Orthopedic Spine Review | Dr Hutaif Spine Surgery Revie -...
Updated: Feb 2026
54 Views
Key Medical Takeaway
For anyone wondering about ORTHOPEDIC MCQS ONLINE 012 SPINE, When a 56-year-old presents with leg weakness and an unsteady, wide-based gait without discrete lower extremity motor weakness, even with mild lumbar stenosis, the next appropriate action is MRI of the thoracic and cervical spine to evaluate for spinal cord compression. This helps resolve a common diagnostic res question a yearold patient’s symptoms can present, especially when lumbar findings are insufficient.
Score: 0%
ORTHOPEDIC MCQS ONLINE 012 SPINE
QUESTION 1
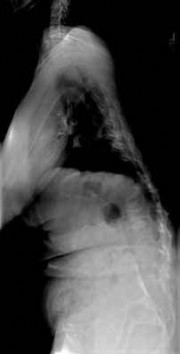
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in
both lower extremities. The patient is slow in getting up from a seated position and has an unsteady widebased gait. An MRI scan of the lumbar spine is shown in Figure
1
What is the next most appropriate course of action?
2
Electromyography and nerve conduction velocity studies of bilateral lower extremities
3
Multilevel lumbar laminectomy
4
MRI of the thoracic and cervical spine
5
MRI of the brain
The patient is having gait problems suspicious for spinal cord compression. MRI of the thoracic and cervical spine should be performed to evaluate for spinal cord compression. Reports of leg
weakness in the absence of discrete motor weakness on manual testing, and the appearance of an unsteady wide-based gait are more consistent with myelopathy as a cause of the gait difficulty rather than lumbar stenosis. Although the MRI scan of the lumbar spine shows multilevel spinal stenosis that is mild to moderate, it does not clearly explain the patient’s signs and symptoms. Electromyography and nerve conduction velocity studies of the lower extremities are unlikely to add significantly to the diagnosis.Epidural steroid injections are not indicated. Lumbar decompression is unlikely to help the patient because the source of the patient’s problem does not originate in the lumbar spine. MRI of the brain could be considered as a secondary imaging study if the cervical and thoracic MRI scans fail to identify an obvious cause for gait instability.
QUESTION 2
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include
1
10% decrease in amplitude, 50% decrease in latency.
2
10% decrease in amplitude, 50% increase in latency.
3
0% loss of amplitude, transient increase in latency.
4
50% decrease in amplitude, 10% increase in latency.
5
50% decrease in amplitude, 10% decrease in latency.
The established criteria for interpreting a significant change are 50% decrease in signal amplitude, 10% latency increase, and/or a complete loss of potential. Intraoperative spinal cord monitoring during spinal surgery generally consists of a combination of monitoring modalities.Somatosensory-evoked potentials in combination with intraoperative electromyography can provide adequate coverage of sensory and motor components of spinal cord and nerve root function. Significant changes in evoked potential waveform characteristics can reflect dysfunction of the ascending somatosensory system.
QUESTION 3
A 44-year-old man was involved in a low speed rear-end motor vehicle accident 4 weeks ago. He predominantly reports pain in the back of the neck, with occasional radiation into the trapezius region
bilaterally. He denies any extremity pain. The pain has not changed in intensity, but is worse with neck range of motion. Cervical spine radiographs were negative for acute osseous trauma or instability. What is the next most appropriate step in management?
1
Continued observation
2
Cervical epidural injections
3
Nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and physical therapy
4
Cervical facet blocks
5
Cervical MRI
The patient was involved in a low speed rear-end collision and sustained a whiplashtype injury, with management most often being nonsurgical. After 4 weeks of persistent pain, continued observation is not reasonable. Studies have shown that treatment including NSAIDs, activity modification and a brief duration of physical therapy allows for improved outcomes after whiplash-type injuries when compared with observation alone. An MRI scan of the cervical spine is not indicated at this time and represents an unnecessary expense. Cervical epidural and facet injections are not indicated in the treatment of patients with whiplash injuries.
QUESTION 4
A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The surgeon elects to proceed with L5-S1 laminectomy and posterior instrumented fusion after reduction of the spondylolisthesis. If a postoperative neurologic deficit develops, what structure has most likely been affected?
1
L4 nerve root
2
L5 nerve root
3
S1 nerve root
4
Genitofemoral nerve
5
Cauda equina
The L5 nerve root is especially vulnerable and prone to injury after the reduction of spondylolisthesis in patients with mid-and high-grade isthmic spondylolisthesis. The genitofemoral nerve is more commonly injured during anterior retroperitoneal approaches to the lumbar spine. Injury to the cauda equina often leads to bowel and bladder dysfunction and lower extremity weakness and is uncommon after reduction maneuvers.
QUESTION 5
A 46-year-old man has a recurrent disk herniation on the left side at L4-5 and has had persistent radicular symptoms for 3 months without neurologic deficit. His previous surgery was performed 13 months ago.What is the best method of surgical treatment?
1
Posterior lumbar interbody fusion
2
Anterior lumbar interbody fusion
3
Revision diskectomy
4
Artificial disk replacement
5
Interspinous process spacer
The patient is a candidate for a revision diskectomy. Outcomes of revision diskectomy are nearly as good as those reported for primary diskectomy. Reduction in leg pain is expected. An indication for fusion would be a concomitant instability at the planned surgical level. Though controversial, artificial disk replacement might be considered if there is a significant component of diskogenic pain without instability.
However, disk replacement is not the first choice of treatment in this case. Interspinous process spacers are not currently indicated in this situation.
QUESTION 6
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis?
1
Diffuse idiopathic skeletal hyperostosis
2
Ankylosing spondylitis
3
Ossification of the posterior longitudinal ligament
4
Rheumatoid arthritis
5
Degenerative cervical stenosis
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis.The cord compression is noted to be not only
at the disk levels but also at the midvertebral body levels,and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of
Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1-C2 on flexionextension radiographs and subaxial subluxations.
QUESTION 7
An 18-year-old man who sustained a lumbar fracture-dislocation with an associated complete spinal cord injury 6 weeks ago underwent instrumented posterior thoracolumbar fusion a few days after the injury. While at a rehabilitation facility, routine postoperative surveillance radiographs are obtained (Figures 11a
through 11d). What is the most appropriate next step in management? ---
1
Observation alone with continued rehabilitation of the spinal cord injury
2
Thoracolumbosacral orthosis bracing for 3 months
3
Revision and extension of the posterior instrumentation and fusion
4
Anterior lumbar corpectomy and fusion
5
Anterior/posterior lumbar decompression and fusion
The patient has sustained a traumatic spondylolisthesis at the level below the caudal instrumented level, likely not appreciated at the index surgery. Surveillance radiographs indicate that there is significant translation in the lumbar spine on sitting, indicating an unstable injury. The lack of significant bony involvement indicates that the injury is predominantly through the anterior and posterior ligamentous complexes, and thus is unlikely to stabilize with nonsurgical management. Because the patient reduces almost completely on lying supine, the most appropriate course of action is extension of the posterior fusion to include the level of the instability. Because the patient has a complete spinal cord injury below the level of the thoracic fracture, decompression is not indicated.
QUESTION 8
What is the predominant type of collagen found in the nucleus pulposus of the intervertebral disk?
1
Type I
2
Type II
3
Type V
4
Type VI
5
Type XII
Types I and II collagen are the predominant types of collagen found in the intervertebral disk. Type I collagen is present in the highest concentration in the annulus fibrosus and type II collagen in the nucleus pulposus. Type V collagen is present in small concentration in the annulus fibrosus. Type VI collagen is a non-fibrillar, short-helix collagen found in both the annulus and nucleus. Type XII is present in the annulus fibrosus only. Figure 14What clinical scenario is most consistent with the MR image of the L4-L5 disk level shown in Figure 14?
1. # Left L4 nerve root radiculopathy
2. # Right L5 nerve root radiculopathy
3. # Bowel and bladder dysfunction
4. # Arachnoiditis
5. # Symptomatic pseudomeningocele
DISCUSSION: The MRI scan reveals a foraminal disk herniation originating from the L4-L5 disk space that has migrated into the foramen compressing the left L4 nerve root. There is no evidence of compression of the right L5 nerve root. Bowel and bladder dysfunction are not associated with L4-mediated nerve function. There is no evidence of arachnoiditis or pseudomeningocele. PREFERRED RESPONSE: 1
QUESTION 9
A 23-year-old man is evaluated in the emergency department after a diving accident. Radiographs reveal bilateral jumped facets at C6-7. Examination reveals no motor function below the C7 level. There is some maintained sensation in the lower extremities. What is the patient’s current grade on the ASIA (American Spinal Injury Association) impairment scale?
1
ASIA A
2
ASIA B
3
ASIA C
4
ASIA D
5
ASIA E
The American Spinal Injury Association (ASIA) provides a standard method of measurement of spinal cord injury. The ASIA impairment scale is based on a
comprehensive motor and sensory examination. An ASIA A grade is ascribed to a patient with an injury with no motor or sensory preservation below the injury. An ASIA B grade is defined as no motor preservation below the level of injury but some sensory preservation below the injury level. An ASIA C grade is defined as a motor function grade of less than 3 below the injury level. An ASIA D grade is defined as a motor function grade of greater than 3 below the injury level. An ASIA E grade is defined as a normal neurologic examination.
