, and valgus-impacted 4-part fractures who have adequate bone stock. Valgus-impacted 4-part fractures pose reduced risk for osteonecrosis because of the preserved blood supply through the medial hinge, which allows for this technique. For displaced 2-part fractures accompanied by
metaphyseal comminution, K-wire fixation cannot provide adequate stability to initiate a graduated home exercise or outpatient physical therapy program. Formal open reduction with intramedullary or plate fixation in addition to bone grafting (fibular strut allograft) is the best surgical option for the clinical scenario involving a displaced surgical neck fracture with comminution. Osteosynthesis of 3-part fractures may be feasible for physiologically young and active patients without humeral head involvement and osteoporosis.
Current indications for primary hemiarthroplasty include most 4-part fractures, 3-part fractures and dislocations in elderly patients with osteoporotic bone, head-splitting articular segment fractures, and chronic anterior or posterior humeral head dislocations with more than 40% of articular surface involvement. Because of the intra-articular nature of this patient’s 4-part injury in this scenario, hemiarthroplasty with anatomic reconstruction of the greater and lesser tuberosities is most appropriate. Relative indications for hemiarthroplasty also include fractures with more than 20 degrees of varus, associated moderate to severe osteopenia, and revision surgery for failed osteosynthesis. Currently accepted indications for rTSA include scenarios in which the fracture pattern, level of comminution, bone quality, and rotator cuff deficiency preclude plate fixation or hemiarthroplasty. Scenarios involving 4-part fractures and associated rotator cuff tears and tuberosity comminution are best served with a reverse shoulder prosthesis. One of the positive attributes of this implant is the ability to achieve functional forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Caution is warranted with this surgical technique because complication rates are higher than for hemiarthroplasty reconstruction. Acute, irreducible 2-part fracture-dislocations of the proximal humerus necessitate open reduction and internal fixation of the affected tuberosities (posterior, lesser tuberosity; anterior, greater tuberosity) through screw, anchor, and/or suture fixation. These fracture-dislocations can be managed with this technique because of the integrity of the vascular supply, which is maintained by the soft-tissue attachments to the intact tuberosities. Repeated attempts at a closed reduction in the 37-year-old with the posterior fracture-dislocation could result in neurovascular injury and myositis ossificans and should be avoided. Arthroplasty reconstruction in this scenario should not be the index procedure in light of concerns regarding implant survivorship in patients of this age and their assumed elevated activity levels.
RECOMMENDED READINGS
1. [Harrison AK, Gruson KI, Zmistowski B, Keener J, Galatz L, Williams G, Parsons BO, Flatow EL. Intermediate outcomes following percutaneous fixation of proximal humeral fractures. J Bone Joint Surg Am. 2012 Jul 3;94(13):1223-8. doi: 10.2106/JBJS.J.01371. ](http://www.ncbi.nlm.nih.gov/pubmed/22760391)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22760391)
2. [Iannotti JP, Ramsey ML, Williams GR Jr, Warner JJ. Nonprosthetic management of proximal humeral fractures. Instr Course Lect. 2004;53:403-16. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/15116630)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15116630)
3. [Mata-Fink A, Meinke M, Jones C, Kim B, Bell JE. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J Shoulder Elbow Surg. 2013 Dec;22(12):1737-48. doi: 10.1016/j.jse.2013.08.021. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24246529)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24246529)
4. [Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/25630370)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25630370)
5. [Bae JH, Oh JK, Chon CS, Oh CW, Hwang JH, Yoon YC. The biomechanical performance of locking plate fixation with intramedullary fibular strut graft augmentation in the treatment of unstable fractures of the proximal humerus. J Bone Joint Surg Br. 2011 Jul;93(7):937-41. ](http://www.ncbi.nlm.nih.gov/pubmed/21705567)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21705567)
6. [Kontakis G, Koutras C, Tosounidis T, Giannoudis P. Early management of proximal humeral fractures with hemiarthroplasty: a systematic review. J Bone Joint Surg Br. 2008 Nov;90(11):1407-13. doi: 10.1302/0301-620X.90B11.21070. Review. PubMed PMID: 18978256. ](http://www.ncbi.nlm.nih.gov/pubmed/18978256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18978256)
7. [Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. ](http://www.ncbi.nlm.nih.gov/pubmed/15220884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15220884)
CLINICAL SITUATION FOR QUESTIONS 67 THROUGH 70
Figure 67 is the radiograph of a right-hand-dominant 70-year-old woman who arrives at the emergency department with acute left shoulder pain following a fall down a flight of stairs. She expresses acute diffuse left shoulder pain and swelling. Prior to her injury, she had full active painless shoulder range of motion.
QUESTION 64
of 100
Which radiographic parameter places this patient at highest risk for osteonecrosis?
1
3-part displaced valgus-type fracture pattern
2
3-part displaced varus-type fracture pattern
3
Anterior fracture extension disrupting the bicipital groove
4
Posteromedial metaphyseal head extension of less than 8 mm
- Posteromedial metaphyseal head extension of less than 8 mm_
QUESTION 65
of 100
What is the most common complication following open reduction locking plate osteosynthesis of this injury?
1
Intra-articular screw penetration
2
Posttraumatic avascular necrosis (AVN)
3
Nonunion
4
Subacromial plate impingement
- Intra-articular screw penetration_
QUESTION 66
of 100
When considering arthroplasty options, which statement is true regarding hemiarthroplasty or rTSA?
1
Midterm objective outcome scores following hemiarthroplasty are superior
2
Results following rTSA are less dependent on anatomic tuberosity healing
3
rTSA is associated with a lower complication rate
4
Patients who undergo hemiarthroplasty report a higher average visual analog pain score
- Results following rTSA are less dependent on anatomic tuberosity healing_
QUESTION 67
of 100
If a patient develops posttraumatic osteonecrosis after undergoing head preservation treatment, which radiographic findings help to predict a lower likelihood of successful conversion to an anatomic shoulder arthroplasty?
1
Valgus malunion of the head shaft angle
2
Varus malunion of the greater tuberosity, necessitating osteotomy
3
Intra-articular screw penetration
4
Cephalic collapse of the humeral head
Fractures of the proximal humerus are now the third-most-common fracture in patients older than 60 years of age. This patient sustained a displaced, commonly described 3-part/4-part proximal humerus fracture. The number of fracture fragments and angulation, as initially described by Codman and then Neer, does not necessarily help to predict risk for subsequent AVN. Although the main blood supply to the humeral head historically was believed to be a branch from the anterior circumflex, adequate perfusion can remain through the posteromedial calcar following trauma. Hertel and associates reported that the most accurate predictor of ischemia was whether the length of the metaphyseal head extension for the calcar segment was shorter than 8 mm.
