Score: 0%
Orthopedics Online MCQs
A 77-year-old man who had right total knee replacement surgery 2½ years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3 and 120 degrees. Radiographs show well-fixed and well-aligned implants. What is the most appropriate next step in management?
Figures 15a and 15b are the 6-week postsurgical anteroposterior hip radiograph and current radiograph of a 54-year-old avid hiker who returns for routine follow-up 3 years after an uncomplicated uncemented modular metal-on-metal hip replacement. He reports mild activity-related aching diffusely around the right hip region, but does not feel restricted with his activities. Examination reveals no local tenderness, a well-healed incision, and mild discomfort at the extremes of rotation. An erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are obtained, showing 9 mm/h (reference range, 0-20 mm/h) and 2.0 mg/L (reference range, 0.08-3.1 mg/L), respectively. What is the etiology of the radiographic finding?


What risk factor is associated with a poor prognosis after revision of a failed metal-on-metal resurfacing hip arthroplasty to total hip arthroplasty?
Ten-year follow-up studies of total hip replacements performed with modern alumina ceramic femoral heads and acetabular liners show what outcomes?
What effect does morbid obesity (body mass index [BMI] higher than 40) have on total knee arthroplasty outcomes?
A 66-year-old woman had fever, chills, and increasing pain in her right hip. She underwent a total hip arthroplasty using large-head metal-on-metal articulation 4 years earlier without complications. Her hip pain began about 1 month ago following several days of productive cough that her primary care physician had diagnosed as a viral illness. She had elevated serology with an erythrocyte sedimentation rate of 70 mm/h (reference range, 0-20 mm/h) and C-reactive protein of 3.5 mg/L (reference range, 0.08-3.1 mg/L). There is no radiographic evidence of loosening or adverse bone remodeling around the hip arthroplasty. What is the most appropriate course of action?
When comparing arthroscopic lavage and knee debridement to placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Figure 25 is the anteroposterior hip radiograph of a 74-year-old healthy and active man who was seen in the office 18 months after a primary uncemented total hip replacement with a history of 3 hip dislocations. The last dislocation occurred 1 week ago and he was treated in the emergency department with a closed reduction and application of a hip abduction brace. All episodes of dislocation occurred when bending forward. Aside from the episodes of dislocation, his hip functions well. Examination revealed a normal gait with good abductor strength and pain-free hip movement. What is the most appropriate next treatment step?

A 67-year-old man who underwent an uncomplicated hip arthroplasty 9 years ago has had a 1-week history of groin pain with movement. Radiographs reveal a well-positioned, well-fixed cementless arthroplasty with mild eccentricity of the femoral head within the polyethylene. His serum C-reactive protein (CRP) level is
3.0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
3.0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
Cryotherapy has been demonstrated to achieve what effect after total knee replacement?
Compared to retention of the native patella in primary total knee arthroplasty, routine patella resurfacing is associated with
What clinical outcome is associated with total hip replacements that have metal-metal bearings (compared to total hip replacements with metal-polyethylene bearings)?
A 55-year-old man with unilateral osteoarthritis of the hip underwent a total hip arthroplasty using cementless fixation. The acetabular cup was 52 mm and the femoral head was 28 mm and made of cobalt-chromium alloy. The bearing surface was made of annealed highly cross-linked polyethylene, with an estimated thickness of 6.5 mm. What should the orthopaedic surgeon tell the patient regarding wear of the bearing surface?
A 49-year-old active man has groin pain 3 years after undergoing an uneventful total hip replacement using a cobalt-chrome femoral head articulating against a cobalt-chrome acetabular insert. The pain intensifies with activity and travels down his thigh. Examination and radiographic evaluation are not particularly helpful; there is no evidence of spinal or vascular disease. What is the next step in the evaluation of this patient?
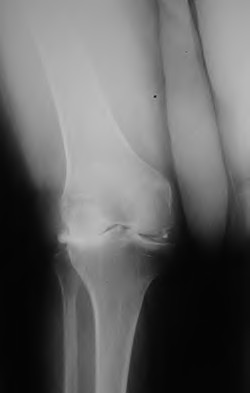
Figures A and B are the radiographs of a 25-year-old woman whose right knee pain has progressed during the last several years to pain with any activity and pain at night. What is the most appropriate treatment?