QUESTION 10
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching.Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a widebased gait, intrinsic ---
wasting, and a postive Hoffman’s sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment?
1
Anterior diskectomy without fusion at C4-C5
2
Epidural injections
3
Anterior diskectomy and fusion at C4-C5 and C5-C6
4
Multilevel laminectomy and fusion
5
Multilevel posterior foraminotomies
The patient has classic symptoms of myelopathy with upper motor neuron signs on examination. His symptoms have been present for years, and are getting worse. The cervical spine MRI scan shows spinal stenosis with multilevel spondylosis causing spinal cord compression at multiple levels. With
the longstanding duration of the patient’s signs and symptoms, combined with involvement of multiple levels in the cervical spine, posterior multilevel laminectomy and fusion is the best treatment option. Two-level anterior diskectomy and fusion would address the two areas of most severe narrowing,but it would fail to decompress the other stenotic areas which also require decompression. Posterior cervical foraminotomies would only address radicular symptoms, which are not present in this patient, and would not succeed in decompression of the spinal cord. Cervical epidural injections are not indicated for myelopathy symptoms, and may in fact place this patient at risk for neurologic deterioration.
QUESTION 11
Of the following signs or findings, which one is most consistent with the diagnosis of cervical radiculopathy?
1
Spurling sign
2
Hoffman sign
3
Clonus
4
Inverted brachioradialis reflex
5
Babinski sign
The Spurling sign is elicited by extending the neck and having the patient rotate his or her head toward the side of the symptoms; reproduction of symptoms, including those of radicular pain,suggests cervical nerve root compression as a contributing factor. The remaining signs and clinical findings are seen with cervical myelopathy. The Hoffman sign is elicited by flicking the terminal phalanx of the third or fourth finger; a positive response is seen as reflex flexion of the terminal phalanx of the thumb. The inverted brachioradialis reflex is seen when the brachioradialis tendon is tapped and a diminished brachioradialis reflex is noted but reflex contraction of the finger flexors is seen.
QUESTION 12
A 42-year-old woman has a 3-week history of acute lower back pain with radiation into the left lower extremity. There is no history of trauma and no systemic symptoms are noted. Examination reveals a positive straight leg test at 25 degrees on the left side. Motor testing reveals mild weakness of the gluteus maximus and weakness of the gastrocnemius at 3/5. Sensory examination reveals decreased sensation along the lateral aspect of the foot. Knee reflex is intact; however, the ankle reflex is absent. MRI scans show a posterolateral disk herniation. The diagnosis at this time is consistent with a herniated nucleus pulposus at what level?
1
L1-2
2
L2-3
3
L3-4
4
L4-5
5
L5-S1
The patient’s history and examination findings are consistent with a lumbar disk herniation at the L5-S1 level. Weakness of the gastrocnemius and gluteus maximus are consistent with an S1 lumbar radiculopathy. Nerve root tension signs are also
consistent with a disk herniation at L5-S1, which typically affects the traversing S1 nerve root.
QUESTION 13
Back injuries occur in approximately 2% of the work force every year,
resulting in workers’ compensation costs of more than $20 billion. What percentage of workers, with symptoms severe enough to require work absence, return to work within 12 weeks?
1
80% to 90%
2
70% to 80%
3
60% to 70%
4
50% to 60%
5
40% to 50%
In adults, 70% to 85% will experience an episode of low back pain at some period during their life. Most recover quickly and without residual functional deficits. Of those patients with symptoms severe enough to require absence from work, 60% to 70% return within 6 weeks and 80% to 90% return within 12 weeks. After 12 weeks of symptoms, return to work is much slower.
QUESTION 14
In the treatment of fungal osteomyelitis of the spine, what is the preferred agent?
1
Cefazolin
2
Vancomycin
3
Combination treatment with isoniazid, ethambutol, rifampin, and pyrazimide
4
Trimethoprim-sulfamethoxazole
5
Amphotericin B
Amphotericin B is a broad-spectrum antifungal that is commonly used as the firstline agent for treatment of fungal infections of the spine. Cefazolin, vancomycin, and trimethoprimsulfamethoxazole are better suited for the treatment of bacterial infections. Combination treatment with
isoniazid, ethambutol, rifampin, and pyrazimide is used for the treatment of tuberculous infections.
QUESTION 15
Which of the following indicates resolution of a postoperative wound infection?
1
C-reactive protein (CRP) has normalized and erythrocyte sedimentation rate (ESR) is improving
2
CRP and ESR remain elevated
3
CRP and ESR are below normal
4
CRP has improved to the same degree as the ESR has improved
5
CRP remains elevated after the ESR has normalized
Khan and associates in a retrospective review found that CRP was more responsive and normalized with resolution of infection, whereas the ESR can remain elevated in the presence of a normal CRP. Since the normal range of ESR and CRP usually begins at 0, a level that is below normal is not likely to be found.
QUESTION 16
Two weeks after being treated for a nondisplaced type II odontoid fracture with a halo fixator, a 78-yearold man reports left anterior pin site pain. On examination, the left anterior pin fixation site is tender andfocal erythema with mild loosening is noted. The patient denies fevers, chills, or any other constitutional symptoms. What is the most appropriate course of action at this time?
1
Removal of the halo and soft collar placement
2
Retightening of the pin and treatment with oral antibiotics
3
Removal of the left anterior pin
4
Treatment with oral antibiotics
5
Surgical treatment of the type II odontoid fracture with posterior C1-C2 fusion
One of the most common complications of halo device fixation is pin loosening. In adults, pin loosening can occur in up to 36% of patients and most commonly occurs in the anterior pins. If there is no infection present, a loose pin can be managed by simply retightening the screw one to two turns. Infection at the pin site is the second most common complication of the halo device, occurring in about 20% of patients.
Infection can be either superficial or deep. Superficial infections can be treated with oral antibiotics and wound care at the pin site. Pin loosening does not always occur with pin site infection. The infection can be treated with or without removing the pin. If a deep infection develops, the pin should be removed. If an abscess develops, parenteral antibiotics and drainage of the abscess may be necessary. A new pin may be placed in a new position. Other complications from halo fixation include skin breakdown and intracranial penetration.
QUESTION 17
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time?
1
Urgent admission to the hospital for surgical intervention
2
Immediate MRI of the lumbar spine as an outpatient
3
Anti-inflammatory medications and activity modification
4
Caudal epidural steroid injection
5
Electromyography
In the absence of any severe progressive neurologic deficits or other red flags, the most appropriate management for an acute lumbar disk herniation is nonsurgical care. Conservative treatments such as limited bed rest, anti-inflammatory medications, and judicious use of pain medications are appropriate in this clinical situation. Up to 90% of patients will experience a resolution of symptoms without the need for surgical intervention within a 3-month window. In the acute setting, with no neurologic deficits, immediate MRI of the lumbar spine is neither beneficial nor warranted. Likewise,without signs of an acute deficit, emergent surgical intervention and caudal epidural steroid injections are not needed.
QUESTION 18
What factor is associated with the highest risk for in-hospital complications for patients undergoing a lumbar fusion for degenerative spondylolisthesis?
1
Hospital size
2
Gender
3
Race
4
Age
5
One comorbidity
Age and having three or more comorbidities is associated with a higher rate of complications in patients undergoing a lumbar fusion for lumbar degenerative spondylolisthesis. Race,gender, and hospital size have not been found to be associated with higher complication rates.
---
QUESTION 19
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group?
1
Less than 10%
2
20% to 25%
3
50% to 60%
4
75% to 80%
5
Greater than 95%
The MRI findings reveal age-related degenerative changes in the cervical spine, which is a very common finding in the adult population. Boden and associates evaluated cervical spine MRI findings on 63 asymptomatic subjects, and found that the prevalence of having at least one degenerative disk was approximately 57% in those older than age 40 years.
QUESTION 20
Figures 28a and 28b show the posteroanterior and lateral radiographs of a 38-year-old woman with adult idiopathic scoliosis. She reports symptoms of longstanding lower back pain, progressive loss of height,and the inability to stand upright at the end of the day. What radiographic finding has been found to most closely correlate with symptoms of lower back pain?
1
Thoracic scoliosis
2
Thoracic hypokyphosis
3
Lumbar disk degeneration
4
Thoracolumbar kyphosis
5
Lumbar hyperlordosis
Adult idiopathic scoliosis and adult “de-novo” scoliosis can present with a number of symptoms that relate to associated degenerative findings
such as stenosis or spondylolisthesis. In the absence of these associated conditions, increased levels of pain in patients with scoliosis has been found to most closely correlate with sagittal imbalance. Thoracolumbar and lumbar curves and thoracolumbar kyphosis have both been found to closely correlate with increased symptoms and lower healthrelated quality of life (HRQL) outcome scores. Thoracic scoliosis, thoracic hypokyphosis,
lumbar hyperlordosis,and lumbar disk degeneration have not been found to correlate with increased symptoms.
QUESTION 21
A 75-year-old woman is undergoing a T10-S1 lumbar decompression and fusion for severe degenerative scoliosis. During the deformity corrective maneuver, intraoperative neuromonitoring revealed a sustained 80% decrease in somatosensory-evoked potential (SSEP) amplitudes. Appropriate lead placement and functioning has been reconfirmed by the neuromonitoring technician. The anesthesiologist has ruled out any anesthetic-related or hemodynamic issues. What is the next appropriate step in management?
