Orthopedic Foot And Ank Review | Dr Hutaif Foot & Ankle -...
Updated: Feb 2026
43 Views
Key Medical Takeaway
Looking for accurate information on Orthopedic MCQS online 012 FOOT AND ANKLE? For avulsion fractures of the calcaneus, immediate open reduction and internal fixation is the best treatment. Nonsurgical management often failed to provide adequate healing, leaving a weak Achilles tendon and high complication rates. Percutaneous Kirschner wire fixation also failed to provide stable fixation against the powerful Achilles tendon, making it unsuitable for this type of injury.
Score: 0%
Orthopedic MCQS online 012 FOOT AND ANKLE
QUESTION 1
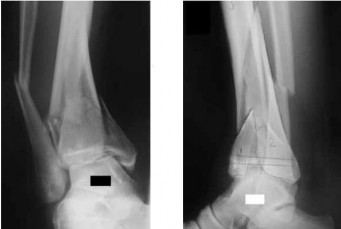
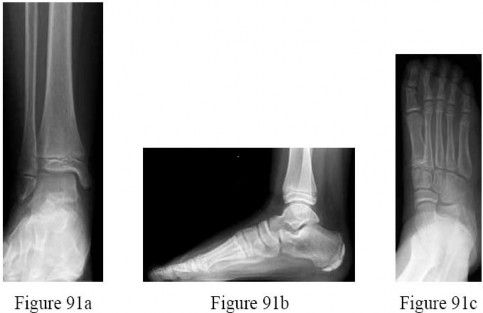
Figure 1 is the radiograph of a 48-year-old man. He is of normal height and weight, medically healthy,and in good physical condition. What is the best treatment option?
1
Short-leg non-weight-bearing cast in plantar flexion
2
Excision of the fragment and reattachment of the Achilles tendon into the calcaneus
3
Immediate open reduction and internal fixation
4
Open reduction and fixation when swelling reduces
5
Percutaneous reduction and Kirschner wire fixation
Immediate open reduction and internal fixation of this fracture is required to prevent necrosis of the overlying soft tissue. Because of the power and proximal pull of the triceps surae,nonsurgical management is not indicated with avulsion fractures of the calcaneus. It leaves a large void that will not fill in with bone, leaves the Achilles tendon weak, and has a high complication rate, especially skin breakdown. The Achilles tendon is securely attached to the fractured tuberosity. Bone-to-bone healing is more reliable than detaching the Achilles tendon from the tuberosity and reattaching it to the remainder of the calcaneus. Because of the size of the avulsed fragment, it will be difficult to correctly tension the tendon if the fractured piece is excised. Percutaneous Kirschner wire fixation is not strong enough to provide a stable fixation of the tuberosity, especially in view of the power of the Achilles tendon contracture.
QUESTION 2
Figures 3a and 3b are the current AP and oblique radiographs of a 44-year-old man who underwent nonsurgical management of a left ankle fracture 6 months ago. What is the most appropriate course of management?
1
Arizona brace
2
Ankle arthroscopy with drilling of the talar osteochondral lesion
3
Medial ankle arthrotomy and débridement with correction of the fibular malunion
4
Ankle arthrodesis
5
Ankle and subtalar arthrodesis
The radiographs reveal a fractured malunited, shortened fibula with deltoid
instability.Corrective osteotomy with fibular lengthening has shown positive results. Nonsurgical management in an active, healthy patient will lead to rapid deterioration of the ankle joint. Without evidence of arthritis, a joint-sacrificing procedure should not be used.
---
QUESTION 3
Figure 5 shows the deformity that developed in a 49-year-old woman who had previously undergone a bunion correction. The patient’s great toe is easily corrected to a neutral position but tends to spring back to a varus position. She reports pain in the first metatarsophalangeal joint and has difficulty wearing most shoes. What is the most appropriate management plan?
1
1-2 toe taping and closed toe shoes
2
Split extensor hallucis longus tendon transfer
3
Great toe fusion
4
Medial soft-tissue release and lateral capsule plication
5
Metatarsal osteotomy, medial capsule release, and split extensor hallucis longus tendon transfer
Osteotomy and tendon transfer is the management of choice. The previous bunion correction resulted in excessive translation of the metatarsal head. The orthopaedic surgeon must first correct the bony deformity and allow the proximal phalanx to sit in a congruent position. The next step is to reconstruct the soft-tissue components and this can be done by releasing the medial capsule,and transferring part of the extensor hallucis longus tendon into the proximal phalanx, under the intermetatarsal ligament laterally. All three procedures are needed to adequately correct this deformity. A great toe fusion is indicated for an uncorrectable deformity or in an older patient.
QUESTION 4
A 28-year-old man has a progressive drop-foot deformity secondary to Charcot-Marie-Tooth disease.Examination reveals no tibialis anterior or peroneus brevis function. He has a 5-degree equinis contracture. Tibialis posterior and flexor digitorum longus are 5/5 strength. There are no fixed deformities of any joints. What is the most appropriate surgical option?
1/. A gastrocnemius lengthening and transfer of the tibialis posterior tendon to the dorsum of the foot
1
A gastrocnemius lengthening and transfer of the peroneus brevis to the dorsum of the foot
2
Transfer of the flexor digitorum longus to the dorsum of the foot
3
An ankle fusion and transfer of the tibialis posterior to the dorsum of the foot
4
A triple arthrodesis to stabilize the drop-foot deformity
At this point, the deformities are supple and fusions are not indicated. The tibialis posterior is the force couple or antagonist of peroneus brevis. With no peroneus brevis, the tibialis posterior is not only a deforming force, pulling the foot into inversion, but it is also the strongest muscle to use as an ankle dorsiflexor. By transferring it, the deforming force is removed and converted into an ankle dorsiflexor. With the equinis contracture, the gastrocnemius should be lengthened to allow the transferred tendon to dorsiflex the ankle beyond neutral.
---
QUESTION 5
Figures 7a and 7b are the weight-bearing radiographs of a 17-year-old girl who has great toe pain with push-off and stiffness 1 year after undergoing a proximal crescentic osteotomy for hallux valgus. Motion at the first metatarsophalangeal joint includes approximately 20° of dorsiflexion. What is the most appropriate treatment? ---
1
Proximal phalanx osteotomy
2
Double metatarsal osteotomy
3
Plantar flexion metatarsal osteotomy
4
Distal biplanar metatarsal osteotomy
5
Capsular release and aggressive physical therapy
The patient has progressed to a dorsiflexion malunion of the first metatarsal. The absence of implants suggests that smooth pin fixation was likely used, likely contributing to the malunion. The patient should be managed with a plantar flexion metatarsal osteotomy. The joint stiffness is likely a result of the malunion acting as a mechanical block to dorsiflexion, thus a capsular release would not be sufficient. The distal biplanar metatarsal osteotomy and double metatarsal osteotomy are used for hallux valgus deformities associated with an increased distal metatarsal articular angle.
The proximal phalanx osteotomy is used for supplemental correction of associated hallux valgus interphalangeus.
---
QUESTION 6
Figures 8a and 8b are the preoperative radiographs of a 47-year-old woman who is being treated for a supple pes plano abductovalgus deformity. She is unable to perform an ipsilateral single leg heel raise. Which of the following is the most likely soft-tissue procedure performed in combination with the bony surgery?
1
Flexor digitorum longus tendon transfer
2
Extensor hallucis longus tendon transfer
3
Spring ligament release
4
Peroneus longus tendon repair
5
Lateral collateral ligament reconstruction
Flexor digitorum longus tendon transfer and augmentation has similar dynamic function to the posterior tibial tendon. Other reported tendon transfers for this procedure include flexor halluces longus and peroneus brevis, but not extensor hallucis longus nor peroneus longus. Spring ligament release accentuates the flatfoot deformity whereas conversely, spring ligament repair/reconstruction is another recognized soft-tissue procedure that may be combined with bony surgery for treatment of flexible acquired flatfoot deformity. Lateral collateral ligament reconstruction addresses lateral ankle instability which the patient does not have.
---
QUESTION 7
Figures 9a and 9b are the radiographs of a 32-year-old woman who has right foot pain after falling down a few steps. For the best long-term outcome, initial treatment should include which of the following? ---
1
Splinting with non-weight-bearing as the definitive treatment
2
Walking boot
3
Closed reduction and casting
4
Percutaneous pinning
5
Primary open reduction and internal fixation (ORIF)
The radiographs show a displaced Lisfranc injury. The outcome of treatment is dependent on achieving an anatomic reduction and stabilization, which is only possible with primary ORIF. Some studies indicate primary fusion may provide superior short-term results compared with ORIF. Closed treatment (reduction with casting or splinting) will not achieve or maintain the reduction, whereas delayed treatment by secondary fusion after arthritis occurs yields inferior outcomes to primary ORIF.
---
QUESTION 8
Figure 10 is the radiograph of a middle-aged woman who has had midfoot pain for the past several years without antecedent trauma. What is the most likely etiology of her condition?
1
Osteomyelitis
2
Kohler disease
3
Rheumatoid arthritis
4
Primary osteoarthritis
5
Osteochondritis dissecans
The radiograph shows isolated degeneration in the talonavicular joint that is symmetric.The symmetry of the degeneration is characteristic of an inflammatory arthritis. In the absence of trauma,isolated arthritis in this joint is uncommon. The navicular is normal sized, ruling out Kohler disease(as well as the patient being in the wrong age group). There are no erosions indicative of osteomyelitis.Osteochondritis dissecans appears as focal osteochondral lesions, which are not present in the radiograph.
---
QUESTION 9
Figure 11a is the radiograph of a 45-year-old woman with a moderate bunion deformity. A Chevron osteotomy was performed and after 6 weeks the patient was doing reasonably well. Six months later she reports increasing pain and stiffness in her toe. Clinically the toe is reasonably straight, but she has significant calluses and overload under the second and third metatarsals. A follow-up radiograph is shown in Figure 11b. The patient wants to be free of pain. What is the most appropriate treatment?
1
Revision bunion repair with a Lapidus procedure
2
Keller’s excision arthroplasty
3
Moberg osteotomy of the proximal phalanx
4
Metatarsophalangeal joint fusion with an autologous bone block
5
Allograft replacement of the metatarsal head
The patient developed osteonecrosis of the metatarsal head with shortening of the first metatarsal and subsequent overload of the lesser metatarsals. The most reliable option is to perform a metatarsophalangeal joint fusion with an autologous bone block to restore length. A revision bunion repair will not address the arthritic
changes. A Keller’s excision arthroplasty will further aggravate the lesser metatarsal overload. An allograft replacement of the metatarsal head has a very low predictability rating and is highly experimental.
---
QUESTION 10
Figure 12 is the radiograph of a patient with type 2 diabetes, a body mass index of 42, and an Hgb A1c of 8. What is the most appropriate management for this injury?
