Score: 0%
ORTHOPEDIC MCQS ONLINE 013 SPORT
QUESTION 1
Quadriceps tendonitis
_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?











_Please select the most likely diagnosis listed above for each clinical situation._
-A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest failed to alleviate his symptoms. He underwent an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reported popping by his clavicle and mild pain. His clavicle demonstrated mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
1
Anterior and superior acromioclavicular joint ligaments
2
Posterior and superior acromioclavicular joint ligaments
3
Conoid ligament
4
Trapezoid ligament
DISCUSSIO-The posterior and superior acromioclavicular ligaments provide the most restraint to posterior translation of the acromioclavicular joint and must be preserved during a Mumford procedure. Anterior and superior acromioclavicular joint ligaments are the opposite of the preferred response and prevent anterior translation of the clavicle. Injuries to the conoid and trapezoid ligaments are more pronounced with grade III or higher acromioclavicular separations, with superior migration of the clavicle relative to the acromion.
_**CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9**_
-A 19-year-old female field hockey player has a right ankle injury that occurred last night during a game.The patient is on crutches and states that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination revealed discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain was elicited during palpation of the anterior talofibular ligament. What examination test should be performed to aid in this diagnosis?
5
Thompson test
--The patient is provided with a medial unloader brace that provides substantial pain relief and he is able to work while wearing the brace. After 4 months he returns to work and says that while the brace enable him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
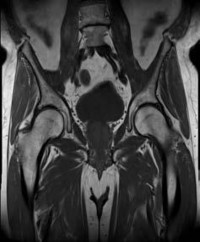
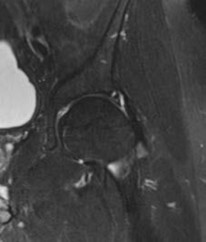
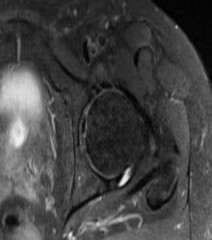
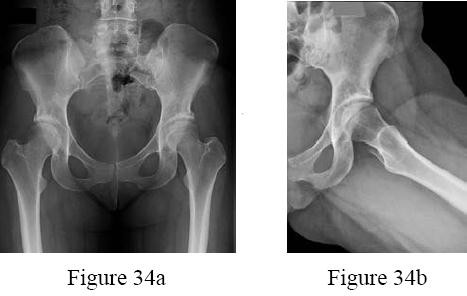
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
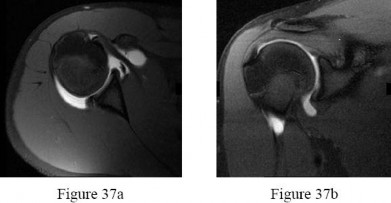
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
1) Valgus-producing high tibial osteotomy (VPHTO)
2) Repeat knee arthroscopy
3) Total knee arthroplasty (TKA)
4) Medial meniscus transplant
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1) Prior arthroscopy
2) Current smoking history
3) BMI of 22
4) Age of 40
FOR QUESTIONS 13 THROUGH 16_
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
-When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure?
1) Graft choice
2) Tunnel position
3) Tibial fixation
4) Femoral fixation
_CLINICAL SITUATION FOR QUESTIONS 18 THROUGH 20_
A 25-year-old healthy woman injured her left knee while playing professional soccer. She has never injured this knee before. Examination 2 days after the injury occurred reveals the following: a moderate effusion, a positive Lachman test result, and mild lateral tenderness. Range of motion is between 20 degrees and 70 degrees. Radiographs reveal no fracture. An MRI scan reveals a complete rupture of the anterior cruciate ligament (ACL), an effusion, and bone bruises of the lateral femoral condyle and lateral tibial plateau. No meniscal tear is seen. The patient would like to continue playing at the professional level.
--What is the next treatment step?
1) Immobilization of the knee for 6 weeks, followed by rehabilitation and delayed ACL reconstruction
2) Immediate ACL reconstruction
3) Immediate rehabilitation for 6 months followed by ACL reconstruction if the patient is unstable in a brace
4) Immediate rehabilitation with delayed ACL reconstruction (when the athlete obtains full knee range of motion)
-What is this patient’s risk for developing osteoarthritis (OA) of the knee?
