Score: 0%
100 Random Orthopedic MCQs for Board Prep (2026 Update)
QUESTION 1
Which of the following cells produce osteocalcin and bone sialoprotein:
1
Osteocytes
2
Osteoblasts
3
Mast cells
4
Osteoclasts
5
Fibroblasts
Osteoblasts are metabolically active cells that line the bone surface. Osteoblasts produce type I collagen and many
noncollagenous proteins such as osteocalcin, bone sialoprotein, and extracellular matrix proteins. Osteoblasts have large amounts of rough endoplasmiCreticulum because they prepare large amounts of protein for export out of the cell. The Golgi apparatus exports the protein.
noncollagenous proteins such as osteocalcin, bone sialoprotein, and extracellular matrix proteins. Osteoblasts have large amounts of rough endoplasmiCreticulum because they prepare large amounts of protein for export out of the cell. The Golgi apparatus exports the protein.
QUESTION 2
In an obese patient undergoing unicondylar knee arthroplasty (UKA):
1
The results are worse than in a normal weight patient.
2
The results are better than in a normal weight patient.
3
The results are not predictably better or worse.
4
The results depend on the design of the prosthesis.
5
Results are gender dependent.
The knee should have less than 15° of deformity in varus or valgus and less than 10° flexion contracture. Inflammatory or crystalline-induced arthritis, knee subluxation, gross ligamentous laxity, and obesity are relative contraindications to the procedure. Scott and colleagues found that increased body weight contributed to failure in UKA and suggested that the best candidates are less than 180 lb
QUESTION 3
Which of the following defects occurs in Albright hereditary osteodystrophy (pseudohypoparathyroidism):
1
Type X collagen
2
Sulfate transporter gene
3
Beta glucosidase
4
Galpha S (GNAS1)
5
C arbonic anhydrase type II, proton pump
Pseudohypoparathyroidism (PHP) (Albright Hereditary Osteodystrophy [AHO]) - end organ insensitivity; in AHO, germline mutation that leads to loss of function of Galpha S (GNAS1); causes end-organ resistance to PTH (Zaleske).
1/. PHP - short stature, short metacarpals (4th and 5th), rounded facies a. Mental retardation, tetany
b. Sex-linked dominant
2/. Laboratory features a. Hypocalcemia
b. Hyperphopshatemia c. Normal PTH
3/. Other features
The other responses refer to:
Metaphyseal chondrodysplasia (Schmid type): Type X collagen
Diastrophic dysplasia: Sulfate transporter gene
Gaucher's disease: Beta glucosidase
Osteopetrosis: C arbonic anhydrase type II, proton pump
1/. PHP - short stature, short metacarpals (4th and 5th), rounded facies a. Mental retardation, tetany
b. Sex-linked dominant
2/. Laboratory features a. Hypocalcemia
b. Hyperphopshatemia c. Normal PTH
3/. Other features
The other responses refer to:
Metaphyseal chondrodysplasia (Schmid type): Type X collagen
Diastrophic dysplasia: Sulfate transporter gene
Gaucher's disease: Beta glucosidase
Osteopetrosis: C arbonic anhydrase type II, proton pump
QUESTION 4
Internal impingement is characterized by which of the following anatomic lesions?

1
Subscapularis tear
2
Bursal-sided rotator cuff tear
3
Articular-sided rotator cuff tear
4
Tight anterior capsule
5
Laxity of the posterior capsule
DISCUSSION: Internal impingement is characterized by articular-sided partial-thickness rotator cuff tears and superior glenoid labral tears. The capsule is characterized by laxity anteriorly and tightness posteriorly.
Scientific References
- : Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 82.
Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I:
Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Figure 27
QUESTION 5
Slide 1 Slide 2
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
1
FGF receptor 3
2
Type I collagen
3
Cartilage oligomeriCmatrix protein
4
Fibrillin
5
Type II collagen
The anteroposterior and lateral radiographs show thinned cortices and a gentle S-shaped curve of the tibia. The overall alignment of the tibia, as well as the physes, is normal. These are the radiographiCfeatures of osteogenesis imperfecta.
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
QUESTION 6
of 100
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?