1
Fracture boot immobilization
2
Casting the ankle in its current position
3
Closed reduction and definitive casting
4
Closed reduction and application of external fixation
5
Open reduction and internal fixation (ORIF)
Several recent studies have shown that while there is an increased risk of complications following ORIF of displaced ankle fractures in diabetic patients compared with nondiabetic patients,the overall risks of treatment are less than that associated with nonsurgical treatment in diabetics. There is also the possibility that ORIF of unstable ankle fractures may forestall the development of Charcot changes in the ankle, although this is not definitively known. Extra rigid fixation may be required because of the patient’s size and poorly controlled diabetes. Nonsurgical management is associated with poorer functional outcomes (due to arthritis secondary to poor reduction of the fracture) and a higher rate of skin breakdown, due to the need for higher skin pressures from the use of highly molded casting used to maintain a closed reduction.
QUESTION 11
A 28-year-old construction worker with a body mass index (BMI) of 31 sustained a Weber C fracture 3 years ago. An open reduction and internal fixation was performed, but he developed degenerative changes in the ankle as seen in Figure 13. Management consisting of bracing, shoe modifications, and other modalities has failed to provide relief. He is symptomatic enough that he wants definitive treatment. What is the best treatment option at this time?
1
Bipolar allograft replacement of the tibial plafond and
talar dome
2
Low profile total ankle arthroplasty
3
Interpositional soft-tissue replacement
4
Arthroscopic ankle débridement
5
Ankle fusion
Ankle fusion will provide the most reliable
pain relief and function for this young manual laboror. At his young age and with a BMI of 31, both total joint
---
arthroplasty and allograft replacement are controversial. An interpositional graft could be
an option, but there is not enough evidence in the literature to recommend it at this time. The radiographs show degenerative changes that are too far advanced for an arthroscopic ankle débridement to be of any benefit.
QUESTION 12
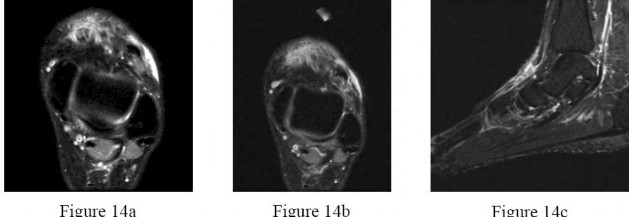
Figures 14a through 14c are the MRI scans of a 37-year-old woman who sustained a traumatic laceration to the anterior aspect of the ankle. The wound was closed in the emergency department. On examination,she has a foot drop and ambulates with a steppage gait. With successful surgical repair, what is the most common long-term residual? ---
1
Numbness in the foot
2
Persistent foot drop
3
Persistent ankle pain
4
Decreased dorsiflexion strength
5
Use of an ankle-foot orthosis for ambulation
Anterior tendon disruption has been described in association with direct trauma, gout,inflammatory arthritis, local steroid injections, and diabetes. When a
rupture is accurately diagnosed in younger, healthy, active patients, surgical repair has been recommended. Surgical repair results in improved patient satisfaction; however, isokinetic testing has shown decreased dorsiflexion and inversion strength compared with the uninvolved side. Numbness can result from missed superficial nerve laceration. Persistent foot drop and use of an ankle-foot orthosis are more frequently seen in chronic missed injuries or with nonsurgical management.
---
QUESTION 13
Figures 15a and 15b are the radiographs of an active 65-year-old woman who has a 3-year history of increasing foot pain and flattening of the left foot. Inversion strength is 5+ and does not reproduce her symptoms. Bracing and nonsteroidal anti-inflammatory drugs have failed to provide adequate relief. She has a supple hindfoot and normal heel cord flexibility. What is the most appropriate treatment? ---
1
Lateral column lengthening and flexor digitorum longus transfer
2
Talonavicular arthrodesis
3
Medial Lisfranc arthrodesis
4
Subtalar arthrodesis
5
Triple arthrodesis
DISCUSSION: The patient has degenerative changes with collapse at the tarsometatarsal joints; therefore,a fusion of the Lisfranc joint is indicated. The other responses are hindfoot procedures that will not address the tarsometatarsal joint. PREFER RESPONSE: 3 Question 16 Figure 16 is the lateral radiograph of a 40-year-old laborer who sustained a displaced intra-articular calcaneus fracture that was treated nonsurgically 1 year ago.

He now reports pain with ankle dorsiflexion,as well as subfibular impingement. What is the most appropriate surgical treatment?
The patient has a calcaneal fracture malunion, with symptomatic subtalar arthritis and anterior ankle and lateral subfibular impingement. Distraction subtalar arthrodesis addresses subtalar arthritis and anterior impingement and lateral wall ostectomy relieves symptoms of lateral impingement.The other procedures do not address all facets of the patient’s symptoms.
QUESTION 14
Figures 18a and 18b are the radiographs of an obese 75-year-old man with a rigid acquired flatfoot deformity. What is the best treatment option?
1
Double calcaneal osteotomy
2
Medial calcaneal osteotomy and tendon transfer
3
Lateral column lengthening and tendon transfer
4
Subtalar arthrodesis
5
Triple arthrodesis
For stage III adult-acquired flatfoot deformity characterized by dysfunction of the posterior tibial tendon, rigid valgus deformity of the hindfoot, and arthritic changes of the hindfoot joints,arthrodesis is the favored procedure. In an overweight patient with degenerative changes affecting the subtalar and Chopart joints, triple arthrodesis is the best treatment option. Subtalar arthrodesis only addresses the talocalcaneal joint and continues to render the patient symptomatic in the talonavicular and calcaneocuboid joints. Advanced stage III disease precludes reconstructive procedures involving calcaneal osteotomy and tendon transfer.
QUESTION 15
Which of the following occurs frequently after nonsurgical management of displaced intra-articular fractures of the calcaneus?
1
Return to normal function
2
Narrowing of the calcaneus
3
Lengthening of the calcaneus
4
Plantar flexion of the talus
5
Peroneal tendinitis
Peroneal tendinitis and stenosis are typically seen following nonsurgical management and results from lateral subfibular impingement, whereby the displaced, expanded lateral wall subluxates the peroneal tendons against the distal tip of the fibula or might even dislocate the tendons. Nonsurgical management of displaced calcaneal fractures offers little chance for return to normal function because of the development of a calcaneal malunion. The articular surface is not reduced, the heel remains shortened
and widened, the talus is dorsiflexed in the ankle mortise, and the displaced lateral wall causes impingement and binding of the peroneal tendons.
QUESTION 16
What is the most important measure to take to reduce the risk of frostbite of the toes while hiking in extreme temperatures?
1
Stop often for recovery breaks.
2
Drink enough warm liquids.
3
Reduce thermal heat loss from shoes.
4
Use triple socks.
5
Adequately "carbo load" before the start.
Several studies showed the most reliable method to reduce the risk of cold exposure injury is to reduce thermal heat loss. This can be done with a combination of protective socks and shoes, and reducing moisture in the shoes.
QUESTION 17
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?
1
Use of cut or trimmed plates
2
Use of straight (uncontoured) plates
3
Use of locked plating
4
Low plate placement with a prominent screw head in the distal hole
5
Low antiglide plate placement
Low plate positioning with a prominent screw head in the most distal hole of the plate was shown to be correlated with peroneal tendon lesions. Distal plate placement in the absence of prominent screws was not associated with tendon lesions. Trimmed plates, locked plates, and uncontoured plates have not been shown to increase the risk of peroneal tendon pathology.
---
QUESTION 18
A patient who sustained an Achilles tendon rupture does Internet research on his injury and its treatment before seeing an orthopaedic surgeon. The patient would like to have surgical repair of the tendon rupture using the technique shown in Figure 24. What can the surgeon tell the patient regarding the possible benefits of the use of this pictured technique versus an open technique for the repair of acute Achilles tendon ruptures?
Overall the same rate of postoperative complications
Trials comparing the results of open repair of acute Achilles tendon rupture to repairs done in a limited open fashion show no difference in rerupture rate, sural neuropathy, or calf circumference.The scarring observed was much less in the group treated in a limited open fashion. There was a significantly greater number of postoperative complications seen in the group treated in an open fashion compared with those treated with a limited open procedure.
QUESTION 19
What is the most common complication with an anterior ankle arthroscopy using a standard lateral arthroscopy portal?
1
Injury to the superficial peroneal nerve
2
Injury to the tibial nerve
3
Vascular injury to the dorsalis pedis
4
Reflex sympathetic dystrophy
5
Deep infection
The most common complication is an injury to the superficial peroneal nerve at the lateral portal. Infection in ankle arthroscopy happens very infrequently. Vascular injury with an anterior scope is very rarely reported. Synovial fistulas are also reported as somewhat common.
QUESTION 20
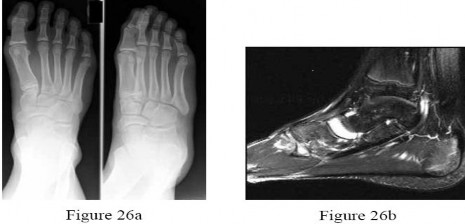
Figures 26a and 26b are the radiographs and MRI scan of a 15-year-old boy who reports midfoot pain for the past 4 months despite no history of injury. The patient plays soccer and is eager to get back to activity.What is the most appropriate treatment to return the patient back to full activity? ---
1
Open reduction and internal fixation
2
Restricted weight bearing in a short-leg cast
3
Weight bearing as tolerated in a fracture boot
4
An orthotic and a bone stimulator
5
A carbon fiber orthotic
The patient has a navicular stress reaction as evidenced by the history and MRI scan findings. This is an acute injury as revealed by the significant edema in the navicular on the MRI scan.Management should consist of restricted weight bearing in a short-leg cast, but possibly a boot. With weight bearing, this fracture could displace and injure the talonavicular joint. A bone stimulator is a good option in conjunction with immobilization. Surgery is indicated when there is a fracture line that extends across two cortices, or across one cortice if there is displacement or cystic changes. This reaction has no fracture line and thus can be treated nonsurgically.
QUESTION 21
A 35-year-old woman has a 6-month history of plantar fasciitis. Which of the following orthoses has been shown to be effective in the treatment of chronic plantar fasciitis?
1
Full-length accommodative insert
2
Semi-rigid insert with a mild medial arch support and a 5° medial post
3
Night splint
4
Cavus foot orthotic
5
Visco gel heel cushion
Of the possible responses, only the night splint has been shown to be effective in the treatment of chronic plantar fasciitis. The role of inserts in plantar fasciitis is controversial with limited scientific data. Although a cavus foot orthotic can be of benefit with respect to plantar fascia symptoms, it is an indirect benefit of accommodating the plantar flexed first ray and has not been scientifically proven.
QUESTION 22
Which of the following nerves is most susceptible to iatrogenic injury during bunion surgery?
1
Terminal branch of the superficial peroneal nerve
2
Terminal branch of the saphenous nerve
3
Dorsolateral cutaneous nerve
4
Medial plantar hallucal nerve
5
Deep peroneal nerve
The dorsomedial cutaneous nerve, which is the terminal branch of the superficial peroneal nerve, is most susceptible to iatrogenic injury, primarily due to the location of surgical incisions. The dorsolateral cutaneous nerve is typically a branch of the
deep peroneal nerve; the medial plantar hallucal nerve is a branch of the medial plantar nerve. The terminal branch of the saphenous nerve provides sensation to the dorsomedial hindfoot.
