Orthopedic Pediatric Review | Dr Hutaif Pediatric Ortho -...
Updated: Feb 2026
40 Views
Key Medical Takeaway
Your ultimate guide to ORTHOPEDIC MCQS ONLINE PEDIATRIC 016 starts here. A headneck junction offset refers to any deviation from optimal anatomical alignment at the craniocervical junction, where the skull meets the upper spine. In pediatric orthopaedics, understanding this offset is vital for assessing structural integrity, potential neurological implications, and risk factors for conditions or injuries, including those related to trauma and athletic activity.
Score: 0%
ORTHOPEDIC MCQS ONLINE PEDIATRIC 016
QUESTION 1
of 100
Second-impact syndrome following a concussion
1
poses minimal concern for morbidity or mortality.
2
is less common in adolescents than in adults.
3
is related to a disruption of cerebral autoregulation.
4
refers to a second head injury after the athlete has been medically cleared to return to play.
According to several consensus statements, no child or adolescent athlete with a concussion should be allowed to return to play on the same day, regardless of severity. Second-impact syndrome refers to a second traumatic head injury that occurs while an athlete is still experiencing symptoms from the first injury. Young athletes are particularly vulnerable to second-impact syndrome. The mechanism by which this syndrome occurs likely is disruption of cerebral autoregulation, which may result in cerebral vascular congestion, diffuse brain swelling, and death.
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6a
Figure 6b
Figure 6c
RESPONSES FOR QUESTIONS 2 THROUGH 6
1. Curettage and/or grafting
2. Radiofrequency ablation
3. Intravenous (IV) antibiotics
4. Incision, drainage, and IV antibiotics
5. Neoadjuvant chemotherapy followed by surgical reconstruction
6. Observation alone
For each clinical vignette seen in the figures, select the best initial treatment from the list above.
QUESTION 2
of 100
Figure 2
1
Curettage and/or grafting
2
Radiofrequency ablation
3
Intravenous (IV) antibiotics
4
Incision, drainage, and IV antibiotics
5
Neoadjuvant chemotherapy followed by surgical reconstruction
- Observation alone Question 3 of 100
Figure 3
1. Curettage and/or grafting
2. Radiofrequency ablation
3. Intravenous (IV) antibiotics
4. Incision, drainage, and IV antibiotics
5. Neoadjuvant chemotherapy followed by surgical reconstruction
6. Observation alone
PREFERRED RESPONSE: 6- Observation alone
QUESTION 3
of 100
Figure 4
1
Curettage and/or grafting
2
Radiofrequency ablation
3
Intravenous (IV) antibiotics
4
Incision, drainage, and IV antibiotics
5
Neoadjuvant chemotherapy followed by surgical reconstruction
- Radiofrequency ablation
QUESTION 4
of 100
Figure 5
1
Curettage and/or grafting
2
Radiofrequency ablation
3
Intravenous (IV) antibiotics
4
Incision, drainage, and IV antibiotics
5
Neoadjuvant chemotherapy followed by surgical reconstruction
- Intravenous (IV) antibiotics
QUESTION 5
of 100
Figure 6a through 6c
1
Curettage and/or grafting
2
Radiofrequency ablation
3
Intravenous (IV) antibiotics
4
Incision, drainage, and IV antibiotics
5
Neoadjuvant chemotherapy followed by surgical reconstruction
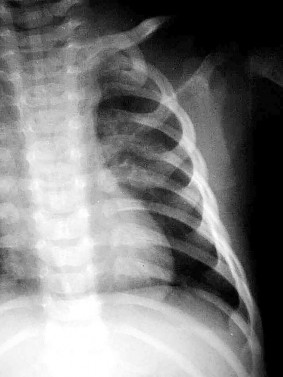
Figure 2 depicts a typical unicameral bone cyst with a pathologic fracture. The decision to treat this lesion should be based on the amount of cortical thinning. If these lesions involve a pathologic fracture, many surgeons will treat them nonsurgically to see if the fracture stimulates healing of the cyst. If the cyst wall remains thin or the patient is symptomatic, then treatment is directed at decreasing cyst volume, increasing cortical thickness, and eliminating symptoms. This can be accomplished by curettage and grafting, injection with autogenous bone marrow, or grafting with 1 of the many available bone void fillers. In some cases, internal fixation may be required. This typically is accomplished with flexible intramedullary nails.
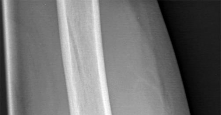
Figure 3 shows a typical nonossifying fibroma. These benign lesions are usually incidental findings on a radiograph and often resolve in adulthood. Treatment usually is not required, and these lesions typically do not produce symptoms.
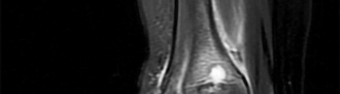
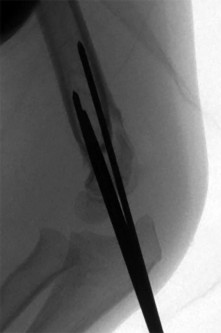
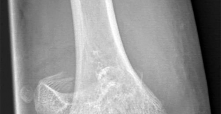
Figure 4 shows an osteoid osteoma of the femoral neck. This is characterized by a central radiolucent nidus surrounded by reactive bone with increased radiodensity. These lesions are painful because of the large amount of prostaglandin they secrete. They temporarily respond to oral anti-inflammatory drugs. Treatment is directed at eliminating the nidus and can be done through curettage, but radiofrequency ablation, which allows for a minimally invasive approach, is often used today.
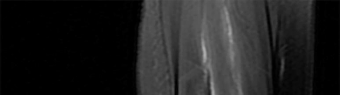
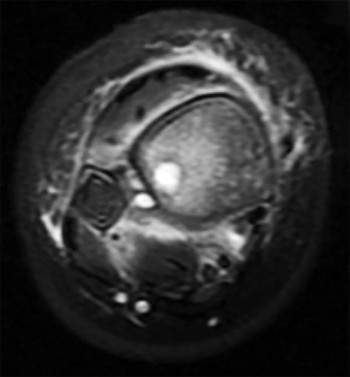
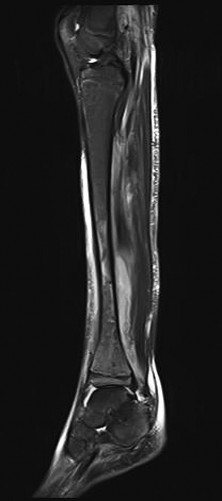
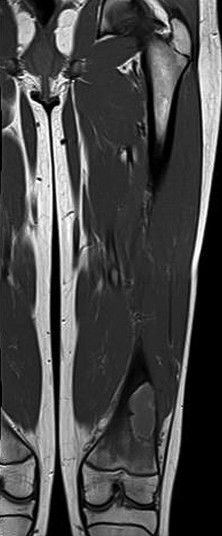
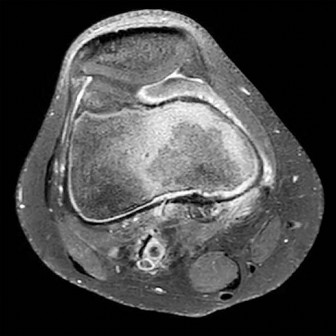
Figure 5 shows diskitis with vertebral osteomyelitis. The disease is characterized by fever and back pain. Movement is extremely uncomfortable for these children, and they may adopt unusual postures to alleviate pain. The MRI shows involvement of 1 vertebrae and an adjacent disk. Left untreated, this condition often spreads to involve multiple vertebrae and also can cause an epidural abscess. Treatment during the early stages is IV antibiotics. Many orthopaedic surgeons also use bracing to prevent late vertebral collapse.
