Score: 0%
100 Random Orthopedic MCQs for Board Prep (2026 Update)
Which of the following fascial structures does not contribute to the formation of the spiral cord:
The main blood supply to the capital femoral epiphysis in a 10-year-old child is supplied from the ](http://www.orthobullets.com/anatomy/10123/hip-blood-supply)
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?


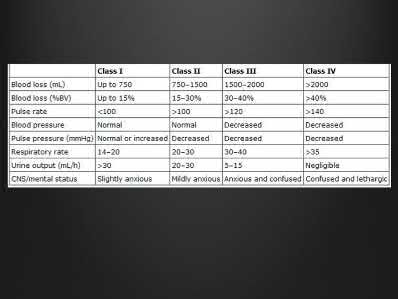
A 20-year-old man who sustains closed femoral and tibial shaft fractures has
2. mild distention of the abdomen, a systolic blood pressure of 75 mm Hg, and a
3. pulse rate of 135/min. His neurovascular examination is normal. Lateral
4. cervical spine, chest, and AP pelvis radiographs are normal. After
5. administration of 2 L of crystalloid, he has a systolic blood pressure of 95 mm
6. Hg and a pulse rate of 120/min. Management should now include
7. 1- diagnostic peritoneal lavage.
8. 2- immediate femoral nailing and splinting of the tibia.
9. 3- immediate stabilization of both the femur and the tibia.
10. 4- splinting the tibia and placing the femur in skeletal traction.
11. 5- simultaneous retrograde femoral nailing and an exploratory laparotomy.
2. mild distention of the abdomen, a systolic blood pressure of 75 mm Hg, and a
3. pulse rate of 135/min. His neurovascular examination is normal. Lateral
4. cervical spine, chest, and AP pelvis radiographs are normal. After
5. administration of 2 L of crystalloid, he has a systolic blood pressure of 95 mm
6. Hg and a pulse rate of 120/min. Management should now include
7. 1- diagnostic peritoneal lavage.
8. 2- immediate femoral nailing and splinting of the tibia.
9. 3- immediate stabilization of both the femur and the tibia.
10. 4- splinting the tibia and placing the femur in skeletal traction.
11. 5- simultaneous retrograde femoral nailing and an exploratory laparotomy.
A mutation in which of the following genes causes a disturbance in normal limb outgrowth patterning:
of 100
The best treatment is
The best treatment is
The best index to measure acetabular deficiency in the coronal plane is:
of 100
When performing an index finger ray amputation, the orthopaedic surgeon should move the
When performing an index finger ray amputation, the orthopaedic surgeon should move the
An 85-year-old woman falls and injures her elbow in her non dominant arm. Radiographs are shown in Figure A and
-
A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
of 100
The most common extraskeletal manifestation of this disease is
The most common extraskeletal manifestation of this disease is
A 24-year-old man has a deep knife wound across the dorsal aspect of his wrist, transecting all of his wrist and finger extensor tendons. How does the surgeon determine which of the proximal tendon stumps in the fourth dorsal compartment is the extensor indicis proprius? ](http://www.orthobullets.com/anatomy/10040/extensor-indicis)Review Topic
of 100
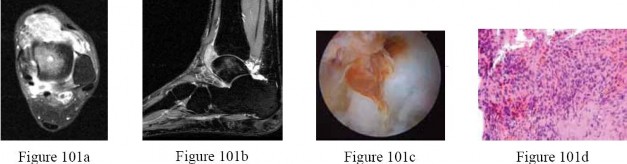
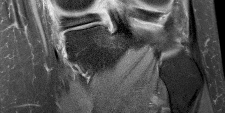
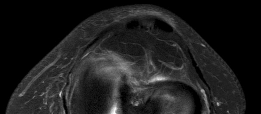
Figures 32a through 32d are the radiographs and MR images of a 13-year-old girl with new posterolateral knee pain following a fall. What is the best next step?