---
QUESTION 23
shows the radiograph of a 27-year-old patient who has had a medial forefoot prominence since he was a child. Over the past 6 years he notes progressive pain in the first metatarsophalangeal joint. Modified shoe wear, custom orthotics, and use of pads and toe spacers have failed to provide relief.He continues to experience daily pain that affects both employment and recreation activities. Clinical examination reveals good maintenance of first metatarsophalangeal joint motion and no evidence of first tarsometatarsal joint hypermobility. What is the most appropriate treatment?
1
Continued nonsurgical management
2
Austin Chevron osteotomy
3
Biplanar distal first metatarsal Chevron osteotomy
4
Proximal first metatarsal osteotomy
5
Lapidus procedure
The hallux valgus deformity consists of a congruent joint with a moderately severe abnormal distal metatarsal articular angle (DMAA). As such, the procedure that will best correct the deformity is a biplanar distal first metatarsal Chevron osteotomy.
The patient has undergone an extended course of nonsurgical management with multiple modalities; therefore, further nonsurgical management is unlikely to relieve his pain. An Austin Chevron osteotomy will not correct the abnormal DMAA. He does not have an increased 1-2 intermetatarsal angle so a proximal first metatarsal osteotomy will not produce the desired correction. No hypermobility of the first tarsometatarsal joint is noted so a Lapidus procedure is not indicated.
QUESTION 24
A 24-year-old man dislocated his right knee in a motorcycle accident 1 year ago. At the time, an anterior cruciate, posterior cruciate, medial collateral, and lateral collateral ligament repair was done, but it was also noted that he sustained a complete transection of the peroneal nerve. A primary nerve repair was done, but he has not recovered any dorsiflexion of the ankle and continues to have a drop foot. Other than using an ankle-foot orthosis, what is the best surgical option to regain maximum function?
1
Sural nerve cable grafting of the peroneal nerve
2
Transfer of the peroneus longus to the tibialis anterior tendon
3
Transfer of the tibialis posterior to the dorsum of the foot
4
Transfer of the extensor hallucis longus to the tibialis anterior tendon
5
Ankle fusion to eliminate the need for an ankle dorsiflexor
With no recovery of dorsiflexion power 1 year after a peroneal nerve repair, it can be assumed that the nerve will not recover. The peroneus brevis and extensor hallucis longus are supplied by the peroneal nerve, so they will be nonfunctional. A nerve grafting after an initial repair is less reliable than a transfer of the tibialis posterior tendon in restoring active dorsiflexion to the ankle. An ankle fusion should not be the first choice for an active, young patient.
QUESTION 25
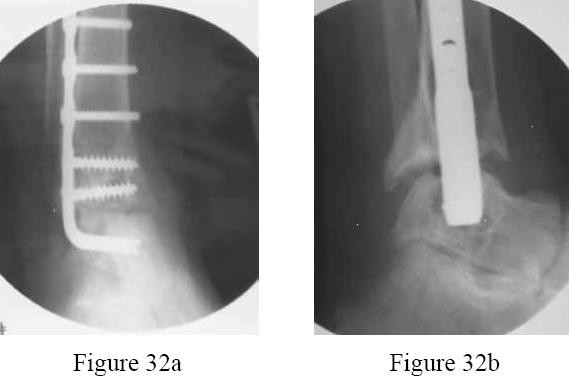
Figures 32a and 32b are the radiographs of a 34-year-old woman who has a painful ankle following an attempted fusion of her ankle 6 months ago. Infection work-up was negative. The subtalar joint is pain free with manipulation. What is the most appropriate treatment? ---
1
Removal of hardware and an intramedullary rod tibiocalcaneal fusion
2
Bone grafting of the nonunion
3
Use of an external bone stimulator
4
Removal of the plate and screws and the addition of an internal bone stimulator
5
Revision fusion with stable compression fixation and bone graft
Because the subtalar joint looks normal, and there is enough talus to work with, the subtalar joint should be spared and only an ankle fusion performed, especially in view of the patient’s young age. There is clearly a distraction at the fusion site and the distal fixation is loose. The patient needs a formal revision with a transfibular approach with compression screws. A simple bone grafting,removal of hardware, and/or a bone stimulator will not be sufficient.
QUESTION 26
Which of the following is associated with tarsal tunnel syndrome?
1
Adult-acquired flatfoot
2
Insertional Achilles tendinitis
3
Hypermobile first ray
4
Metatarsal stress fracture
5
Gastrocnemius contracture
Of the possible hoices, only adult-acquired flatfoot is associated with tarsal tunnel syndrome. The so-called "heel pain triad" includes adult-acquired flatfoot, plantar fasciitis, and tarsal tunnel syndrome, in which failure of the dynamic and static supports of the medial longitudinal arch increase traction on the tibial nerve.
PREFERRED RESPONSE: 1
QUESTION 27
An 18-year-old man sustained a traumatic laceration of the common peroneal nerve when glass fell on the outer part of his leg 1 year ago. He has used a molded foot and ankle orthosis for the past 10 months,but would now like surgical intervention. Electromyography shows no function in the anterior or lateral compartments. He has 5/5 muscle strength of the superficial and deep posterior compartments. What is the most appropriate treatment?
1
Gastrocsoleus recession
2
Subtalar fusion
3
Split anterior tibial tendon transfer
4
Split posterior tibial tendon transfer
5
Flexor hallucis longus tendon transfer
In a patient with a drop foot and with 5/5 muscle strength of the posterior tibial tendon, a split posterior tibial tendon transfer would be the most appropriate treatment option based on the options presented. The deep peroneal nerve innervates the anterior tibial tendon. This muscle has been affected by the injury; therefore, the anterior tibial tendon cannot be transferred. A subtalar fusion would help correct inversion and eversion deformities, but is not effective for plantar flexion deformities.
The foot drop is caused by a neurologic condition in this patient, not a contracture of the gastrocsoleus complex.Therefore, a recession would not be beneficial. A flexor hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
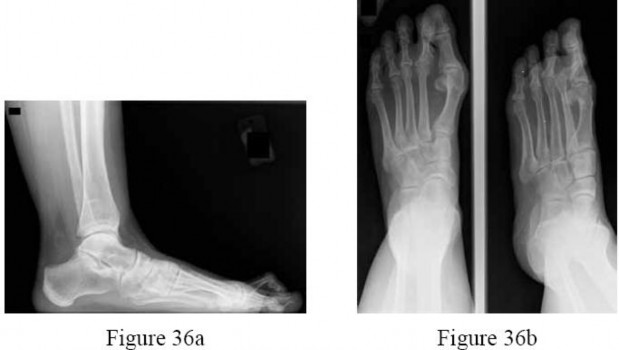
QUESTION 28
Figures 36a and 36b are the AP and lateral radiographs of a 65-year-old woman who has a dislocated second toe and a prominent bunion. Besides repairing the bunion, what procedures are recommended to address the fixed second hammertoe and the resulting metatarsalgia? ---
PIP resection arthroplasty, extensor tendon lengthening, and Weil osteotomy
3
Flexor to extensor tendon transfer and metatarsal head excision
4
PIP fusion and DuVries arthroplasty
5
Metatarsal head excision and proximal phalanx resection
The patient has a subluxated second metatarsophalangeal (MTP) joint, but no evidence of second metatarsal head destruction. The patient also has a fixed claw toe. The claw toe is repaired with a PIP resection arthroplasty or a PIP fusion. The likelihood of
completely correcting the MTP joint dislocation with just these two procedures, however, is small and the addition of the Weil osteotomy is more likely to allow decompression of the joint and complete relocation of the MTP joint. The flexor to extensor transfer is indicated for a flexible hammertoe. A metatarsal head excision is a salvage option of the toe that still cannot be reduced after the Weil osteotomy, but this may lead to transfer lesions.The DuVries arthroplasty will not help reduce the MTP joint. Combined metatarsal head excision and proximal phalanx resection would be extreme and is not recommended.
QUESTION 29
During gait evaluation of a 25-year-old patient who had polio at age 5, it is noted that the right foot slaps
the floor at heel strike, and the toes extend during the swing phase. Examination reveals a flexible cavus foot, claw toes, and an equinus deformity. The patient has tried various orthoses and would like surgical correction if possible. What is the most appropriate treatment?
Calcaneal osteotomy, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
3
Calcaneal osteotomy, plantar fascia release, Achilles tendon lengthening, tibialis posterior transfer to the dorsum of the foot, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
4
Triple arthrodesis, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
5
Plantar fascia release, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, tibialis posterior transfer to the dorsum of the foot, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
Weakness of the tibialis anterior can be noted with a tendency of the foot to slap the floor at heel strike. Extension of the toes during the swing phase of gait may be due to the toe extensors attempting to substitute for weakness of the tibialis anterior. Because this patient is young and has flexible deformities, avoiding arthrodesis is recommended and soft-tissue procedures are recommended to balance the foot. The plantar fascia release helps decrease the cavus. Transfer of the tibialis posterior tendon to the dorsum of the foot is necessary to provide dorsiflexion and limit the slapping of the foot on the floor.Transfer of the extensor hallucis longus to the metatarsal neck
addresses the claw toe deformity of the great toe and the flexor digitorum longus transfer provides additional dorsiflexion assist. Because the patient has a flexible deformity, osteotomies are unlikely to be needed.
QUESTION 30
A 45-year-old man has a grade 4 hallux rigidus secondary to a turf toe sustained as a football player in high school. He is an avid golfer and plays tennis on occasion. His activities are severely limited because of pain in his great toe and nonsurgical management has failed to provide relief. His goal is to be pain free, continue with his activities, and require no further orthopaedic care in the future. What is the best
treatment option for this patient?
1
Keller’s excision arthroplasty
2
Bipolar replacement
3
Cheilectomy and débridement
4
Great toe metatarsophalangeal (MTP) fusion
5
Fascia lata interposition graft
There has been some research about interpositional grafting, whether autologous or allograft, but there is no convincing evidence at this point that there is a better functional outcome than with a great toe MTP fusion. A Keller procedure is not indicated for a young, active person. A joint replacement of the great toe similarly has not proven to be a reliable option for younger, active people.Cheilectomy will not provide reliable pain relief in grade 4 arthrosis of the first MTP joint.
---
QUESTION 31
Figure 39 is the radiograph of a 67-year-old woman with rheumatoid arthritis who reports an 8-month history of increasing pain, swelling, and deformity. Anti-inflammatory drugs, orthotics, and extra-depth shoes have failed to provide relief. What is the next most appropriate step in treatment?
1
First metatarsophalangeal joint arthrodesis and lesser metatarsal head resections
2
First metatarsophalangeal joint replacement and lesser metatarsal head resections
3
Keller arthroplasty and lesser metatarsal head resections
4
Distal Chevron osteotomy and lesser metatarsal head resection
5
Lapidus procedure and Weil osteotomies
The patient has a severe rheumatoid forefoot deformity involving all metatarsophalangeal joints. Coughlin and Mann have found that 90% of patients have excellent and good results with combined first metatarsophalangeal fusion and lesser metatarsal head resection. Keller Arthroplasty does not provide a stable platform for walking and is associated with recurrent deformity and pain. The first metatarsophalangeal joint replacement has not been shown to provide reliable long-term results.Osteotomies may be indicated in patients without erosive joint changes. The Lapidus procedure is an arthrodesis of the first tarsometatarsal joint, which would not address the patient’s arthritic first metatarsophalangeal joint.