1
Completion of the surgical procedure with continued monitoring
2
Reversal of the corrective maneuver and consideration of a wake-up test
3
Administration of high dose corticosteroids intraoperatively
4
Removal of all instrumentation
5
Discontinue monitoring
The most appropriate management is discontinuation of the spinal instrumentation procedure, including releasing any distractive forces. Given the ongoing changes, proceeding with the procedure and/or resetting the baseline amplitudes is inadvisable. If the SSEPS amplitudes fail to return in a timely fashion, it is strongly recommended to consider a wake-up test. The purpose of intraoperative neuromonitoring is to provide a real-time assessment of the functional integrity of the central and peripheral nervous systems during surgery to prevent iatrogenic injury.
Sustained decreased SSEP amplitudes of greater than 50% and transcranial electric Motor-Evoked Potentials (tceMEP) amplitudes of greater than 75% are indicative of a possible significant intraoperative neurologic complication. Although intraoperative corticosteroids might be helpful, especially in the event of a continued SSEP change, the most important next step would be to release the distractive forces and reevaluate the patient’s neurologic status.
QUESTION 22
Which of the following is most commonly associated with the use of bisphosphonates in the setting of
metastatic breast cancer?
1
Reduction of skeletal-related events by 30% to 40%
2
Jaw osteonecrosis in 15% of patients
3
Pain improvement in 20% of patients
4
Acceleration of hypercalcemic symptoms and signs
5
Accelerated bone destruction
Bisphosphonate therapy in breast cancer patients is indicated for the correction of hypercalcemia and the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during longterm bisphosphonate therapy.
QUESTION 23
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her healthrelated quality of life (HRQL) outcomes?
1
Correction of the thoracolumbar curve
2
Sagittal balance
3
Coronal balance
4
Correction of the thoracic curve
5
Shoulder balance
Sagittal balance is the most reliable predictor of clinical symptoms and HRQL outcomes on the SRS 29, SF-12, and Oswestry Disability Index. Coronal balance, shoulder balance,curve magnitude, and degree of curve correction are less critical in determining clinical symptoms and outcomes.
QUESTION 24
Pedicle subtraction osteotomies (PSO) are commonly performed in the lumbar spine to treat sagittal imbalance. What is the most common complication following a PSO in the lumbar spine?
1
Pseudarthrosis
2
Nerve root injury
3
Spinal cord injury
4
Aortic injury
5
Dural tear
The rate of pseudarthrosis at 5-year follow-up is 29%, with most occurring at the thoracolumbar junction cephalad to the site of the PSO. The rate of postoperative neurologic deficits is 11%, with 2.8% resulting in permanent deficits. Spinal cord injury is rare because the PSO is typically performed in the lumbar spine below the conus.
QUESTION 25
What is the most commonly involved level for brachial plexus stretch injuries or “stingers” in younger athletes involved in collision sports?
1
C3-4
2
C4-5
3
C5-6
4
C6-7
5
C7-T1
The most commonly involved level for brachial plexus traction injuries in young athletes is C5-6, ostensibly due to the greater mobility in the midcervical spine. “Stingers” in older athletes may be due to foraminal stenosis in combination with extension and nerve root compression.
QUESTION 26
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery?
1
Pedicle screw misplacement
2
Patient positioning
3
Spinal cord ischemia
4
Retractor placement
5
Hypertension
Patient positioning that results in local nerve compression, plexus traction, or improper neck alignment is the most common non-anesthetic-related cause of changes in intraoperative neurophysiologic monitoring data during spinal surgery. Pedicle screw malpositioning, spinal cord ischemia, and retractor placement are all less common causes. Hypotension, not hypertension, can be a cause of intraoperative neurophysiologic changes.
---
QUESTION 27
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? ---
1
Improvement in her pain and sensory symptoms following surgery but may have residual bladder dysfunction
2
Decreased pain following surgery; sensory deficits and bladder function are not likely to improve
3
No change in her symptoms following surgery
4
Complete resolution of pain and will have normal sensation and bladder function following surgery
5
Improvement in her pain and complete return of bladder function following surgery; sensation may not return
The patient with cauda equina syndrome should be taken to surgery urgently to provide the best chance of symptom resolution. However, many studies indicate that patients with cauda equine syndrome do not return to a completely normal status even following urgent surgery. Whereas pain is typically relieved after surgery, other deficits, especially bladder and sexual dysfunction, may persist.Particularly in light of the patient’s severe saddle anesthesia, she may have a poor prognosis for recovery of normal bladder function.
QUESTION 28
What complication is associated with the use of epidural morphine and steroid paste after laminectomy?
1
Surgical site infection
2
Arachnoiditis
3
Urinary retention
4
Disk space infections
5
Nerve irritation
Kramer and associates conducted a retrospective review during an
“epidemic” period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound débridement, and an 11% rate of surgical site complications. There is no evidence in the literature verifying the incidence of postoperative urinary retention and arachnoiditis.
QUESTION 29
Giant cell tumors of the spine can metastasize to other areas of the body. They most likely metastasize to which of the following areas?
1
Brain
2
Lung
3
Liver
4
Kidney
5
Colon
Giant cell tumors of the spine can metastasize to other areas of the body. Donthineni and associates identified seven cases (three females and four males) of lung metastases from a total of 51 cases of giant cell tumors of the spine (13.7%). Four of the seven patients had a spine recurrence after previous treatments and the rest developed recurrences later. The treatments for the lung nodules consisted of metastectomy in two and chemotherapy in six patients. At the latest follow-up (ranging from 18 to 126 months), two had died of the disease, two had no evidence of the disease, and three were alive with disease. This series shows a higher metastatic rate from spine giant cell tumor as compared with those from the extremities, but the overall behavior and treatment outcomes of the lung metastases are similar. Tunn and associates also showed a predilection for pulmonary metastatic lesions.
QUESTION 30
A positive straight leg raising sign is when pain radiates distal to the knee when the affected leg is passively elevated. The increased tension generally occurs between
1
0 degrees to 30 degrees.
2
30 degrees to 70 degrees.
3
45 degrees to 90 degrees.
4
60 degrees to 90 degrees.
5
90 degrees.
A positive straight leg raising sign causes pain radiating distal to the knee when the nerve is under tension. This increased tension generally occurs between 30 degrees and 70 degrees of passive elevation.
---
QUESTION 31
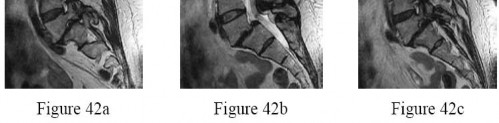
Figures 42a through 42c show the MRI scans of a 56-year-old woman with progressively worsening low back and bilateral lower extremity pain. Based on these images, what muscle or muscle group would be expected to be weak on physical examination?
1
Quadriceps
2
Hamstrings
3
Hip adductors
4
Extensor hallucis longus
5
Gastrocnemius
Whereas subjective complaints of leg pain are common among patients seeking surgical treatment for spondylolisthesis, documented neurologic deficit or radiculopathy is seen less frequently.Subjective decreases to light touch over the dorsum of the foot and mild weakness of the extensor halluces longus are the most common neurologic abnormalities, correlating with L5 nerve root irritation as seen with L5-S1 spondylolisthesis. Many patients with spondylolisthesis report hamstring tightness; however,these structures are not usually weak. Quadriceps and tibialis anterior weakness is seen with L4 nerve root irritation. The gastrocnemius is generally weak in S1 nerve root syndromes.
QUESTION 32
Which of the following is the best method of treatment for a dominant vertebral artery injury during an occipitocervical fusion?
1
Packing the area with Surgicel
2
Stenting
3
Proximal and distal ligation
4
Direct repair
5
Screw placement to control bleeding
In dominant vertebral artery injury (usually left sided), direct repair is the best method of treatment despite the technical demands of the exposure and microvascular repair. Direct repair can minimize immediate and delayed risks of injury and ischemia. Aggressive packing can result in delayed hemorrhage or fistula formation. Ligation-associated morbidities such as cerebellar infarction, cranial nerve palsies, hemiplegia, and even a mortality rate of 12% have been reported. Screw placement is usually sufficient to control bleeding, but should be considered as a last resort in cases of dominant vertebral artery injury.
QUESTION 33
Which of the following materials has the highest modulus of elasticity?
1
Cortical bone
2
Cobalt-chrome
3
Ceramic
4
Titanium
5
Stainless steel
Young’s modulus of elasticity is a measure of the stiffness of a material and its ability to resist deformation. This is the slope of the stress/strain curve in the elastic range. The highest modulus is ceramic, followed by: cobalt-chrome alloy, stainless steel, titanium, and then cortical bone.
QUESTION 34
Morphogenic factors such as bone morphogenetic protein-2, bone morphogenetic protein-7, and transforming growth factor-beta have been postulated to play a role in reversing the process of intervertebral disk degeneration. These molecules work via what mechanism?
1
Increase cell proliferation leading to increased cell numbers within the disk and enhanced matrix synthesis
2
Inhibit the catabolic effects of matrix metalloproteinases
3
Increase the chondrogenic phenotype of disk cells and increase matrix synthesis
4
Promote increased end plate vascularity and nutritional diffusion within the disk
5
Block receptors for tumor necrosis factor-alpha and interleukin-1
Bone morphogenetic protein-2, bone morphogenetic protein-7, and transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of disk matrix.Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
QUESTION 35
Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at 5 to 10 years after lumbar fusion?