Figures 32a through 32d are the radiographs and MR images of a 13-year-old girl with new posterolateral knee pain following a fall. What is the best next step?
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
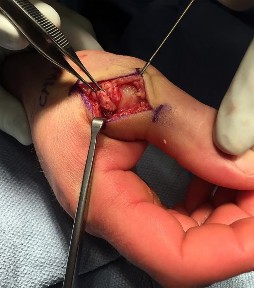
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
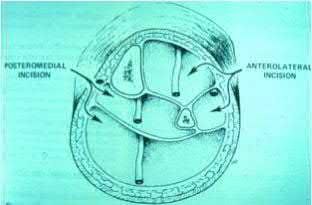
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---

Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
Anatomic reduction and stabilization of the posterior malleolus fracture component
---
The clinical photograph of the hand of a 72-year-old woman who sustained a
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
2. laceration of the flexor pollicis longus in her thumb is shown in Figure 45. She
3. cannot actively flex the interphalangeal joint. Which pulley, in addition to the
4. oblique pulley, has been lacerated?
5. 1- A-1
6. 2- A-2
7. 3- A-3
8. 4- A-4
9. 5- A-5
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?


Slide 1 Slide 2
A 42-year-old male patient presents with a history of repeated giving way of his ankle. He notes that this has been present for 1 year. He does not experience any pain, even with the episodic bouts of the ankle buckling. On examination, the ankle range of motion is normal, no pain is elicited, and there is no crepitus. A stress radiograph (Slide 1) and a lateral weight-bearing radiograph (Slide 2) are presented. The patient does not want to undergo surgery, but he needs to know the possibility of problems with his ankle in the future. The patient should be advised that:
A 42-year-old male patient presents with a history of repeated giving way of his ankle. He notes that this has been present for 1 year. He does not experience any pain, even with the episodic bouts of the ankle buckling. On examination, the ankle range of motion is normal, no pain is elicited, and there is no crepitus. A stress radiograph (Slide 1) and a lateral weight-bearing radiograph (Slide 2) are presented. The patient does not want to undergo surgery, but he needs to know the possibility of problems with his ankle in the future. The patient should be advised that:
of 100
A concussion diagnosis is made when there is







A concussion diagnosis is made when there is
Figure 11a is the radiograph of a 45-year-old woman with a moderate bunion deformity. A Chevron osteotomy was performed and after 6 weeks the patient was doing reasonably well. Six months later she reports increasing pain and stiffness in her toe. Clinically the toe is reasonably straight, but she has significant calluses and overload under the second and third metatarsals. A follow-up radiograph is shown in Figure 11b. The patient wants to be free of pain. What is the most appropriate treatment?

Varus malunion following talar neck fracture is best corrected by:
A tailorâs bunion is an abnormal prominence of the lateral aspect of the 5th metatarsal head. Similar to hallux valgus deformities, tailorâs bunions can be due to a widened intermetatarsal angle between the 4th and 5th metatarsal shafts. The normal 4-5 intermetatarsal angle is:
Which of the following resist articular cartilage compression and fluid flow:
of 100
Figures 1 and 2 are the MR images of a 5-year-old who has had progressive right knee pain and swelling, fevers to 38.4°C, and refusal to bear weight for the past several days. Laboratory evaluation reveals hematocrit 29.9, WBC count 17.5 with 92% neutrophil on differential count, ESR 48, and CRP level of 8.2. What is the most appropriate course of action?

Figures 1 and 2 are the MR images of a 5-year-old who has had progressive right knee pain and swelling, fevers to 38.4°C, and refusal to bear weight for the past several days. Laboratory evaluation reveals hematocrit 29.9, WBC count 17.5 with 92% neutrophil on differential count, ESR 48, and CRP level of 8.2. What is the most appropriate course of action?
of 100
Figures 25a through 25c are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?