---
QUESTION 32
Figures 40a and 40b are the radiographs of a 53-year-old woman. If her symptoms warrant, what is the most appropriate surgical management? ---
1
Plantar release
2
Dorsal cheilectomy
3
Interpositional soft-tissue arthroplasty
4
Arthrodesis
5
Prosthetic replacement
Surgical indications for management of hallux rigidus involve pain, reduced range of motion, and degenerative changes at the first metatarsophalangeal joint. Using the radiographic classification of hallux rigidus, grade 0 denotes normal or minimal joint-space narrowing without osteophytes, whereas grade 1 denotes minimal joint-space narrowing with primary dorsal spurring. In general, plantar release yields adequate clinical results in the surgical management of grade 0 arthritis.Dorsal cheilectomy is used in the surgical management of grade 1 or 2 hallux rigidus, and arthrodesis or resection arthroplasty is used for grade 3 arthritis of the first metatarsophalangeal joint. Treatment with prosthetic arthroplasty is controversial given the increased difficulty with salvage procedures after possible failure.
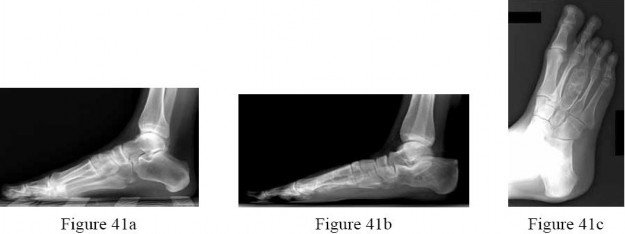
QUESTION 33
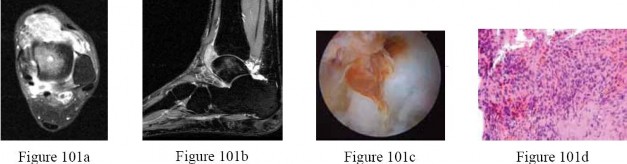
Figures 41a through 41c are the radiographs and Figure 41d is the biopsy specimen of a 14-year-old girl who has had increasing foot pain for several months. What is the most likely diagnosis? ---
1
Infection
2
Giant cell tumor
3
Unicameral bone cyst
4
Aneurysmal bone cyst
5
Hemangioma
Aneurysmal bone cysts frequently occur in the first two to three decades of life. Patients report pain and a slow-growing lesion. Radiographs show an expansile lesion with septae or striations.Treatment is usually curettage and grafting of the lesion. In the foot, unicameral bone cysts are seen most frequently in the calcaneus, and are usually incidental findings rarely requiring treatment. Infection or acute osteomyelitis typically shows lucency of bone, periosteal reaction, and a permeative pattern on radiographs.
Patients often have systemic complaints as well. Giant cell tumor is usually seen in the epiphysis of long bone with radiographs revealing a radiolucent lesion with a small rim of reactive bone.
---
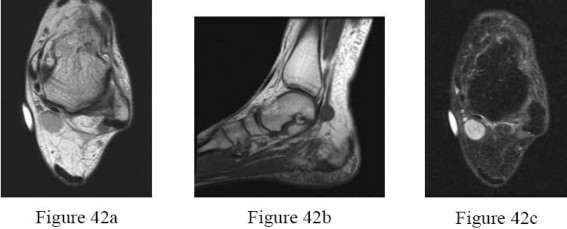
QUESTION 34
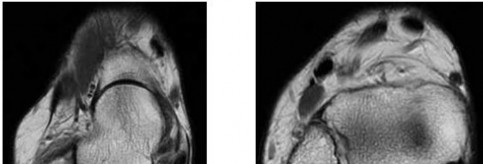
Figures 42a through 42c are the MRI scans of a 42-year-old woman who has a 1.5-cm medial ankle mass.She has pain when shoes compress the area. A positive Tinel’s sign is noted over the tarsal tunnel. What is the most likely diagnosis?
1
Astrocytoma
2
Neurilemoma
3
Neurofibroma
4
Lipoma
27
5
Ganglion
Neurilemoma (Schwannoma) is a benign tumor of nerve sheath (Schwann cell) origin.It is usually a solitary, well-encapsulated lesion located on the surface of a peripheral nerve. Careful excision without damaging the underlying nerve is the treatment of choice. Neurofibroma is a spindle cell tumor arising within a peripheral nerve. Due to its location, it can interfere with distal nerve function.Neurofibromas can be solitary or multiple. A portion of these patients have von Recklinghausen’s disease.Because of the invasive nature of the tumor, resection requires removal of the affected nerve, resulting in distal nerve dysfunction. This lesion does not show the MRI characteristics of either a lipoma or a ganglion.
---
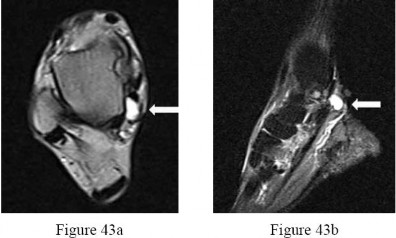
QUESTION 35
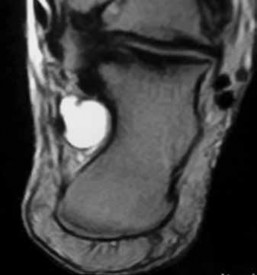
Figures 43a and 43b are the MRI scans of a 54-year-old woman who reports a 2-year history of progressive shooting and burning-type pain in the posteromedial ankle. What is the most appropriate management?
1
Needle aspiration
2
Tarsal tunnel release
3
Incisional biopsy
4
Surgical excision
5
Referral to an orthopaedic surgeon specializing in oncology
The MRI scans show a bright, homogeneous mass (white arrow) on the T2-weighted images consistent with a ganglion cyst, which is likely emanating from the flexor digitorum longus tendon sheath. Because of the neuritic symptoms from the tibial nerve, the patient is best managed with surgical excision. Whereas needle aspiration can provide temporary relief by mass decompression, the location of the lesion in this instance, adjacent to the tibial nerve and posterior tibial artery, makes this option less optimal. Although the cyst is deep to the flexor retinaculum, which necessitates a tarsal tunnel release to access the lesion, release of the flexor retinaculum alone will not likely provide full resolution of symptoms. Incisional biopsy is indicated for potentially malignant lesions, which also makes referral to an orthopaedic surgeon specializing in oncology in this case unnecessary.
QUESTION 36
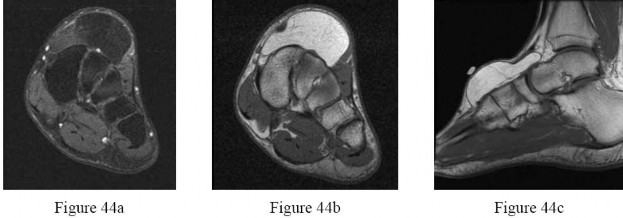
Figures 44a through 44c are the MRI scans of a 45-year-old man who has an enlarging mass on the right foot and has difficulty wearing shoes. What is the most appropriate management for this tumor? ---
1
Amputation
2
Marginal excision
3
Radical excision
4
Local excision with adjuvant chemotherapy
5
Radiation therapy
A lipoma in the foot frequently presents as a dorsal foot mass. The MRI appearance of the lesion is homogenous with density of subcutaneous fat on all sequences. There is no enhancement of the lesion with administration of contrast. The mass is consistent with a simple lipoma. Treatment for a simple lipoma is marginal excision. Amputation, radical excision, and adjuvant therapies are most appropriate for malignant tumors.
QUESTION 37
Figures 46a and 46b are the radiographs of a 20-year-old collegiate varsity athlete who reports lateral foot pain. What is the most appropriate management at this time? ---
1
Rest and nonsteroidal anti-inflammatory drugs
2
Orthosis and non-weight-bearing status
3
Orthosis, weight bearing as tolerated, and use of a bone stimulator
4
Short-leg cast
5
Internal fixation
Fractures of the fifth metatarsal proximal metaphyseal-diaphyseal junction (Jones fracture)generally occur in young athletic patients and have relatively high rates of delayed union or nonunion with nonsurgical management. The fracture occurs in the hypovascular zone between the insertion of the peroneus brevis and tertius. These tendons cause a shearing across the fracture site, preventing stability and healing.
Nonsurgical functional bracing or casting may lead to a high rate of delayed union and nonunion. Internal fixation in the high-level athlete leads to the most predictable healing of the fracture in a timely fashion. The use of bone stimulators for this fracture is controversial.
---
QUESTION 38
The lesion in Figure 47 would most likely cause which of the following symptoms?
1
Anterior tarsal tunnel paresthesias
2
Burning and numbness on the bottom of the foot
3
Heel pain that is worst in the morning
4
Night pain in the heel
5
Loss of toe extension
The lesion would most likely cause burning and numbness on the bottom of the foot,symptoms related to tarsal tunnel, or entrapment of the tibial nerve and its medial and lateral plantar nerves. The MRI scan shows a benign ganglion cyst that is in the tarsal tunnel. This would irritate the nerves and cause pain in the medial heel and plantar foot. Anterior tarsal tunnel paresthesias refers to the anterior tarsal tunnel that is anterior to the ankle and involves the deep peroneal nerve. Heel pain that is most severe in the morning refers to plantar fasciitis. Loss of toe extension is incorrect because the mass may affect toe flexion, not extension. Night pain in the heel is more common with a malignant tumor.
QUESTION 39
A 42-year-old woman sustained an open grade 3B tibial shaft fracture with a severe degloving injury involving the anterior and lateral compartments 1 year ago.
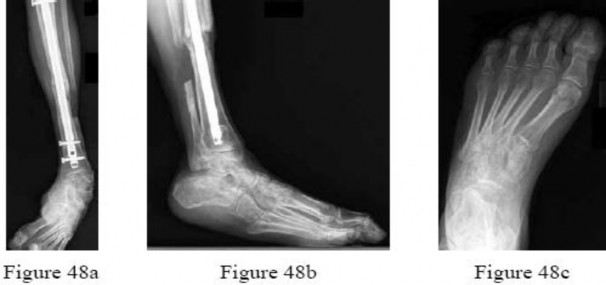
She underwent multiple débridements,definitive fracture treatment, and flap coverage. She now reports that she has difficulty ambulating.Examination includes a 20° equinovarus contracture, 2+ dorsiflexion, 2+ eversion, 5+ inversion, and 5+ plantar flexion strength. She has a supple forefoot and intact sensation throughout. Figures 48a through 48c are current weight-bearing radiographs. Attempted surgical correction should include Achilles lengthening, calcaneal osteotomy, and ---
1
flexor hallucis longus to peroneal transfer.
2
posterior tibial tendon transfer.
3
split anterior tibial tendon transfer.
4
first metatarsal osteotomy.
5
ankle arthrodesis.