Locking plates have provided surgical alternatives to many unstable fracture patterns previously considered ominous. Although much enthusiasm remains for this use, a relatively high level of
complications has been reported with their use. A multicenter study reported a 14% incidence of intra-articular screw perforation as the most common complication.
When patients are deemed poor candidates for head preservation treatment, both hemiarthroplasty and rTSA can provide successful results when applied and performed appropriately. An increasing body of evidence appears to support consideration of a reverse prosthesis for older patients. A crucial aspect of hemiarthroplasty success is anatomic healing of the tuberosities around the implant. If the greater tuberosity displaces or reabsorbs, patients experience significant loss of active motion. The level of pain, however, is unpredictable. Although beneficial in a reverse prosthesis, anatomic tuberosity position does not appear to be as crucial. Depending on the definition of “complication,” some researchers have reported a higher complication rate for the reverse prosthesis.
If posttraumatic necrosis develops following head preservation treatment, conversion to an anatomic shoulder arthroplasty can provide good success in motion and function, particularly when the tuberosities heal in a relatively anatomic position. However, several researchers, most recently Moineau and associates, report suboptimal results when the greater tuberosity is positioned in a substantial amount of varus that necessitates osteotomy. In this scenario, rTSA should be considered.
RECOMMENDED READINGS
8. [Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. ](http://www.ncbi.nlm.nih.gov/pubmed/15220884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15220884)
9. [Südkamp N, Bayer J, Hepp P, Voigt C, Oestern H, Kääb M, Luo C, Plecko M, Wendt K, Köstler W, Konrad G. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am. 2009 Jun;91(6):1320-8. PubMed PMID: 19487508. ](http://www.ncbi.nlm.nih.gov/pubmed/19487508)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19487508)
10. [Anakwenze OA, Zoller S, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for acute proximal humerus fractures: a systematic review. J Shoulder Elbow Surg. 2014 Apr;23(4):e73-80. doi: 10.1016/j.jse.2013.09.012. Epub 2014 Jan 7. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24406120)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24406120)
11. [Jarrett CD, Brown BT, Schmidt CC. Reverse shoulder arthroplasty. Orthop Clin North Am. 2013 Jul;44(3):389-408, Epub 2013 Apr 29. Review. PubMed PMID: 23827841. ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[View Abstract ](http://www.ncbi.nlm.nih.gov/pubmed/23827841)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23827841)
12. Moineau G, McClelland WB Jr, Trojani C, Rumian A, Walch G, Boileau P. Prognostic factors and limitations of anatomic shoulder arthroplasty for the treatment of posttraumatic cephalic collapse or necrosis (type-1 proximal humeral fracture sequelae). J Bone Joint Surg Am. 2012 Dec 5;94(23):2186-
[94/. doi: 10.2106/JBJS.J.00412. PubMed PMID: 23224389. ](http://www.ncbi.nlm.nih.gov/pubmed/23224389)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23224389)
13. [Namdari S, Horneff JG, Baldwin K. Comparison of hemiarthroplasty and reverse arthroplasty for treatment of proximal humeral fractures: a systematic review. J Bone Joint Surg Am. 2013 Sep 18;95(18):1701-8.. PubMed PMID: 24048558. ](http://www.ncbi.nlm.nih.gov/pubmed/24048558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24048558)
QUESTION 68
of 100
Figures 71a and 71b are the radiographs of a 65-year-old right-hand-dominant woman who sustained a Mason type III radial head fracture 3 years ago. She was treated with radial head replacement, but she never regained normal function and now has pain. What do the radiographs reveal?
1
No visible pathology
2
Osteomyelitis with loosening of the implant
3
Posttraumatic changes with an “overstuffed” radial head
4
Evidence of fibrodysplasia ossificans progressiva
The radiographs reveal a radial head implant that is too thick. Overlengthening the lateral side of the joint has caused medial translocation of the ulna on the trochlea, and the ulna-humeral joint is not congruent. The patient has developed stiffness and pain as a result. There is no evidence of infection or loosening. Although there is heterotopic ossification, there are no distinctive signs of fibrodysplasia ossificans progressiva.
RECOMMENDED READINGS
14. Alolabi B, Studer A, Gray A, Ferreira LM, King GJ, Johnson JA, Athwal GS. Selecting the diameter of a radial head implant: an assessment of local landmarks. J Shoulder Elbow Surg. 2013 Oct;22(10):1395-9. doi: 10.1016/j.jse.2013.04.005. Epub 2013 Jun 20. PubMed PMID: 23790674.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23790674)
15. [King GJ. Management of comminuted radial head fractures with replacement arthroplasty. Hand Clin. 2004 Nov;20(4):429-41, vi. Review. PubMed PMID: 15539098.](http://www.ncbi.nlm.nih.gov/pubmed/15539098)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15539098)
CLINICAL SITUATION FOR QUESTIONS 72 THROUGH 75
Figures 72a and 72b are the radiographs of a 54-year-old man who is experiencing shoulder pain after falling down the stairs at work.
QUESTION 69
of 100
Based on his radiograph findings, what is the best next step?
1
Sling and physical therapy
2
Narcotic analgesics
3
Axillary radiograph
4
Electromyography
- Axillary radiograph_
QUESTION 70
of 100
The patient is placed in a sling. Figure 73 is the MR image obtained 5 days later. What is the best next step?
1
Immediate closed reduction under anesthesia
2
Physical therapy
3
Nonsteroidal anti-inflammatory medications
4
Limited work duty recommendation
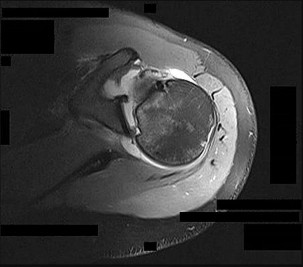
- Immediate closed reduction under anesthesia_
QUESTION 71
of 100
What is the most common long-term problem associated with the condition seen in Figure 73?
1
Neurologic injury
2
Persistent pain
3
Recurrent instability
4
Rotator cuff pathology
- Recurrent instability_
QUESTION 72
of 100
What is the best next treatment step?