Figures 25a through 25c are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
During fracture repair systemiCas well as local factors come into play. Which of the following is considered a systemiCfactor in fracture healing:
Which of the following factors is associated with a decrease in the accuracy of measurement of congenital scoliosis:
of 100
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain?
22A B

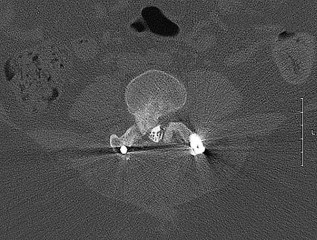
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain?
22A B
An active 38-year-old male carpenter reports activity-related medial knee pain. Arthroscopy performed 3 years ago revealed a torn medial meniscus that was debrided and mild condylar changes of the medial femoral condyle and medial tibial plateau. Current standing radiographs reveal Ahlback stage II changes with mild medial femoral joint space narrowing and a 5-degree varus deformity. What is the best treatment option?
Time to soft-tissue coverage was not shown to have a statistically significant difference on the rate of infection in the level II study by Pollak et. al
A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?

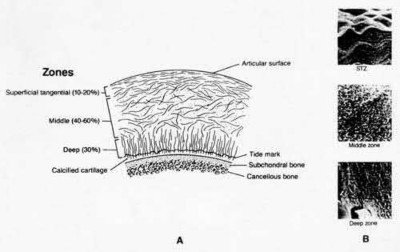







































A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?
Which of the following are characteristic of osteoarthritis:
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
**Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?









SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
**Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?
The net effect of 1,25 dihydroxyvitamin D3 on the calcium and phosphate concentration of the extracellular fluid and serum is:
Figures 60a and 60b show the radiographs of the ankle and distal leg of an 1-
2. year-old girl after she twisted her ankle while playing soccer. She has no
3. history of ankle or leg pain. Examination reveals localized swelling and
4. tenderness over the lateral ankle, and the tibia is not tender. The bone lesion
5. identified in the tibia most likely is
6. 1- osteoblastoma.
7. 2- osteoid osteoma.
8. 3- ossifying fibroma.
9. 4- fibrous dysplasia.
10. 5- nonossifying fibroma.
2. year-old girl after she twisted her ankle while playing soccer. She has no
3. history of ankle or leg pain. Examination reveals localized swelling and
4. tenderness over the lateral ankle, and the tibia is not tender. The bone lesion
5. identified in the tibia most likely is
6. 1- osteoblastoma.
7. 2- osteoid osteoma.
8. 3- ossifying fibroma.
9. 4- fibrous dysplasia.
10. 5- nonossifying fibroma.
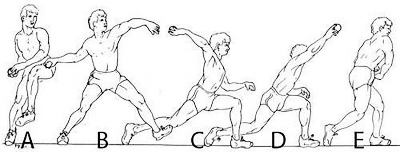
A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. Which phase of the throwing cycle shown in Figure 1 will most likely reproduce his symptoms?
---
---
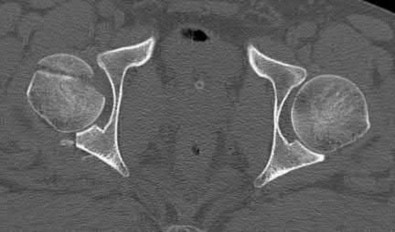
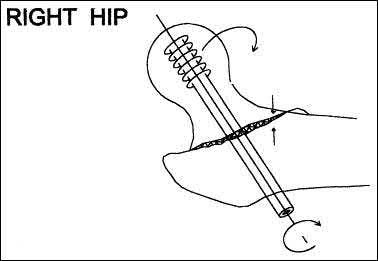
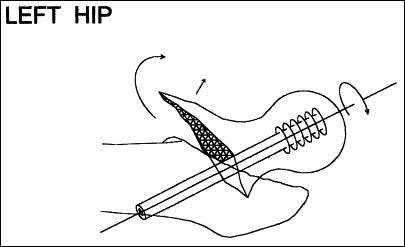
A 10-year-old boy hit a tree with his sled and is seen in the emergency department with extreme left hip pain and inability to ambulate. He has no history of pain in the left groin, thigh, or knee. Radiographs are seen in Figures 29a and 29b. What is the most common complication resulting from this injury?
of 100
Figure 68 is the MR image of an 85-year-old patient who cannot ambulate unless leaning over things. While sitting, the patient has minimal pain. Which structure is the arrow pointing to?
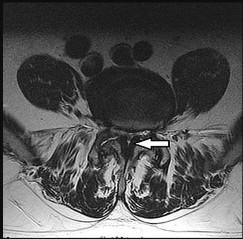