The patient has developed an equinovarus contracture from overpull of the posterior tibial tendon, presumably due to the degloving injury and lack of protective splinting. In this instance, the patient is best treated with an Achilles lengthening, lateralizing calcaneal osteotomy, and posterior tibial tendon transfer. Flexor hallucis longus to peroneal transfer will not restore dorsiflexion. Ankle arthrodesis would allow deformity correction through the ankle joint but does not address the remainder of the foot,such that the patient would likely have trouble clearing the floor during the swing phase of gait. A first metatarsal osteotomy is indicated in the instance of a forefoot-driven cavus foot deformity. A split anterior tibial tendon transfer is indicated for correction of ankle and hindfoot varus contractures, and requires an intact and functional anterior tibial tendon, making it contraindicated in this instance.
QUESTION 40
The MRI scan of the ankle shown in Figure 50 reveals a tear of what structure?
1
Superficial peroneal retinaculum
2
Posterior tibial tendon
3
Peroneus longus tendon
4
Peroneus brevis tendon
5
Anterior talofibular ligament (ATFL)
The MRI scan shows a tear of a tendon behind the fibula. The peroneus brevis is deep to the longus (closer to the fibula). There should only be two structures behind the fibula, but the peroneus brevis tendon is shown as two distinct structures which is clearly
a longitudinal tear. The posterior tibial tendon would be posteromedial to the tibia. The superficial peroneal retinaculum is behind the fibula, but would show up as a tear if the peroneal tendons were dislocated, or lateral to the fibula. The ATFL runs from the anterior fibula to the talus.
QUESTION 41
What is the most common pathogen for soft-tissue infection of the foot caused by a puncture wound?
1
Staphylococcus aureus
2
Pseudomonas aeruginosa
3
Eikenella corrodens
4
Pasteurella multocida
5
Vibrio species
Staphylococcus and Streptococcus species are the most common causes of soft-tissue infections in the foot due to punctures. Pseudomonas is the most common cause of osteomyelitis of the foot due to puncture wounds. Pasteurella and Eikenella are seen in animal and human bites, respectively.Vibrio species are found in marine environments.
QUESTION 42
A 38-year-old man with a congenital pes cavus deformity reports lateral foot pain that has become increasingly debilitating. He has calluses over the lateral column and 3/5 muscle strength of the lateral compartment muscles. Nonsurgical management has failed to provide relief. In surgery, he undergoes a plantar fascial release, peroneus longus to brevis transfer, dorsiflexion osteotomy of the first metatarsal,and a Dwyer osteotomy. He has a hyperextended deformity of the first metatarsophalangeal joint. What tendon transfer will help to address this deformity?
1
Flexor hallucis longus
2
Extensor hallucis longus
3
Extensor hallucis brevis
4
Extensor digitorum longus
5
Tibialis anterior
In cavus foot reconstructions with a hyperextended deformity of the first metatarsophalangeal joint, a first-toe Jones procedure is indicated. This is an interphalangeal joint fusion of the first toe with an extensor hallucis longus tendon transfer. The flexor hallucis longus, extensor hallucis brevis, extensor digitorum longus, and tibialis anterior tendons are not of adequate length or in the correct direction to correct this deformity.
QUESTION 43
What is the most common complication following surgical treatment of a displaced talar neck fracture?
1
Osteonecrosis
2
Varus malunion
3
Posttraumatic arthritis
4
Fracture delayed union/nonunion
5
Wound dehiscence/delayed wound healing
The most frequent complication is posttraumatic arthritis. With talar neck fractures,osteonecrosis is relatively common, occurring in up to 50% of patients. Fracture nonunion occurs in 10%to 12% of patients. Varus malunion can occur with medial comminution. Wound dehiscence and deep infection are much less frequently encountered.
QUESTION 44
A 44-year-old woman with forefoot pain has pain with weight bearing during toe-off. She reports the pain is worse when she is barefoot and better when wearing tennis shoes. She has no numbness or tingling. Examination reveals increased pain with second toe dorsiflexion and plantar flexion. Traction to the second toe decreases pain with motion. She has no pain with medial lateral forefoot compression.Radiographically, her second metatarsal is longer than the first. What is the most likely diagnosis?
1
Second metatarsal stress fracture
2
Second metatarsophalangeal (MTP) synovitis
3
Second to third web space neuroma
4
Second flexible hammer toe
5
Transfer metatarsalgia
A test for metatarsophalangeal synovitis is pain with motion that is decreased with traction and motion. A patient with a neuroma typically has less pain when barefoot, does not have pain with MTP motion, and often has pain and a click with medial lateral forefoot compression. A metatarsal stress fracture would cause pain with weight bearing. The drawer test is the most useful test for diagnosis of instability of the metatarsophalangeal joint. Transfer metatarsalgia could be considered but typically does not cause pain with toe motion or have a positive drawer test.
QUESTION 45
Figure 55 is the radiographs of a 37-year-old patient who reports pain and swelling over the lateral forefoot (fifth metatarsal) that has become progressively worse over time. Shoe wear modifications have not been successful. Based on the radiographs, what is the appropriate treatment at this time? ---
1
Chevron osteotomy
2
Diaphyseal osteotomy
3
Metatarsal head resection
4
Exostectomy of the lateral eminence
5
Exostectomy of the lateral eminence with a fifth toe extensor tenotomy and capsular release
The most appropriate treatment is a diaphyseal osteotomy. The patient has a painful bunionette with a large 4-5 intermetatarsal (IM) angle (a type 3 bunionette) that is best treated with a diaphyseal or proximal osteotomy. Exostectomy of the lateral eminence applies to type 1 bunionettes that can
also have a fifth hammer toe. A Chevron osteotomy is best used for a type 1 or 2 bunionette with a normal 4-5 IM angle. A metatarsal head resection is not indicated as a primary procedure for a bunionette,especially in a younger patient because it sacrifices the fifth metatarsophalangel joint.
QUESTION 46
Figure 58 is the radiograph of a laborer who has hindfoot and ankle pain. He is a type 1 diabetic, and has a BMI of 25 and a Hgb A1c of 6. What is the most appropriate management at this time?
1
Total contact casting
2
Arthrodesis
3
Open reduction and internal fixation
4
Bed rest
5
Standard walking boot
The radiograph shows Charcot changes in the subtalar joint. In the absence of gross deformity, the initial treatment is nonsurgical, consisting of total contact casting, with frequent cast changes and progression to weight bearing when swelling subsides and early consolidation is seen radiographically. A walking boot will not provide sufficient immobilization, whereas bed rest carries the risk of significant deconditioning in an otherwise active patient with well-controlled diabetes. Surgery as the initial treatment is not indicated in the absence of gross deformity or ulceration.
QUESTION 47
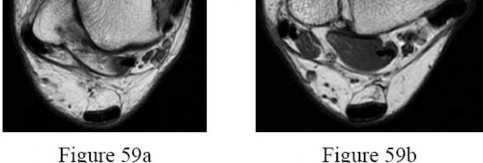
A 26-year-old competitive skier sustained an injury to her right ankle and now reports pain and clicking.Radiographs obtained at the time of the injury did not show any abnormality. She was diagnosed with an ankle sprain and treated in a short-leg cast for 6 weeks. While in the cast she was comfortable but the pain and clicking returned almost immediately after the immobilization was discontinued. Physical therapy has only made the problem worse. Current MRI scans are shown in Figures 59a and 59b. What is the most appropriate treatment at this time? ---
1
A stirrup splint
2
Continuation of cast immobilization until the clicking stops
3
Débridement and repair of longitudinal tears within the peroneal tendons
4
Débridement of the peroneal tendons, fibular groove deepening, and repair of the superior peroneal retinaculum
5
Excision of the region of the diseased peroneal tendon, tenodesis of the stumps to the intact tendon, and repair of the peroneal retinaculum
The MRI scans show dislocated peroneal tendons. Figure 59b reveals a convex fibular groove. Because cast immobilization has failed to provide relief,
débridement, fibular groove deepening,and repair of the superior peroneal retinaculum will address all of the patient’s problems. Further immobilization is unlikely to produce any improvement. A stirrup splint similarly is unlikely to give her relief. Surgical débridement with repair of tears would not alone prevent the recurrent dislocation.
There is no evidence of longitudinal tears based on the images. Excision of any area of diseased tendon with tenodesis to the remaining tendon does not address the problem of dislocation.
---
QUESTION 48
Figure 60 is the radiographs of a patient who underwent surgery to alleviate pain under her second metatarsal that is worsened by wearing high heel shoes. What is the most common complication of the osteotomy shown in the radiographs?
1
Osteonecrosis
2
Nonunion of the osteotomy
3
Significant transfer lesions
4
Metatarsophalangel (MTP) arthritis
5
Dorsiflexion contracture at the MTP joint
The radiographs show a Weil osteotomy that is used to treat metatarsalgia, which is often associated with severe claw toes. The most common complication is a floating toe, or dorsiflexion contracture
at the MTP joint. This is because the interossei muscles move dorsally with respect to the axis of the MTP joint due to depression of the plantar fragment and that the center of rotation is altered after the osteotomy. Multiple studies have shown that the floating toe is the main complication and that the other listed complications rarely occur with this type of osteotomy.
QUESTION 49
Figures 61a and 61b are the radiographs of a 56-year-old woman who reports medial foot and ankle pain and notes a progressive change in the shape of her foot over the past year. Her normal activities are limited by pain. Nonsurgical management has failed to provide relief. Pain is present from the navicular to the medial malleolus. Single leg heel rise is accompanied by correction of hindfoot valgus but is painful. What is the best course of treatment? --- ---
1
Débridement of the posterior tibial tendon
2
Transfer of the flexor digitorum longus to the medial navicular
3
Medializing calcaneal osteotomy with transfer of the flexor digitorum longus to the medial navicular
4
Medializing calcaneal osteotomy with lateral column lengthening and flexor digitorum longus transfer to the medial navicular
5
Triple arthrodesis
The radiographs reveal significant pes planus with a large degree of talar head uncoverage.This is a posterior tibial insufficiency with a stage 2 correctable deformity. Reconstruction requires tendon transfer, lateral column lengthening to address the talar uncoverage, and a medializing calcaneal osteotomy. The medializing calcaneal osteotomy corrects the hindfoot valgus and protects the tendon transfer.
Débridement of the posterior tibial tendon has been shown to be effective treatment for stage I adult-acquired flatfoot deformity but not more advanced stages. Transferring a tendon without correction of the hindfoot valgus will lead to early failure of the transfer. This patient does not require a triple arthrodesis because the deformity is supple and she has no radiographic evidence of arthritis.
QUESTION 50
A 72-year-old woman with a moderately reducible hallux varus has pain in the first metatarsophalangeal(MTP) joint that is activity related and reports that she cannot find any comfortable shoes. She wants to know what treatment plan offers her the most predictable outcome in terms of pain relief, activity, and the ability to get into shoes?
1
First MTP fusion
2
MTP joint replacement
3
Great toe amputation
4
Keller resection arthroplasty
5
Tendon transfer and capsular release
A great toe fusion is the most appropriate treatment. It is an excellent procedure for pain relief and it gives a predictable result for return to activity and lack of recurrence. A soft-tissue correction is not indicated due to patient age and reducibility. An amputation is not indicated in this case in terms of activity level and is an unreasonable choice for an otherwise healthy 72-year-old patient. The Keller resection arthroplasty and the MTP joint replacement allow motion, but they offer unpredictable results for pain relief, activity, and recurrence.