1
Rotator cuff repair
2
Posterior labral repair
3
Acromioplasty
4
Anterior Bankart repair
Figures 72a and 72b provide evidence of a posterior dislocation. These are often missed, occurring in only 2% to 4% of dislocations. The anteroposterior radiographs show the “lightbulb” sign and loss of the normal overlap of the humerus on the glenoid. Axillary radiographs are the preferred means of diagnosis. The MR image clearly shows a locked posterior dislocation. This necessitates
urgent reduction under anesthesia. If the reduction is stable, nonsurgical treatment can be indicated. If unstable, the modified McLaughlin procedure, which involves transferring the lesser tuberosity into the anterior Hill-Sachs lesion, can be effective.
RECOMMENDED READINGS
16. [Hawkins RJ, Neer CS 2nd, Pianta RM, Mendoza FX. Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. 1987 Jan;69(1):9-18. PubMed PMID: 3805075. ](http://www.ncbi.nlm.nih.gov/pubmed/3805075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3805075)
17. [McLAUGHLIN HL. Posterior dislocation of the shoulder. J Bone Joint Surg Am. 1952 Jul;24 A(3):584-90. PubMed PMID: 14946209. ](http://www.ncbi.nlm.nih.gov/pubmed/14946209)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14946209)
18. [Checchia SL, Santos PD, Miyazaki AN. Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg. 1998 Jan-Feb;7(1):53-65. PubMed PMID: 9524341. ](http://www.ncbi.nlm.nih.gov/pubmed/9524341)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9524341)
QUESTION 73
of 100
A 49-year-old man has a recalcitrant history of atraumatic right elbow pain. He describes sharp stabbing pain just anterior and distal to the lateral epicondyle that is exacerbated by grabbing, lifting, and pulling activities. He denies any paresthesias. Upon examination, he expresses reproducible pain with resisted wrist extension, particularly with the elbow fully extended. He states that he was “diagnosed with tennis elbow” and has undergone 15 months of unsuccessful nonsurgical treatment including cortisone injections, physical therapy, and activity modification. After extensive consultation, he elects to proceed with surgical debridement. A histological examination of the debrided tissue likely would reveal
1
pooling of premature lymphocytes.
2
macrophage infiltration.
3
mature hypertrophic blood vessels.
4
angiofibroblastic hyperplasia.
Lateral elbow tendinopathy, commonly referred to as “tennis elbow,” remains among the most common causes of elbow pain. The term “tennis elbow” has fallen out of favor because the majority of patients with this diagnosis do not play tennis. Although its exact etiology remains elusive, a preponderance of evidence points to a repetitive microtrauma in a watershed zone near the common extensor origin with an inadequate reparative response. Although this condition initially was believed to be an inflammatory process, histological assessment of diseased tissue points to a lack of inflammatory cells. Investigators have confirmed an infiltration of immature vessels and fibroblasts, resulting in a disorganized collagen deposit referred to as “angiofibroblastic hyperplasia.”
RECOMMENDED READINGS
19. [Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999 Feb;81(2):259-78. Review. PubMed PMID: 10073590.](http://www.ncbi.nlm.nih.gov/pubmed/10073590)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10073590)
20. Jarrett CD, Sotereanos DG. Lateral and medial elbow tendinopathy. In: Weiss APC ed. _Textbook of Hand & Upper Extremity Surgery_. Chicago, IL: American Society for Surgery of the Hand; 2014:165-171.
21. [Regan W, Wold LE, Coonrad R, Morrey BF. Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med. 1992 Nov-Dec;20(6):746-9. PubMed PMID: 1280910. ](http://www.ncbi.nlm.nih.gov/pubmed/1280910)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1280910)
QUESTION 74
of 100
A 60-year-old man has elbow pain and an effusion. You send an aspirate for evaluation. Which result would lead you to diagnose inflammatory arthritis?
1
Total protein = 2.1 g/dL, glucose = 90 mg/dL, white blood cells (WBC) = 63/mm3
2
Total protein = 2.99 g/dL, glucose = 90 mg/dL, WBC = 1000/mm3
3
Total protein = 6.0 g/dL, glucose = 10 mg/dL, WBC = 100000/mm3
4
Total protein = 4.20 g/dL, glucose = 40 mg/dL, WBC = 40000/mm3
Response 4 is correct: total protein = 4.20 g/dL, glucose = 40 mg/dL, and WBC = 40000/mm3. Response 1 features normal reference value for synovial fluid. Response 2 values are seen in osteoarthritis. Response 3 values are seen in septic arthritis. There is less total protein in synovial fluid than in plasma. When inflammation occurs, total protein levels rise toward those of normal serum plasma. In osteoarthritis, for which there is no inflammatory process, synovial protein levels are normal. In inflammatory arthritis and septic arthritis, synovial fluid protein levels increase.
Synovial fluid glucose level can be used to differentiate infection from inflammation. It is normally just below fasting serum glucose levels. In both infection and inflammation, the synovial fluid total protein level is increased. In the setting of septic arthritis, the synovial fluid glucose level drops below 20 mg/dL, and the WBC count usually is above 60000/mm3.
RECOMMENDED READINGS
22. [Courtney P, Doherty M. Joint aspiration and injection and synovial fluid analysis. Best Pract Res Clin Rheumatol. 2013 Apr;27(2):137-69. doi: 10.1016/j.berh.2013.02.005. Review. PubMed PMID: 23731929.](http://www.ncbi.nlm.nih.gov/pubmed/23731929)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23731929)
23. [Farng E, Friedrich JB. Laboratory diagnosis of rheumatoid arthritis. J Hand Surg Am. 2011 May;36(5):926-7; quiz 928. doi: 10.1016/j.jhsa.2011.01.036. Epub 2011 Apr 2. Review. PubMed PMID: 21458927. ](http://www.ncbi.nlm.nih.gov/pubmed/21458927)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21458927)
QUESTION 75
of 100
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
1
The posterior bundle demonstrates the greatest change in tension from flexion to extension.
2
The posterior bundle is isometric.
3
The anterior bundle becomes tight in flexion and lax in extension.
4
The anterior and posterior bundles are isometric.
The anterior bundle is the most important portion of the complex when treating valgus instability of the elbow. The ligament originates from the anteroinferior surface of the medial epicondyle. The anterior bundle inserts on the medial border of the coronoid at the sublime tubercle.