A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
1
Medical management with intravenous (IV) antibiotics and observation
2
CT-guided aspiration of the abscess before initiating antibiotics
3
Surgical decompression and IV antibiotics
4
Blood cultures and re-evaluation in 24 hours
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
QUESTION 7
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that
has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is provided with a medial unloader brace that provides substantial pain relief, and he is able to work while wearing the brace. After 4 months, he returns to work and reports that while the brace enables him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace, and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is provided with a medial unloader brace that provides substantial pain relief, and he is able to work while wearing the brace. After 4 months, he returns to work and reports that while the brace enables him to work, it is uncomfortable. Consequently, his symptoms return when he is not wearing the brace, and he is requesting a surgical intervention for his problem. What is the most appropriate surgical treatment?
1
Valgus-producing high tibial osteotomy (VPHTO)
2
Repeat knee arthroscopy
3
Total knee arthroplasty (TKA)
4
Medial meniscus transplant
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO but does not influence technique.
QUESTION 8
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?**
1
Shoulder arthrography
2
MRI of the cervical spine
3
CT of the head
4
Technetium Tc 99m bone scan
5
Electromyography and nerve conduction velocity studies
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch.
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
QUESTION 9
of 100
Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).


Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with 2 weeks of pain at the left distal femur, a limp, and an inability to dance. Knee motion is 0 to 135 degrees with minimal pain and there is no effusion. Her temperature is 37.0°C, WBC is 12000 /µL (rr, 4500-11000 /µL), CRP is 0.8 mg/L (rr, 0.08-3.1 mg/L), and ESR is 21 mm/h (rr, 0-20 mm/h).
1
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
2
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
3
Aspiration, cultures, Lyme serology, and oral amoxicillin
4
Biopsy, culture, curettage, bone graft, and possible internal fixation
5
Physical therapy, ibuprofen, and an antinuclear antibody test
Figures 14a through 14e show a 13-year-old boy with osteomyelitis of the distal tibia and a large subperiosteal abscess. The patient has failed treatment with IV ceftriaxone, and methicillin-resistant Staphylococcus aureus infection is likely. Aspiration, cultures, irrigation and debridement, IV vancomycin, an infectious disease consult, and an evaluation for possible deep vein thrombosis is prudent initial treatment. Figure 15a through 15c show a 7-year-old girl who sustained a deer tick bite while vacationing in Connecticut. She has Lyme arthritis and a Lyme “bulls-eye” rash on the same leg. Aspiration, cultures, Lyme serology, and oral amoxicillin for 30 days is prudent initial treatment. Figures 16a and 16b are the radiograph and MR image of a 15-year-old dance athlete with a probable minor fracture via a benign cyst of the distal femur. The geographic cyst may be a nonossifying fibroma, eosinophilic granuloma, Brodie abscess, or simple bone cyst. Biopsy, culture, curettage and bone graft, and possible internal fixation is reasonable initial treatment.
Figure 17
Figure 17
QUESTION 10
aOne year after undergoing a primary total knee arthroplasty, a 65-year-old man has a 1-week history of new onset anterior knee pain. He can perform a straight-leg raise with no extension lag. Radiographs reveal a transverse patella fracture with 8 mm of displacement and an intact patellar component. The best course of treatment is
1
patellectomy with retinacular repair.
2
immobilization in extension for 6 weeks.
3
open reduction and cerclage wiring.
4
internal fixation and patellar component revision.
This patient has a displaced periprosthetic patella fracture with an intact extensor mechanism. Surgical treatment for this condition has been associated with relatively poor clinical results because the fracture occurs late (attributable to patella osteonecrosis). The optimal initial treatment is to treat the fracture nonsurgically with immobilization of the knee in extension either with a long-leg cast or knee immobilizer.
18
18
QUESTION 11
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
1
No superior translation during abduction
2
Retention of ball-and-socket kinematics with more than 30 degrees of abduction
3
Loss of ball-and-socket kinematics with less than 30 degrees of abduction
4
Superior translation of the humeral head with more than 30 degrees of abduction
5
Superior translation of the humeral head with external rotation
Normal glenohumeral kinematics are represented by ball-and-socket modeling when the rotator cuff is intact. This is true for motion that involves more than 30 degrees of abduction. In patients with shoulder pain and symptomatic rotator cuff tears, superior translation occurs with abduction beyond 30 degrees. This is quite evident in massive tears but is seen consistently to a lesser degree with smaller tears.
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
QUESTION 12
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?