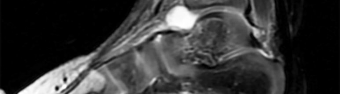
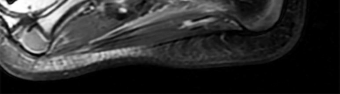
Figures 6a through 6c show septic arthritis of the ankle with metaphyseal osteomyelitis. The recommended treatment is incision and drainage followed by IV antibiotics. MRI may be considered before surgery to assess for an associated osteomyelitis or abscess that may also necessitate surgical debridement. Increasingly, these scenarios are managed with a rapid transition to oral antibiotics.
QUESTION 6
of 100
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
1
patients younger than age 6.5.
2
patients who bear weight immediately after surgery.
3
patients weighing more than 50 kg (110 pounds).
4
patients with grade 1 open transverse midshaft fractures.
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.
Video 8a
Video 8b
QUESTION 7
of 100
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR
imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
1
He has osteomyelitis with a significant subperiosteal abscess that will necessitate open drainage in the operating room.
2
He has osteomyelitis without any abscess, so continued IV antibiotics and clinical observation are recommended.
3
He has a muscle abscess that would best be treated by percutaneous drainage in interventional radiology.
4
The MR image shows cellulitis with some adjacent myositis, so a short course of IV antibiotics followed by 2 to 3 weeks of appropriate oral antibiotics is recommended.
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.
Figure 9a
Figure 9b
---|---
CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
QUESTION 8
of 100
What is the most likely mechanism of injury?
1
Fall directly onto the elbow
2
Fall onto an outstretched elbow and hand
3
The direct impact of the elbow against the bars upon falling
4
Entrapment of the upper extremity under the trunk
- Fall onto an outstretched elbow and hand
QUESTION 9
of 100
Treatment should address predictable
1
instability of the fracture.
2
absence of the radial pulse.
3
inability to oppose the thumb and index finger.
4
rigidity of the forearm muscles.
- instability of the fracture.
QUESTION 10
of 100
The most mechanically stable fixation pattern for this fracture involves
1
lateral pins that diverge at the fracture site.
2
lateral pins that converge at the fracture site.
3
lateral and medial pins.
4
parallel lateral pins.
- lateral and medial pins.
QUESTION 11
of 100
After reduction and pinning, the radial pulse is absent by both palpation and Doppler.
Capillary refill in the fingers appears normal. What is the most likely explanation?
1
Laceration of the brachial artery during reduction
2
Compression of the brachial artery by a pin
3
Abnormal arterial supply
4
Spasm in the brachial artery
This is a classic extension-type supracondylar elbow fracture typically caused by a fall on an outstretched hand. The medial comminution of this fracture renders it predictably unstable and susceptible to varus malunion. Extra attention with fixation is required. In general, use of lateral-entry pins alone is effective for most supracondylar humeral fractures. The best technique for fixation with lateral-entry pins only involves maximization of pin separation at the fracture site, engaging sufficient bone in both the proximal segment and the distal fragment and using more than 2 lateral entry pins (if needed) for stability. In the presence of medial comminution, medial fixation also may be necessary.
Brachial artery spasm is the usual cause of absence of radial pulse if capillary refill is normal. Close postsurgical monitoring is warranted after reduction and pinning.
QUESTION 12
of 100
What is the most appropriate way to communicate instructions to a family when there is a language barrier?
1
Use a translation program to print out instructions in the family’s native language and ask if they have questions
2
Have the patient translate the instructions if his or her English skills are adequate
3
Use a member of the hospital’s nonmedical staff to translate
4
Use a professional medical interpreter
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.
Figure 14a
Figure 14b
Figure 14c
Figure 14d
Figure 14e
Figure 15a
Figure 15b
Figure 15c
Figure 15d
---|---|---
Figure 16a
Figure 16b
RESPONSES FOR QUESTIONS 14 THROUGH 16
1. Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2. Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3. Aspiration, cultures, Lyme serology, and oral amoxicillin
4. Biopsy, culture, curettage, bone graft, and possible internal fixation
5. Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
QUESTION 13
of 100
Figures 14a through 14e are the clinical photograph, radiographs, and MR images of a 13-year-old boy with a 10-day history of a painful right ankle following a slide into second base that resulted in skin abrasions. He cannot bear weight and he has severe pain with any ankle motion. His primary care physician treated him 2 days ago and 7 days ago with intravenous ceftriaxone, but there has been no improvement. His temperature is 38.8°C, his white blood cell count (WBC) is 21000 /µL (reference range [rr], 4500-11000 /µL), C-reactive protein (CRP) is 6.8 mg/L (rr, 0.08-3.1 mg/L), and erythrocyte sedimentation rate (ESR) is 95 mm/h (rr, 0-20 mm/h).
1
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3
Aspiration, cultures, Lyme serology, and oral amoxicillin
4
Biopsy, culture, curettage, bone graft, and possible internal fixation
5
Physical therapy, ibuprofen, and an antinuclear antibody test
- Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
QUESTION 14
of 100
Figures 15a through 15d are the clinical photographs and radiographs of a 7-year-old girl with a markedly swollen left knee, a limp (but she can bear weight), and a rash on her inner left thigh. Her temperature is 38.1°C, WBC is 14000 /µL (rr, 4500-11000 /µL), CRP is 2.1 mg/L (rr, 0.08-3.1 mg/L), and ESR is 34 mm/h (rr, 0-20 mm/h). She has no pain with knee range of motion from 45 to 110 degrees. The patient vacationed in central Connecticut 1 month ago.
1
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3
Aspiration, cultures, Lyme serology, and oral amoxicillin
4
Biopsy, culture, curettage, bone graft, and possible internal fixation
5
Physical therapy, ibuprofen, and an antinuclear antibody test
- Aspiration, cultures, Lyme serology, and oral amoxicillin
QUESTION 15
of 100
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
1
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3
Aspiration, cultures, Lyme serology, and oral amoxicillin
4
Biopsy, culture, curettage, bone graft, and possible internal fixation
5
Physical therapy, ibuprofen, and an antinuclear antibody test
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.
Figure 17
QUESTION 16
of 100
Figure 17 is the radiograph of a 3-year-old girl who has shoulder pain after a fall. What is the best next step?