The anterior bundle of the ulnar collateral ligament (UCL) is the primary restraint to valgus stress, and the radial head is a secondary restraint. With anterior bundle sectioning, the resultant instability is most substantial between 60 and 70 degrees and is lowest at full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the UCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the 2 functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion.
Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response 3 incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses 2 and 4 are incorrect. The posterior bundle of the MCL also demonstrates the most change in length from extension to flexion of all the elbow ligaments.
RECOMMENDED READINGS
24. [Hotchkiss RN, Weiland AJ. Valgus stability of the elbow. J Orthop Res. 1987;5(3):372-7. PubMed PMID: 3625360.](http://www.ncbi.nlm.nih.gov/pubmed/3625360)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3625360)
25. [Morrey BF, An KN. Functional anatomy of the ligaments of the elbow. Clin Orthop Relat Res. 1985 Dec;(201):84-90. PubMed PMID: 4064425.](http://www.ncbi.nlm.nih.gov/pubmed/4064425)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/4064425)
26. [Schwab GH, Bennett JB, Woods GW, Tullos HS. Biomechanics of elbow instability: the role of the medial collateral ligament. Clin Orthop Relat Res. 1980 Jan-Feb;(146):42-52. PubMed PMID: 7371268. ](http://www.ncbi.nlm.nih.gov/pubmed/7371268)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7371268)
CLINICAL SITUATION FOR QUESTIONS 79 THROUGH 81
Figure 79 is the radiograph of a 65-year-old active, right-hand-dominant woman with a 6-month history of right shoulder pain, motion loss, and progressive weakness after undergoing a hemiarthroplasty to address osteoarthritis 1 year ago. She denies recent trauma to her right shoulder and denies constitutional symptoms. Her surgical wound site is benign. She can actively forward flex to 90 degrees and abduct to 60 degrees. Passive forward flexion and abduction are 150 degrees and 90 degrees, respectively.
QUESTION 76
of 100
What is the most likely cause of her symptoms?
1
Infection
2
Rotator cuff tear
3
Implant loosening
4
Implant instability
- Rotator cuff tear_
QUESTION 77
of 100
She completes the necessary testing and wishes to proceed with revision surgery. The most appropriate surgical option in this scenario involves implant removal and
1
unconstrained total shoulder arthroplasty (TSA).
2
resection arthroplasty.
3
reverse total shoulder arthroplasty (rTSA).
4
hemiarthroplasty.
- reverse total shoulder arthroplasty (rTSA)._
QUESTION 78
of 100
Intraoperative frozen section analysis reveals 10 neutrophils per high-power field and a positive gram stain result. What is the best next step?
1
Implant removal, irrigation and debridement, and resection arthroplasty
2
Implant removal, irrigation and debridement, and rTSA
3
Implant removal, irrigation and debridement, and revision hemiarthroplasty
4
Implant removal, irrigation and debridement, and antibiotic cement spacer placement
The radiograph reveals a rotator cuff dysfunction secondary to malpositioning of the humeral stem and a nonanatomic humeral head. Glenohumeral kinematics have been altered, resulting in damage to the rotator cuff, which in turn has led to impingement with the coracoacromial arch. This single radiograph reveals excessive humeral head height, “overstuffing” of the joint, and severe narrowing of the acromiohumeral interval. Osteolysis and implant loosening are not radiographically apparent. An orthogonal view (axillary lateral) would be necessary to evaluate for shoulder instability. A CT arthrogram is the most appropriate advanced imaging test in the setting of a retained shoulder arthroplasty to evaluate the integrity of the rotator cuff. An MRI evaluation would be obfuscated by artifact. Three-phase and indium-tagged white blood cell scans may be appropriate in the setting of an occult infection evaluation, but not as a test to evaluate rotator cuff injury.
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
1. [Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. ](http://www.ncbi.nlm.nih.gov/pubmed/17015609)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17015609)
2. [Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. ](http://www.ncbi.nlm.nih.gov/pubmed/25704211)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25704211)
3. [Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. ](http://www.ncbi.nlm.nih.gov/pubmed/25595360)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25595360)
4. [Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. ](http://www.ncbi.nlm.nih.gov/pubmed/21872496)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21872496)
5. [Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. ](http://www.ncbi.nlm.nih.gov/pubmed/15726070)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15726070)
6. [Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.](http://www.ncbi.nlm.nih.gov/pubmed/1583043)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1583043)
7. [Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. ](http://www.ncbi.nlm.nih.gov/pubmed/24647499)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24647499)
QUESTION 79
of 100
A 78-year-old woman falls from standing, resulting in a displaced proximal humerus fracture with a dysvascular head. Treatment of the fracture with arthroplasty is indicated. Which statement best describes the outcome differences between hemiarthroplasty and reverse total shoulder arthroplasty (rTSA)?
1
Hemiarthroplasty is more likely to yield good internal rotation.
2
rTSA is associated with more implant-related complications.
3
rTSA is likely to yield better forward elevation.
4
Infection rates are higher for rTSA in this setting.
The major difficulty with hemiarthroplasty for fractures is getting the tuberosities to reliably heal. Failure of the tuberosities to heal results in loss of compressive force of the rotator cuff and pseudoparalysis (loss of the ability to raise the arm because of rotator cuff dysfunction). Complication rates do not appear to be worse for those who undergo rTSA, and internal rotation is not substantially different. Two systematic reviews demonstrate that patients treated with rTSA
for their proximal humerus fractures have better forward elevation, likely because tuberosity healing is not required for elevation when using a deltoid-dependent implant.
RECOMMENDED READINGS
8. [Mata-Fink A, Meinke M, Jones C, Kim B, Bell JE. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J Shoulder Elbow Surg. 2013 Dec;22(12):1737-48. doi: 10.1016/j.jse.2013.08.021. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24246529)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24246529)
9. [Ferrel JR, Trinh TQ, Fischer RA. Reverse total shoulder arthroplasty versus hemiarthroplasty for proximal humeral fractures: a systematic review. J Orthop Trauma. 2015 Jan;29(1):60-8. doi: 10.1097/BOT.0000000000000224. PubMed PMID: 25186842.](http://www.ncbi.nlm.nih.gov/pubmed/25186842)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25186842)
QUESTION 80
of 100
When using antibiotic-laden polymethylmethacrylate (PMMA) to treat osteomyelitis, vancomycin and tobramycin are heat stable and have not produced systemic toxicity at various levels. Which dose is closest to the highest recommended concentration for each drug?