An orthopaedic surgeon noticed a displaced calcar fracture during stem insertion when performing total hip arthroplasty using cementless fixation. What is the most appropriate course of action?
A 48-year-old woman had an 8-month history of spontaneous onset of left medial knee pain. She was otherwise healthy with an unremarkable past medical history. Prior to the onset of knee pain, she jogged, played tennis, and golfed regularly. She wished to remain active. Examination showed a fit woman with a BMI of 26, a stable left
knee with full range of motion, and some mild medial joint line tenderness. Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
knee with full range of motion, and some mild medial joint line tenderness. Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
Figure 36 is the postoperative photograph of a patient who underwent a total knee arthroplasty 10 days after surgery. Knee aspiration suggests a _Streptococcus_ infection.

What is the difference in outcome when comparing high tibial osteotomy (HTO) to total knee arthroplasty (TKA)?
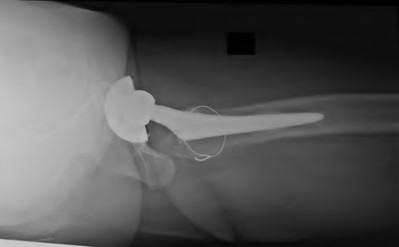
Figure 39 is a radiograph of a 72-year-old man who underwent an open reduction and internal fixation of a right femoral neck fracture. After 3 months he started to develop pain, and during the next 8 months he complained of progressive pain and shortening of the hip. What is the most appropriate treatment?

Figure 40 is the radiograph of a 68-year-old woman who has right knee pain that is limiting her activity and severe preoperative valgus deformity. During total knee arthroplasty, what pathologic features are typically encountered?
A 59-year-old active woman underwent elective total hip replacement using a posterior approach. She had minimal pain and was discharged to home 2 days after surgery. Four weeks later she dislocated her hip while shaving her legs. She underwent a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Patellar pain, subluxation, or dislocation after total knee arthroplasty can result from which of the following component orientations?
How does the risk for periprosthetic infection after total knee arthroplasty compare to risk for infection after total hip arthroplasty?
What factor is associated with a higher risk for dislocation after total hip arthroplasty?
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
A 67-year-old active man returns for routine follow up 12 years after hip replacement. He has no hip pain. Radiographs revealed a
well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate, assuming well-fixed cementless total hip components exist?
well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate, assuming well-fixed cementless total hip components exist?
What has been identified as a risk factor for total knee arthroplasty failure after previous high tibial osteotomy?
You are caring for an 18-year-old boy with severe hip arthritis and pain from a missed slipped capital femoral epiphysis. You decide that a hip arthrodesis is the best treatment option. What is the optimum position for a hip arthrodesis to maximize function and prevent complications?
What limits indications for the use of constrained liners?
What serum inflammatory marker has the highest correlation with periprosthetic joint infection?
A 68-year-old man reports hip pain 15 years after successful cementless total hip arthroplasty. Radiographs show 3 mm of linear wear of the modular acetabular liner and a retro-acetabular osteolytic lesion. Both the titanium femoral and acetabular components appear to be well fixed. The orthopaedic surgeon recommends revision of the acetabular liner and femoral head. This patient is at increased risk for
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
The range of knee mobility after total knee replacement is multifactorial and dependent upon implant design, surgical implantation accuracy, and patient-specific variables. What total knee implant design is associated with the most knee flexion after total knee replacement?
In total knee arthroplasty, in vitro testing has shown that crosslinking can diminish the rate of polyethylene wear by 30% to 80%.
What other change in material properties is possible when polyethylene is highly cross-linked?
What other change in material properties is possible when polyethylene is highly cross-linked?
What factor is associated with a high risk for developing pseudotumors after metal-on-metal hip resurfacing?
A 70-year-old man is scheduled to undergo bearing surface revision for wear and osteolysis 10 years after cementless total hip arthroplasty. The femoral head is 28 mm alumina-oxide ceramic material. The components are in good position, and there is no evidence of fixation loosening of either component by radiograph or preoperative bone scan. What outcome is associated with isolated polyethylene exchange?
A healthy, active 68-year-old woman had a total hip arthroplasty 3 months ago. She has been to the emergency department with a posterior dislocation 3 times during the last 2 months. Plain radiographs and a CT scan confirm that the acetabular component is oriented in 5 degrees of retroversion and 55 degrees of abduction.
What is the most appropriate treatment?
What is the most appropriate treatment?
What is the most common complication after a total hip replacement done through the anterior (Smith-Peterson) approach?
Figure 73 is the anteroposterior pelvis radiograph of a 58-year-old woman who reported chronic hip pain and a clunking sensation 18 months after hip surgery. Laboratory test findings are negative for infection. What is the most appropriate treatment?

Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
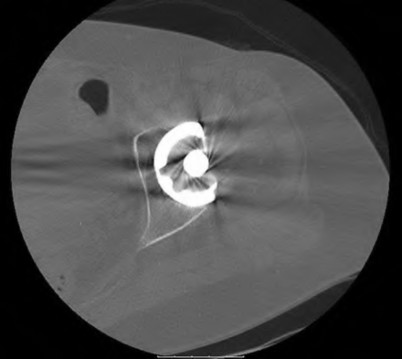
Figures 75a through 75c are the radiographs and CT scan of a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when she actively flexed her hip. She had trouble walking up stairs and getting out of her car.

A 72-year-old woman returns 3 weeks after a right total knee replacement. She has been experiencing increasing pain, swelling, and
decreasing range of motion during the last 10 days. Examination shows the knee to be more swollen and warm than what is typical at 3 weeks after surgery. The knee feels stable, but she has diffuse tenderness and range of motion is between 15 and 85 degrees. What is the most appropriate investigation(s) to diagnose the etiology of her current problem?
decreasing range of motion during the last 10 days. Examination shows the knee to be more swollen and warm than what is typical at 3 weeks after surgery. The knee feels stable, but she has diffuse tenderness and range of motion is between 15 and 85 degrees. What is the most appropriate investigation(s) to diagnose the etiology of her current problem?
What is the difference between annealed (below the melting temperature) and remelted highly crossed-linked polyethelyne?
When discussing metal on metal hip resurfacing versus metal on polyethylene total hip replacement, the surgeon should inform the patient that all of the following are disadvantages of hip resurfacing EXCEPT?
A 68-year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck with final implant insertion. What is the most appropriate treatment?
Figure 94 is the radiograph of a patient who underwent component removal, insertion of an antibiotic spacer, and recent completion of 6 weeks of intravenous antibiotic therapy. The patient's C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) have decreased and are now within defined limits. The skin is supple and the patient has a range of motion between 10 and 70 degrees.
What is the most appropriate next step?