1
4 to 6 weeks of immobilization
2
Incisional biopsy followed by curettage and bone grafting
3
Irrigation and debridement and then antibiotics based on culture findings
4
Radical excision
Patients with a pathologic fracture of a unicameral bone cyst or simple bone cyst should first pursue nonsurgical treatment and 4 to 6 weeks of immobilization. Spontaneous healing occurs in fewer than 10% of patients, possibly due to cyst decompression. The most appropriate form of surgical treatment is controversial. Many substances have been injected with variable results. Injection with steroid, bone marrow, demineralized bone matrix, and calcium phosphate/calcium sulfate have been attempted. Curettage and bone grafting and
decompression have been attempted. Indications for treatment are based on cyst size, symptoms, and location. Unicameral bone cysts typically resolve as patients reach skeletal maturity.
Figure 18
CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 23
Figure 18 is the lateral radiograph of the lumbar spine of an 11-year-old boy who has had lower back pain for 2 months. There is no history of injury. He denies radiating pain to his legs, numbness, weakness, and bowel or bladder changes. His usual activities include soccer practices and games 3 to 5 times per week. He has used over-the-counter anti-inflammatory medications, but has had no other treatment.
QUESTION 17
of 100
An examination most likely will reveal pain with
1
forward bending of the back.
2
hyperextension of the back.
3
flexion, abduction, and external rotation testing of the hips.
4
passive straight-leg raising.
- hyperextension of the back.
QUESTION 18
of 100
The addition of oblique lumbar radiographs has been shown to
1
allow easier classification of the condition severity.
2
allow easier determination of the stage of healing.
3
provide greater diagnostic accuracy for the condition.
4
provide no significant benefit.
- provide no significant benefit.
QUESTION 19
of 100
Initial treatment for this condition should include
1
activity modification and therapy to support the lumbar musculature.
2
a thoracolumbar sacral orthosis to immobilize the lower lumbar spine.
3
a diagnostic/therapeutic injection of the defect.
4
open treatment with fusion and instrumentation of the defect.
- activity modification and therapy to support the lumbar musculature.
QUESTION 20
of 100
The family is curious about the likelihood that the condition could worsen. What is the main risk factor for progression of this condition?
1
Male gender
2
Age
3
The involved level
4
Ethnicity
- Age
QUESTION 21
of 100
What is the statistical likelihood that this boy could develop a progressive deformity for which surgery would be necessary?
1
Lower than 5%
2
10%
3
25%
4
50%
- Lower than 5%
QUESTION 22
of 100
This condition is most prevalent in people of which ancestry?
1
Northern European
2
Asian
3
Native American
4
Sub-Saharan African
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.
Figure 24a
Figure 24b
QUESTION 23
of 100
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
1
Immediate open reduction with an anterior approach
2
Immediate open reduction with a posterior approach
3
Obtain an immediate arteriogram
4
Perform closed reduction and reassess perfusion and pulse
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
QUESTION 24
of 100
A concussion diagnosis is made when there is
1
a 20% decrease in the neurocognitive score from baseline.
2
a brain MRI with abnormal findings.
3
a loss of consciousness for longer than 15 seconds.
4
evidence of a traumatic brain injury that alters the way the brain functions.
Neurocognitive testing is a helpful tool in the management of concussions, but testing does not independently determine if an athlete has experienced a concussion or when he or she can return to play. Neuroimaging findings typically are normal in concussive injury. Loss of consciousness occurs in fewer than 10% of patients with concussions. A concussion diagnosis is difficult to determine because of the lack of objective clinical and/or imaging findings. In general, a concussion is a disturbance in brain function caused by a direct or indirect force to the head.
Figure 26
Figure 27a
Figure 27b
Figure 28
Figure 29
Figure 30
Figure 31a
Figure 31b
RESPONSES FOR QUESTIONS 26 THROUGH 31
1. Plain radiographs
2. CT scan
3. MRI
4. Arthrogram
Which imaging method listed above is most appropriate for definitive diagnosis and management of each clinical scenario described below?
QUESTION 25
of 100
Figure 26 is a radiograph of an 11-year-old boy with insidious-onset anterior knee pain.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- MRI
QUESTION 26
of 100
Figures 27a and 27b are the radiographs of a 2-month-old with a swollen ankle and abdominal bruising.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- Plain radiographs
QUESTION 27
of 100
Figure 28 is the radiograph of a 14-year-old boy with an ankle injury.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- CT scan
QUESTION 28
of 100
Figure 29 is the radiograph of a 12-year-old female gymnast with elbow pain.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- MRI
QUESTION 29
of 100
Figure 30 is the radiograph of a newborn admitted to the neonatal intensive care unit (NICU) with a swollen elbow following a difficult birth.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- Arthrogram
QUESTION 30
of 100
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.
Figure 32
QUESTION 31
of 100
Figure 32 is the current right femur lateral radiograph of a 9-year-old boy who went to the emergency department after falling from his skateboard. He has acute right leg pain, deformity, and cannot bear weight. Vascular and neurologic examination findings are normal. His skin is intact; however, he has a healed 3-inch scar on the lateral side of his right thigh. The boy weighs 90 pounds. Treatment should include
1
a 1-1/2 hip spica cast.
2
removal of the plate and insertion of flexible titanium nails.
3
removal of the plate and insertion of a rigid reamed nail with an entry point for the nail starting at the piriformis fossa.
4
placement of a proximal tibial traction pin for 4 weeks of skeletal traction followed by a 1-leg spica cast.
This patient’s first femur fracture at age 7 was treated with a compression plate after he was struck by a motor vehicle. He sustained a second femur fracture at the end of the plate after a fall from a skateboard. Spica casting typically is recommended patients up to the age of 6 who weigh less than 25 kg. Tibial traction pins are not recommended for children because of risk for injury to the proximal tibial physis. A trochanteric entry rigid nail can be used, but a piriformis entry nail is not recommended for children because of risk for avascular necrosis of the femoral head. Removal of the plate and fixation with flexible titanium nails is a prudent option to fix the transverse fracture with a load-sharing device. Flexible nails are indicated for children weighing up to 50 kg.
CLINICAL SITUATION FOR QUESTIONS 33 THROUGH 36
A 10-year-old girl has right knee pain related to activity. An avid soccer player, she has noted pain after the first 15 minutes of running but no swelling or mechanical symptoms. Radiographs show a large 2-cm osteochondritis dissecans (OCD) lesion.
QUESTION 32
of 100
What is the most appropriate treatment?
1
Activity restriction and follow-up radiographs in 3 months
2
Long-leg casting for 3 months
3
Arthroscopic evaluation and drilling
4
Arthroscopic vs an open osteochondral autograft transfer system (OATS) procedure
- Activity restriction and follow-up radiographs in 3 months
QUESTION 33
of 100
The patient returns after 3 months and the lesion is still present radiographically, with minimal appreciable healing. Her symptoms are controlled with activity restriction. What is the best next step at this stage?
1
Activity restriction and follow-up radiographs in 3 months
2
Long-leg casting for 3 months
3
Arthroscopic evaluation and drilling
4
Arthroscopic vs an open OATS procedure
- Activity restriction and follow-up radiographs in 3 months
QUESTION 34
of 100
The patient falls and undergoes imaging that demonstrates the lesion is unstable. What is the best next step?