1) There is no risk for development of knee OA after reconstruction of the ligament.
2) There is no risk for development of knee OA after a double-bundle ACL reconstruction.
3) There is no evidence that ACL reconstruction reduces the incidence of knee OA.
4) There is 100% likelihood that she will develop knee OA after single-bundle ACL reconstruction.
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
1) There is no significant difference in ACL anatomy between men and women.
2) A woman’s ACL has a smaller cross-sectional area.
3) The cross-sectional area of a woman’s ACL is larger.
4) The intercondylar notch is wider in women than in men.
FOR QUESTIONS 18 THROUGH 20_
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.
-Figure 21 is the radiograph of a 31-year-old man who had left shoulder pain after a fall during a snow boarding jump. Residual displacement of 5 mm after closed reduction is most likely to result in which of the following?
1) Nonunion
2) Osteonecrosis
3) Altered rotator cuff mechanics
4) Normal shoulder function
-What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates?
1) Separate players with infections in a separate locker room or changing area.
2) Treat teammates of the infected player with prophylactic antibiotics.
3) Cover any skin lesions with occlusive dressing during sporting activity.
4) Ban players with infections from any team event.
-Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
1) Forward elevation in the scapular plane
2) External rotation and abduction
3) Flexion, adduction, and internal rotation
4) Flexion and abduction
_**CLINICAL SITUATION FOR QUESTIONS 24 AND 25**_
During the third quarter of a high school football game, a 16-year-old running back gets tackled and limps off the field. During the initial sideline evaluation, he has tenderness on the right iliac crest. He is a little dizzy, has a headache, and tells you, “I need to get back in the game to help the team score before halftime.”
-How can this scenario be managed most effectively?
1) Initiate rest, ice the iliac crest, and return to play when he is not limping.
2) Initiate rest, ice the iliac crest, and return to play after 20 minutes.
3) Keep the player on the sideline, perform a cognitive evaluation, and repeat the physical assessment.
4) Keep the player out of the game and send him emergently to the hospital for imaging.
-Sideline examination of this patient showed no cervical pain or tenderness; motor and sensory function were normal; and his pupils were equal, round, and reactive. He was alert and oriented to the score of game, time on the clock, and current quarter of play. His iliac crest had mild tenderness but no swelling or crepitus. The player states that he has a slight headache and is no longer dizzy. What is the most appropriate treatment?
1) Return him to the game and observe his play closely.
2) Do not return to the game and do not allow play for the remainder of the season.
3) Do not return to the game and begin a graduated return-to-play protocol for future games.
4) Perform a sideline noncontact exercise testing examination and return him to the game if he is asymptomatic.
FOR QUESTIONS 24 AND 25_
Although this player limps off the field, the fact that he felt dizzy, had a headache, and did not initially recognize that he was playing in the third quarter indicates that he sustained a concussion. The player should be kept out of the game until a cognitive examination and repeat physical assessment is completed.Even if his physical symptoms have resolved, a certain period of time has expired, or he states that he is“ready,” he should not be returned to play prior to this assessment. Sending the patient to an emergency department should be considered only after this assessment and appropriate initial sideline treatment is initiated. The Consensus Statement on Concussion in Sport recommends that no athlete with concussion symptoms be returned to same-day play. This patient still has a slight headache, but even if this resolved he should not return to the game. Adolescents and high school athletes may have neurophysiological deficits that may not be evident on the sideline, or they may have a delayed onset of symptoms. A graduated return to play for future games is recommended.
_CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29_
A 32-year-old woman has a 2-year history of progressively worsening right groin pain that is exacerbated by activity. She reports no traumatic injury and an extensive work-up by her gynecologist has ruled out an intrapelvic source of her pain. The patient is a recreational athlete and exercises regularly in the gym.The pain is preventing her from performing these activities. She reports no catching or locking symptoms.Her examination reveals a physically fit female (BMI of 20) with limited right hip range of motion. She has no tenderness to palpation around the hip. While lying supine and bringing her hip into progressive flexion with internal rotation and adduction, her groin pain is reproduced. She has normal limb lengths and demonstrates weakness secondary to pain with hip flexion on the affected side.
-What is the most likely cause of this patient’s groin pain?