1
5.5% at 5 years and 75.5% at 10 years
2
10.1% at 5 years and 65.2% at 10 years
3
16.5% at 5 years and 36.1% at 10 years
4
26.5% at 5 years and 56.1% at 10 years
5
49.2% at 5 years and 15.1% at 10 years
Ghiselli and associates described a rate of symptomatic degeneration at an adjacent segment warranting either decompression or arthrodesis to be 16.5% at 5 years and 36.1% at 10 years based on a Kaplan-Meier analysis. Question 49 Halo treatment for preadolescent children typically requires the use of which of the following?
1. # 4 to 6 pins with an insertional torque of 1 to 5 in-lb
2. # 4 to 6 pins with an insertional torque of 4 to 6 in-lb
3. # 4 to 6 pins with an insertional torque of 6 to 8 in-lb
4. # 8 to 12 pins with an insertional torque of 1 to 5 in-lb
5. # 8 to 12 pins with an insertional torque of 4 to 6 in-lb
DISCUSSION: The complication rate with halo vest treatment in children is reported to be as high as 68% in contrast to a 36% complication rate in adults. These complications include not only pin tract infections,but also skull penetration. Multiple pins allow for the early removal of pins without fixation consequences should pin site infections begin to develop. Moreover, there is significant variability in the insertional torque applied by a variety halo pin torque wrenches, including those from the same manufacturer.
Consequently, the use of a large number of pins (8 to 12) placed a very low insertional torque (1 to 5 in-lb) in children is recommended. A CT scan of the head should also be considered to assess for the thickest areas of the skull suitable for pin application. PR: 4
QUESTION 36
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy?
1
Sagittal alignment
2
History of diabetes mellitus and tobacco use
3
Performance of an uninstrumented fusion (ie, no plate and screws)
4
Use of allograft (instead of autograft)
5
Fusion at the C3-C4 level
Various factors affect the pseudarthrosis rate in patients who undergo anterior cervical decompression and fusion. Patient factors, including history of smoking and history of diabetes mellitus,have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category,there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
QUESTION 37
A 60-year-old woman has an 8-month history of left-sided arm and neck pain. Her symptoms developed insidiously. The patient reports burning dysesthesias in the left forearm and middle finger. Examination reveals weakness of the left triceps and wrist flexors. An axial MR scan at the level of the C6-7 disk is shown in Figure 51.
The patient wishes to avoid surgery if possible and asks about epidural steroid injections. What is the likelihood of long-term relief of her symptoms following a steroid injection? ---
1
5% to 10%
2
10% to 20%
3
30% to 40%
4
50% to 70%
5
80% to 90%
The patient has a C7 radiculopathy in the left upper extremity. Several studies indicate that relief of radicular symptoms for periods of longer than 1 year can be achieved in 50% to 70% of
patients following administration of epidural steroids.
QUESTION 38
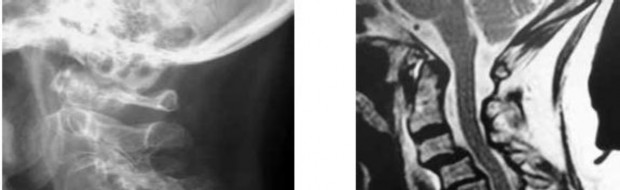
A 60-year-old woman has progressive neck pain, upper extremity pain, and paresthesias. A lateral cervical spine radiograph and an MRI scan are shown in Figures 52a and 52b. What is the most likely underlying diagnosis? ---
1
Osteomyelitis
2
Ankylosing spondylitis
3
Age-related degenerative changes
4
Rheumatoid arthritis
5
Previous cervical decompression
The radiograph and sagittal T2-weighted MRI scan show multilevel degenerative changes and subaxial subluxations with anterolisthesis at C3-C4 and C4-C5 and retrolisthesis at C5-C6. In addition, there is evidence of midcervical kyphosis. Such findings are often seen in patients with rheumatoid arthritis. Patients with osteomyelitis typically show increased signal intensity in the disks and vertebral bodies. Patients with ankylosing spondylitis typically show ankylosis of the disks and vertebral
bodies. Age-related degenerative changes typically manifest as degenerative disk disease with occasional single-level spondylolisthesis, but not typically multilevel spondylolisthesis, as seen in this patient. The spinous processes are intact; these changes do not appear to be postoperative.
QUESTION 39
A 66-year-old woman reports chronic mild low back pain. Over the last 3 years, she has noticed worsening buttock and posterior leg pain with standing and walking. Sitting seems to improve the pain.She also reports numbness in both legs with walking. An MRI scan and standing radiographs of the lumbar spine are shown in Figures 53a through 53c. She has undergone two epidural injections with good, but short-term relief. Further treatment to alleviate this patient’s symptoms should consist of which of the following? ---
1
Manual therapy
2
Multilevel laminectomy
3
Facet injections
4
L4-5 laminotomy
5
Laminectomy and fusion
The patient reports symptoms that are classic for neurogenic claudication secondary to lumbar spinal stenosis. Nonsurgical management has failed to provide relief, thus a surgical approach is a reasonable treatment option at this point. Studies have shown significant benefit in patients with lumbar stenosis who choose to undergo surgical treatment. Manual or manipulative therapy is unlikely to provide relief. Facet injections are not effective for neurologic symptoms. An L4-5 laminotomy will not
adequately address the patient’s pathology. In the absence of instability on imaging studies, arthrodesis is not indicated.
QUESTION 40
When evaluating a patient with a lumbar burst fracture, the integrity of the posterior ligamentous complex must be evaluated. Which of the following is a complete and accurate list of the components of the posterior ligamentous complex?
1
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules
Supraspinous ligament, interspinous ligament, and ligamentum flavum
4
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joints
5
Supraspinous ligament, interspinous ligament, ligamentum flavum, facet joint capsules, facet joints, and the posterior longitudinal ligament
DISCUSSION: The components of the posterior ligamentous complex are the supraspinous ligament,interspinous ligament, ligamentum flavum, and the facet joint capsules. Recent studies have emphasized the importance of the posterior ligamentous complex. The Thoracolumbar Injury Classification and Severity Score (TLICS) is a classification system that allows for efficient and effective classification of thoracolumbar spine injuries. It evaluates three characteristics of the injury:
QUESTION 41
In the treatment of chondrosarcomas of the spine and sacrum, which of the following is a significant factor associated with a worse prognosis with respect to local control and/or survival?
1
Lower histologic tumor grade of the lesion
2
Increasing patient age
3
Negative excisional margins
4
Initial biopsy done at the tumor center
5
Spine location as opposed to pelvic location of the tumor
Bergh and associates examined 69 patients with chondrosarcoma and looked at prognostic factors affecting local recurrence and survival. There were 61 conventional chondrosarcomas, grades1-3 (with 13 arising in a preexisting osteochondroma) and eight grade 4 chondrosarcomas (seven dedifferentiated and one mesenchymal). The overall local recurrence rate was 27%, and the estimated overall 5-and 10-year survival rates were 72% and 67%, respectively. In contrast, the observed local recurrence rate was 3% (1 patient) in 31 patients whose conventional chondrosarcomas were resected with adequate surgical margins; 90% of these patients survived and most of them (26 of 31 or 84%)were continuously disease free. Significant factors associated with a worse prognosis with respect to local control and/or survival were high histologic tumor grade, increasing patient age, primary surgery outside of a tumor center, incisional biopsy versus a noninvasive diagnostic procedure, and inadequate surgical margins. Lee and associates also looked at factors affecting outcome and found that predictors of metastasis and death included local recurrence, a pelvic location of the tumor, a tumor that was more than 100 cubic centimeters in size, a ploidic abnormality (aneuploidy coupled with a high mean DNA index), a histologic grade of 3, and a dedifferentiated type of tumor (p < 0.001).
QUESTION 42
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
1
lateral placement, directly within the temporalis muscle.
2
within the lateral third of the superior orbital rim.
3
lateral to the superior orbital rim.
4
medial third of the superior orbital rim.
5
lateral between the temporalis muscle and zygomatic temporal nerve.
Halo fixation is the most rigid form of cervical orthosis but complications can arise from improper placement of the fixation pins. A relatively safe zone for anterior pin placement is located 1 cm above and within the lateral third of the superior orbital rim. This position avoids the supraorbital and supratrochlear nerves over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication.
QUESTION 43
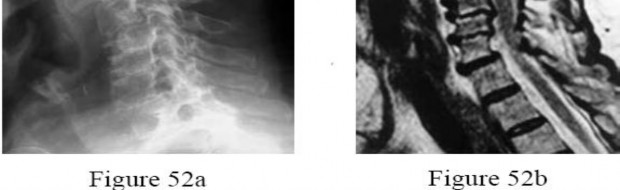
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? ---
1
Referral to a pain clinic for epidural injections
2
Activity modification and anti-inflammatory medications
3
Urgent hospital admission followed by hemilaminotomy and diskectomy
4
Hemilaminotomy and diskectomy scheduled as an elective procedure
5
Posterior laminectomy and fusion
The patient has an L5-S1 disk herniation, which has a favorable prognosis without surgical intervention. Most acute lumbar disk herniations resolve with nonsurgical management. The most appropriate course of initial treatment should be analgesics and activity modification, followed by rehabilitation as the symptoms allow. Although the MRI scan indicates a large disk herniation, he has no symptoms or signs that
would warrant urgent surgical decompression. Planned elective discectomy should be considered only if nonsurgical management fails to provide relief. Epidural injections could be considered if the initial course of treatment fails to give the patient significant relief. Posterior laminectomy and fusion is not indicated without the presence of instability.