1
Continued observation for 3 more months
2
Arthroscopic evaluation and drilling
3
Arthroscopic evaluation and fixation
4
Open debridement and osteochondral autograft transfer
- Arthroscopic evaluation and fixation
QUESTION 35
of 100
The patient does well initially but returns for the 4-month postsurgical evaluation with ongoing stiffness and pain despite going to physical therapy twice weekly and working on motion at home. She is unable to bear weight comfortably. What is the best next step?
1
Manipulate the knee under anesthesia
2
Aspirate the knee for persistent hematoma to improve motion
3
Obtain advanced imaging to evaluate the lesion and fixation
4
Prescribe more intensive physical therapy 3 to 5 times a week to achieve motion
In a skeletally immature patient with OCD and minor symptoms, the lesion can be observed and healing obtained with activity limitations if the cartilage is stable (but this cannot be determined radiographically or clinically). Activity restriction and serial follow-up are appropriate if an MRI reveals a stable lesion. MRI is indicated when there is concern that a lesion may be unstable. Surgical treatment depends on MRI findings.
Observation is recommended for OCD lesions in growing patients for 6 months because healing has been observed. Early surgical procedures, although they may be needed in the future, are not appropriate for patients with well-controlled symptoms.
If symptoms continue for longer than 6 months, arthroscopic drilling is not indicated for unstable OCD. The appropriate treatment is OCD fixation. Debridement is not appropriate with a stable lesion.
Evaluation of the fixation and stability of the lesion with advanced imaging after weight bearing and therapy initiation is the most appropriate option. Manipulating the knee without determining whether the stiffness is attributable to subsidence of the fixation or mechanical block is not appropriate. After 4 months, aspiration of a hematoma (if still present) would not yield much benefit. More therapy is not likely to be useful when a patient is attending therapy regularly and working on a home program.
Figure 37a
Figure 37b
Figure 37c
QUESTION 36
of 100
Figure 37a is the initial radiograph of a 7-year-old boy who fell from monkey bars 4 hours ago. He has intact motor function in his fingers and normal capillary refill, but his radial pulse is not palpable. Figures 37b and 37c are the radiographs following closed reduction and pinning. This boy’s hand and fingers remain pink, but his radial pulse remains nonpalpable. What is the best next step?
1
An arteriogram to evaluate the brachial artery
2
Open exploration and repair of the brachial artery
3
Pin removal to rereduce the fracture
4
Additional splinting and continued observation in the hospital
Figure 37a shows a completely displaced supracondylar humerus fracture. The first step in the situation described, which involves a pink pulseless hand, is to perform an urgent closed manipulation and pinning. The vascular examination should be reassessed following the reduction. When adequate reduction has been achieved and the pulse remains nonpalpable but the hand is pink and capillary refill is normal, the fracture may be splinted and the patient observed closely in the hospital. Arteriography is not useful and may delay revascularization or increase vessel spasm. Although some investigators have concluded that exploration of the brachial artery may be indicated, the algorithm that includes observation only is the most supported and the most commonly practiced treatment. The radiographs show adequate reduction and fixation without medial widening at the fracture site, which might indicate a site of brachial artery entrapment. Therefore, pin removal and fracture rereduction is not indicated.
RESPONSES FOR QUESTIONS 38 THROUGH 45
1. Sclerosis of the proximal femoral epiphysis with subchondral lucency
2. Abnormal femoral head-neck junction offset
3. Widening of the proximal femoral physis with normal femoral head-neck junction offset
4. Absence of the proximal femoral epiphysis secondary ossification center
For each clinical scenario below, select the most likely associated radiographic finding from the list above.
QUESTION 37
of 100
A 6-year-old boy has a 2-month history of intermittent, mild, unilateral thigh pain and a limp. An examination reveals a Trendelenburg sign and restricted hip abduction and internal rotation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Sclerosis of the proximal femoral epiphysis with subchondral lucency
QUESTION 38
of 100
An 11-year-old obese boy has a 5-month history of unilateral knee pain and a limp. An examination reveals obligate external rotation with flexion and pain with attempted hip internal rotation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Abnormal femoral head-neck junction offset
QUESTION 39
of 100
An 18-month-old girl was treated at the age of 4 months with medial open reduction of a unilateral developmental hip dislocation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Absence of the proximal femoral epiphysis secondary ossification center
QUESTION 40
of 100
A 15-year-old boy who underwent in situ fixation of a stable slipped capital femoral epiphysis 2 years ago now has groin pain and mechanical symptoms.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Abnormal femoral head-neck junction offset
QUESTION 41
of 100
A 10-year-old boy has chronic renal failure and activity-related groin pain.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Widening of the proximal femoral physis with normal femoral head-neck junction offset
QUESTION 42
of 100
A 12-year-old girl was treated with open reduction and internal fixation for an unstable slipped capital femoral epiphysis. Anatomic alignment with normal femoral head-neck offset was achieved, but she now has worsening groin pain. Examination reveals an antalgic gait, and her hip has limited passive internal and external rotation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Sclerosis of the proximal femoral epiphysis with subchondral lucency
QUESTION 43
of 100
A 17-year-old male baseball catcher has groin pain and intermittent hip locking. Examination demonstrates reproduction of the pain with hip flexion, internal rotation, and adduction. MR imaging reveals an anterosuperior labral tear.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Abnormal femoral head-neck junction offset
QUESTION 44
of 100
A 10-month-old boy has an untreated developmental hip dislocation.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.
Figure 46a
Figure 46b
Figure 46c
Figure 46d
QUESTION 45
of 100
Figures 46a through 46d are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?
1
Compartment syndrome
2
Loss of elbow motion
3
Avascular necrosis (AVN) of the radial head
4
Nonunion of the fracture site
This girl sustained a fracture dislocation of the elbow with a severely displaced and rotated radial neck fracture. Required treatment was open reduction and internal fixation (ORIF). Less severely displaced radial neck fractures can be treated with closed reduction, percutaneous pinning, or flexible nail manipulation. In this scenario, interposed capsular tissue and rotation of the radial head were indications for ORIF. ORIF is associated with a higher risk for poor
outcomes. Complications following ORIF of radial neck fractures in children include posterior interosseous neuropraxia, valgus angulation, premature closure of the radial head physis, AVN of the radial head, nonunion, and elbow stiffness. Stiffness is most common. Compartment syndrome, infection, and anterior interosseous nerve palsy are less common complications.
Figure 47a
Figure 47b
CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 6-year-old boy arrives at the emergency department with forearm pain. Today he was picking up his backpack when he felt a pop in his forearm that resulted in the current injury. His history is significant for 6 other fractures treated nonsurgically. His mother states that she had 15 fractures during childhood but is healthy now. Both the boy and his mother have blue sclera. Figures 47a and 47b are the radiographs of his injured forearm.
QUESTION 46
of 100
Based on this history and radiographic examination, how should you advise the family?
1
Many people fracture during childhood, so no further workup is indicated.
2
The boy likely has osteogenesis imperfecta (OI).
3
The boy has rickets and needs treatment with vitamin D.
4
The fracture pattern does not match the history and is suspicious for nonaccidental trauma.
- The boy likely has osteogenesis imperfecta (OI).
QUESTION 47
of 100
What is the most likely underlying bone problem?