1) Femoroacetabular impingement (FAI)
2) Osteoarthritis of the sacroiliac joint
3) Intra-articular loose body
4) Trochanteric bursitis
-The patient is enrolled in physical therapy for 6 weeks with little improvement of her hip symptoms.What is the next most appropriate diagnostic test to determine the presence of an associated acetabular labral tear in this patient?
1) Diagnostic arthroscopy of the hip
2) MRI scan of the hip
3) MRI arthrogram of the hip
4) Ultrasound of the hip
-The study obtained in confirms the presence of an anterosuperior acetabular labral tear and pincer morphology of the acetabulum. What is the most likely location of a chondral injury associated with these findings?
1) Posteroinferior acetabulum
2) Posterosuperior acetabulum
3) Femoral head above the fovea
4) Femoral head below the fovea
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
1) Suture anchor repair of the labral tear and no bony resection
2) Suture anchor repair of the labral tear and bony resection of the pincer lesion
3) Debridement of the labral tear and bony resection of the pincer lesion
4) Debridement of the labral tear with no bony resection of the pincer lesion
FOR QUESTIONS 26 THROUGH 29_
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
_**CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32**_
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.
-What examination findings are most consistent with the pathology seen in the radiographs?
1) Pain with resisted hip flexion
2) Pain with a half sit-up, plus tenderness at the pubic ramus
3) Pain with a combination of hip flexion, adduction, and internal rotation
4) Tenderness to palpation at the greater trochanter
-What is the most likely diagnosis for the source of this patient’s pain?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Hip flexor strain
4) Athletic pubalgia
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
1) Significant cartilage loss on the acetabulum
2) Labral tear
3) Femoral neck stress fracture
4) Tendonopathy of the rectus femoris
FOR QUESTIONS 30 THROUGH 32_
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
-A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always “feels loose.” Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization?
1) Range of motion might be slightly better after an arthroscopic procedure.
2) Rate of recurrent instability is lower after an arthroscopic procedure.
3) Rates of return to work are higher after an arthroscopic procedure.
4) Rates of return to sports are higher after an arthroscopic procedure.
-Figures 34a and 34b are the radiographs of a 38-year-old woman who had increasing left hip pain with activity. She noted no lower back or buttock pain and no pain along her lateral thigh. The pain usually only bothers her with running and cycling.
Nonsteroidal anti-inflammatory drugs helped initially but are not relieving her pain now. Examination with the patient supine reveals pain with internal and external rotation of her hip
with her hip and knee in an extended position. With her hip flexed to 90 degrees, she has internal rotation only to neutral, but full external rotation. What is the most likely diagnosis?
1) Cam-type femoroacetabular impingement
2) Pincer-type femoroacetabular impingement
3) Intra-articular loose body
4) Snapping psoas tendon
-A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
1) Hamstring autograft
2) Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
3) Revision ACL reconstruction and posteromedial corner reconstruction
4) Revision ACL reconstruction and posterolateral corner reconstruction
-A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling “on top of his knee,” and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap.
Examination reveals significant swelling of his prepatellar bursa,with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient?
1) Initiate oral antibiotics for 7 days.
2) Reaspirate the bursa and inject a corticosteroid.
3) Recommend padding the patella for kneeling and ice.
4) Perform an open bursectomy and start intravenous antibiotics.
_CLINICAL SITUATION FOR QUESTIONS 37 AND 38_
An 18-year-old right-hand-dominant college freshman who is a third baseman has pain in his right shoulder after using his outstretched right arm for support while diving to catch a low line drive. He describes pivoting on his right hand and arm while reaching out to make the catch with his left-hand glove. He had pain in his shoulder but was able to finish the game with some pain while throwing. Five days later, he experiences popping pain deep in his shoulder that has improved since the injury but continued to be bothersome deep in the shoulder with higher-velocity throwing. Examination demonstrated decreased internal rotation, posterior pain with cross-body adduction and posteriorly directed force, and full rotator cuff strength. Radiograph findings were normal. After 6 weeks of physical therapy (PT), his range of motion has improved but he continues to experience deep pain with therapy. Examination shows symmetric range of motion and posterior pain with the jerk test and Kim test. His rotator cuff is strong.Figure 37a Figure 37b
-What is the next step in treatment?