1
Angiography
2
Immediate closed reduction and casting in extension
3
Surgical exploration and repair of the artery, followed by skeletal stabilization
4
Closed reduction and pinning, followed by reassessment of the vascular status
5
Magnetic resonance angiography (MRA)
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed.
REFERENCES: Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
REFERENCES: Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
QUESTION 13
of 100
Figures 1 through 4 are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?

Figures 1 through 4 are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?
1
Compartment syndrome
2
Loss of elbow motion
3
Avascular necrosis (AVN) of the radial head
4
Nonunion of the fracture site
■
This girl sustained a fracture dislocation of the elbow with a severely displaced and rotated radial neck fracture. Required treatment was open reduction and internal fixation (ORIF). Less severely displaced radial neck fractures can be treated with closed reduction, percutaneous pinning, or flexible nail manipulation. In this scenario, interposed capsular tissue and rotation of the radial head were indications for ORIF. ORIF is associated with a higher risk for poor outcomes. Complications following ORIF of radial neck fractures in children include posterior interosseous neuropraxia, valgus angulation, premature closure of the radial head physis, AVN of the radial head, nonunion, and elbow stiffness. Stiffness is most common. Compartment syndrome, infection, and anterior interosseous nerve palsy are less common complications.
QUESTION 14
Which of the following most accurately approximates the estimated risk of a musculoskeletal allograft containing the human immunodeficiency virus (HIV) despite adequate screening?
1
1 in
600
2
1 in
6,000
3
1 in
60,000
4
1 in
1,600,000
5
1 in
6,000,000
DISCUSSION: The calculated risk of a musculoskeletal allograft containing HIV despite adequate screening has been estimated to be approximately 1 in 1.6 million. This estimate is based on the risk of HIV in the population, projected population estimates, and current methods of donor screening.
REFERENCES: McAllister D, Joyce M, Mann B, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;2148-2158.
Buck B, Malinin T: Human bone and tissue allografts: Preparation and safety. Clin Orthop Relat Res 1994;303:8 -
17.
Buck B, Malinin T, Brown M: Bone transplantation and human immunodeficiency virus: An estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin Orthop Relat Res 1989;240:129-136.
_A i;___
Figure 92
QUESTION 15
When an anterior approach to the cervical spine is being performed, many
2. surgeons prefer the left-sided approach to the right-sided approach because on
3. the left side the recurrent laryngeal nerve is
4. 1- larger.
5. 2- more consistent in location.
6. 3- entirely within the carotid sheath.
7. 4- well protected by the strap muscles of the neck.
8. 5- located between the longus colli and the esophagus.
2. surgeons prefer the left-sided approach to the right-sided approach because on
3. the left side the recurrent laryngeal nerve is
4. 1- larger.
5. 2- more consistent in location.
6. 3- entirely within the carotid sheath.
7. 4- well protected by the strap muscles of the neck.
8. 5- located between the longus colli and the esophagus.
1
surgeons prefer the left-sided approach to the right-sided approach because on
2
the left side the recurrent laryngeal nerve is
3
1- larger.
4
2- more consistent in location.
5
3- entirely within the carotid sheath.
1.
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, pp 265-269.
#
1. [next question](content://com.estrongs.files/storage/emulated/0/Download/OITE%201997.html#-1,-1,NEXT)
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, pp 265-269.
#
QUESTION 16
Delayed unions and nonunions of base of fifth metatarsal fractures have been demonstrated to heal by:
1
Prolonged cast immobilization and non-weight bearing
2
Pulsed electromagnetic fields
3
C ontinued use of a fracture boot with protected weight-bearing
4
Injection of demineralized bone matrix
5
Rigid carbon fiber shoe inserts
Nine delayed unions and nonunions of the proximal fifth metatarsal were treated with pulsed electromagnetic fields. All fractures healed in a mean of 4 months (follow-up 39 months, no refractures).
QUESTION 17
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The _A_ A _L-M_ P _a_ r _d_ a _e_ d _n_ i _a_ o _C_ g _o_ r _p_ a _y_ ph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage?