1
None; this is suspicious for nonaccidental trauma
2
A genetic defect in the type I collagen gene
3
A genetic defect in the type II collagen gene
4
A genetic defect in the prolyl 3-hydroxylase 1 gene (LEPRE1)
- A genetic defect in the type I collagen gene
QUESTION 48
of 100
The fracture location and pattern can be explained because
1
there is a sudden change in elasticity between the plated and unplated bone.
2
there is probably an unrecognized infection from the original open fracture.
3
the plates were put in improperly.
4
the original fracture never completely healed.
- there is a sudden change in elasticity between the plated and unplated bone.
QUESTION 49
of 100
Which treatment of the current fracture will provide the best long-term outcome?
1
Casting it in its current position, which is acceptable alignment
2
Closed reduction and casting
3
Functional brace because this is a stable fracture
4
Open reduction with revision of the current implants
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
Figure 51a
Figure 51b
Figure 51c
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
QUESTION 50
of 100
The workup to exclude other congenital abnormalities should include evaluation of which systems?
1
Cardiac, renal, and gastrointestinal (GI)
2
Cardiac, renal, and auditory
3
Cardiac, pulmonary, and GI
4
Cardiac, pulmonary, and neural axis
- Cardiac, renal, and auditory
QUESTION 51
of 100
This shoulder deformity often is associated with an abnormal connection between the scapula and the
1
posterior ribs.
2
clavicle.
3
humerus.
4
spine.
- spine.
QUESTION 52
of 100
Recommendations for sports activity should include
1
full participation without restrictions.
2
avoidance of contact or collision sports.
3
avoidance of racquet sports.
4
avoidance of throwing sports.
- avoidance of contact or collision sports.
QUESTION 53
of 100
Genetic mutations that may result in the cervical abnormalities noted in the figures generally affect the
1
embryonic process of neurulation.
2
embryonic process of gastrulation.
3
segmentation or resegmentation of somites.
4
differentiation of somites into sclerotome, myotome, and dermatome segments.
The figures are characteristic of a child with Klippel-Feil syndrome (congenital cervical spine abnormalities) in association with congenital scoliosis in the upper thoracic spine and a right-sided Sprengel deformity (congenital elevation of the scapula). Sprengel deformity occurs in as many as 30% of children with Klippel-Feil syndrome. Other congenital conditions that are commonly associated with Klippel-Feil, and that should be screened for, include deafness in 30%, genitourinary abnormalities in 25% to 35%, and cardiovascular abnormalities in 4% to 29% of children with Klippel-Feil syndrome.
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.
Figure 55a
Figure 55b
Figure 55c
QUESTION 54
of 100
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
1
Anesthesia in the first dorsal web space
2
Inability to extend the fingers
3
Inability to abduct the fingers
4
Inability to flex the thumb interphalangeal (IP) joint
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.
Figure 56
QUESTION 55
of 100
Figure 56 is the radiograph of an otherwise healthy 3-year-old boy who fell and sustained the isolated injury shown. What is the best treatment modality?
1
Elastic intramedullary nailing
2
Submuscular plating
3
Early hip spica casting
4
Traction as definitive treatment
At 3 years of age, children do well with nonsurgical treatment with early spica casting and early mobilization. There is no indication to perform surgical stabilization in such a closed isolated injury. The fracture is not shortened unacceptably according to clinical practice guidelines, and traction for this fracture is unnecessary. Traction also may be problematic for the family and healthcare system.
RESPONSES FOR QUESTIONS 57 THROUGH 62
1. Cortical thickening in the region of the lesion
2. Erosive metaphyseal lesion with loss of cortical integrity
3. Normal bony anatomy on radiographs
4. Diffuse articular erosion with loss of joint space
5. Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
6. Eccentric well-circumscribed metaphyseal lesion with a scalloped border
Match the orthopaedic condition described below with the expected radiographic finding listed above.
QUESTION 56
of 100
Osteomyelitis with 72 hours of symptoms
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
- Normal bony anatomy on radiographs
QUESTION 57
of 100
Osteomyelitis with 14 days of symptoms
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
- Erosive metaphyseal lesion with loss of cortical integrity
QUESTION 58
of 100
Septic arthritis with 48 hours of symptoms
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
- Normal bony anatomy on radiographs
QUESTION 59
of 100
Osteoid osteoma with 1 year of symptoms
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
- Cortical thickening in the region of the lesion
QUESTION 60
of 100
Unicameral bone cyst
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
- Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
QUESTION 61
of 100
Nonossifying fibroma
1
Cortical thickening in the region of the lesion
2
Erosive metaphyseal lesion with loss of cortical integrity
3
Normal bony anatomy on radiographs
4
Diffuse articular erosion with loss of joint space
5
Round, expansive, well-circumscribed metaphyseal lesion with thinning of the cortex
Early osteomyelitis and septic arthritis appear as normal bony anatomy on radiographs, with perhaps only soft-tissue swelling seen. Radiographic changes with metaphyseal erosion appear in a delayed fashion, often after 7 or more days in indolent infections, but may present earlier in association with virulent infections such as methicillin-resistant Staphylococcus aureus. Osteoid osteoma has a radiolucent small nidus that may be difficult to see on radiograph; however, chronic cases cause marked cortical hypertrophy. Unicameral bone cysts are expansile metaphyseal lesions that are never wider than the physis. They are symmetric, well circumscribed, and can have cortical thinning. When fractures through the cyst are
present, the fallen leaf sign is visible as cortical fragments fall to the bottom of the cyst. Nonossifying fibromas are eccentric metaphyseal lesions with scalloped borders.
QUESTION 62
of 100
In the United States, groups at risk for community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) within the pediatric and adolescent populations include
1
tennis players.
2
toddlers in daycare.
3
children who are home schooled.
4
African Americans.
CA-MRSA is a growing problem in the United States. Groups at risk for CA-MRSA include athletes in contact sports and children in daycare. Tennis players, golfers, and runners are at lowest risk because their sports do not require close contact with teammates or competitors. Outbreaks have been noted in Alaskan native, Native American, and Pacific Islander minority populations.
Figure 64a
Figure 64b
Figure 64c
Figure 64d
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 68
Figures 64a through 64d are the radiographs of an 11-year-old boy with a prolonged history of activity-related ankle pain. An examination is notable for restricted subtalar motion and moderate pes planovalgus.
QUESTION 63
of 100
The diagnosis is
1
Freiberg infraction.
2
tarsal coalition.
3
accessory navicular.
4
neglected clubfoot.
- tarsal coalition.
QUESTION 64
of 100
Which inheritance pattern has been described for the condition shown in Figures 64a through 64d?
1
Autosomal recessive
2
Autosomal dominant
3
X-linked recessive
4
X-linked dominant
- Autosomal dominant
QUESTION 65
of 100
The condition shown in Figures 64a through 64d is overrepresented among craniosynostosis syndromes with mutations in
1
MSX-2 and MSX-3.
2
EFNB-1.
3
TWIST-1.
4
FGFR-1, FGFR-2, and FGFR-3.
- FGFR-1, FGFR-2, and FGFR-3.
QUESTION 66
of 100
The patient fails nonsurgical treatment. What is the best next step?