QUESTION 44
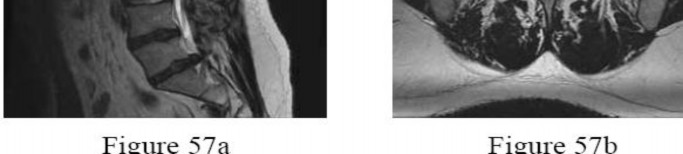
An 80-year-old man who was involved in a fall from ground height is evaluated in the emergency department for head lacerations and mild neck pain. Examination reveals only mild tenderness of the posterior neck region with some limitation of motion. Neurologic examination is normal. Radiographs of the cervical spine are shown in Figures 58a and 58b. What is the next most appropriate step in management for this patient? ---
1
Admission for 24-hour observation for possible intracranial hematoma
2
Discharge with a soft collar and follow-up in 24 hours
3
CT of the cervical spine
4
Repeat radiographs of the cervical spine, including flexion and extension views
5
Hard cervical collar for 6 weeks
The patient has radiographic findings compatible with diffuse idiopathic skeletal hyperostosis (DISH) of the cervical spine. Characteristics of DISH include flowing, non-marginal osteophytes at four or more levels. Patients with DISH develop a significant loss of flexibility of the spine. The spine acts more as a long bone with minimal force needed to create unstable fractures. Any minor trauma in patients with DISH should be
worked up aggressively to rule out occult fracture. In this patient, radiographs fail to clearly rule out a fracture; therefore, CT of the cervical spine is indicated.Without a suspicion of history of a head injury, admission specifically for a possible intracranial hematoma is not warranted. The more concerning injury in a patient with DISH is occult neck fracture. Treatment with a soft or hard collar is not advised until a fracture is ruled out. Repeat radiographs are unlikely to show any occult fractures, and flexion and extension views would not be advised in a patient with a suspected vertebral fracture.
QUESTION 45
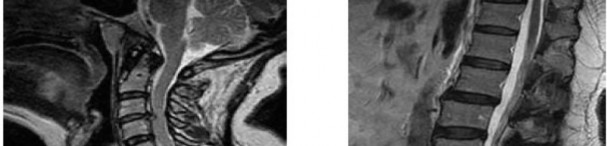
A 40-year-old woman is admitted to the hospital with a history of new-onset right lower extremity weakness resulting in frequent falls. She reports that a few weeks prior to the onset of the lower extremity symptoms, she experienced an episode of acute back pain, which has since resolved. Examination reveals 1-2/5 strength in the right hip flexors, abductors, and quadriceps. There is 0-1/5 strength noted in the right ankle plantar and dorsiflexors. Deep tendon reflexes are hyperactive in the lower extremities and there is clonus on dorsiflexion of the right ankle. The patient has a positive Babinski sign on the right side. The patient denies neck or arm symptoms, and the upper extremity neurologic examination is within normal limits. Figures 59a and 59b show the MRI scans of the patient’s cervical and lumbar spine. What is the
next most appropriate step in management? ---
1
Multilevel anterior cervical diskectomy and fusion
2
Cervical laminectomy
3
Lumbar laminectomy
4
Lumbar laminectomy and fusion
5
Thoracic MRI
Symptoms of thoracic disk herniation may present in one of three distinct patterns:axial pain, radicular pain, or myelopathy. This patient demonstrates obvious upper motor neuron signs,including lower extremity hyperflexia, clonus, and a positive Babinski sign; therefore, the next most appropriate step is a MRI scan of the thoracic spine. Thoracic disk herniations presenting with axial pain usually involve the mid to lower thoracic region. The pain is usually worsened with activity and improved with rest. Radicular pain syndromes are usually described as starting in the back and radiating anteriorly in a band-like pattern to the anterior chest wall. The pain and paresthesias generally follow a dermatomal distribution. The MRI scan of this patient’s cervical spine demonstrates spondylotic changes;however, she denied neck or upper extremity symptoms and more importantly, has a normal neurologic examination. There are degenerative changes involving the lumbar spine, but these cannot explain the upper motor neuron findings.
---
QUESTION 46
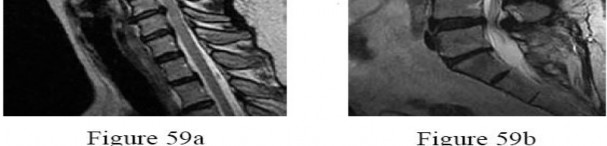
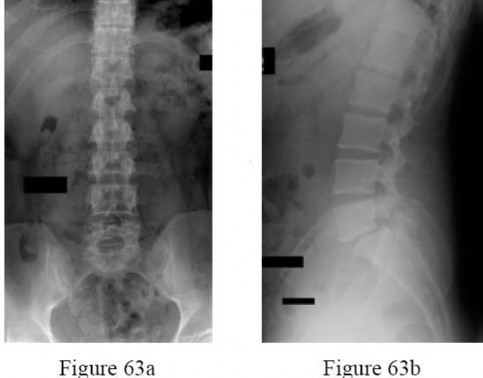
Which of the angles depicted in Figure 60 has been found to most closely correlate with a patient’s lumbar lordosis, thoracic kyphosis, and overall sagittal alignment?
1
A
2
B
3
C
4
D
5
A and D
Angle A represents pelvic incidence (PI), a constant anatomic relationship between the pelvis and sacrum. Angle B represents pelvic tilt, and angle C represents sacral slope. Pelvic tilt and sacral slope can change depending on the rotation of the pelvis. Pelvic incidence has been found directly correlate with the magnitude of lumbar lordosis and thoracic kyphosis because it determines the angle at the base
of the spine (the lumbosacral junction). To obtain sagittal balance, the remainder of the spine compensates, resulting in the degree of lumbar lordosis and thoracic kyphosis to maintain an upright posture. Thus, PI must be considered in the evaluation of sagittal balance and potential reconstructive procedures. Angle D represents the T1 angle.
QUESTION 47
A 38-year-old man reports right upper extremity pain that radiates from his neck to his anterior arm,dorsoradial forearm, and into the index finger. Examination reveals weakness of the biceps muscle group and loss of his brachioradialis reflex on that side. At which level is he most likely to have a right-sided cervical disk protrusion on an MRI scan?
1
C4-C5
2
C5-C6
3
C6-C7
4
C6 vertebral body
5
Far lateral C6-C7
The patient has a typical right C6 radiculopathy based on his history and physical examination. A posterolateral disk protrusion at the C5-C6 level is mostly likely to cause a C6 radiculopathy because the C6 nerve roots exit just above the C6 pedicle and therefore would be compressed by a right-sided C5-C6 disk protrusion. In contrast to the lumbar spine, far lateral disk protrusions are not typically described in the cervical spine.
---
QUESTION 48
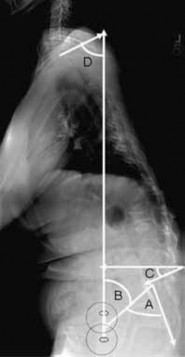
Figures 63a and 63b show the radiographs of a 38-year-old man who reports low back and bilateral lower extremity pain. The spondylolisthesis is best classified as which of the following?
1
Pathologic
2
Isthmic
3
Acquired
4
Degenerative
5
Dysplastic
Spondylolisthesis can be classified into five types. Type I, dysplastic, occurs at the lumbosacral junction as a result of congenital abnormalities of the upper sacrum and/or the arch of L5.Type II, isthmic, refers to those involving a lesion in the pars interarticularis. Type IIA, lytic, represents fatigue fractures of the pars. Type IIB describes those with elongated, but intact pars. Type IIC describes those that are a result of an acute fracture of the pars. Type III, degenerative spondylolisthesis, results from longstanding intersegmental disease. Type IV, traumatic, refers to those resulting from fractures in regions other than the pars, such as the pedicles. Type V, pathologic, refers to spondylolisthesis resulting from generalized or local bone disease. The radiographs demonstrate type II, isthmic spondylolisthesis.
QUESTION 49
Which of the flowing trajectories is preferred for placement of C1 lateral mass screws?
1
7.5 degrees lateral and 5 degrees cephalad
2
7.5 degrees medial and 10 degrees cephalad
3
10 degrees medial and 22 degrees cephalad
4
10 degrees lateral and 22 degrees cephalad
5
20 degrees medial and 22 degrees caudal
The C1 lateral mass can safely accommodate screw fixation. Trajectory of 10 degrees medial and 22 degrees cephalad was safely applied in a series of 50 patients.
Postoperative CT scans confirmed the safe trajectory. The benefit of lateral mass screws is that they can be safely placed despite the existence of an anomalous vertebral artery that could preclude the safe placement of transarticular screws.
QUESTION 50
Which of the following tumors is considered highly vascular?
1
Thyroid
2
Breast
3
Colon
4
Prostate
5
Lung
Preoperative embolization is often used for highly vascular lesions such as renal andthyroid metastases.