1
Hip arthroscopy and labral debridement
2
Femoroacetabular osteoplasty and labral repair
3
Femoral osteotomy
4
Hemiarthroplasty
5
Total hip arthroplasty
The patient has femoroacetabular impingement. The prominence on the femoral neck has
resulted in a labral tear and detachment. An MR-arthrogram is the most appropriate modality for diagnosis of a labral tear. The diagnosis of a labral tear per se is not an indication for surgical intervention because the natural incidence of this condition is not known. Labral debridement without addressing the underlying anatomic abnormality is likely to result in a suboptimal outcome. The most appropriate treatment, when indicated, is shaving down of the femoral neck to remove the bony prominence and attachment of the labrum. Femoral osteotomy has no role in the treatment of this condition. The patient has minimal arthritis; therefore, arthroplasty is not indicated.
REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003;417:112-120.
Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
resulted in a labral tear and detachment. An MR-arthrogram is the most appropriate modality for diagnosis of a labral tear. The diagnosis of a labral tear per se is not an indication for surgical intervention because the natural incidence of this condition is not known. Labral debridement without addressing the underlying anatomic abnormality is likely to result in a suboptimal outcome. The most appropriate treatment, when indicated, is shaving down of the femoral neck to remove the bony prominence and attachment of the labrum. Femoral osteotomy has no role in the treatment of this condition. The patient has minimal arthritis; therefore, arthroplasty is not indicated.
REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003;417:112-120.
Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
QUESTION 18
of 100
If the culture results are positive, which treatment will most likely resolve the infection?
If the culture results are positive, which treatment will most likely resolve the infection?
1
Arthroscopic debridement
2
Intravenous antibiotics
3
Single-stage revision
4
Double-stage revision
Osteolysis of this magnitude is uncommon in the setting of an uncemented hemiarthroplasty. Further workup for infection is indicated, such as aspiration under fluoroscopy or ultrasound. Infection needs to be ruled out before proceeding. Observation and physical therapy are not indicated. Arthroscopy has been shown in several studies to have greater sensitivity and specificity than aspiration and can be especially effective to obtain cultures of slow-growing organisms such as Propionibacterium acnes. Blood tests are unreliable, and a bone scan would not reliably differentiate between loosening and infection. Arthroscopic debridement would not be reliable for treatment. Intravenous antibiotics can be used for suppression, but the best results in terms of resolving the infection would be achieved with 2-stage revision.
RECOMMENDED READINGS
31. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
32. Hersch JC, Dines DM. Arthroscopy for failed shoulder arthroplasty. Arthroscopy. 2000 Sep;16(6):606-
[12/. PubMed PMID: 10976121. ](http://www.ncbi.nlm.nih.gov/pubmed/10976121)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976121)
33. [Foruria AM, Fox TJ, Sperling JW, Cofield RH. Clinical meaning of unexpected positive cultures (UPC) in revision shoulder arthroplasty. J Shoulder Elbow Surg. 2013 May;22(5):620-7. doi: 10.1016/j.jse.2012.07.017. Epub 2012 Sep 13. PubMed PMID: 22981448. ](http://www.ncbi.nlm.nih.gov/pubmed/22981448)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22981448)
RECOMMENDED READINGS
31. [Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 3;96(23):1952-8. doi: 10.2106/JBJS.M.01512. PubMed PMID: 25471909. ](http://www.ncbi.nlm.nih.gov/pubmed/25471909)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25471909)
32. Hersch JC, Dines DM. Arthroscopy for failed shoulder arthroplasty. Arthroscopy. 2000 Sep;16(6):606-
[12/. PubMed PMID: 10976121. ](http://www.ncbi.nlm.nih.gov/pubmed/10976121)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10976121)
33. [Foruria AM, Fox TJ, Sperling JW, Cofield RH. Clinical meaning of unexpected positive cultures (UPC) in revision shoulder arthroplasty. J Shoulder Elbow Surg. 2013 May;22(5):620-7. doi: 10.1016/j.jse.2012.07.017. Epub 2012 Sep 13. PubMed PMID: 22981448. ](http://www.ncbi.nlm.nih.gov/pubmed/22981448)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22981448)
QUESTION 19
The distinction between a Lauge-Hansen supination-external rotation III injury and a Lauge-Hansen supination-external rotation
IV injury is:
IV injury is:
1
A spiral oblique fracture of the lateral malleolus
2
Anteroinferior tibiofibular ligament (AITFL) disruption
3
Posteroinferior tibiofibular ligament (PITFL) disruption or posterior malleolus fracture
4
Deltoid ligament disruption or medial malleolus fracture
5
Anterior talo-fibular ligament disruption
The sequence of injury according to the Lauge-Hansen classification system in supination-external rotation injuries is AITFL disruption, spiral oblique fracture of the lateral malleolus, PITFL disruption or posterior malleolus fracture, and finally stage IV, which is a deltoid ligament disruption or medial malleolus fracture.