1
CT scan
2
MRI
3
Bone scan
4
Laboratory studies: complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), antinuclear antibody (ANA), and rheumatoid factor (RF)
- CT scan
QUESTION 67
of 100
The CT scan shows the involvement area is approximately 30% of the posterior facet.
What is the most appropriate treatment?
1
Surgical resection
2
Lateral column lengthening
3
Coalition resection and lateral column lengthening
4
Triple arthrodesis
Radiographs reveal a talocalcaneal coalition. The incidence of tarsal coalition in the general population ranges between 2% and 13%. The incidence of tarsal coalition among patients with FGFR-related craniosynostosis syndromes is much higher than among the general population. Tarsal coalitions have been noted in FGFR-1-, FGFR-2-, and FGFR-3-related craniosynostosis syndromes of Apert, Pfeiffer, Crouzon, Jackson-Weiss, and Muenke, but not in Beare-Stevenson or Crouzonodermoskeletal syndromes. The FGFR genes are involved in cell proliferation, differentiation, migration, apoptosis, and pattern formation.
Additionally, nonsyndromic familial coalitions have been described with autosomal-dominant patterns of inheritance.
Cross-sectional imaging should always be obtained prior to resection of a radiographically evident coalition to define the extent of the coalition and determine the coexistence of an additional coalition. CT scan is the gold standard test; however, MRI can be helpful to define a suspected fibrous coalition if a CT scan is nondiagnostic. A bone scan may be useful if pain or history is atypical for a symptomatic coalition. Laboratory tests such as CBC, ESR, CRP, ANA, and RF may be indicated if the imaging evaluation does not confirm a tarsal coalition and if there is concern for malignancy, infection, or inflammatory arthritis.
Investigators have suggested that larger talocalcaneal coalitions with surface areas larger than 33% to 50% of the size of the posterior facet are unsuitable for resection and primary arthrodesis should be considered. However, a study by Koshbin and associates found that with long-term follow-up, favorable functional outcomes were seen even with resections of large talocalcaneal coalitions occupying more than 50% of surface area.
QUESTION 68
of 100
A 4-year-old girl who attends daycare had knee swelling for 21 days. She has been afebrile, her white blood cell (WBC) count is 13000/mm3 (reference range [rr], 4500-11000 /µL), and her C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are slightly elevated. The child is unable to walk because of her pain. Radiographs show a knee effusion. A sedated knee aspiration reveals 22000 cells/ml (a normal result is less than 1000 cells/mL). A culture of the aspirate is pending. What is the best next step?
1
Presumptively treat for toxic synovitis of the knee
2
Presumptively treat for juvenile idiopathic arthritis
3
Perform polymerase chain reaction (PCR) screening for Kingella kingae (K. kingae)
4
Perform arthroscopic debridement and knee irrigation
K. kingae is variably invasive and is a facultative anaerobic gram-negative bacillus. K. kingae is a common bacteria that causes osteoarticular infections in young children. Presentation is often delayed because of the moderate course of the infection. Ten percent of young children are colonized with K. kingae. Colonization occurs in the oropharynx and is a prerequisite for invasive K. kingae septic arthritis. The PCR test screens for the RTX protein,
the factor responsible for the bacteria’s cytotoxicity. Among children in daycare centers, 28% are colonized. The sensitivity of the oropharyngeal swab PCR has been reported at 100%, and the specificity is 90.5%.
RESPONSES FOR QUESTIONS 70 THROUGH 74
1. Thrower's elbow/physeal irritation of the medial epicondylar physis
2. Osteochondritis dissecans (OCD)
3. Supracondylar humeral stress fracture
4. Patellar sleeve fracture
5. Distal femoral physeal fracture
6. Sinding-Larsen-Johansson syndrome/inferior pole patella apophysitis
7. Medial meniscal tear
8. Patellar tendon rupture
9. Patellofemoral pain syndrome
10. Popliteal cyst
11. Osteochondroma
12. Synovial sarcoma
Match the appropriate orthopaedic condition above with the clinical scenario below.
QUESTION 69
of 100
A 10-year-old Little League pitcher has elbow pain and stiffness. Upon examination, he has a flexion contracture of 10 degrees and lateral elbow pain on palpation.
1
Thrower's elbow/physeal irritation of the medial epicondylar physis
2
Osteochondritis dissecans (OCD)
3
Supracondylar humeral stress fracture
4
Patellar sleeve fracture
5
Distal femoral physeal fracture
- Osteochondritis dissecans (OCD)
QUESTION 70
of 100
An 8-year-old basketball player jumped up and felt a pop in his knee. He has diffuse anterior swelling and pain, and he is unable to perform a straight-leg raise. A small fleck of bone is seen distal to the patella on his radiograph.
1
Thrower's elbow/physeal irritation of the medial epicondylar physis
2
Osteochondritis dissecans (OCD)
3
Supracondylar humeral stress fracture
4
Patellar sleeve fracture
5
Distal femoral physeal fracture
- Patellar sleeve fracture
QUESTION 71
of 100
A 13-year-old soccer player describes popping and catching on the medial side of his knee with activity. This has slowly worsened during the season. Upon examination, there is medial joint line tenderness and medial pain with McMurray testing.
1
Thrower's elbow/physeal irritation of the medial epicondylar physis
2
Osteochondritis dissecans (OCD)
3
Supracondylar humeral stress fracture
4
Patellar sleeve fracture
5
Distal femoral physeal fracture
- Medial meniscal tear
QUESTION 72
of 100
A 9-year-old cheerleader is brought in for concern regarding a knee mass. She has no pain but is experiencing waxing and waning swelling at the back of her knee. There is no anterior swelling, and range of motion is full. Upon examination, the 3-cm x 3-cm posteromedial mass is mobile and it transilluminates.
1
Thrower's elbow/physeal irritation of the medial epicondylar physis
2
Osteochondritis dissecans (OCD)
3
Supracondylar humeral stress fracture
4
Patellar sleeve fracture
5
Distal femoral physeal fracture
- Popliteal cyst
QUESTION 73
of 100
A 13-year-old girl has had to restrict her activity because of anterior knee pain. Upon examination, she has no point tenderness or effusion with normal knee range of motion. She has a normal gait and normal knee alignment and appearance. A ligamentous examination is stable. There is mild patellofemoral crepitation. Her radiograph findings are normal.
1
Thrower's elbow/physeal irritation of the medial epicondylar physis
2
Osteochondritis dissecans (OCD)
3
Supracondylar humeral stress fracture
4
Patellar sleeve fracture
5
Distal femoral physeal fracture
OCD of the capitellum presents in throwing athletes with lateral pain and a flexion contracture vs medial epicondylar physeal overuse, which is associated with medial pain and possible widening of the physis on radiograph.
Midsubstance patellar tendon rupture is rare in skeletally immature patients; usually, disruption of the extensor mechanism occurs either through a tibial tubercle physis fracture or a patellar sleeve fracture because these cartilaginous areas are structurally weaker than the patellar tendon. Often, only a small bony fleck is seen, and the main fracture is cartilaginous.
Medial joint line pain and a positive McMurray test result are most consistent with a medial meniscal tear. Sinding-Larsen-Johansson syndrome would produce soreness over the inferior pole of the patella.