1
2 grams each per 40 mg PMMA
2
3.6 grams each per 40 mg PMMA
3
10 grams each per 40 mg PMMA
4
20 grams each per 40 mg PMMA
Vancomycin and tobramycin do not produce systemic toxicity in doses as high as 10.5 grams of vancomycin and 12.5 grams of tobramycin per 40 mg of PMMA.
RECOMMENDED READINGS
10. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
11. [Springer BD, Lee GC, Osmon D, Haidukewych GJ, Hanssen AD, Jacofsky DJ. Systemic safety of high-dose antibiotic-loaded cement spacers after resection of an infected total knee arthroplasty. Clin Orthop Relat Res. 2004 Oct;(427):47-51. PubMed PMID: 15552135. ](http://www.ncbi.nlm.nih.gov/pubmed/15552135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15552135)
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figure 84 is the noncontrast MR image obtained at 2 weeks postinjury for a 52-year-old man who was injured after falling from a ladder. His arm is caught in an abducted, externally rotated
position. There is no sense of dislocation. Initial radiograph findings are normal. The radiologic review reads “Probable superior labral anterior to posterior (SLAP) tear.”
QUESTION 81
of 100
What is the most appropriate next step?
1
Arthroscopic labral repair
2
Repeat MR imaging with contrast
3
Examination under anesthesia
4
Nonsteroidal anti-inflammatory drugs and physical therapy
- Nonsteroidal anti-inflammatory drugs and physical therapy_
QUESTION 82
of 100
Diagnosis of SLAP tears is difficult because
1
MR imaging is not performed without contrast.
2
examination findings are unreliable.
3
surgeons tend to agree on the pathology at arthroscopy.
4
SLAP lesions are uncommon in older individuals.
- examination findings are unreliable._
QUESTION 83
of 100
In this age group, symptomatic SLAP lesions are best treated with
1
biceps tenodesis.
2
open labral repair.
3
arthroscopic labral repair.
4
repair with bioabsorbable tacks.
SLAP lesions are difficult to diagnose with MR imaging. Radiologic review generates a high number of false-positive reports. For this reason, initial nonsurgical evaluation with MR imaging that suggests a SLAP lesion is appropriate. Most authors contend that SLAP repair should be performed in no more than 3% of cases, even in a tertiary care shoulder practice. An examination, MRI scanning with or without contrast, and surgeon agreement on visual pathology at surgery are all highly variable. Many older patients will have increased signal in the labrum as a normal variant. Several studies suggest that SLAP lesions in older people may be better addressed with biceps tenodesis than labral repair.
RECOMMENDED READINGS
12. [Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009 May;37(5):929-36.Epub 2009 Feb 19. PubMed PMID: 19229046. ](http://www.ncbi.nlm.nih.gov/pubmed/19229046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19229046)
13. [Burns JP, Bahk M, Snyder SJ. Superior labral tears: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2011 Mar;20(2 Suppl):S2-8. doi: 10.1016/j.jse.2010.11.013. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/21281918)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21281918)
14. Gobezie R, Zurakowski D, Lavery K, Millett PJ, Cole BJ, Warner JJ. Analysis of interobserver and intraobserver variability in the diagnosis and treatment of SLAP tears using the Snyder classification. Am J Sports Med. 2008 Jul;36(7):1373-9. doi: 10.1177/0363546508314795. Epub 2008 Mar 19.
[PubMed PMID: 18354142. ](http://www.ncbi.nlm.nih.gov/pubmed/18354142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18354142)
15. [Katz LM, Hsu S, Miller SL, Richmond JC, Khetia E, Kohli N, Curtis AS. Poor outcomes after SLAP repair: descriptive analysis and prognosis. Arthroscopy. 2009 Aug;25(8):849-55. doi: 10.1016/j.arthro.2009.02.022. Erratum in: Arthroscopy. 2009 Nov;25(11):1361. Ketia, Eric [corrected to Khetia, Eric]. PubMed PMID: 19664504. ](http://www.ncbi.nlm.nih.gov/pubmed/19664504)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19664504)
16. [Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery. Arthroscopy. 2006 Jun;22(6):615-9.](http://www.ncbi.nlm.nih.gov/pubmed/16762699)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16762699)
17. [Weber SC, Martin DF, Seiler JG 3rd, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012 Jul;40(7):1538-43. doi: 10.1177/ 0363546512447785. Epub 2012 May 24. PubMed PMID: 22628153.](http://www.ncbi.nlm.nih.gov/pubmed/22628153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22628153)
QUESTION 84
of 100
A 65-year-old man has a 6-month history of diffuse left shoulder pain. He does not recall a previous shoulder or neck injury. Pain is worse with use of his shoulder and when he rolls over on the affected side at night. An examination reveals isolated atrophy of the infraspinatus without scapular winging. He has good strength in internal rotation and isolated supraspinatus testing.
There is weakness with resisted external rotation. Radiographs reveal degenerative change at the acromioclavicular joint. MR imaging of the left shoulder most likely would reveal
1
a suprascapular notch cyst.
2
a degenerative labral tear and spinoglenoid notch cyst.
3
a medial subluxation of the biceps tendon.
4
supraspinatus and infraspinatus tears retracted to the level of the glenoid.
Isolated infraspinatus atrophy and weakness is most commonly the result of compression of the suprascapular nerve at the spinoglenoid notch. This condition often is found in the setting of a labral tear and an associated spinoglenoid notch cyst. Compression of the supraspinatus nerve at the suprascapular notch would result in weakness of both the supraspinatus and infraspinatus muscles. Medial subluxation of the biceps is often seen with subscapularis tearing, and weakness with internal rotation can be expected. A massive rotator cuff tear with retraction of the supraspinatus and infraspinatus would likely result in weakness and atrophy of both the supraspinatus and infraspinatus.
RECOMMENDED READINGS
18. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677. ](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
19. [Mall NA, Hammond JE, Lenart BA, Enriquez DJ, Twigg SL, Nicholson GP. Suprascapular nerve entrapment isolated to the spinoglenoid notch: surgical technique and results of open decompression. J Shoulder Elbow Surg. 2013 Nov;22(11):e1-8. doi: 10.1016/j.jse.2013.03.009. Epub 2013 May 8. PubMed PMID: 23664748.](http://www.ncbi.nlm.nih.gov/pubmed/23664748)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23664748)
QUESTION 85
of 100
When using antibiotic-laden polymethylmethacrylate (PMMA) beads, the elution characteristics produce which profile?