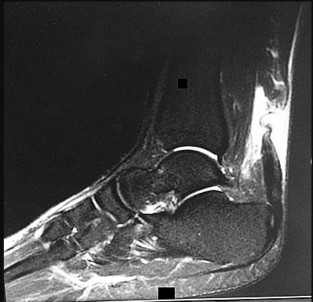
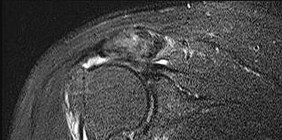
QUESTION 20
A 36-year-old recreational athlete feels a pop in his antecubital fossa while lifting weights. He has pain, swelling, and deformity. Representative sagittal and coronal MRI slices are shown in Figures 1 and 2, respectively. What is the most common major complications associated with surgical repair of this structure?
74
74
1
Symptomatic heterotopic ossification requiring reoperation
2
Brachial artery laceration
3
Deep infection
4
Posterior interosseous nerve palsy
The MRI scan shows a distal biceps tendon rupture with retraction. Tendon rerupture and PIN palsy are the two most common major complications following distal biceps repair surgery. Major complication rates are not found to differ by sex, history of tobacco use, age, exposure type (single versus two
incisions), tear morphology (full versus partial), or type of fixation used.
incisions), tear morphology (full versus partial), or type of fixation used.
QUESTION 21
Which of the following is the rate-limiting step in the production of biologically active Vitamin D:
1
25 hydroxylation in the liver
2
Absorption of calcium in the duodenum
3
Conversion of 7 dehydrocholesterol to vitamin D3 in the skin
4
1 hydroxylation in the kidney
5
Absorption of calcium in the jejunum
The addition of a second hydroxyl group at the 1 position to 25 hydroxy vitamin D3 is the rate-limiting step in the formation of the active from of vitamin D3. Impaired renal function is common in older individuals
QUESTION 22
You design a research study in which you ask patients who have a nonunion of the tibia to fill out a questionnaire in which they report on a variety of medical conditions and social/behavioral practices. You compare these findings to a similar group who did not develop a nonunion in order to identify medical and/or social conditions that might be risk factors for the development of tibial nonunions. This would be an example of what type of study?
1
Case series
2
Meta-analysis
3
Case control study
4
Retrospective cohort study
5
Prospective cohort study
#
A case control series starts with the occurrence of a specific disease or observation, and then compares data on those individuals to a similar group without the disease (control group) in order to identify potential risk factors for the development of the disorder. A case series is an observational study in which an investigator follows a series of patients who received a specific treatment, recording the results and outcomes of that treatment. A meta- analysis is the combination of several separate studies that look at similar hypotheses in an effort to create a larger patient population for analysis. A cohort study looks for the incidence of a specific outcome in two groups (cohorts) of patients who are similar with the exception of a particular
research variable (risk factor).
QUESTION 23
of 100
During an anterior approach to correct thoracolumbar scoliosis, there is a sudden decrease in somatosensory-evoked potential (SSEP) and motor-evoked potential (MEP) signals. Correction maneuvers have not been attempted when signals go down. All neuromonitoring and anesthesia concerns have been addressed, and the measured abnormalities persist. What is the likely reason behind the neuromonitoring abnormalities?
During an anterior approach to correct thoracolumbar scoliosis, there is a sudden decrease in somatosensory-evoked potential (SSEP) and motor-evoked potential (MEP) signals. Correction maneuvers have not been attempted when signals go down. All neuromonitoring and anesthesia concerns have been addressed, and the measured abnormalities persist. What is the likely reason behind the neuromonitoring abnormalities?
1
Occlusion of the artery of Adamkiewicz
2
Neurapraxia
3
Mechanical injury to the cord via instrumentation
4
False positive, proceed as planned
Change in SSEP and MEP should not be taken lightly during scoliosis surgery. A change in signal can occur because of anesthesia, patient, and surgical variables. If any changes occur in neuromonitoring signals, patient and anesthesia variables should be rechecked to ensure there is no cause of false-positive readings such as body temperature, low blood pressure, or malfunction of neuromonitoring leads.