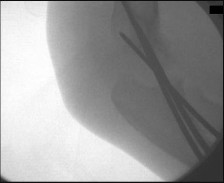
Figure 68 is the MR image of an 85-year-old patient who cannot ambulate unless leaning over things. While sitting, the patient has minimal pain. Which structure is the arrow pointing to?
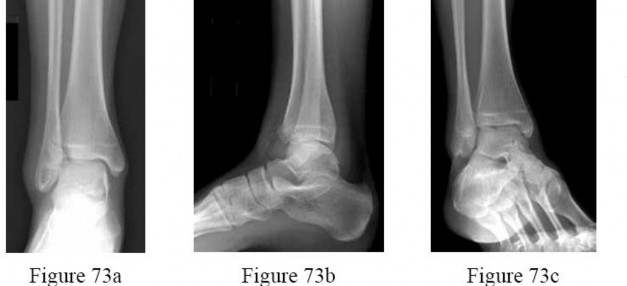
Figures 73a through 73c are the radiographs of a 14-year-old girl who sustained an ankle injury in a fall.What ligament is attached to the displaced fragment?
---
---
of 100 A 50-year-old pipefitter falls from a ladder at work and dislocates his non-dominant shoulder. His MRI scan shows supraspinatus and infraspinatus tears with retraction to the glenoid. He cannot actively raise his arm away from his side. He denies prior shoulder symptoms before his fall. Three weeks of physical therapy have failed to improve his function. Which factor has been demonstrated to result in a poor clinical outcome following surgical intervention?
Patients treated with zoledronic acid within 90 days of a hip fracture, followed up with annual treatment, will most likely show:
Initial treatment for De Quervain disease involves:
of 100
Figure 1 is the radiograph of a 6-year-old boy who falls off a tire swing and sustains an isolated left femur fracture that is treated with submuscular plating (Figure 2). He went on to uneventful union and full return to activity without disability. Recommendations should include

Figure 1 is the radiograph of a 6-year-old boy who falls off a tire swing and sustains an isolated left femur fracture that is treated with submuscular plating (Figure 2). He went on to uneventful union and full return to activity without disability. Recommendations should include
A patient presents for treatment of a painful hallux. The pain is over the dorsal surface of the hallux metatarsophalangeal joint and is worsened with plantar flexion of the toe. The passive range of motion is 30° of dorsiflexion and 10° of plantarflexion. The radiographs confirm the presence of mild arthritis of the metatarsophalangeal joint, with dorsal osteophytes on the metatarsal head. Which of the following procedures is most likely to be associated with a long-term satisfactory outcome:
Which of the following defects occurs in Albright hereditary osteodystrophy (pseudohypoparathyroidism):
Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
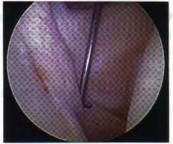
Figure 56 shows an arthroscopic view of the long head of the biceps; it has an incompetent biceps sling and is unstable, and an axial glenohumeral MRI scan reveals that it is dislocated medially out of the intertubercular groove. What structure is also most likely injured?





DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.
Figure 56
Figure 56 shows an arthroscopic view of the long head of the biceps; it has an incompetent biceps sling and is unstable, and an axial glenohumeral MRI scan reveals that it is dislocated medially out of the intertubercular groove. What structure is also most likely injured?
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Which of the following describes the inheritance pattern of hypophosphatasia:
A 10-year-old boy hit a tree with his sled and is seen in the emergency department with extreme left hip pain and inability to ambulate. He has no history of pain in the left groin, thigh, or knee. Radiographs are seen in Figures 29a and 29b. What is the most common complication resulting from this injury?
Androgens prevent bone resorption. Receptors for androgens are found on which of the following cells:
A patient underwent a right hip arthroscopy, CAM resection, and labral repair while positioned supine on a fracture table with a perineal post. The leg was in traction for 4 hours, and no intrasurgical complications were noted. At the 2‐week follow‐up appointment, the patient was experiencing numbness and tingling in the perineum on the surgical side and noted pain predominantly while sitting. What is the likely cause of these symptoms?
25
25
of 100
What is the zone of injury?
What is the zone of injury?
..A 21-year-old college swimmer presents with an inability to compete for longer than 1 year because of right shoulder pain and subjective symptoms of instability despite physical therapy. Recent radiographs and an MRI scan of her shoulder demonstrate an intact labral complex. Her symptoms are reproduced with sulcus testing and load and shift maneuvers in both anterior and posterior directions. What is the most appropriate next treatment step?
The daily elemental calcium requirement for a pregnant woman is:
Which of the following fractures occurs through a single application of force:
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
of 100
Which treatment of the current fracture will provide the best long-term outcome?