1
Rapid release during the initial 24 hours, followed by a period of rapid decrease, transitioning to a more steady decrease to very low levels by 5 weeks
2
Rapid release during the initial 24 hours, followed by a period of rapid decrease, transitioning to a more steady decrease to very low levels by 10 weeks
3
Rapid release during the initial 24 hours, followed by a period of gradual decrease, transitioning to a more steady decrease to very low levels by 1 week
4
Rapid release during the initial 72 hours, followed by a period of gradual decrease, transitioning to a more rapid decrease to very low levels by 7 weeks
The elution of antibiotics from polymethylmethacrylate beads is characterized by a rapid release during the initial 24 hours, followed by a period during which the release rate quickly decreases and then reaches a steadily declining rate release. Elution can produce very low levels of release by week 5.
RECOMMENDED READINGS
20. [Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015 Aug;46(8):1447-56. doi: 10.1016/j.injury.2015.05.008. Epub 2015 May 14. Review. PubMed PMID: 26007616. ](http://www.ncbi.nlm.nih.gov/pubmed/26007616)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26007616)
21. [Anagnostakos K, Wilmes P, Schmitt E, Kelm J. Elution of gentamicin and vancomycin from polymethylmethacrylate beads and hip spacers in vivo. Acta Orthop. 2009 Apr;80(2):193-7. doi: 10.3109/17453670902884700. PubMed PMID: 19404802. ](http://www.ncbi.nlm.nih.gov/pubmed/19404802)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19404802)
22. [Penner MJ, Duncan CP, Masri BA. The in vitro elution characteristics of antibiotic-loaded CMW and Palacos-R bone cements. J Arthroplasty. 1999 Feb;14(2):209-14. ](http://www.ncbi.nlm.nih.gov/pubmed/10065729)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10065729)
RESPONSES FOR QUESTIONS 89 THROUGH 96
1. Humeral head resurfacing/shoulder hemiarthroplasty
2. Anatomic total shoulder arthroplasty (TSA)
3. Reverse total shoulder arthroplasty (rTSA)
4. Rotator cuff repair
5. Open reduction and internal fixation (ORIF)
Which intervention listed above is most appropriate to address each scenario described below? When chronic conditions are described, nonsurgical interventions such as physical therapy, anti-inflammatory medications, and corticosteroid injections have been exhausted.
QUESTION 86
of 100
A 62-year-old man experiences pain in his right shoulder (Figures 89a through 89c).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)


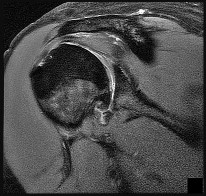
- Anatomic total shoulder arthroplasty (TSA)_
QUESTION 87
of 100
A 58-year-old man has right shoulder pain. An examination reveals full range of motion in all planes but 4/5 forward elevation strength (Figures 90a and 90b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Rotator cuff repair_
QUESTION 88
of 100
A 78-year-old woman with an acute shoulder injury (Figures 91a and 91b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Reverse total shoulder arthroplasty (rTSA)_
QUESTION 89
of 100
A 55-year-old man experiences right shoulder pain 2 years after undergoing hemiarthroplasty for osteoarthritis. His laboratory values indicate normal C-reactive protein, erythrocyte sedimentation rate, and white blood cell count levels. He undergoes a shoulder aspiration and culture and an arthroscopic biopsy; all findings are negative. Belly-press and bear-hug test results are normal (Figures 92a and 92b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)

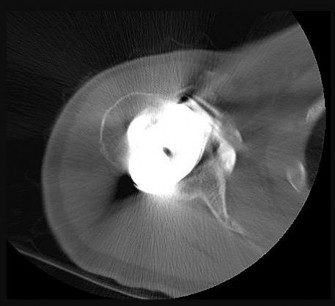
- Anatomic total shoulder arthroplasty (TSA)_
QUESTION 90
of 100
A 72-year-old woman experiences left shoulder pain and dysfunction. An examination demonstrates 45 degrees of active forward elevation with 2/5 strength. The deltoid fires in the anterior, middle, and posterior heads (Figure 93).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Reverse total shoulder arthroplasty (rTSA)_
QUESTION 91
of 100
A 40-year-old male laborer with an acute left shoulder injury (Figures 94a and 94b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Open reduction and internal fixation (ORIF)_
QUESTION 92
of 100
A 71-year-old woman has had 2 previous rotator cuff repairs to her right shoulder. An examination reveals 70 degrees of active forward elevation and 3/5 strength. An infection workup is negative (Figures 95a through 95c).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Reverse total shoulder arthroplasty (rTSA)_
QUESTION 93
of 100
A 35-year-old active woman with rheumatoid arthritis experiences right shoulder pain following an extended course of corticosteroids (Figures 96a and 96b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
The indication for anatomic TSA is end-stage glenohumeral arthritis with an intact rotator cuff. For the 62-year-old man, his radiographs reveal osteoarthritis, and his MR image shows an intact rotator cuff. Although humeral head replacement has historically been employed for this disorder, pain relief is not as reliable as with TSA, and the revision rate is higher. rTSA is generally reserved for patients with a nonfunctional rotator cuff.
For this 58-year-old patient with a full-thickness rotator cuff tear, preserved motion, and weakness in forward elevation, a rotator cuff repair is the most appropriate treatment. In the absence of degenerative changes, shoulder hemiarthroplasty or anatomic TSA is not indicated. Although indications for rTSA continue to evolve, well-compensated range of motion and a medium-sized rotator cuff tear in a younger patient are not among them.
rTSA is an emerging treatment for comminuted proximal humerus fractures in elderly patients. Although hemiarthroplasty has been a traditional treatment, current evidence suggests rTSA more reliably restores range of motion, and this 78-year-old patient's CT scan shows a small and comminuted greater tuberosity fragment that is unlikely to heal. ORIF is another option, but the CT scan also shows a small humeral head fragment that suggests osteopenia, making fixation more tenuous and likely less reliable.
A common problem associated with hemiarthroplasty for glenohumeral osteoarthritis is symptomatic glenoid degeneration that necessitates revision. This 55-year-old patient’s images reveal this is the case, although his infection workup is negative. His examination findings suggest an intact subscapularis repair. With a functioning rotator cuff and symptomatic glenoid arthritis, a conversion to anatomic TSA is indicated. In the absence of a functioning rotator cuff in an older patient, an rTSA is a better option.