QUESTION 51
A 50-year-old man fell from a height of 10 feet and sustained an axial loading injury to the cervical spine.He reports neck pain and right upper extremity weakness and has weakness in the lower extremities.An MRI scan is shown Figure 67. What imaging study should be obtained next to further evaluate this patient?
1
Cervical spine flexion and extension radiographs
2
AP radiograph of the cervical spine
3
CT of the cervical, thoracic, and lumbar spine
4
Electromyography and nerve conduction velocity studies of the upper extremities
5
MRI of the lumbar spine
The MRI scan shows a C7 burst fracture. A CT scan of the cervical spine will allow for optimal evaluation of this C7 burst fracture. Specifically, it will provide additional osseous detail and will assist with the detection of additional fractures,
including those of the posterior elements. Additional CT imaging of the thoracic and lumbar spine is required to rule out concommitant injuries (which may be present in 10% to 15% of patients). Anteroposterior and lateral cervical spine radiographs would be a good option for further evaluation but are not included in the available choices here.
Cervical spine flexion and extension radiographs should not be obtained in a patient who is known to have a relatively unstable spine and a neurologic deficit. Electromyography and nerve conduction velocity studies are best used to evaluate for cervical radiculopathy secondary to degenerative abnormalities and are usually not indicated in the acute trauma setting.
QUESTION 52
Which of the following actions increases radiation exposure to patients and personnel when using fluoroscopy?
1
The use of lead glasses, thyroid shield, and a lead apron with a equivalent lead thickness of 0.25 mm
2
Orienting the cathode ray tube beneath the patient with the image intensifier receptor as close to the patient as possible
3
Limiting the beam on time to only what is clinically important
4
The use of continuous fluoroscopy to ensure proper placement of implants
5
Orienting the beam in the opposite direction of the working team and keeping the team outside a 6-foot radius from the fluoroscopy machine
Continuous fluoroscopy and cineradiography exposes the patient and personnel to markedly increased levels of direct and scatter radiation exposure.
Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient,scatter radiation exposure to the personnel is minimized.
QUESTION 53
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down.Proprioception is maintained. What is the most likely diagnosis at this time?
1
Anterior cord syndrome
2
Central cord syndrome
3
Brown-Sequard syndrome
4
Posterior cord syndrome
5
Spinal shock
Incomplete cord syndromes include anterior cord syndrome, Brown-Sequard syndrome,central cord syndrome, and posterior cord syndrome. The anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception as seen in this patient. The Brown-Sequard syndrome involves an ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. The posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain and light touch, with loss of proprioception and temperature sensation below the level of the lesion. The central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness.
Spinal shock is the period of time, usually 24 hours, after a spinal injury characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury.
QUESTION 54
What is the most common physical finding in myelopathic patients?
1
Babinski sign
2
Hoffman sign
3
Hyperreflexia
4
Clonus
5
Ataxic gait
The Hoffman sign is the most common finding, occurring in 80% of myelopathic patients,and it is more common with increasing severity of the myelopathy. The prevalence of hyperreflexia has been shown to be no different from the prevalence in individuals without myelopathy. Sustained clonus and Babinski signs have been shown to occur in only one third of the patients with myelopathy.
QUESTION 55
What is the most common presenting problem in patients with cauda equina syndrome?
1
Urinary retention
2
Urinary incontinence
3
Saddle numbness
4
Lower extremity numbness and weakness
5
Back and leg pain
In one recent retrospective cohort study of 42 patients with cauda equina syndrome, 83% had low back pain at presentation, 90% had radicular lower extremity pain, 60% had urinary retention, and 55% had urinary incontinence. Objective findings at presentation included 55% with leg weakness, 62% with sensory deficit, 62% with absent ankle jerk reflexes, 76% with perianal sensory deficit, and 50% with decreased rectal tone.
QUESTION 56
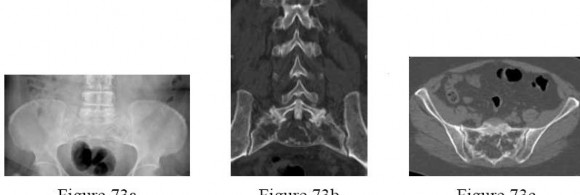
A 61-year-old woman has a history of a left thigh melanoma that was widely resected approximately 12 years ago. The patient also has a history of nephrolithiasis and has just undergone an abdominal CT scan for evaluation of her kidneys. The patient was incidentally found to have a lytic lesion of the sacrum. A radiograph is shown in Figure 73a. CT scans are shown in Figures 73b through 73d. Open biopsy was performed and the biopsy specimen is shown in Figure 73e. What is the most appropriate management? ---
1
En bloc excision of the sacrum and lesion
2
Both radiation therapy and chemotherapy
3
Embolization of the vascular supply to the lesion
4
Chemotherapy as the initial treatment, followed by surgical resection
5
Bisphosphonate therapy
The patient is asymptomatic from the sacral lesion, but has a history of a malignant lesion,so the suspicion is high that the sacral lesion is a recurrence or a metastatic lesion. The radiograph and CT scans show a lytic lesion within the osseous margins of the sacrum, and the histologic section shows no malignant cells. The diagnosis is Paget’s disease, which is typically treated medically. Bisphosphonate treatment is typical, but is currently controversial as to whether it helps more than just controlling the local symptoms. Radiographic features vary but can reveal cortical thickening, coarse trabeculae, and sclerotic or enlarged vertebral bodies. The sacrum is typically involved.
Histologically there is “mosaic” appearing bone with numerous random intersecting lines, overly active osteoclasts and/or osteoblasts, and fibrous tissue replacement of marrow.
The specimen shows disordered appearance of the bone and the multiple intersecting lines.
QUESTION 57
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
1
Nicotine impairs osteoblast activity, thus interfering with bone remodeling.
2
The effects of smoking on bone healing are multifactorial and not yet fully understood.
3
The vasoconstrictive and platelet-activating properties of nicotine inhibit fracture healing.
4
Nicotine inhibits the function of fibroblasts, red blood cells, and macrophages.
5
Hydrogen cyanide inhibits oxidative metabolism at the cellular level.
Tobacco smoking is now the leading avoidable cause of morbidity and mortality in the United States. The musculoskeletal effects of smoking have been implicated in osteoporosis, low back pain, degenerative disk disease, poor wound healing, and delayed fusion and fracture healing. A number of studies have demonstrated the relationship between smoking and development of pseudarthrosis.Numerous studies have been performed to offer an explanation of the mechanism mediating this effect.Whereas all of the above have been postulated as explanations, more recent studies have demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood. Question 76 Which of the following is the least common primary tumor of the spine?
1. # Osteosarcoma
2. # Hemangioma
3. # Osteoid osteoma
4. # Eosinophilic granuloma
5. # Giant cell tumor
DISCUSSION: Osteoid osteoma, aneurysmal bone cysts, hemangiomas, eosinophilic granuloma, and giant cell tumors are more commonly seen in the spine as opposed to chondrosarcomas, Ewing’s sarcoma,and osteosarcomas which are uncommon in the spine. Osteosarcoma is the second most common primary tumor of bone, but spinal involvement is rare, accounting for 3% of all osteosarcomas. PREFERRED RESPONSE: 1
QUESTION 58
Which of the following tumors rarely metastasizes to the spine?
1
Colon
2
Breast
3
Lung
4
Renal
5
Thyroid
Metastatic tumors are the most common tumors found in the spine. Up to 75% of all bony metastases occur in patients with carcinoma of the breast, lung, kidney, prostate, thyroid, and multiple myeloma. Carcinoma of the colon rarely metastasizes to the spine.
QUESTION 59
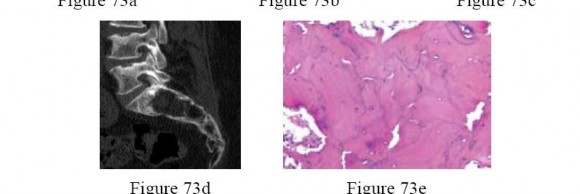
Which of the following would be associated with the spinal deformity shown in Figures 79a and 79b? ---
1
Improved gait
2
Deformity progression
3
Delayed satiety
4
No further risk of fracture
5
Improved lung function
The images delineate progressive osteoporotic collapse. As outlined by Kado and associates, Schlaich and associates, and Gold and associates, the progression of spinal deformity and the functional consequences of vertebral compression fractures are persistent even in those patients who are pain free. Vertebral compression fractures are associated with deteriorating gait, early satiety, further future fracture risk, and deteriorating lung function.
QUESTION 60
When compared with individuals with diffuse idiopathic scoliosis (DISH), patients with ankylosing spondylitis have which of the following rates of neurologic injury, treatment complications, and mortality?
1
Higher rates of neurologic injury, higher rates of treatment complications, and higher mortality following spine trauma
2
Lower rates of neurologic injury, higher rates of treatment complications, and lower mortality following spine trauma
3
Similar rates of neurologic injury, treatment complications, and mortality following spine trauma
4
Higher rates of neurologic injury, higher rates of treatment complications, and similar mortality following spine trauma
5
Higher rates of neurologic injury, higher rates of treatment complications, and lower mortality following spine trauma
All patients with hyperostotic conditions of the spine are at a high risk of neurologic injury following even minor trauma. However, several studies have shown that patients with ankylosing spondylitis have higher rates of neurologic injury and complications related to treatment compared with individuals with DISH. A recent meta-analysis was unable to show a significantly increased risk of mortality for patients with ankylosing spondylitis relative to those with DISH (3-month mortality estimated at 17% to 20%).