QUESTION 51
A 43-year-old woman with long-standing rheumatoid arthritis has a large prominence with soft-tissue swelling under the fifth metatarsal head and over the lateral eminence of the fifth metatarsophalangeal(MTP) joint. She has minimal hammer toes with no significant metatarsalgia. Radiographs show a 4-5intermetatarsal angle of 7° and a congruent fifth MTP joint. What is the recommended surgical treatment to address this problem?
1
Simple exostectomy
2
Metatarsal head excision
3
Distal metatarsal osteotomy
4
Diaphyseal metatarsal osteotomy
5
Simple exostectomy with soft-tissue mass excision
Exostectomy with soft-tissue mass excision is the treatment of choice. The patient has a type 1 bunionette but most of her symptoms are coming from a rheumatoid nodule that is under the metatarsal head. This is mainly a soft-tissue problem and does not require any type of osteotomy because the 4-5 intramedullary angle is minimally elevated. A metatarsal head resection is commonly performed in patients with rheumatoid arthritis, but is not indicated in this patient because there is a normal fifth MTP joint and no metatarsalgia.
QUESTION 52
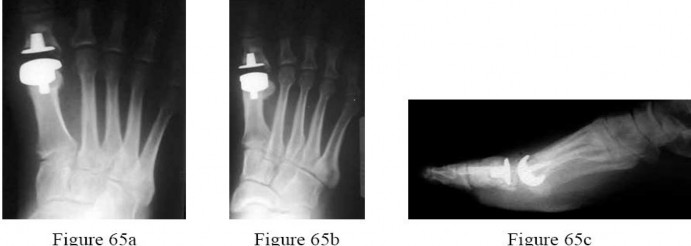
Figures 65a through 65c are the weight-bearing radiographs of a 42-year-old male manual laborer who has a 6-month history of persistent great toe swelling and pain after undergoing a total joint Arthroplasty for hallux rigidus 9 months ago. He denies postoperative wound complications, recent fevers, chills, or other constitutional signs; however, he has never been able to ambulate without pain since his return to work. Examination reveals moderate diffuse swelling, but no fluctuance or drainage.
Range of motion includes 25° of dorsiflexion. Laboratory studies show an erythrocyte sedimentation rate of 18 mm/h and a c-reactive protein level of <0.7 mg/L. What is the most likely source of his symptoms? ---
1
Septic arthritis
2
Mechanical failure
3
Periprosthetic fracture
4
Aseptic loosening from polyethylene debris
5
Metatarsal shortening/transfer metatarsalgia
The patient has developed mechanical failure as evidenced by the lucency surrounding the proximal phalanx component. His pain has correlated with his return to work as a manual laborer.Although septic arthritis is a possibility, it is less likely based on the normal laboratory studies and lack of infectious signs. Periprosthetic fracture is unlikely because of the lack of a traumatic event or a sudden change in symptoms rather than a persistent inability to progress his activities. A transfer lesion from metatarsal shortening would result in pain from mechanical overload at areas adjacent to the first
metatarsal. Aseptic loosening from polyethylene debris would imply that the implant has previously been stable and well-fixed, and subsequently loosened over an extended period of time.
QUESTION 53
A patient with foot pain is noted to have a cavovarus foot. The heel corrects to slight valgus on Coleman block testing. This finding indicates that the deformity should correct with which of the following procedures?
1
Triple arthrodesis
2
Subtalar arthrodesis
3
Peroneal brevis lengthening
4
Medializing calcaneal osteotomy
5
Dorsiflexion first metatarsal osteotomy
The Coleman block test is used to demonstrate a flexible hindfoot. If the heel corrects from varus to neutral or slight valgus by bearing weight on a block supporting the lateral column of the foot, the subtalar joint remains flexible. This indicates that the varus position is secondary to the plantar flexed first ray or valgus position of the forefoot. Therefore, the most appropriate procedure is a dorsiflexion first metatarsal osteotomy. Arthrodesis is indicated in degenerative conditions. The peroneal brevis does not contribute to the cavus foot deformity. Medializing calcaneal osteotomy assists in correction of a flexible flatfoot.
QUESTION 54
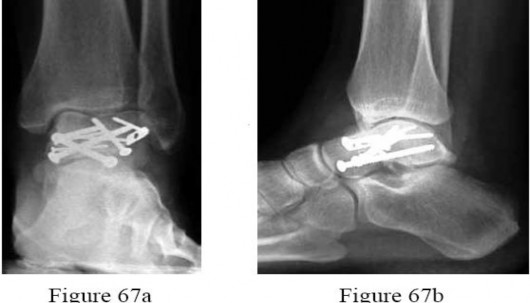
A 19-year-old woman sustained a displaced talar neck fracture while cliff jumping. The fracture is managed with open reduction and internal fixation. Which of the following best describes the findings in the 2-months postoperative radiographs shown in Figures 67a and 67b, and subsequent treatment plan? ---
1
There is a positive Hawkins sign, indicating the patient is unlikely to develop osteonecrosis.
2
There is a positive Hawkins sign, indicating the patient has developed osteonecrosis.
3
Hawkins sign cannot be determined on radiographs; therefore, MRI is required.
4
No Hawkins sign is visible, and therefore the patient is not likely to develop osteonecrosis.
5
No Hawkins sign is visible; therefore, the patient should be kept non-weight-bearing until a Hawkins sign appears
The radiographs reveal a positive Hawkins sign, a subchondral lucency in the talar dome best seen on a mortise radiograph indicating viability of the talar body. Once a Hawkins sign appears,it is unlikely that that the patient will develop osteonecrosis.
Osteonecrosis is best diagnosed with radiographs. Although MRI can be helpful in assessing the extent of osteonecrosis, it is unnecessary for purely diagnostic purposes. A Hawkins sign typically will appear at 6 to 8 weeks after fracture; however,the absence of a Hawkins sign at that time does not necessarily indicate osteonecrosis. Most authors agree that even in the absence of a Hawkins sign, weight bearing can commence at 10 to 12 weeks after surgery.
QUESTION 55
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident.The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria?
1
Clostridium
2
Acinetobacter
3
Pseudomonas
4
Mycobacterium
5
Staphylococcus aureus
In farm or soil-contaminated wounds, including lawnmower injuries, penicillin is added to broad-spectrum cephalosporin and aminoglycoside therapy to cover against Clostridium. Psuedomonas is frequently seen after puncture wounds through the shoes. Acinetobacter is generally a hospital-acquired infection.
QUESTION 56
A 35-year-old man sustains a large degloving injury overlying the distal tibia. The traumatic wound is managed with surgical débridement, followed by application of a negative pressure dressing. Compared with standard damp-to-dry dressing changes, use of a negative pressure dressing offers which of the following advantages?
1
Increased limb vascularity
2
Decreased hospital stay
3
Decreased bacterial count
4
Decreased need for repeat débridement
5
Accelerated granulation tissue formation
The development of negative pressure dressings has been a significant advance in wound management. These devices remove excess interstitial fluid, which promotes increased local vascularity and, with mechanical deformation of cells from the negative pressure, accelerates granulation tissue formation. A negative pressure dressing does not substitute for thorough surgical débridement; it has not been shown to decrease bacterial counts within the wound or decrease overall length of hospital stays.
QUESTION 57
What is the most common cause of persistent pain after excision of a Morton neuroma?
1
Tarsal tunnel syndrome
2
Painful plantar scar formation
3
Metatarsophalangeal joint synovitis
4
Presence of an amputation stump neuroma
5
Inadequate resection of an interdigital neuroma
The most frequent cause of recurrent pain after neuroma excision is tethering of the common digital nerve to the plantar skin by plantar-directed branches of the nerve, possibly preventing retraction of the nerve, due to inadequate resection of the neuroma. These plantar branches were not found to be present 4 cm proximal to the transverse metatarsal ligament. Therefore, an effort should be made to cut the nerve at this level.
QUESTION 58
A 40-year-old man with lateral column overload and a cavovarus foot has failed to respond to nonsurgical management. Examination reveals an Achilles tendon contracture. With the knee in extension, ankle dorsiflexion is to neutral; with the knee in flexion, ankle dorsiflexion is to 15°. In addition to correction of the cavovarus deformity, what is the most appropriate surgical management with regard to the Achilles tendon contracture?
1
Heel cord lengthening
2
Percutaneous Achilles tendon lengthening
3
Open Achilles tendon lengthening
4
Gastrocnemius recession
5
Gastrocnemius and soleus recession
The Silfverskiold test indicates that the patient has an isolated contracture of the gastrocnemius; therefore, a gastrocnemius recession is indicated. Open Achilles tendon lengthening,gastrocnemius and soleus recession, and percutaneous Achilles tendon lengthening are all indicated for management of concomitant gastrocnemius and soleus contractures.
QUESTION 59
A 28-year-old man reports a 3-month history of foot pain and swelling after stepping on a nail while working at a construction site. He was wearing rubber-soled boots at the time he sustained this deep puncture wound. Initial management consisted of tetanus prophylaxis, superficial wound cleansing, and oral antibiotics.
Imaging shows no evidence of bony infection. What is the most appropriate treatment?
1
IV antibiotics
2
Reinstitution of oral antibiotics
3
CT-guided drainage procedure and IV antibiotics
4
Surgical wound exploration with débridement followed by hydrotherapy
5
Surgical wound exploration with débridement and IV broad-spectrum antibiotics
Patients wearing rubber-soled shoes while sustaining deep puncture wound injuries to the foot may experience complications such as abscess formation and osteomyelitis. Frequently, there is delayed diagnosis of potential retained foreign bodies. Therefore, appropriate treatment involves wound exploration, débridement with removal of the foreign material, and IV antibiotics. A combination of formal surgery and administration of antibiotics is required for treatment of these deep wound infections;drainage or antibiotics alone will not suffice.
QUESTION 60
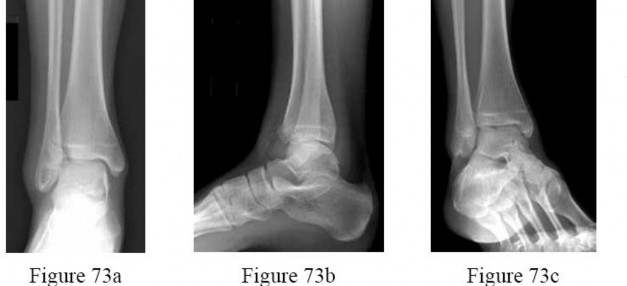
Figures 73a through 73c are the radiographs of a 14-year-old girl who sustained an ankle injury in a fall.What ligament is attached to the displaced fragment? ---
1
Long plantar ligament
2
Anterior talofibular ligament
3
Posterior talofibular ligament
4
Anterior inferior tibiofibular ligament
5
Posterior inferior tibiofibular ligament
The patient has sustained a Tillaux fracture. This fracture of the anterolateral portion of the distal tibia epiphysis occurs in early adolescence. The medial portion of the growth plate fuses first.The anterior inferior tibiofibular ligament attaches to the anterolateral portion of the tibial epiphysis and avulses the fragment, usually in response to an external rotation force. The other named ligaments are lateral in location but do not attach to the shown tibial fragment.