Which treatment of the current fracture will provide the best long-term outcome?
The optimal position for hallux interphalangeal joint arthrodesis is:
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
A 9-year-old boy is examined due to a closed distal forearm fracture. The radius and ulna are both fractured and translated
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The least invasive treatment which would produce acceptable results is:
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The least invasive treatment which would produce acceptable results is:
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Figures 23a and 23b show
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
2. radiographs of a 52-year-old man
3. with diabetes who has had purulent
4. drainage from the medial side of his
5. right great toe for 3 weeks. He was
6. recently started on insulin.
7. Examination reveals a good dorsalis
8. pedis pulse but poor sensation from
9. the malleoli to the toes. Treatment
10. should consist of
11. 1- amputation of the great toe.
12. 2- bone culture and 6 weeks of IV
13. antibiotics.
14. 3- joint aspiration and 2 weeks of IV
15. antibiotics.
16. 4- excision interphalangeal arthroplasty.
17. 5- excision of infected bone and
18. interphalangeal joint arthrodesis.
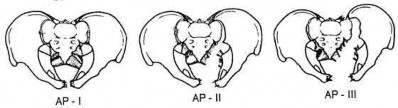
-Pelvic packing for a hemodynamically unstable patient with a pelvic ring fracture is best described by which of the following techniques?
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
The most common risk factors for stress fractures is:
A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
of 100
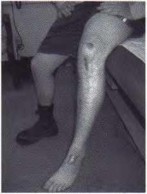
Figure 1 is the clinical photograph of an 11-year-old otherwise healthy boy who presents to the emergency department following 3 days of progressive left lateral ankle pain, difficulty bearing weight, swelling, and fever. He has a temperature of 102°F and other vitals are normal. He denies other areas of pain. He tolerates gentle ankle motion, and has exquisite point tenderness overlying the region of the distal fibular metaphysis. Radiographs of the ankle are normal. CRP is 32 mg/dL, ESR is 17, WBC count is 10.4. An MRI (Figure

Figure 1 is the clinical photograph of an 11-year-old otherwise healthy boy who presents to the emergency department following 3 days of progressive left lateral ankle pain, difficulty bearing weight, swelling, and fever. He has a temperature of 102°F and other vitals are normal. He denies other areas of pain. He tolerates gentle ankle motion, and has exquisite point tenderness overlying the region of the distal fibular metaphysis. Radiographs of the ankle are normal. CRP is 32 mg/dL, ESR is 17, WBC count is 10.4. An MRI (Figure
of 100
Figures 1 and 2 are the radiographs of a 5-year-old boy who was treated for a nondisplaced ulna fracture. Eight months later, he complains of a painful prominence over the elbow, causing pain with direct trauma during activity, occurring for several months. What is the best next step in the management of this patient?