1) Continued PT
2) Subacromial injection
3) CT scan
4) MRI arthrogram
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
1) Open reduction internal fixation (ORIF)
2) Rotator cuff repair
3) Labrum repair
4) Chondroplasty
FOR QUESTIONS 37 AND 38_
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
A high school athlete sustained a noncontact injury to his right knee. He says that during a football game he felt a pop and his leg gave way. He attempted to continue to play but was unable secondary to pain.Five days after the injury, radiographs of his right knee do not reveal any abnormalities. On examination,he has an effusion on the injured side and no joint line tenderness. His range of motion is full extension to 110 degrees of flexion. At 20 degrees of flexion, he has increased anterior translation compared to the contralateral, uninjured left side. At 90 degrees of flexion, the tibia does not translate posteriorly. As his knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a“clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
1) In extension, the medial tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau reduces.
2) In extension, the medial tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the medial tibial plateau subluxates.
3) In extension, the lateral tibial plateau is reduced; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau subluxates.
4) In extension, the lateral tibial plateau is subluxated; as an internal rotation/valgus force is applied in conjunction with flexion, the lateral plateau reduces.
_**CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 42**_
A 9-year-old boy was injured while playing soccer. His examination revealed painful range of motion between 5 degrees and 75 degrees. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality.
-What is the next diagnostic step?
1) Repeat radiographs while the patient is weight bearing
2) Ultrasound of the lower extremity and calf
3) Stress radiographs
4) CT scan
-What is the most likely area of injury?
1) Femoral attachment of the medial collateral ligament
2) Tibial attachment of the medial collateral ligament
3) Hypertrophic zone of the growth plate
4) Proliferative zone of the growth plate
FOR QUESTIONS 40 THROUGH 42_
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
1) Psoriasis
2) Tinea corporis
3) Herpes simplex virus
4) Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA)
_CLINICAL SITUATION FOR QUESTIONS 44 AND 45_
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
-Range of motion of the knee is between 0 degrees and 70 degrees. What is the most appropriate treatment option?
1) Nonweight-bearing activity with crutches
2) Microfracture of the chondral defect
3) Immediate anterior cruciate ligament (ACL) reconstruction
4) Delayed ACL reconstruction
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
1) increased laxity.
2) no differences in long-term results.
3) increased risk for graft failure.
4) lower Knee Injury and Osteoarthritis Outcome Scores (KOOS).
FOR QUESTIONS 44 AND 45_
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
-Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
1) onset most often by age 30.
2) a temporary state of neuronal and axonal derangement.
3) manifestations of affect such as apathy, irritability, and suicidal ideation.
4) absence of gross pathological brain changes upon autopsy.
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
1) Rotator interval
2) Infraspinatus
3) Anterior band of the inferior glenohumeral ligament
4) Posterior band of the inferior glenohumeral ligament
_**CLINICAL SITUATION FOR QUESTIONS 48 AND 49**_
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
-What is the most appropriate treatment?
1) Switch to oral trimethoprim-sulfamethoxazole double-strength twice per day for 10 to 14 days
2) Switch to oral ciprofloxacin 500 mg twice per day for 10 to 14 days
3) Begin cefazolin 1 gram intravenously (IV) every 8 hours for 7 to 10 days
4) Irrigation and debridement with empiric IV antibiotic coverage
-Assuming that the lesion can be covered appropriately and there is no drainage from the lesion, when should the patient be allowed to safely return to wrestling?
1) When the absence of pain is reported by the wrestler for 3 consecutive days
2) When 72 hours of antibiotics have been administered and there is no extension of the lesion for 48 hours
3) When laboratory values are within defined limits and the patient remains afebrile for 3 days
4) When the lesion has decreased in size by 50%
FOR QUESTIONS 48 AND 49_
This patient has cellulitis, which is typically caused by group A Streptococcus or Staphylococcus. The patient’s lack of improvement with first-line antibiotics is concerning for methicillin-resistant Staphylococcus aureus (MRSA) infection. MRSA cellulitis is becoming more prevalent in young athletes,and a high index of suspicion is required to provide appropriate intervention during this
aggressive disease process. The diagnosis is typically made clinically without the use of cultures. Oral trimethoprimsulfamethoxazole (a sulfonamide-class drug) double strength twice daily for 10 to 14 days or doxycycline (a tetracycline-class drug) 100 mg twice daily for 10 to 14 days are recommended for first-line treatment of suspected MRSA cellulitis. There is no indication to proceed with irrigation and debridement; however, if the patient develops a soft-tissue abscess or the underlying joint becomes involved, this would be an appropriate intervention. Switching the athlete to an IV cephalosporin (cefazolin) is not likely to be effective against the presumed resistant bacteria.