QUESTION 61
When using a single-incision flexor hallucis longus transfer for augmentation of a repair for chronic Achilles tendon rupture, which of the following can be expected?
Transfer metatarsalgia of the lesser metatarsal heads
4
Increased plantar pressure at the first metatarsal head
5
Increased recruitment of the short hallucal flexors
The only significant change occurring after transfer of the flexor hallucis longus for chronic Achilles ruptures and Achilles tendinosis findings was decreased hallucal phalangeal pressure. No transfer metatarsalgia or increased pressure under the first metatarsal head was found. AOFAS MTP-IP scores remained high and averaged 96.4 out of 100.
QUESTION 62
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome?
1
Physical therapy
2
Early weight bearing
3
Anatomic alignment
4
Early range of motion of the ankle
5
Calcium and vitamin D administration
The only factor that is prognostic for outcomes is the quality of the reduction. None of the other factors has any effect on the outcome. Early range of motion or physical therapy may offer temporary effects, but these small advantages do not last beyond 3 months after surgery.
QUESTION 63
Recurrence of hallux valgus deformity after corrective surgery has been shown to be related to which of the following?
1
Inversely correlated with presence of bipartite fibular sesamoid
2
Associated with residual increased tibial sesamoid displacement
3
Associated with squared lateral first metatarsal shape
4
Unrelated to preoperative 1-2 intermetatarsal angle
5
Unrelated to preoperative hallux valgus angle
DISCUSSION: Okuda and associates have studied the factors associated with the recurrence of hallux valgus deformity following correction with proximal first metatarsal osteotomy. The factors that they found associated with recurrence of deformity postoperatively are a rounded shape to the lateral first metatarsal head, severe lateral displacement of the tibial sesamoid, an increased preoperative 1-2 intermetatarsal angle, and an increased preoperative hallux valgus angle. The reported rate of recurrence of deformity after proximal first metatarsal osteotomy is 4% to 11%. PREFERRED RESPO: 2 Question 79 A 33-year-old woman has had plantar first metatarsophalangeal joint pain for 3 years. Examination reveals that she is tender under the medial sesamoid. She has no swelling or ecchymosis. The first metatarsophalangeal joint motion is equal and stable bilaterally. Radiographically, there is some fragmentation of the medial sesamoid with increased density in some of the fragments. Various orthotic and shoe modifications have failed to provide relief. What is the most appropriate management?
Medial sesamoid stress fractures with fragmentation that have not responded to nonsurgical management have done well after sesamoid excision. Excision of both sesamoids is not recommended. A first metatarsophalangeal joint arthrodesis is not going to resolve the issue of weight loading on the stress fractured, fragmented sesamoid. Open reduction can be considered if there are two large fragments without osteonecrosis. Corticosteroid injection is not going to provide long-term relief.Shoe modifications have already been tried, without relief.
QUESTION 64
What is the most common organism in osteomyelitis of the foot that results from a puncture wound in a non-diabetic patient?
1
Proteus
2
Clostridia
3
Pseudomonas
4
Streptococcus
5
Staphylococcus aureus
Although Staphylococcus aureus is the most common causative agent for soft-tissue infection following puncture wounds of the foot, pseudomonas is the most common organism found when osteomyelitis occurs.
QUESTION 65
A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the site of the tenderness, about 7 cm above the lateral heel, provided temporary relief of the pain. What is the recommended course of management for the persistent burning pain?
1
Subtalar fusion
2
Neuroplasty of the superficial peroneal nerve
3
Neuroplasty of the sural nerve and implant removal
4
Excision and burial of the sural nerve in deep muscle or vein
5
Electromyography/nerve conduction velocity studies to evaluate local nerve entrapment versus radiculopathy
The patient has a sural nerve neuroma, which is a known complication of the extensile lateral approach. Of the available choices, excision and burial of the sural nerve in muscle or vein is the best choice because it gives better pain relief due to the better blood supply in muscle than bone. Recent authors advocate burying the nerve in
vein as the best option. Neuroplasty is a possibility (but not of the superficial peroneal nerve), but the sural nerve is usually very sensitive and often pain relief with a release is incomplete. Additionally, implant removal is not indicated because of the patient’s
complaints; also,the implants should not be removed at 6 months. A subtalar fusion is the choice for posttraumatic arthritis from the calcaneus fracture. Electromyography/nerve conduction velocity studies are reasonable choices if there was an indication the pain could be coming from the back or there was no clear evidence of a sural nerve neuroma.
QUESTION 66
A cavovarus foot reconstruction is planned. Which of the following tendon transfers will decrease the plantar flexion forces being applied to the first metatarsal head?
1
Split anterior tibial tendon transfer
2
Peroneal longus to peroneal brevis
3
Flexor digitorum to posterior tibial tendon
4
Flexor digitorum longus to extensor digitorum longus
5
Posterior tibial tendon transfer through the interosseous to the dorsal lateral cuneiform
Cavus results from muscle imbalances in both the intrinsic and extrinsic groups.Weakness of the anterior tibialis with strong peroneal longus muscle tone is believed to be one of the factors causing a plantar flexed first metatarsal. The flexor digitorum longus to posterior tibial tendon transfer is used for posterior tibial tendon dysfunction. Posterior tibial tendon transfer to the dorsal foot is used to help correct weak dorsiflexion. The split anterior tibial tendon transfer is used to help correct equinovarus deformities or excessive forefoot inversion during the swing phase. Flexor digitorum longus to extensor digitorum longus transfers are used for correction of flexible hammer or claw toes.
QUESTION 67
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for?
1
Cardiovascular evaluation
2
Ophthalmologic evaluation
3
MRI of the spine
4
Radiographs of the hip
5
Genetic testing
The current diagnostic criteria for Marfan syndrome, called the Ghent criteria, are based on clinical findings and family history. The role of genetic testing in establishing the diagnosis is limited,because testing for FBN1 mutations is neither sensitive nor specific for Marfan syndrome. By making the diagnosis and arranging for cardiovascular evaluation, the orthopaedic surgeon can help prevent sudden death in these patients. The cardiovascular manifestations, including dissection and dilation of the ascending aorta and mitral valve prolapse, are responsible for nearly all of the precocious deaths of patients with Marfan syndrome. Patients with Marfan syndrome do have problems with protrusion acetabuli, scoliosis, and opthalmologic problems but the life-threatening problem that must be considered is the risk of cardiovascular sudden death.
---
QUESTION 68
A 35-year-old man sustained a Lisfranc dislocation 2 years ago. He was treated with standard open reduction and fixation. At 4 months, the screws were removed. He now has increasing pain and discomfort. A current radiograph is shown in Figure 85. What is the best treatment option?
1
Reduction and fusion of the medial three tarsometatarsal (TMT) joints
2
Reduction and fusion of all five tarsometatarsal joints
3
Revision open reduction and internal fixation with bridge plates to avoid further damage to the joints
4
Revision open reduction and internal fixation but leave the screws in indefinitely
5
Soft-tissue interpositional grafts for the tarsometatarsal joints
The most reliable treatment will be a reduction and fusion of the medial three TMT joints.There is adequate proof in the literature that fusion of all five TMT joints should be avoided because the fusion rate as well as functional outcome is inferior with fusion of all five joints compared with fusion of the medial three TMT joints and preservation of mobility in the 4-5 TMT joints. There is too much deformity and arthritis to warrant a revision open reduction and internal fixation. An interpositional graft is not proven to help in this situation because it neither corrects the deformity nor aids in stability.
---
QUESTION 69
Figures 87a and 87b are the radiographs and MRI scan of a 17-year-old cross country runner who reports pain in his forefoot around the third and fourth metatarsals. The pain is mostly on top of the foot and appears to be activity related. There is minimal swelling on examination and diffuse tenderness over the third and fourth metatarsal shafts. What is the most appropriate management? ---
1
Three-phase bone scan
2
Bone density examination
3
Non-weight-bearing short-leg cast
4
Fracture boot with weight bearing as tolerated
5
Limit his miles and repeat radiographs in 2 weeks
The most appropriate management is a fracture boot with weight bearing as tolerated.The radiographs are normal, but the history strongly suggests a metatarsal stress fracture. The MRI scan clearly shows edema of the third metatarsal which is consistent with a stress fracture. Patients can be treated successfully with weight-bearing
immobilization and activity modification. Some physicians treat metatarsal base fractures with limited weight bearing. Limiting his miles and repeat radiograph in 2 weeks would be an acceptable option if the MRI scan showing the fracture had not been obtained. A bone density examination typically will be normal in a teenager, and it does not help in treatment. A bone scan is a good test to diagnose the fracture, but an MRI scan has already been obtained.
QUESTION 70
The peroneus brevis is the primary antagonist to which of the following structures?
1
Anterior tibialis
2
Posterior tibialis
3
Peroneus longus
4
Flexor hallucis longus
5
Extensor hallucis longus
The primary function of the peroneus brevis is eversion of the foot, thus acting as the primary antagonist of the posterior tibialis, which inverts the foot, and secondarily plantar flexes the ankle.The anterior tibialis secondarily inverts the foot and only acts as a partial antagonist of the posterior tibialis. The peroneus longus plantar flexes the first ray.
QUESTION 71
Lisfranc’s ligament connects which of the following structures?
1
Base of the first metatarsal to the base of the second metatarsal
2
Base of the first metatarsal to the middle cuneiform
3
Base of the second metatarsal to the middle cuneiform
4
Base of the second metatarsal to the medial cuneiform
5
Medial cuneiform to the middle cuneiform
The stability of the Lisfranc joint complex results from bony and ligamentous contributions. The metatarsal cuneiform articulations form a Roman arch configuration. The second metatarsal is recessed between the medial and lateral cuneiforms, adding more stability. Strong intermetatarsal ligaments are present between each of the lateral four metatarsals but are absent between the first and second metatarsals. In this region, the base of the second metatarsal is joined to the medial cuneiform by Lisfranc’s ligament.
QUESTION 72
A football player who injured his right lower extremity during a game could not get up and reported extreme pain. The initial sideline evaluation showed a probable anterior cruciate, posterior cruciate,and lateral collateral ligament rupture with a very unstable knee. He also reports pain in his ankle and is unable to dorsiflex the ankle. He has limited sensation over the dorsum of his foot. Examination reveals no swelling of the ankle and no pain with passive range of motion of the ankle. What is the most likely diagnosis?
1
Tibial nerve injury
2
Associated ankle fracture
3
Acute compartment syndrome
4
Injury to the common peroneal nerve
5
Rupture of the tibialis anterior tendon
It is not uncommon to sustain a peroneal nerve injury in association with a knee dislocation or multi-ligament injury. There should always be a high index of suspicion for this injury, and the vascular status to the leg should be carefully evaluated. From the history and examination, there is no indication that the ankle was fractured. A compartment syndrome will not develop within a few minutes of the injury. It takes several hours for a compartment syndrome to develop and become symptomatic.The tibial nerve supplies the plantar aspect of the foot. An acute rupture of the tibialis anterior tendon in a young person is very uncommon, and it is associated with pain and localized swelling about the ankle. It is also unlikely that it would lead to sensory loss. 56
---
QUESTION 73
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?