This 72-year-old patient has classic symptoms and radiographs of cuff tear arthropathy. For patients with massive rotator cuff tear and glenohumeral arthritis, neither anatomic TSA nor rotator cuff repair is indicated. Hemiarthroplasty has historically been indicated for cuff tear arthropathy, but rTSA outcomes for this disorder have been superior and are now the preferred option.
Comminuted proximal humerus fractures in young, active patients are treated primarily with ORIF. The absence of glenohumeral arthritis removes anatomic TSA as a possibility, and concerns about implant longevity in younger, active patients such as this 40-year-old laborer contraindicate rTSA. Hemiarthroplasty is still employed in 3- and 4-part fractures but is generally reserved for subacute presentations or dislocations in which the humeral head is dysvascular and unlikely to survive. In this acute setting, a fixation procedure is preferred.
The 71-year-old patient who has had 2 failed rotator cuff repairs has an MR image that reveals another recurrent tear that is retracted to the glenoid. Her examination findings reveal classic signs
of a decompensated rotator cuff tear with pseudoparalysis and weakness in forward elevation. Although infection is a concern in the setting of multiply failed rotator cuff repair, the workup is negative in this scenario. Because this patient has a dysfunctional rotator cuff and has failed previous attempts at repair, a conversion to rTSA is the better option. In the absence of degenerative changes, hemiarthroplasty and anatomic TSA are not indicated.
The indications for hemiarthroplasty continue to narrow, but it is still a consideration for young patients with unipolar shoulder degeneration. In this 35-year-old patient, her MR image shows avascular necrosis in the humeral head, and her arthroscopy suggests arthritic change only on the humeral side with an uncompromised glenoid. To best treat young and active patients, a hemiarthroplasty that articulates with healthy glenoid cartilage can provide good pain relief and functional outcomes. Anatomic TSA is also reasonable but not an optimal option considering the normal glenoid condition. rTSA is not a consideration when a young patient’s MR images reveal an intact rotator cuff.
RECOMMENDED READINGS
1. [Torchia ME, Cofield RH, Settergren CR. Total shoulder arthroplasty with the Neer prosthesis: longterm results. J Shoulder Elbow Surg. 1997 Nov-Dec;6(6):495-505. PubMed PMID: 9437598. ](http://www.ncbi.nlm.nih.gov/pubmed/9437598)[View](http://www.ncbi.nlm.nih.gov/pubmed/9437598)[ ](http://www.ncbi.nlm.nih.gov/pubmed/9437598)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9437598)
2. [Chalmers PN, Slikker W 3rd, Mall NA, Gupta AK, Rahman Z, Enriquez D, Nicholson GP. Reverse total shoulder arthroplasty for acute proximal humeral fracture: comparison to open reduction-internal fixation and hemiarthroplasty. J Shoulder Elbow Surg. 2014 Feb;23(2):197-204. doi: 10.1016/j.jse.2013.07.044. Epub 2013 Sep 27. PubMed PMID: 24076000. ](http://www.ncbi.nlm.nih.gov/pubmed/24076000)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24076000)
3. [Groh GI, Wirth MA. Results of revision from hemiarthroplasty to total shoulder arthroplasty utilizing modular component systems. J Shoulder Elbow Surg. 2011 Jul;20(5):778-82. doi: 10.1016/j.jse.2010.09.014. Epub 2011 Jan 13. PubMed PMID: 21232989. ](http://www.ncbi.nlm.nih.gov/pubmed/21232989)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21232989)
4. [Orfaly RM, Rockwood CA Jr, Esenyel CZ, Wirth MA. Shoulder arthroplasty in cases with avascular necrosis of the humeral head. J Shoulder Elbow Surg. 2007 May-Jun;16(3 Suppl):S27-32. Epub 2006 Nov 16. PubMed PMID: 17113317. ](http://www.ncbi.nlm.nih.gov/pubmed/17113317)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17113317)
5. [Sershon RA, Van Thiel GS, Lin EC, McGill KC, Cole BJ, Verma NN, Romeo AA, Nicholson GP. Clinical outcomes of reverse total shoulder arthroplasty in patients aged younger than 60 years. J Shoulder Elbow Surg. 2014 Mar;23(3):395-400. doi: 10.1016/j.jse.2013.07.047. Epub 2013 Oct 12. PubMed PMID: 24129052. ](http://www.ncbi.nlm.nih.gov/pubmed/24129052)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24129052)
QUESTION 94
of 100
A 78-year-old woman falls and sustains a displaced proximal humerus fracture with a dysvascular humeral head. Which best describes her likely outcome if she chooses treatment with total shoulder arthroplasty (TSA)?
1
Hemiarthroplasty is associated with lower infection rates than reverse total shoulder arthroplasty (rTSA)
2
rTSA provides better internal rotation than hemiarthroplasty
3
rTSA is associated with lower revision surgery rates than hemiarthroplasty
4
Periprosthetic fracture rates are higher for hemiarthroplasty than for rTSA
In the study by Sebastiá-Forcada and associates, some patients treated with hemiarthroplasty developed proximal migration resulting in conversion to rTSA. Infection rates between the groups were similar, internal rotation was not affected (external rotation was better in patients who underwent hemiarthroplasty), and periprosthetic fractures were not seen. Similar outcomes have been described by other authors.
RECOMMENDED READINGS
6. [Sebastiá-Forcada E, Cebrián-Gómez R, Lizaur-Utrilla A, Gil-Guillén V. Reverse shoulder arthroplasty versus hemiarthroplasty for acute proximal humeral fractures. A blinded, randomized, controlled, prospective study. J Shoulder Elbow Surg. 2014 Oct;23(10):1419-26. doi: 10.1016/j.jse.2014.06.035. Epub 2014 Jul 30. PubMed PMID: 25086490. ](http://www.ncbi.nlm.nih.gov/pubmed/25086490)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25086490)
7. [Cuff DJ, Pupello DR. Comparison of hemiarthroplasty and reverse shoulder arthroplasty for the treatment of proximal humeral fractures in elderly patients. J Bone Joint Surg Am. 2013 Nov 20;95(22):2050-5. doi: 10.2106/JBJS.L.01637. PubMed PMID: 24257664. ](http://www.ncbi.nlm.nih.gov/pubmed/24257664)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24257664)
QUESTION 95
of 100
Three months ago, a 33-year-old right-hand-dominant man fell on his right shoulder. He also sustained an anterior shoulder dislocation while playing football 12 years ago that was treated with an arthroscopic Bankart repair. He reports he did well after surgery until 5 years ago, at which time he sustained a right anterior shoulder dislocation and underwent a revision arthroscopic Bankart repair and capsular shift. After rehabilitating his shoulder, he states that he was doing well until 3 months ago when he fell. He feels that the shoulder is “sliding out” when he puts his arm in an abducted and externally rotated position. The symptoms remain unchanged despite participating in 2 months of physical therapy. Apprehension test findings are positive, and his symptoms improve with Jobe relocation testing. He has full range of motion without weakness. A CT arthrogram reveals 20% loss of bone of the anterior inferior glenoid but no Bankart tear. There is a nonengaging Hill-Sachs lesion. What is the most appropriate treatment?