The artery of Adamkiewicz originates in more than 90% of patients between T8 and L1. It has been postulated that the artery of Adamkiewicz is the primary blood supply to the thoracic spinal cord. Standard anterior retroperitoneal- and thoracotomy-based approaches typically necessitate sacrifice of segmental vessels that can disrupt blood supply to the anterior thoracic cord.
It is unlikely at this point in the surgery that neurapraxia caused this change because no correction maneuvers have been attempted and no instrumentation has been placed; however, these interventions can indeed trigger neuromonitoring issues during a procedure.
RECOMMENDED READINGS
11. [Fanous AA, Lipinski LJ, Krishna C, Roger EP, Siddiqui AH, Levy EI, Leonardo J, Pollina J. The Impact of Preoperative Angiographic Identification of the Artery of Adamkiewicz on Surgical Decision Making in Patients Undergoing Thoracolumbar Corpectomy. Spine (Phila Pa 1976). 2015 Aug 1;40(15):1194-9. PubMed PMID: 25816140.](http://www.ncbi.nlm.nih.gov/pubmed/25816140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25816140)
12. [Gonzalez AA, Jeyanandarajan D, Hansen C, Zada G, Hsieh PC. Intraoperative neurophysiological monitoring during spine surgery: a review. Neurosurg Focus. 2009 Oct;27(4):E6. doi: 10.3171/2009.8.FOCUS09150. Review. PubMed PMID: 19795955. ](http://www.ncbi.nlm.nih.gov/pubmed/19795955)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19795955)
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figure 20 is the MR image of a 27-year-old man who was playing basketball when he sustained the injury shown.
The artery of Adamkiewicz originates in more than 90% of patients between T8 and L1. It has been postulated that the artery of Adamkiewicz is the primary blood supply to the thoracic spinal cord. Standard anterior retroperitoneal- and thoracotomy-based approaches typically necessitate sacrifice of segmental vessels that can disrupt blood supply to the anterior thoracic cord.
It is unlikely at this point in the surgery that neurapraxia caused this change because no correction maneuvers have been attempted and no instrumentation has been placed; however, these interventions can indeed trigger neuromonitoring issues during a procedure.
RECOMMENDED READINGS
11. [Fanous AA, Lipinski LJ, Krishna C, Roger EP, Siddiqui AH, Levy EI, Leonardo J, Pollina J. The Impact of Preoperative Angiographic Identification of the Artery of Adamkiewicz on Surgical Decision Making in Patients Undergoing Thoracolumbar Corpectomy. Spine (Phila Pa 1976). 2015 Aug 1;40(15):1194-9. PubMed PMID: 25816140.](http://www.ncbi.nlm.nih.gov/pubmed/25816140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25816140)
12. [Gonzalez AA, Jeyanandarajan D, Hansen C, Zada G, Hsieh PC. Intraoperative neurophysiological monitoring during spine surgery: a review. Neurosurg Focus. 2009 Oct;27(4):E6. doi: 10.3171/2009.8.FOCUS09150. Review. PubMed PMID: 19795955. ](http://www.ncbi.nlm.nih.gov/pubmed/19795955)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19795955)
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figure 20 is the MR image of a 27-year-old man who was playing basketball when he sustained the injury shown.
QUESTION 24
Slide 1 Slide 2 Slide 3
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The genetic pattern seen in patients with this type of presentation is:
A 12-year-old boy is brought to the clinic by his concerned parents. The boyâs forearm is bowed, and his parents are confused as to the possible diagnosis and treatment options. You notice that the right forearm of the child is bowed ulnarwards and is shorter compared to the left forearm. The pronosupination is markedly decreased on the right side but is also limited on the left side. The patient has a good grip, pinch, and grasp. He is neurologically intact as well.
The parents say that they first noticed the deformity around 6 or 7 years ago, and the mother informs you that she had noticed a hard bump on the forearm. She has recently noticed another bump on his right leg. The child does not complain of pain and is using both of his hands quite well. The parents were informed by a previous physician that the child has Madelungâs deformity and are concerned that the disease is now involving other areas of his body.
You order a radiograph of the forearm. The anteroposterior radiograph is shown (Slide 1). The childâs skeletal radiograph survey is also presented (Slide 2 and Slide 3).