QUESTION 61
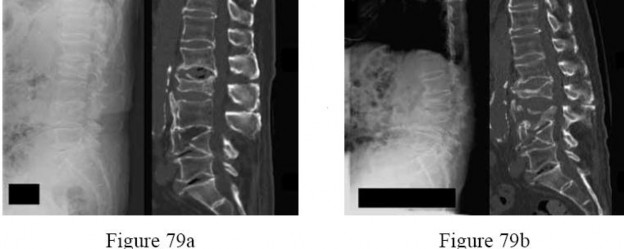
Figures 81a through 81c show the MRI scans of a 53-year-old man who has experienced a long history of progressively worsening right-sided back pain with radiation to the buttocks and right lower extremity.Examination reveals weakness and hyperreflexia in the right lower extremity. He reports intermittent episodes of urinary incontinence. What is the most appropriate surgical approach? ---
1
Costotransversectomy
2
Laminectomy
3
Transpedicular
4
Lateral extracavitary
5
Transthoracic
The presence of stenosis in the thoracic region with its related clinical manifestations has only recently been appreciated. The pathogenesis of thoracic stenosis is similar to that found in the cervical or lumbar spine. Two distinct clinical syndromes of thoracic stenosis have been identified,the most common being associated with degenerative changes of the spine. Clinical manifestations include development of
unilateral or bilateral symptoms of pseudoclaudication. Focal radicular pain or paresthesias may also be present. The neurologic examination initially may be normal, but as the degree of neural compression progresses, posterior column dysfunction and long tract signs appear. If allowed to progress untreated, the patient may develop significant difficulty with gait and bowel/bladder function.Thoracic spinal cord stenosis secondary to congenital narrowing of the spinal canal is associated with a more abrupt onset of symptoms. The typical clinical manifestations of myelopathy may commence following minor or moderate trauma. Radicular symptoms are rare in congenital thoracic stenosis. One indication for thoracic laminectomy is a patient in whom imaging has demonstrated evidence of spinal canal stenosis secondary to hypertrophy of the posterior elements. A laminectomy should not be the primary approach when stenosis results from a significant ventral epidural osteophyte or herniated disk;these lesions are more effectively and safely managed by a posterolateral (transpedicular, transfacetal, or costotransversectomy) or an anterior approach.
QUESTION 62
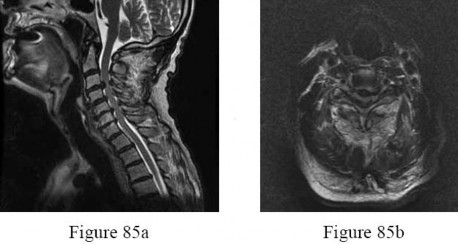
A 69-year-old man has nonpainful weakness in the upper and lower extremities. He also notes progressive instability in his gait and increasing difficulty ambulating, as well as manipulating small objects with his hands. MRI scans of his cervical spine are shown in Figures 85a and 85b. When would be the most appropriate time to proceed with surgical treatment? ---
1
When the patient is medically stable for surgery
2
When the MRI scans show multisegmental high-intensity intramedullary signal changes on T2-weighted sequences
3
When he reaches a Nurick grade of IV for his preoperative neurologic function
4
When he reports neck and/or extremity pain that becomes intolerable or not controlled by medication
5
When he develops bowel or bladder incontinence
The natural history of cervical myelopathy is one of slow deterioration over time, typically in a stepwise fashion with a variable period of stable neurologic function. More recent studies suggest that surgery should be performed as soon as possible when cervical spondylotic myelopathy has been diagnosed. Both anterior and posterior are effective and there is no statistical difference between their outcomes. Surgical outcome is related to the patient’s age, disease course, the presence of osseous spinal stenosis, preoperative comorbidities, the preoperative spinal cord functional score, and the presence of high-signal abnormalities on T2-weighted images. To improve the operative result, all the influencing factors should be considered. Patients with focal high-intensity intramedullary signal changes on T2-weighted images have better clinical outcomes following surgery than do patients with demonstrable multisegmental high-intensity intramedullary signal changes on T2-weighted sequences. The transverse area and shape of the spinal cord at the involved segment may also be predictive of surgical outcome.
With progressive compression, the cross section of the spinal cord changes from a boomerang shape to a teardrop shape to a triangular shape. In patients with a Nurick grade of I, there are signs of cord involvement, but gait remains normal. With a Nurick grade of II, there are mild gait abnormalities,not affecting the patient’s employment status. With a Nurick grade of III, gait abnormalities prevent employment, but the patient remains able to ambulate without assistance. In Nurick grade IV, the patient is only able to ambulate with assistance. In Nurick grade V, the patient is chair-bound or bedridden. Clearly, it is desirable to operate when the patient is functioning with a Nurick grade of I or II. Whereas many patients presenting with cervical spondylotic myelopathy also report axial neck pain and radicular symptoms in the upper extremities, this is not always the case. Surgical intervention will generally be effective in eliminating this pain; however, the pain is not the determining factor for performing surgery.Surgery is performed to preserve and restore function. Changes in bowel and bladder function can occur
in extremely severe cases of myelopathy, but this is quite rare.
QUESTION 63
Which of the following statements best describes the instantaneous axis of rotation (IAR) for thefunctional spinal unit?
1
The IAR is calculated by movement around six different axes.
2
The IAR consists of potential movements or 12 degrees of freedom.
3
The IAR is fixed and consistent and is the axis about which each vertebral segment rotates.
4
The IAR can be derived from AP and lateral radiographs.
5
Degenerative disease, fractures, and ligamentous injuries can affect the IAR.
The instantaneous axis of rotation is the axis about which each vertebral segment rotates,but is theoretical depending on how it is defined, and varies depending on multiple factors. It is not a fixed point but can move depending on the position of the spine, and it is affected by degenerative conditions,fractures, injuries, and other anatomic changes of the spine. There are three axes of movement with 6 degrees of freedom (rotation and translation movements about each axis).
QUESTION 64
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms,although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What
is the next most appropriate step in management?
1
DEXA scan
2
Brace treatment with a Jewett hyperextension brace
3
Anterior lumbar corpectomy and arthrodesis with instrumentation
4
Posterior lumbar decompression and fusion
5
Vertebral cement augmentation
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
---
QUESTION 65
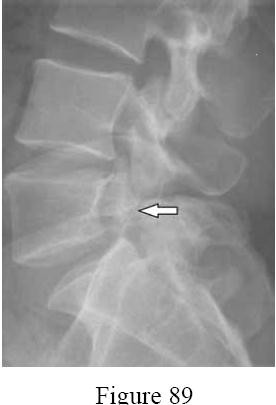
What is the incidence of the radiographic finding shown in Figure 89 in the adult population in North America?
1
Less than 2%
2
4% to 6%
3
8% to 10%
4
12% to 14%
5
Greater than 15%
The pars interarticularis is a thin bicortical region of the posterior arch of the lumbar vertebra, where the lamina and inferior articular process intersect with the pedicle and superior articular process. A fibrocartilaginous cleft in this region is referred to as a spondylolysis or a pars defect. This finding is present in 4% to 6% of the North American adult population.
Buetler and associates conducted a prospective study of 500 children and followed them through young adulthood. They found the incidence of spondylolysis to be 4.4% in children aged 6 years. An additional eight subjects developed
spondylolysis between the ages of 12 and 25 years for an adult incidence of 6%. Ninety percent of the pars defects occurred at the L5-S1 level, with two thirds of the defects occurring in males.
QUESTION 66
A 78-year-old man is seen in the emergency room 3 hours after a fall from a standing position. The patient sustained a mild scalp laceration and the injury shown in Figure 90. He reports severe neck pain and is unable to move his hands and legs.
Examination reveals absent motor function in the wrist flexors,triceps, and fingers. He cannot move his lower extremities during motor testing. The patient has some sensation in the lower extremities. Bulbocavernosus reflex is absent. Based on examination findings and the imaging findings, what is the most definitive treatment option? ---
1
Closed reduction and immobilization in a halo-thoracic vest
2
Halo application and cervical traction for 6 weeks, followed by 8 weeks of immobilization in a halo-thoracic vest
3
Open reduction, decompression, and fusion with anterior-posterior stabilization
4
Open reduction, anterior decompression, and fusion
5
Uninstrumented posterior fusion spanning the injured segment
The patient has a hyperostotic condition of the cervical spine, most likely ankylosing spondylitis. Because of a rigid and osteoporotic spine, relatively minor falls can result in unstable spinal injuries with significant instability and a high risk for neurologic sequelae. The patient has an unstable injury at C6 with an incomplete spinal cord injury, necessitating urgent decompression and stabilization.Studies have shown that, in
patients with ankylosing spondylitis, stand-alone anterior stabilization results in a high failure rate. Halo-thoracic vests carry a high risk of septic and pulmonary issues, especially in the elderly. Uninstrumented fusion will provide insufficient stability in such patients.
QUESTION 67
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management?