Ciprofloxacin (a fluoroquinolone-class drug) is effective against many bacteria, but not MRSA. The current recommendation for wrestlers with cellulitis is that return to competition be allowed after 72 hours of antibiotic treatment if there has been no extension of the cellulitis for 48 hours, the lesion can be covered, and there is no drainage from the lesion. The other responses are not current recommendations for return to competition.
-A 19-year-old linebacker underwent a coracoid transfer procedure for recurrent anterior glenohumeral instability. At his 1-week postsurgical check-up, his incision is doing well; however, he reports numbness over the lateral aspect of his forearm. What nerve may have been injured during his surgery?
1) Axillary
2) Median
3) Musculocutaneous
4) Radial
-What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA?
1) Beta-lactamase
2) Penicillin-binding protein 2a
3) Panton-Valentine leukocidin (PVL)
4) Staphylococcus cassette chromosome (SCCmec) type I
_CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 54_
A 13-year-old baseball player fell while rounding second base 2 days ago. He said it felt like his knee buckled when he turned toward third base. He could not finish the game, but was able to bear weight with a limp. He has had no previous knee injuries, but now complains of pain in his right knee. Initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. He was otherwise ligamentously stable. No other noteworthy physical findings were found.
-What is the next treatment step?
1) Radiographs
2) Arthroscopy
3) MRI scan
4) Duplex ultrasound
-What do the radiographs shown in Figures 52a and 52b reveal?
1) Medial femoral chondyle physeal widening
2) Osseous or osteochondral loose fragment
3) Osgood-Schlatter disease
4) Patella nondisplaced fracture
-Figures 52c and 52d show the proton density fat-saturated MRI scans. Treatment at this stage includes arthroscopy and
1) early functional rehabilitation.
2) proximal realignment alone.
3) attempted internal fixation.
4) medial collateral ligament (MCL) repair.
FOR QUESTIONS 52 THROUGH 54_
This patient’s examination indicates a patellar or peripatellar knee injury. Initial evaluation with radiographs will assess for fracture, subluxation, or osteochondral injury. Examination findings did not demonstrate a need for emergent surgery, an MRI scan, or an ultrasound, so radiographs are the initial diagnostic imaging choice. Radiographs show an osseous or osteochondral loose fragment.
There is no evidence of obvious nondisplaced fracture or physeal changes. In suspected patella dislocation or subluxation with loose fragment seen on radiographs, an MRI scan is indicated. Lateral release alone is seldom indicated in a knee that was normal before injury. Acute proximal realignment has not been shown to alter long-term outcomes for first-time dislocators. The examination and MRI scan did not indicate a need for MCL repair. Closed reduction of the osteochondral fragment would not be indicated or appropriate for this injury. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed.
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
1) Compartment syndrome
2) Plate breakage
3) Neurologic injury
4) Proximal tibiofibular joint disruption
_**CLINICAL SITUATION FOR QUESTIONS 56 THROUGH 58**_
Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
-What examination test is most likely to reveal abnormal findings?
1) Pivot shift test
2) Quadriceps active test
3) Patellar apprehension test
4) External rotation recurvatum test
-What is the most appropriate treatment?
1) Delayed ligament reconstruction
2) Physical therapy and functional bracing
3) Immediate ligament repair
4) Immediate ligament reconstruction
-What is the most likely mechanism of injury?
1) External rotation
2) Posterior translation
3) Hyperextension and varus
4) Anterior translation and internal rotation
FOR QUESTIONS 56 THROUGH 58_
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
1) Achilles rupture
2) Gastrocnemius strain
3) Calcaneal apophysitis
4) Os trigonum syndrome
_CLINICAL SITUATION FOR QUESTIONS 60 AND 61_
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
-What is the most significant risk factor for the development of little leaguer’s shoulder in this scenario?