The genetic pattern seen in patients with this type of presentation is:
1
Autosomal recessive
2
Autosomal dominant
3
Sex-linked recessive
4
Sex-linked dominant
5
Sporadic
Multiple hereditary exostoses is inherited in an autosomal-dominant manner with 90% penetrance.
QUESTION 25
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
1
Anterior sternoclavicular joint dislocation
2
Posteroinferior sternoclavicular joint dislocation
3
Anterior acromioclavicular joint dislocation
4
Posterior acromioclavicular joint dislocation
5
Acromial fracture
Anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anterior or anterosuperior to the anterior margin of the sternum. In a study by Omer, 31% of athletic injuries have been known to cause a dislocation of the sternoclavicular joint. The serendipity view can show this dislocation, as will CT of the chest. This view requires the x-ray beam to be aimed at the manubrium with 40 degrees of cephalic tilt. An anterior sternoclavicular joint dislocation will appear superiorly displaced, while a posterior sternoclavicular joint dislocation is inferiorly displaced on the serendipity view.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
QUESTION 26
The risk of nerve injury following revision total hip arthroplasty (THA) is approximately:
1
0.5%
2
1%
3
1% to 10%
4
10% to 20%
5
More than 20%
Following primary THA, the incidence of nerve palsy is reported to be approximately 1.3%, but may be as high as 5.2% for primary THA performed for developmental dysplasia or dislocation. For revision surgery, the incidence may be as high as
7.60%
7.60%
QUESTION 27
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
1
Traumatic neuroma tethered by plantar neural branches
2
Regeneration of the transverse intermetatarsal ligament
3
Development of an intermetatarsal synovial cyst
4
Complex regional pain syndrome
5
Metatarsophalangeal joint synovitis
When a recurrent neuroma forms at the end of the resected nerve, it does not retract far enough because either the transection was not proximal enough or it is tethered by plantar neural branches. The transverse intermetatarsal ligament may reform, but it is not associated with pathology. Synovial cysts and synovitis are part of the differential diagnosis but are not associated with neuroma excision. Complex regional pain syndrome may result from neuroma excision, but this is rare and the symptoms are different.
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
QUESTION 28
A 35-year-old male with a pronation abduction ankle injury would have which of the following radiographs?





1
Figure A
2
Figure B
3
Figure C
4
Figure D
5
Figure E
Figure D shows a pronation abduction ankle fracture according to the Lauge-Hansen classification. This injury pattern is associated with a comminuted fibula fracture above the level of the syndesmosis and frequently has a concominant syndesmotic injury.
Lauge-Hansen's classic article describes in detail his proposed classification of ankle fractures based on both the position of the foot (supination or pronation) and an externally applied deforming force (adduction, abduction, external rotation). The Lauge-Hansen classification system is based on cadaveric experiments using manually applied forces and roentographs performed at each stage of injury.
Edwards and DeLee review their results in managing diastasis of the tibiofibular joint without an associated fracture. The authors propose a classification system of this uncommon injury and and theorize that the injury results from a pronation abduction mechanism.
Incorrect Answers:
Answer 1: Figure A represents a supination adduction fracture based on the vertical medial malleolar fracture, medial dislocation on the talus, and low transverse fibula fracture.
Answer 2: Figure B represents a pronation external rotation injury; note the high oblique fibula fracture and corresponding transverse medial malleolus fracture.
Answer 3: Figure C represents a supination external rotation ankle injury based on the oblique fibula fracture at the level of syndesmosis and the associated transverse medial malleolar fracture.
Answer 4: Figure E represents a pilon fracture based on the significant articular comminution signifiying an axial loading mechanism instead of a rotational injury.
Lauge-Hansen's classic article describes in detail his proposed classification of ankle fractures based on both the position of the foot (supination or pronation) and an externally applied deforming force (adduction, abduction, external rotation). The Lauge-Hansen classification system is based on cadaveric experiments using manually applied forces and roentographs performed at each stage of injury.
Edwards and DeLee review their results in managing diastasis of the tibiofibular joint without an associated fracture. The authors propose a classification system of this uncommon injury and and theorize that the injury results from a pronation abduction mechanism.
Incorrect Answers:
Answer 1: Figure A represents a supination adduction fracture based on the vertical medial malleolar fracture, medial dislocation on the talus, and low transverse fibula fracture.