Because the knee mass is painless and cystic, synovial sarcoma is unlikely because these sarcomas are solid, progressive, and painful. An osteochondroma would be a bony protrusion and would not transilluminate, which is a feature of cystic masses. It also would not change size. Popliteal cysts are common in children, with most resolving spontaneously over several years.
Patellofemoral pain syndrome can cause mild anterior compartment crepitation but does not produce point tenderness over a specific apophysis like Sinding-Larsen-Johansson syndrome (inferior pole of patella tenderness). It is common in pubertal girls and is treated with rest, ice, nonsteroidal anti-inflammatory drugs, and therapy exercises with resolution in most cases.
Figure 75a
Figure 75b
QUESTION 74
of 100
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
1
Brachialis muscle
2
Radial nerve
3
Median nerve
4
Ulnar nerve
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
Figure 76
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
QUESTION 75
of 100
The pathogenesis of this condition is associated with
1
a PITX1 mutation.
2
a point polymorphism in a regulatory sequence for the COLIA-1 gene.
3
mutations in the EXT gene family.
4
mutations in the COL5A or COL3A genes.
- a PITX1 mutation.
QUESTION 76
of 100
The idiopathic form of this condition may be associated with
1
absence of the anterior tibial artery.
2
absence of the fibula.
3
duplication of the first ray.
4
postaxial polydactyly.
- absence of the anterior tibial artery.
QUESTION 77
of 100
The bony abnormalities in this condition occur mostly in the
1
tibiotalar joint.
2
tarsal bones.
3
tarsal-metatarsal joint.
4
forefoot.
- tarsal bones.
QUESTION 78
of 100
The infant underwent Ponseti casting for 5 weeks. Afterward, a heel cord release was done 1 cm proximal to the insertion site of the Achilles tendon and was casted in long-leg casts with the knee flexed and an external rotation mold on the leg for 3 weeks. Straight-last shoes with an abduction bar set at 70 degrees of external rotation were fitted. The infant’s feet remained in the corrected position at a 1-month check, but, at a 3-month check, ankle equinus and forefoot varus were present. Recurrence of the deformity is most likely attributable to
1
noncompliance with postsurgical bracing.
2
insufficient length of time in postsurgical casts.
3
proximal placement of the incision for heel cord release.
4
excessive rotation of postsurgical bracing.
- noncompliance with postsurgical bracing.
QUESTION 79
of 100
Recurrence of this deformity after initial treatment should be treated with
1
recasting.
2
anterior tibialis tendon transfer.
3
extensive posteromedial-lateral release.
4
tibial osteotomy.
Single nuclear polymorphism (SNP) on chromosome 12q24.31, an intergenic SNP, is the PITX1-TBX4 transcriptional pathway that codes for hindfoot formation and is associated with clubfoot. The COLIA-1 gene is related to osteoporosis. Mutations in EXT genes that control formation of tumors cause multiple hereditary exostosis. Mutations in the COL5A or COL3A genes are associated with Ehlers-Danlos syndrome. All idiopathic clubfeet involve abnormalities of or around the talus.
The classic Ponseti technique is associated with a low recurrence rate when followed precisely. The most common reason for recurrence is noncompliance with postsurgical bracing. The initial treatment for recurrence after Ponseti casting is recasting.
NCOA2 fusion transcripts has been noted in mesenchymal chondrosarcoma. Ring chromosomes with CDK4 and MDM2 amplification may be identified with low-grade central osteosarcoma or parosteal osteosarcoma. Fusion transcripts of CDH11-USP6 have been observed in aneurysmal bone cysts.
Figure 82a
Figure 82b
Video 85
CLINICAL SITUATION FOR QUESTIONS 82 THROUGH 85
Figures 82a and 82b are the radiographs of a 10-year-old girl who was an unrestrained back seat passenger in a motor vehicle collision. Her sole injury is to her left leg. She has a deformed valgus knee with lateral swelling and bruising, and no wound is visible. Upon examination, she has symmetric pulses to her right leg but diminished sensation on the dorsum of the foot and in the first web space. She cannot dorsiflex her left foot or toes but can plantar flex and invert them. Weak ankle eversion is present. Sensation to the plantar foot, medial ankle, and lateral ankle is intact. She likely will reach skeletal maturity at age 14.
QUESTION 80
of 100
What is the zone of injury?
1
Proliferative zone
2
Resting zone
3
Hypertrophic zone
4
Zone of maturation
- Hypertrophic zone
QUESTION 81
of 100
The examination suggests a neurologic deficit of which nerve?
1
Common peroneal nerve
2
Superficial peroneal nerve
3
Deep peroneal nerve
4
Tibial nerve
- Common peroneal nerve
QUESTION 82
of 100
The patient is treated with emergent open reduction and internal fixation via a lateral approach to the distal femur. The peroneal nerve is found intact but is under pressure by a proximal bone fragment. After fixation, there is near-anatomic fracture reduction and no tension on the nerve. The patient is comfortable at a postsurgical check 4 hours later. Her toes
are warm and pink and there is no pain with passive dorsiflexion/plantar flexion of the toes. However, she continues to have absent first web space sensation, diminished dorsal foot sensation, and absent toe/ankle dorsiflexion. What is the best next step?
1
Return to surgery emergently for 4-compartment fasciotomy because she has a compartment syndrome and the nerve will not otherwise recover
2
Return to surgery urgently within the next few days for nerve exploration and potential microsurgical repair (vs cable grafting) to the damaged nerve to speed repair
3
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
4
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 12 months after surgery
- Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
QUESTION 83
of 100
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
1
The fracture is healed and the physis is growing well with no problems expected.
2
Complete physeal closure has occurred. There will be no significant leg length difference because the patient is almost done growing.
3
Complete physeal closure has occurred. There will be a significant (> 2-cm) leg length difference if no other surgical treatment is offered.
4
Asymmetric physeal closure has occurred. There will be an increasing angular deformity at the knee as well as a significant (> 2-cm) leg length difference if no other surgical treatment is offered.
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
QUESTION 84
of 100
A 17-year-old cross country athlete runs 7 miles per day, 6 days per week. She has new-onset right groin pain. Passive flexion of her hip is normal, but internal rotation of the hip, resisted hip flexion, and knee extension reproduce the pain. Hip radiograph findings are normal. What is the best next step?
1
Recommend decreasing her training regimen
2
Obtain a bone scan
3
Obtain an MRI
4
Obtain a dual-energy x-ray absorptiometry (DEXA) scan
A stress fracture of the femoral neck or pelvis should be ruled out in this patient. She should be placed on crutches and not allowed to run. The consequences of missing such a diagnosis can be devastating. Superior cortical femoral neck stress fractures are tension injuries and can progress to a complete fracture and avascular necrosis. Surgical fixation may be indicated. Plain radiographic findings often do not appear until late in the clinical course. MRI is more accurate, more specific, and is superior to radionuclide bone scanning for the diagnosis of stress fracture in young endurance athletes. MRI detects early changes in osseous
stress injury and allows precise definition of the anatomy and extent of injury. This patient may have the female athletic triad: disordered eating, amenorrhea, and osteoporosis. However, the workup for this condition (including a possible DEXA scan) may be delayed until after the stress fracture is diagnosed and treated.