What is the most appropriate next step?
What factor is associated with decreased range of motion to impingement?
A 68-year-old woman undergoes an uncomplicated total knee replacement through a midline incision that is extended distally to join a previous incision from a high-tibial osteotomy done 12 years previously. Despite relief of pain and appropriate knee mobility at 2 weeks, drainage continues from the distal part of the wound. What are the most appropriate next step(s) in treatment?
Three years after undergoing a metal-on-polyethylene total hip arthroplasty, a 72-year-old woman develops pain with weight bearing and rest. Hip flexion and internal rotation is associated with pain.
Radiographs show no evidence of loosening. What is the most appropriate next step in this evaluation?
Radiographs show no evidence of loosening. What is the most appropriate next step in this evaluation?
During total knee replacement with the trial components in place, the knee achieves full extension but experiences tightness in flexion with a range to only 90 degrees. What is the most appropriate action?
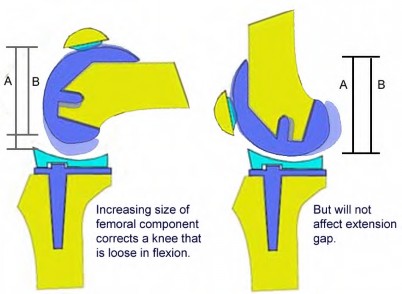
A 62-year-old man undergoes total knee arthroplasty. Preoperative radiographs are shown in Figure A. Following bone resections and placement of trial implants, the knee is stable in flexion, but cannot achieve full extension. Which of the following interventions will most likely result in a knee that is balanced in flexion and extension?
While obtaining informed consent for a lateral closing-wedge tibial osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge tibial osteotomy?
A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
A 28-year-old woman underwent a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reported improvement in her medial pain and resumed normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
A 45-year-old postmenopausal smoker with a body mass index (BMI) of 22 has had severe knee pain for the past year. The pain has been progressing and the patient is now only able to perform activities
of daily living. Knee radiographs reveal medial compartment osteoarthritis without any involvement of the patellofemoral joint or the lateral compartment. What is the contraindication for a high tibial osteotomy (HTO) in this patient?
of daily living. Knee radiographs reveal medial compartment osteoarthritis without any involvement of the patellofemoral joint or the lateral compartment. What is the contraindication for a high tibial osteotomy (HTO) in this patient?
Highly cross-linked ultra high molecular weight polyethylene has which of the following characteristics as compared to conventional polyethylene?
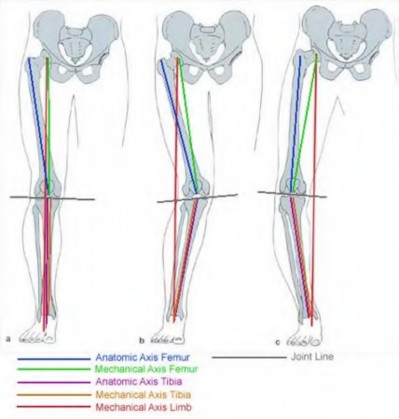
Which of the following describes the mechanical axis of a normally aligned limb?
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
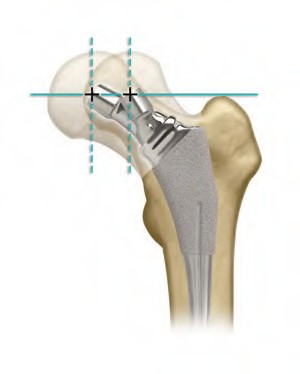
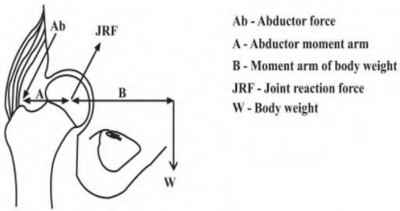
In total hip arthroplasty, which of the following techniques will lead to improved stability by increasing the abductor tension?
Significant anterior tibial translation occurs during which of the following rehabilitation exercises?
A 65-year-old female has severe knee arthritis with a significant flexion contracture and valgus deformity. In the recovery room following her total knee replacement, she is unable to dorsiflex her ankle. Management should include?
A 67-year-old female presents to the emergency department with the distal femur fracture shown in figure A. She undergoes procedure 1 shown in figures B and C. When compared to procedure 2 shown in figures D and E, which of the following is true regarding procedure 1?





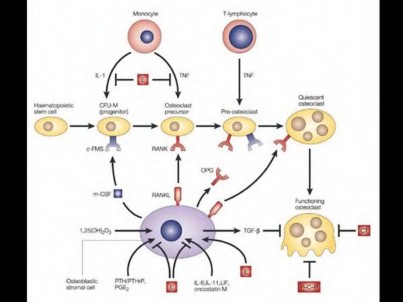
Ultra-high-molecular-weight polyethylene (UHMWPE) particles have been associated with osteoclastogenesis, a key component of osteolysis in total joint replacement. Which of the following accurately describes the expression of vascular endothelial growth factor (VEGF) and receptor activator of nuclear factor kappa-B ligand (RANKL) during UHWMPE induced osteolysis?
Figures A and B show a 65-year-old woman with a history of a well functioning right total knee done 5 years prior who presents with pain and inability to bear weight after a fall from standing height. Her midline knee incision is well healed. What is the best treatment at this time?