1) Recent increase in the number of pitches
2) Gender (male)
3) Glenohumeral internal rotation deficit
4) Genetic factors
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
1) Screw fixation of the epiphysis
2) Arthroscopic debridement
3) A shut-down period until the boy is asymptomatic, and gradual return to pitching via a throwing program
4) An intra-articular cortisone injection
FOR QUESTIONS 60 AND 61_
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.
-is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal.What is the main function of the structure delineated by the black asterisks?
1) Resist anterior translation during knee flexion
2) Resist posterior translation during knee flexion
3) Resist rotatory loads during knee flexion
4) Resist rotatory loads during knee extension
-A 25-year-old wrestler has been experiencing increasing left knee pain since his last professional cage fight. He complains of both pain and instability on the medial side of his left knee. Examination reveals a grade 3 Lachman and pseudolaxity with valgus stress. Dial test findings are normal. Radiographs show medial degenerative changes and 5 degrees of varus alignment. What is the most appropriate treatment?
1) Rehabilitation with vibration-platform weight-bearing squats
2) Anterior cruciate ligament (ACL) reconstruction with autograft bone-tendon-bone
3) High-tibial osteotomy (HTO)
4) HTO plus ACL reconstruction at the same time
-What is an example of cognitive rest after concussion?
1) Playing chess
2) Increasing reading
3) Working online
4) Limiting video games
_**CLINICAL SITUATION FOR QUESTIONS 65 THROUGH 67**_
Figure 65 is the radiograph of a 24-year-old man who had left knee pain after sustaining a twisting injury while playing Ultimate Frisbee. On examination, he had a large effusion with tenderness over the lateral joint line. Pivot shift testing results were positive. Prone dial testing results at 30 degrees and 90 degrees were negative. An MRI scan shows a tear of the anterior cruciate ligament (ACL).
-Based on the radiograph, the attachment for which structure has been disrupted?
1) Iliotibial band
2) Popliteus tendon
3) Lateral meniscus
4) Lateral capsular ligament
-Compared with a transtibial technique, what effect will drilling the femoral tunnel through the anteromedial portal have?
1) Produces a longer femoral tunnel
2) Improves visualization while drilling
3) Should be performed at 90 degrees of knee flexion
4) Allows for independent access to the anatomic femoral insertion
-The patient requests anatomic double-bundle ACL reconstruction. Compared with transtibial singlebundle ACL reconstruction, anatomic double-bundle ACL reconstruction is more likely to
1) restore improved knee kinematics.
2) allow for earlier return to sports.
3) result in better clinical outcomes scores.
4) be associated with lower surgery cost.
FOR QUESTIONS 65 THROUGH 67
The radiograph shows a Segond fracture, an avulsion fracture involving the lateral capsular ligament.
This radiographic finding has been associated with ACL rupture in 75% to 100% of cases. Drilling the femoral tunnel through the anteromedial portal allows for independent access to the native femoral attachment. Fiber orientation is more oblique than with a transtibial technique and more closely resembles that of the native ligament. Double-bundle reconstruction attempts to duplicate native ACL anatomy.Biomechanical studies have shown that double-bundle reconstruction more
closely reproduces normal knee kinematics; however, this technique does not offer a clear advantage in terms of clinical outcomes.The iliotibial band inserts onto Gerdy’s tubercle. The popliteus tendon originates from the lateral femoral condyle. The lateral meniscus attaches near the intercondylar eminence at the anterior and posterior meniscal roots. Recent advances in ACL reconstruction focus on restoring the native ACL anatomy.Studies have determined that a knee flexion angle of 110 degrees is optimal to avoid blowout of the back wall and injury to the lateral structures while drilling.
Femoral tunnel length is typically shorter than with a transtibial approach and decreases with higher-flexion angles. Double-bundle reconstruction is associated with higher surgical costs because of the need for additional fixation and, in the case of allograft reconstruction, a second graft.
-A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability.Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-tomoderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain?
1) Distal femoral osteotomy
2) Unicompartmental knee replacement
3) High tibial osteotomy (HTO), lateral closing wedge
4) HTO, medial opening wedge with decreased tibial slope
_**RESPONSES FOR QUESTIONS 69 THROUGH 71**_