Figure 87a
Figure 87b
Figure 88
Figure 89
Figure 90
CLINICAL SITUATION FOR QUESTIONS 87 THROUGH 90
Figures 87a and 87b are the clinical photograph and radiograph of a 14-year-old high school football player who fractured his dominant right clavicle. The skin is closed and vascular and neurologic examination findings are normal.
QUESTION 85
of 100
What is the best initial treatment?
1
A sling and careful follow-up
2
Open reduction and internal fixation (ORIF) using an intramedullary pin
3
ORIF using a 4-hole semitubular plate
4
ORIF using an 8-hole pelvic reconstruction plate
- A sling and careful follow-up
QUESTION 86
of 100
Figure 88 is the current radiograph. The patient received nonsurgical treatment. Two months later he is pain free and vascular and neurological examination findings have remained normal, but he has a large palpable bony bump under his skin. What is the best next step?
1
Open reduction of the clavicle and compression plating
2
Open reduction of the clavicle malunion and compression plating
3
Open reduction of the clavicle malunion and intramedullary fixation with a flexible titanium nail
4
Observation and careful follow-up
- Observation and careful follow-up
QUESTION 87
of 100
Figure 89 is the radiograph of this boy 3 months later. The patient and family ask if he can safely play baseball in the spring. He is pain free at this time. What is the best advice?
1
No sports allowed; recommend clavicle bump resection, contouring, and plating
2
No sports allowed; recommend clavicle bump resection (no plate needed)
3
Allow baseball as tolerated and careful follow-up
4
Recommend an electrical stimulator and advise him to change his sport and join the swim team
- Allow baseball as tolerated and careful follow-up
QUESTION 88
of 100
Figure 90 is the radiograph of this patient 5 months later when he returned for his preseason football physical. He is asymptomatic. What is the best next step?
1
Advise against football because of increased risk for clavicle fracture
2
Order a bone density test prior to return to football
3
Allow football as tolerated and follow up as the situation demands
4
Perform a clavicular osteotomy and plating
This patient has a closed midshaft clavicle fracture with significant displacement that has healed and remodeled nicely with nonsurgical treatment. Functional disability or nonunion after nonsurgical treatment of clavicle fractures in adolescents is rare. Schulz and associates showed no differences in pain, strength, range of motion, or subjective outcome scores between injured and uninjured limbs treated nonsurgically to address displaced, shortened midshaft clavicle fractures in adolescents. Bae and associates demonstrated that clavicle fracture malunions in adolescents do not cause loss of motion or strength.
Figure 91a
Figure 91b
Figure 92
Figure 93
Figure 94a
Figure 94b
Figure 94c
Figure 95a
Figure 95b
Figure 96
RESPONSES FOR QUESTIONS 91 THROUGH 96
1. Chromosome 17 mutation
2. MYH3 mutation
3. Embryonic vascular interruption
4. Infantile vascular interruption
5. Chromosome 11 mutation
6. Sporadic inheritance
Select the appropriate etiology listed above for each pictured syndrome.
QUESTION 89
of 100
Figures 91a and 91b
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Embryonic vascular interruption
QUESTION 90
of 100
Figure 92
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Infantile vascular interruption
QUESTION 91
of 100
Figure 93
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Sporadic inheritance
QUESTION 92
of 100
Figures 44a through 94c
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- MYH3 mutation
QUESTION 93
of 100
Figures 95a and 95b
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Chromosome 17 mutation
QUESTION 94
of 100
Figure 96
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
Poland syndrome and Sprengel deformity (Figure 91) are hypothesized to occur as the result of interruption of the embryonic subclavian blood supply. Poland syndrome occurs proximal to the internal thoracic artery and distal to the vertebral artery; Sprengel deformity is thought to occur via interruption of the subclavian, internal thoracic, or suprascapular artery.
Hair tourniquet syndrome (Figure 92) occurs most often in children younger than 2 years of age. Human hair, which is often not seen in the band, circumferentially strangulates a digit or extremity. If not recognized and treated promptly, auto-amputation distal to the hair tourniquet may occur.
No known genetic or environmental factors are associated with the etiology of Fibular hemimelia (Figure 93). Nearly all of these patients have an absent Anterior Cruciate Ligament. Additional associations include, absent rays of the foot, tarsal coalition, hypoplastic or aplastic fibula, leg-length discrepancy, femoral and tibial hypoplasia and lower extremity angular deformity.
Freeman-Sheldon syndrome, Sheldon-Hall Syndrome and Distal arthrogryposis (Figure 94) have been associated with mutations of MYH3, the gene which codes for myosin heavy chain 3.
Fifty percent of patients with Neurofibromatosis type 1(NF1) (Figure 95) will have musculoskeletal manifestation of the disease; most commonly scoliosis and pseudarthrosis of the tibia. Twenty percent of patients with NF1 present with scoliosis. Dystrophic scoliosis is typical of NF1. Dystrophic features of include: scalloped vertebra, penciled ribs, severe
rotation, sharp and short (4-6 vertebrae) kyphoscoliosis. Although NF1 has autosomal dominant inheritance, 50% of new cases are due to sporadic mutation. The NF1 gene on chromosome 17 codes for neurofibromin, a tumor suppressor.
Beckwith-Wiedemann syndrome (Figure 96) is associated with chromosome 11 mutations near the IGF gene. Neonatal hypoglycemia; macroglossia; visceromegaly; hemihypertrophy; and embryonal tumors, especially Wilms tumor, are associated with mutations of chromosome 11.
45
Figure 100a
Figure 100b
CLINICAL SITUATION FOR QUESTIONS 97 THROUGH 100
A 12-year-old boy with a 2-day history of fever and right knee pain is admitted to the pediatric service. You are asked to provide an orthopaedic consultation. The patient denies recent trauma. His temperature is 39.4°C and his gait is antalgic. There is no palpable knee effusion and mild tenderness and swelling of the distal thigh area. Hip and knee range of motion is not limited. Radiographs of the femur are unremarkable. His white blood cell (WBC) count is within defined limits, and the differential shows 80% segmented neutrophils. His erythrocyte sedimentation rate is 46 mm/h (reference range [rr], 0-20 mm/h), and his C-reactive protein level is 5.6 mg/L (rr, 0.08-3.1 mg/L).
QUESTION 95
of 100
What is the best next step? 1- Knee aspiration
1
Blood cultures
2
Indium-labeled WBC scan
3
Pelvic radiographs
- Blood cultures
QUESTION 96
of 100
The pediatric service orders an MRI, and findings are unremarkable. Results from the tests ordered above are pending. The clinician should recommend
1
discharge home on crutches with an ibuprofen prescription.
2
discharge home with an oral antibiotic prescription.
3
initiation of intravenous (IV) antibiotics.
4
a knee CT scan.
- initiation of intravenous (IV) antibiotics.
QUESTION 97
of 100
Blood cultures drawn by the pediatric intern grow gram-positive cocci. Antibiotics should include coverage for
of 200
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
1
filling the tibial defect with methylmethacrylate.
2
revision of the tibial component with porous metal augmentation.