Figures 1 and 2 are the radiographs of a 5-year-old boy who was treated for a nondisplaced ulna fracture. Eight months later, he complains of a painful prominence over the elbow, causing pain with direct trauma during activity, occurring for several months. What is the best next step in the management of this patient?
Human calcium absorption occurs in the
Which of the following features is associated with type 2 osteoporosis:
A 63-year-old man has long-standing type 2 diabetes. He has had associated ongoing neuropathy for approximately 5 years. He now reports a red, hot, swollen right foot for the past 2 days. You place him supine in your office with the foot elevated for 30 minutes. You return to see that the redness has dissipated. What is the most likely diagnosis?
A 14-year-old boy sustains an intercondylar fracture of the distal humerus. There is a single fracture line into the joint between the capitellum and the trochlea. The medial column of the distal humerus is comminuted, but the lateral column is not. All fragments are highly displaced. Neurovascular status is normal. The recommended treatment is:
C ardinal signs of evenomation include all of the following except:
of 100
Figures 67a and 67b are the radiographs of a 58-year-old man who has a painful left shoulder. Three months ago he underwent an anatomic total shoulder arthroplasty (TSA) for glenohumeral osteoarthritis. He was doing some yardwork when he felt a pop in his shoulder. What is the most likely diagnosis?


Figures 67a and 67b are the radiographs of a 58-year-old man who has a painful left shoulder. Three months ago he underwent an anatomic total shoulder arthroplasty (TSA) for glenohumeral osteoarthritis. He was doing some yardwork when he felt a pop in his shoulder. What is the most likely diagnosis?
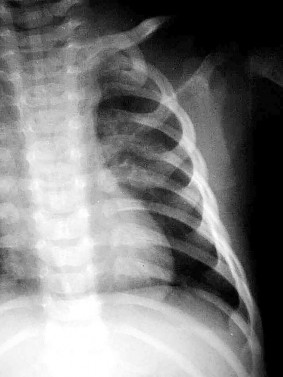
An 18-month-old boy is brought to your office for a clawing deformity of his right hand. The parents inform you that he was born full term after a difficult delivery complicated by shoulder dystocia. The boy weighed 9½ lbs at birth. The child had a brief episode of apnea with an APGAR score of 5 at birth and needed resuscitation and admission to the natal intensive care unit. Parents recall having noted a bump on his right clavicle, which was tender and was diagnosed as clavicle fracture. They also noticed a week later that the child did not flex the fingers of his right hand. The neonatologist had informed them that the
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
A 22-year-old male soccer player reports left hip and groin pain. He states that symptoms began before a preseason tournament but have worsened steadily for the past 2 weeks. He denies any recent fever or sickness and is otherwise healthy. Examination reveals tenderness over the symphysis pubis and pain with resisted rectus abdominus testing. Radiographs are negative. What is the next step in the proper management of this patient?
Figures 1 and 2 are the T2-weighted MR images of a 54-year-old woman with medial knee pain and catching of 6 months’ duration. Which treatment option is most likely to be associated with a favorable outcome?