1
Anesthetic injections in both sacroiliac joints
2
Sacroiliac fusion with plate fixation
3
Anti-inflammatory medications, physical therapy, and HLA-B27 testing
4
Patient reassurance and follow-up as needed
5
Immediate bilateral sacroiliac joint aspiration and culture
The patient has a classic presentation of early ankylosing spondylitis. Sacroiliac joint fusion is the earliest radiographic finding and is typically followed by cephalad spinal progression. Early treatment of ankylosing spondylitis consists of nonsteroidal anti-inflammatory drugs and physical therapy to preserve spinal motion. HLA-B27 testing is positive in most (about 95%) patients; however, it is not pathognomonic because it can be positive with other conditions. Considering the progressive nature of this disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected;however, in the absence of fever or other constitutional symptoms, infection is unlikely.
QUESTION 68
Which of the following is the most common site for compression and burst fractures?
1
L2 level
2
L3 level
3
L4 level
4
L5 level
5
S1 level
Thoracolumbar compression and burst fractures occur most frequently at the thoracolumbar junction (between T12 and L2) and represent more than 50% of all thoracic and lumbar fractures. The thoracolumbar junction represents a transition from the stiff thoracic spine to the more flexible lumbar spine.
QUESTION 69
Figure 93 shows the axial T2-weighted MRI scan of the lumbar spine of a 70-year-old man. The arrow points to which of the following structures? ---
1
Lamina
2
Facet joint
3
Lumbar synovial cyst
4
Ligamentum flavum
5
Epidural space
The ligamenta flava (singular, ligamentum flavum, Latin for yellow ligament) are ligaments that connect the laminae of adjacent vertebra, all the way from the axis to the first segment of the sacrum. In T2-weighted sequencing, ligamentous structures possess a low signal intensity. The ligamentum in this patient is markedly
thickened, resulting in severe spinal stenosis. The epidural space lies ventral and medial to the ligamentum flavum and should possess a high signal intensity secondary to the presence of cerebrospinal fluid. However, in the case of high-grade stenosis, there may be little if any cerebrospinal fluid present, making the epidural space and central canal difficult to identify. A lumbar synovial cyst should also have high signal intensity because of the presence of synovial fluid.
QUESTION 70
The findings in Brown-Séquard syndrome include loss of which of the following?
1
Greater loss of upper extremity motor function than lower extremity function
2
Ipsilateral motor function and ipsilateral pain and temperature sensation
3
Ipsilateral motor function and contralateral pain and temperature sensation
4
Contralateral motor function and ipsilateral pain and temperature sensation
5
Lower of extremity proprioception and balance
Brown-Séquard syndrome is most commonly seen after penetrating injuries to the spinal cord and results in ipsilateral loss of motor function and contralateral loss of pain and temperature sensation. Patients with central cord syndrome have greater weakness in the upper extremities than in the lower extremities. Loss of proprioception is typically seen in patients with posterior cord syndrome.
QUESTION 71
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness.Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities.Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following?
1
Brachial plexus injury
2
Anterior cord syndrome
3
Posterior cord syndrome
4
Central cord syndrome
5
Brown-Séquard syndrome
The MRI scan shows advanced multilevel degenerative changes and moderate to severe stenosis at C3-C4 and C4-C5 with associated cord signal change. The patient has greater weakness in the upper extremities than in the lower extremities. This pattern is most compatible with central cord syndrome. Patients with brachial plexus injury will have unilateral weakness. Patients with anterior cord syndrome will have greater weakness in the legs than in the arms, and those with Brown-Séquard syndrome will have ipsilateral motor deficits and contralateral pain and temperature deficits.
QUESTION 72
A patient who underwent an L5-S1 hemilaminotomy and partial diskectomy for radiculopathy 3 weeks ago now reports increasing leg and back pain with radicular signs. An axial T2-weighted MRI scan is shown in Figure 97a, an axial T1-weighted MRI scan is shown in Figure 97b, and a contrast enhanced T1-weighted MRI scan is shown in Figure 97c. What is the most appropriate management for the
patient’s symptoms? ---
1
Irrigation and débridement of deep wound infection
2
CT-guided needle biopsy and IV antibiotics
3
Revision laminotomy and diskectomy
4
L4-L5 anterior débridement and fusion
5
Open repair of the L4-L5 pseudomeningocele
The MRI scans show a recurrent disk herniation. There is no increase fluid signal or enhancement to suggest infection or any other pathologic process. There is no infection; therefore, IV antibiotics and débridement are not indicated. Similarly, a pseudomeningocele is not present. In addition,with progressive weakness, physical therapy is not appropriate. A revision diskectomy is useful for recurrent radiculopathy.
QUESTION 73
Thoracic disk herniations most typically occur at what level of the thoracic spine?
1
Upper third
2
Junction of upper third and middle third
3
Middle third
4
Junction of middle third and lower third
5
Lower third
Most thoracic disk herniations occur in the lower (caudal) third of the thoracic spine. This predilection may be related to the unique anatomic and biomechanical environment of that region. The 11th and 12th ribs do not join the rib cage anteriorly and do not form a true articulation with the transverse processes posteriorly.
Furthermore, flexion and torsional forces tend to concentrate between T10 and L1.
QUESTION 74
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root?
1
L3
2
L4
3
L5
4
S1
5
S2
Posterolateral disk herniations will generally compress the transversing nerve root.Therefore, a posterolateral disk herniation at the L4-5 level will typically compromise the L5 nerve root.Far lateral (extraforaminal) disk herniations generally compromise the exiting nerve root. Therefore, an extraforaminal herniation at the L4-5 level will typically compromise the exiting L4 nerve root.
QUESTION 75
Which of the following groups of tumors is most likely to metastasize to the spine?
1
Uterine, thyroid, renal, lung
2
Breast, prostate, lung, kidney, thyroid
3
Breast, prostate, lung, kidney, skin
4
Breast, prostate, other osseous, skin, thyroid
5
Breast, prostate, hemangioma, lung, kidney
The primary tumors most likely to metastasize to the vertebral column are breast (16%to 37% of breast cancer patients develop spine metastases), prostate (9% to 15%), lung (12% to 15%),kidney (3% to 6%), and thyroid (4%). Symptomatic lesions typically are found in the thoracic (68% to 70%), lumbosacral (16% to 22%), and cervical (8% to 15%) spine. Hemangiomas are benign tumors of the spine and are typically seen in the vertebral body as lesions that are bright on T1- and T2-weighted images; they do not typically metastasize to the spine. RESPONSES FOR QUESTIONS 101 THROUGH 103
1. C4
2. C5
3. C6
4. C7
5. C8
For each patient, please select the correct nerve root involvement.
QUESTION 76
What is the most likely diagnosis?
1
Fibrous dysplasia
2
Aneurysmal bone cyst
3
Osteosarcoma
4
Giant cell tumor
5
Osteomyelitis
_ _
QUESTION 77
Workup of this patient should specifically include which of the following studies?
1
Westergren sedimentation rate
2
Platelet function tests
3
CT scan of the chest
4
Serum electrophoresis
5
Prostate-specific antigen
_ _
QUESTION 78
Which of the following represents the most appropriate treatment at this time?
1
Amputation of the leg
2
Distal femoral replacement
3
Chemotherapy and radiation therapy with non-weight-bearing until the lesion heals
4
Curettage, with local phenol and cementation
5
Hormonal therapy
_ _
DISCUSSION FOR QUESTIONS 104 THROUGH 106:
This is a classic presentation of a giant cell tumor. It is a benign aggressive bone tumor consisting of distinct undifferentiated mononuclear cells. Most occur in patients 30 years to 50 years of age (90% are older than age 20 years) and affect woman more than men. Pain and swelling for 2 to 3 months is classic.The most common location is the distal femur. The biopsy specimen shows multinucleated giant cells amid a background of mononuclear cells. This benign tumor may rarely metastasize to the lung (less than 2% of the time). A CT scan of the chest is required to rule out any further lesions. Curettage, with local adjuvants, such as phenol, cryotherapy, or argon beam, and cementation represents the best treatment option at this time.
CLINICAL SITUATION FOR QUESTIONS 107 THROUGH 109
An otherwise healthy 65-year-old man reports progressive and unrelenting back pain for the last 6 weeks that is nonmechanical in nature. He denies leg pain, weakness, bowel or bladder symptoms, and any significant past medical history. His pain is increased at night. Examination reveals pain with percussion throughout his thoracic spine. He is neurologically intact. AP and lateral radiographs of the thoracic and lumbar areas show diffuse osteopenia with no fractures.
QUESTION 79
What is the most appropriate test to order at this time?
1
PET scan
2
CT scan of the thoracic spine
3
Upright scoliosis series
4
MRI with gadolinium of the thoracic spine
5
Total body bone scan
_ _
QUESTION 80
If the scan shows metastatic, noncontiguous lesions throughout the thoracic spine without epidural spinal cord compression with no known primary lesion, what is the next step in establishing a diagnosis?
1
Open biopsy of the spine lesion
2
Image-guided biopsy
3
Bone marrow aspirate of the ilium
4
CT scan of the chest, abdomen, and pelvis
5
Urine electrolytes
_ _
QUESTION 81
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
1
Cement augmentation
2
En bloc resection
3
Chemotherapy
4
Radiation therapy
5
Intralesional excision
_ _
DISCUSSION FOR QUESTIONS 107 THROUGH 109:
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.