1
MRI
2
Custom orthotics
3
Activity modification
4
Calcaneal epiphysiodesis
5
Percutaneous Achilles tendon lengthening
The patient has calcaneal apophysitis, an overuse syndrome common in children ages 9 to12 years. Symptoms are usually the result of excess tension and a tight heel cord. Management includes activity modification, as well as heel cord stretching, nonsteroidal anti-inflammatory drugs, icing, and other modalities. Radiographs are typically negative; MRI is unnecessary. Custom orthotics are not indicated. The condition is self-limiting, in that the symptoms fully resolve once the apophyses fuses,such that surgery is rarely indicated.
QUESTION 74
Figures 92a through 92c are the clinical photographs and radiograph of a 22-year-old man who has had a 6-month history of lateral ankle pain following minor ankle trauma. He has undergone physical therapy,which only made it more symptomatic. What is the most appropriate management? ---
1
Arthrodesis
2
Bar resection
3
Immobilization
4
Corrective osteotomy
5
Injection of the peroneal tendons
The clinical photographs show a rigid pes planus, with the radiograph showing a calcaneonavicular coalition. Most patients will have symptomatic improvement with a short course of immobilization. Only after that has failed would surgery be contemplated. Although the pain may be along the peroneal tendons, injecting them will not yield long-term relief because their symptoms are only secondary to the tarsal coalition.
QUESTION 75
A 50-year-old woman with a mild flexible planovalgus foot deformity has lateral hindfoot pain. What is the simplest modification of her shoe wear to help offload the lateral hindfoot?
1
Medial hindfoot posting
2
Lateral hindfoot posting
3
Rigid foot orthotic
4
Semi-rigid foot orthotic
5
Accommodative foot orthotic
DISCUSSION: Lateral hindfoot pain is often the result of impingement as the planovalgus foot pronates and abducts. Medial hindfoot posting or wedge will elevate the medial aspect of the heel and decrease the lateral hindfoot pressures. This may be done in a dress shoe as well as a tie shoe with a simple heel posting wedge. Adding lateral hindfoot posting would increase the lateral pressures. An orthotic, whether rigid, semi-rigid, or accommodative, will support the arch but without medial hindfoot posting, the foot will often still pronate and abduct with continued lateral hindfoot pressure. PREFE RESP: 1 Question 94 Figures 94a through 94d are the weight-bearing radiographs of a 45-year-old man who is an avid tennis player and has intermittent lateral midfoot pain. He has sustained three ankle sprains in the past 10 years and has occasional sensations of instability. Examination includes mild laxity with lateral ankle ligament testing, normal ankle and hindfoot motion, a supple forefoot, and no ankle joint line pain. What is the most appropriate management?
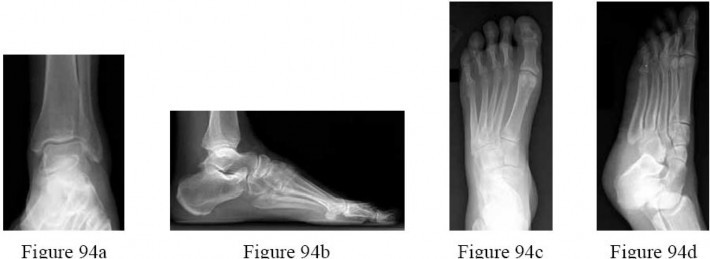
The patient has lateral column overload and functional ankle instability due in part to the subtle cavus foot. Because of the cavus posture and mild ankle instability, physical therapy and a cavus foot orthotic are indicated. Although MRI can be of benefit in the diagnosis of osteochondral lesions of the talus, it is of little value in this patient based on the absence of ankle joint line symptoms.NSAIDs and lace-up bracing can be helpful with regard to the ankle, but do not address the lateral column overload. Orthotic management with arch support and medial posting is contraindicated with a cavus foot deformity. Temporary immobilization would be indicated in the event of a suspected stress fracture, in which case the lateral midfoot symptoms would be more constant in nature.
QUESTION 76
A 49-year-old woman underwent a successful right ankle fusion. She now reports an altered gait. In an attempt to improve her gait, what is the most appropriate device?
1
Arizona brace
2
Rocker-bottom sole
3
Double upright drop-lock brace
4
Non-articulated ankle-foot orthosis
5
Carbon fiber insert with a Morton’s extension
The plantar flexion-dorsiflexion motion of the ankle can be partially mimicked with a rocker-bottom shoe adaptation. A carbon fiber insert would not provide any improvement in her gait. An ankle-foot orthosis, Arizona brace, and double upright drop-lock brace would immobilize the ankle, which is already achieved with the ankle fusion.
QUESTION 77
With respect to the clinical photograph shown in Figure 97, what artery provides the most blood supply to the area of the planned incision?
1
Lateral tarsal
2
Lateral calcaneal
3
Lateral malleolar
4
Common peroneal
60
5
Artery of the tarsal sinus
The photograph shows the planned incision for an extensile lateral approach to the calcaneus. The lateral calcaneal artery, usually a branch of the peroneal artery, provides blood supply to the majority of the full-thickness flap of an extensile lateral approach. Other branches also contribute,including the lateral malleolar and lateral tarsal arteries, although to a lesser degree.
QUESTION 78
A 39-year-old woman sustains a grade III inversion ankle sprain and is treated with boot immobilization,crutches, and physical therapy, through her primary care physician. The patient is referred for evaluation 3 weeks later because of persistent pain and inability to bear weight. Examination reveals mild residual swelling and exquisite tenderness to light touch overlying the anterolateral ankle and dorsolateral foot.Passive range of motion also reproduces extreme pain. Radiographs are negative for fracture and an MRI scan shows a tear of the anterior talofibular ligament. What is the most appropriate management?
1
Cast immobilization
2
Anticonvulsant therapy
3
Brostrom ligament reconstruction
4
Ankle arthroscopy with débridement
5
Proprioceptive physical therapy and a lace-up ankle brace
The patient has most likely developed a stretch neurapraxia of the superficial peroneal nerve. Localized pain, particularly to light touch which has not improved after 3 weeks (in this instance) raises the likelihood of a neurologic etiology. Anticonvulsant medication, such as gabapentin or pregabalin, can be invaluable in dissipating and often resolving neuritic symptoms. Antidepressant medication, such as amitriptyline, could alternatively be used. Proprioceptive physical therapy is likely to worsen the neuritic symptoms, but may be indicated once the neuritic symptoms subside. Cast immobilization can be used acutely in promoting dissipation of swelling and offering soft-tissue support;however, further immobilization in this instance is likely to be of limited benefit. Surgical intervention is not indicated in the acute management of ankle sprains.
QUESTION 79
Which of the following factors predisposes patients undergoing lateral ankle reconstruction to surgical failure?
1
Low functional demand
2
Anatomic reconstruction
3
Cavovarus foot deformity
4
Planovalgus foot deformity
5
History of acute instability (preoperative)
Bony malalignment such as hindfoot varus, first ray plantar flexion, or cavovarus foot deformity renders patients more susceptible to chronic lateral ankle sprains and can cause failure of isolated lateral ankle reconstruction. Planovalgus foot deformity principally strains the medial ankle ligamentous structures. Low functional demand patients, as well as patients with a preoperative history of acute traumatic ankle instability and patients undergoing anatomic reconstruction all have decreased rates of surgical failure with lateral ankle ligament reconstruction.
QUESTION 80
A 63-year-old man has long-standing type 2 diabetes. He has had associated ongoing neuropathy for approximately 5 years. He now reports a red, hot, swollen right foot for the past 2 days. You place him supine in your office with the foot elevated for 30 minutes. You return to see that the redness has dissipated. What is the most likely diagnosis?
1
Cellulitis
2
Osteomyelitis
3
Charcot arthropathy
4
Sjogren syndrome
5
Reynaud syndrome
Charcot arthropathy is a progressive condition of the musculoskeletal system that is characterized by joint dislocations, pathologic fractures, and debilitating deformities. This disorder results in progressive destruction of bone and soft tissues at weight-bearing joints; in its most severe form, it may cause significant disruption of the bony architecture. In patients with diabetes, the incidence of acute Charcot arthropathy of the foot and ankle ranges from 0.15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot’s skin temperature), erythema,joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective
sensation, are often pathognomonic of acute Charcot arthropathy.Cellulitis is an infection of the skin and osteomyelitis is an infection of the bone; examination of the limb would remain unchanged after 30 minutes of elevation. Reynaud and Sjogren syndromes are rheumatologic conditions that do not have these symptoms. CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 103
A 27-year-old woman has had pain in her right ankle for 2 years. Examination reveals a slightly warmjoint, without erythema. Ankle range of motion is limited by pain.
Radiographs are unremarkable.Because management consisting of immobilization, nonsteroidal anti-inflammatory drugs, and physiotherapy has failed to provide relief, MRI scans are obtained and shown in Figures 101a and 101b.An intraoperative image and the histology are shown in Figures 101c and 101d.
---
QUESTION 81
What is the best descriptor for the lesion shown in Figures 101a and 101b?
1
Normal anatomic variant
2
Inflammatory
3
Dedifferentiated malignancy
4
Well-differentiated malignancy
5
Locally aggressive
_ _
QUESTION 82
The orthopaedic surgeon treats the lesion arthroscopically. An intraoperative image is shown in Figure101c. What is the most appropriate immediate treatment?
1
Careful removal of the instrumentation without disrupting the lesion
2
Obtain a tissue biopsy, removal of the instrumentation, and wound closure
3
Obtain a tissue biopsy and perform an extensive arthroscopic débridement
4
Place a supramalleolar tourniquet to prevent metastasis of tumor cells
5
Transilluminate the lesion with the arthroscope and place sutures in the overlying skin forfuture brachytherapy catheter placement
_ _
QUESTION 83
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
1
Arthrofibrosis
2
Local recurrence
3
Chondrolysis
4
Disseminated infection
5
Metastasis
_ _
_**DISCUSSION FOR QUESTIONS 101 THROUGH 103:**_
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
1. # Toe is fused too straight (plantar flexed)
2. # Toe is fused in too much valgus
3. # Toe is fused in too much dorsiflexion
4. # There is a nonunion of the fusion
5. # Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
QUESTION 84
What structure attaches at the fracture site shown in Figures 107a and 107b?
1
Anterior talofibular ligament (ATFL)
2
Anterior inferior tibiofibular ligament (AITFL)
3
Deltoid ligament
4
Calcaneofibular ligament (CFL)
5
Superficial peroneal retinaculum (SPR)
_** **_
QUESTION 85
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
1
Brostrom procedure
2
Syndesmosis repair or stabilization
3
Allograft lateral ligament reconstruction
4
Excision of loose body/fracture fragment
5
Repair of the SPR with possible fibular groove deepening
_** **_
_**DISCUSSION FOR QUESTIONS 107 AND 108:**_
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.