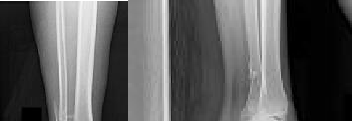
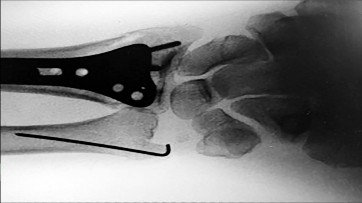
Figures 7a and 7b show the wound and radiograph
2. of a 44-year-old man who underwent plating for a
3. closed fracture of his tibia 7 months ago. The
4. wound has been draining for 4 months, and cultures
5. are positive for Staphylococcus aureus. In addition
6. to antibiotics, metal removal, and debridement,
7. treatment should include
8. 1- electrical stimulation and casting.
9. 2- soft-tissue coverage and replating with a bone graft.
10. 3- bone grafting, soft-tissue coverage, and application
11. of a cast.
12. 4- external fixation, staged soft-tissue coverage, and
13. bone grafting.
14. 5- intramedullary rodding, staged soft-tissue coverage,
15. and bone grafting.
2. of a 44-year-old man who underwent plating for a
3. closed fracture of his tibia 7 months ago. The
4. wound has been draining for 4 months, and cultures
5. are positive for Staphylococcus aureus. In addition
6. to antibiotics, metal removal, and debridement,
7. treatment should include
8. 1- electrical stimulation and casting.
9. 2- soft-tissue coverage and replating with a bone graft.
10. 3- bone grafting, soft-tissue coverage, and application
11. of a cast.
12. 4- external fixation, staged soft-tissue coverage, and
13. bone grafting.
14. 5- intramedullary rodding, staged soft-tissue coverage,
15. and bone grafting.
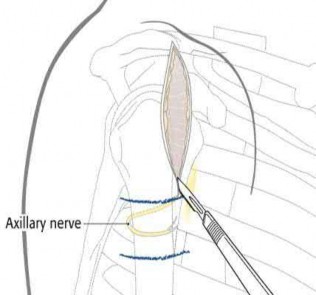
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the
time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Recurrence of osteochondroma is likely if:
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation?
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has
deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Scoliosis in Marfan syndrome, as compared to idiopathic scoliosis, is characterized by which of the following:
An 88-year-old nursing home resident is seen in the emergency department after a fall. At the time of admission, physical examination of the affected extremity reveals absent pulses and inadequate capillary refill. A radiograph is seen in Figure 48. Appropriate management includes which of the following?
A 46-year-old woman sustains an extra-articular fracture of the distal radius and undergoes open reduction and internal fixation with a volar plate and screw construct. During postoperative recovery from this injury, what benefit does formal physical therapy have as compared to a patient-guided home exercise program?
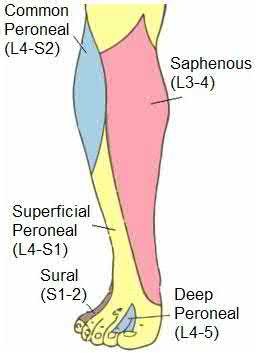
Which of the following leg muscles often has its own fascial envelope (separate compartment):
of 100
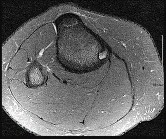
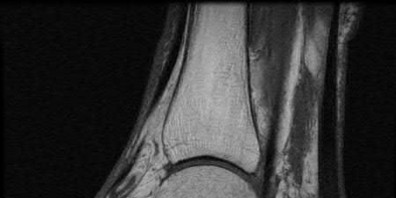
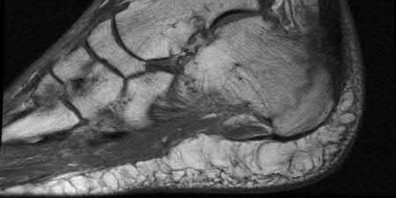
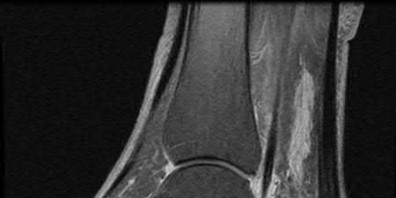
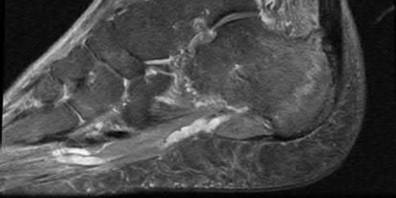
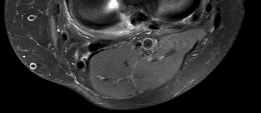
Figures 74a and 74b are the MR images of a 36-year-old man with a 3-month history of excruciating left leg pain. Which finding upon examination would be most consistent with the MR images?


Figures 74a and 74b are the MR images of a 36-year-old man with a 3-month history of excruciating left leg pain. Which finding upon examination would be most consistent with the MR images?
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
-is the initial lateral radiograph of the foot of a 55-year-old woman who felt a pop in her left foot as she stepped off the curb. She subsequently had severe heel pain and could not bear weight.Examination in the emergency department revealed a bony prominence over the posterior aspect of the heel with blanching of the surrounding skin. What is the most appropriate orthopaedic management?

A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Organisms survive on biosynthetiCsurfaces, such as total hips, because of:
2010 Pediatric Orthopaedic Examination Answer Book *15
Achondroplasia is caused by an abnormality of which of the following?
Achondroplasia is caused by an abnormality of which of the following?