1
Revision arthroscopic Bankart repair with remplissage
2
Open Bankart repair with capsular shift
3
Transfer of the coracoid to the anterior glenoid
4
Injection of platelet-rich plasma
The history and examination are consistent with recurrent anterior shoulder instability. Although this patient does not have an identifiable Bankart tear on CT arthrogram and bone loss is 20% of the glenoid, a Latarjet with transfer of the coracoid to the anterior glenoid would most likely provide long-term stability to his shoulder. A remplissage with tenodesis of the infraspinatus to the Hill-Sachs lesion can be helpful if the symptoms are related to engagement of the Hill-Sachs lesion. An open capsular shift and Bankart with remplissage are less likely to be helpful in the setting of significant bone loss.
RECOMMENDED READINGS
8. Streubel PN, Krych AJ, Simone JP, Dahm DL, Sperling JW, Steinmann SP, O'Driscoll SW, Sanchez-Sotelo J. Anterior glenohumeral instability: a pathology-based surgical treatment strategy. J Am Acad Orthop Surg. 2014 May;22(5):283-94. doi: 10.5435/JAAOS-22-05-283. Review. PubMed PMID:
[24788444.](http://www.ncbi.nlm.nih.gov/pubmed/24788444)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24788444)
9. [Bhatia S, Frank RM, Ghodadra NS, Hsu AR, Romeo AA, Bach BR Jr, Boileau P, Provencher MT. The outcomes and surgical techniques of the latarjet procedure. Arthroscopy. 2014 Feb;30(2):227-35. doi: 10.1016/j.arthro.2013.10.013. Review. PubMed PMID: 24485116. ](http://www.ncbi.nlm.nih.gov/pubmed/24485116)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24485116)
QUESTION 96
of 100
A 28-year-old man is subjected to a blast and sustains the fragmentary injury shown in the plain radiographs in Figures 99a and 99b. He lacks distal radial nerve function. His wounds have associated soft-tissue damage, although they do not appear grossly contaminated, and tissue loss would not prevent either primary or delayed closure. Which surgical plan is associated with the lowest rate of revision surgery and complications?
1
Open reduction and intramedullary fixation
2
Primary closure and coaptation splinting
3
Nerve exploration and intramedullary fixation
4
Nerve exploration and internal fixation
Two indications for nerve exploration are open fractures and high-velocity injuries. Nerve exploration under these circumstances can improve outcomes. Intramedullary fixation is associated with higher revision surgery and complication rates vs open reduction and internal fixation. Nonsurgical treatment in the setting of a high-energy injury is associated with a higher nonunion rate.
RECOMMENDED READINGS
10. [Heineman DJ, Poolman RW, Nork SE, Ponsen KJ, Bhandari M. Plate fixation or intramedullary fixation of humeral shaft fractures. Acta Orthop. 2010 Apr;81(2):216-23. doi: 10.3109/17453671003635884. Review. Erratum in: Acta Orthop. 2010 Oct;81(5):647. PubMed PMID: 20170424. ](http://www.ncbi.nlm.nih.gov/pubmed/20170424)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20170424)
11. [Bishop J, Ring D. Management of radial nerve palsy associated with humeral shaft fracture: a decision analysis model. J Hand Surg Am. 2009 Jul-Aug;34(6):991-6.e1. doi: 10.1016/j.jhsa.2008.12.029. Epub 2009 Apr 10. PubMed PMID: 19361935. ](http://www.ncbi.nlm.nih.gov/pubmed/19361935)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19361935)
QUESTION 97
of 100
A 63-year-old right-hand-dominant woman has a nontraumatic history of gradually progressive right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and has difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
1
Anterior portion of the supraspinatus tendon adjacent to the biceps tendon
2
15 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
3
Superior portion of the subscapularis tendon
4
30 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiating site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and
length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
RECOMMENDED READINGS
12. [Kim HM, Dahiya N, Teefey SA, Middleton WD, Stobbs G, Steger-May K, Yamaguchi K, Keener JD. Location and initiation of degenerative rotator cuff tears: an analysis of three hundred and sixty shoulders. J Bone Joint Surg Am. 2010 May;92(5):1088-96. doi: 10.2106/JBJS.I.00686. PubMed PMID: 20439653. ](http://www.ncbi.nlm.nih.gov/pubmed/20439653)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20439653)
13. [Burkhart SS, Esch JC, Jolson RS. The rotator crescent and rotator cable: an anatomic description of the shoulder's "suspension bridge". Arthroscopy. 1993;9(6):611-6. Erratum in: Arthroscopy 1994 Apr;10(2):239. PubMed PMID: 8305096. ](http://www.ncbi.nlm.nih.gov/pubmed/8305096)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8305096)
14. [Jarrett CD, Schmidt CC. Arthroscopic treatment of rotator cuff disease. J Hand Surg Am. 2011 Sep;36(9):1541-52; quiz 1552. doi: 10.1016/j.jhsa.2011.06.026. Epub 2011 Aug 6. Review. PubMed PMID: 21821368. ](http://www.ncbi.nlm.nih.gov/pubmed/21821368)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21821368)
15. [Mall NA, Kim HM, Keener JD, Steger-May K, Teefey SA, Middleton WD, Stobbs G, Yamaguchi K. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. J Bone Joint Surg Am. 2010 Nov 17;92(16):2623-33. doi: 10.2106/JBJS.I.00506. PubMed PMID: 21084574. ](http://www.ncbi.nlm.nih.gov/pubmed/21084574)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21084574)
_This is the last question of the exam._
_GOOD LUCK_