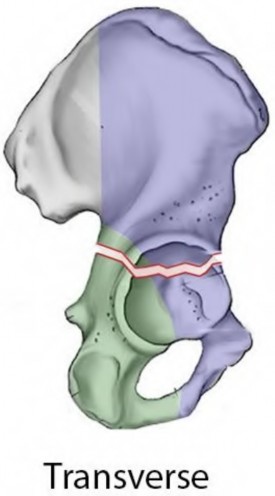
An 80-year-old female presents following a fall from standing. She was an active, independent, community ambulator prior to this event. Past surgical history is significant for a left total hip arthroplasty 10 years prior. A left hip XR is obtained and shown in Figure A. A CT is obtained and demonstrates a displaced transverse acetabulum fracture with medial cup migration. There is no evidence of femoral component loosening or fracture. There is no concern for infection and all inflammatory markers are within appropriate limits. Which treatment is most appropriate?




While trialing components during a routine total knee arthroplasty, the flexion gap is felt to be loose and the extension gap is stable. Which of the following are possible ways to treat this intraoperative instability?
A 65-year-old active female presents with medial sided knee pain of 2 years duration that has failed nonoperative modalities.
Radiographs are shown in Figure A. Which of the following variables is the strongest contraindication to unicompartmental knee arthroplasty in this patient?

Radiographs are shown in Figure A. Which of the following variables is the strongest contraindication to unicompartmental knee arthroplasty in this patient?
Which of the following complications is the primary reason for early reoperation following the procedure shown in Figure A?


Which of the following is the most common reason for reoperation following hip resurfacing in the first 6 months following the operation?

A 40-year-old male presents with chronic severe and progressively worsening right hip pain which has been intractable to conservative management. He has a history of avascular necrosis of the femoral head with subsequent collapse and development of severe osteoarthritis. After discussion of his surgical options, he elects to proceed with the procedure shown in Figure A. He presents to the emergency department 2 months later with severe groin pain and inability to bear weight. Radiographs obtained at this time are shown in Figure B. Each of the following has been shown to increase the risk for development of this complication post-operatively EXCEPT:


When comparing conventional polyethylene liners to the newer highly cross-linked polyethylene liners, all of the following are true EXCEPT for one. Which of these statements about conventional poly liners is incorrect?
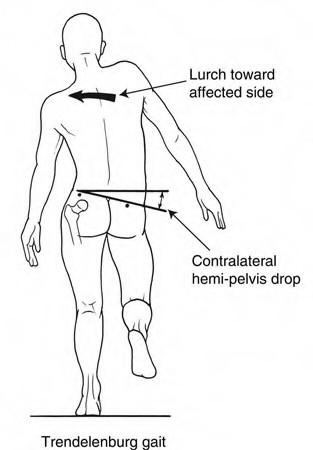
Patients display a Trendelenburg gait to compensate for weakness in which of the following muscle groups?
A 73 year-old female underwent total knee arthroplasty 10 years ago. She sustained a proximal tibial shaft periprosthetic fracture after a ground level fall. Radiographs show that the fracture involves the tibial component's stem with loosening of the tibial component. Which of the following is the most appropriate treatment?
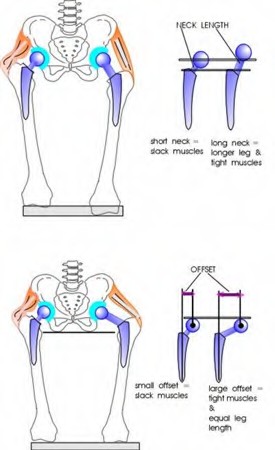
All of the following interventions help restore anatomic limb length following total hip arthroplasty EXCEPT:

Keywords