Answer 2: Figure B represents a pronation external rotation injury; note the high oblique fibula fracture and corresponding transverse medial malleolus fracture.
Answer 3: Figure C represents a supination external rotation ankle injury based on the oblique fibula fracture at the level of syndesmosis and the associated transverse medial malleolar fracture.
Answer 4: Figure E represents a pilon fracture based on the significant articular comminution signifiying an axial loading mechanism instead of a rotational injury.
QUESTION 29
During gait evaluation of a 25-year-old patient who had polio at age 5, it is noted that the right foot slaps
the floor at heel strike, and the toes extend during the swing phase. Examination reveals a flexible cavus foot, claw toes, and an equinus deformity. The patient has tried various orthoses and would like surgical correction if possible. What is the most appropriate treatment?
the floor at heel strike, and the toes extend during the swing phase. Examination reveals a flexible cavus foot, claw toes, and an equinus deformity. The patient has tried various orthoses and would like surgical correction if possible. What is the most appropriate treatment?
1
Calcaneal osteotomy, Achilles tendon lengthening, metatarsal osteotomies
2
Calcaneal osteotomy, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
3
Calcaneal osteotomy, plantar fascia release, Achilles tendon lengthening, tibialis posterior transfer to the dorsum of the foot, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
4
Triple arthrodesis, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
5
Plantar fascia release, Achilles tendon lengthening, extensor hallucis longus transfer to the first metatarsal neck, tibialis posterior transfer to the dorsum of the foot, flexor digitorum longus to extensor digitorum longus transfer of the lesser toes
Weakness of the tibialis anterior can be noted with a tendency of the foot to slap the floor at heel strike. Extension of the toes during the swing phase of gait may be due to the toe extensors attempting to substitute for weakness of the tibialis anterior. Because this patient is young and has flexible deformities, avoiding arthrodesis is recommended and soft-tissue procedures are recommended to balance the foot. The plantar fascia release helps decrease the cavus. Transfer of the tibialis posterior tendon to the dorsum of the foot is necessary to provide dorsiflexion and limit the slapping of the foot on the floor.Transfer of the extensor hallucis longus to the metatarsal neck
addresses the claw toe deformity of the great toe and the flexor digitorum longus transfer provides additional dorsiflexion assist. Because the patient has a flexible deformity, osteotomies are unlikely to be needed.
addresses the claw toe deformity of the great toe and the flexor digitorum longus transfer provides additional dorsiflexion assist. Because the patient has a flexible deformity, osteotomies are unlikely to be needed.
QUESTION 30
of 100
A 58-year-old man has right shoulder pain. An examination reveals full range of motion in all planes but 4/5 forward elevation strength (Figures 90a and 90b).

A 58-year-old man has right shoulder pain. An examination reveals full range of motion in all planes but 4/5 forward elevation strength (Figures 90a and 90b).
1
Humeral head resurfacing/shoulder hemiarthroplasty
2
Anatomic total shoulder arthroplasty (TSA)
3
Reverse total shoulder arthroplasty (rTSA)
4
Rotator cuff repair
5
Open reduction and internal fixation (ORIF)
- Rotator cuff repair_
QUESTION 31
What is the most common cause of reoperation following contemporary hip resurfacing for degenerative coxarthrosis?
1
Limb-length discrepancy
2
Altered femoral offset
3
Snapping psoas tendon
4
Limitation of hip movement
5
Femoral neck fracture
DISCUSSION: Femoral neck fracture, necessitating revision surgery to a total hip arthroplasty, is the most likely common early complication after hip resurfacing. Cortical notching, varus positioning, and other technical variables appear to predispose to this complication. Limb lengths do not change appreciably after hip resurfacing; the same applies to femoral offset. Hip movement is not limited by hip resurfacing, and there is no evidence that psoas tendon impingement is increased by hip resurfacing.
REFERENCES: Steffen RT, Pandit HP, Palan J, et al: The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J Bone Joint Surg Br 2008;90:436-441.
Amstutz HC: Present state of metal-on-metal hybrid hip resurfacing. J Surg Orthop Adv 2008;17:12-16.
REFERENCES: Steffen RT, Pandit HP, Palan J, et al: The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J Bone Joint Surg Br 2008;90:436-441.
Amstutz HC: Present state of metal-on-metal hybrid hip resurfacing. J Surg Orthop Adv 2008;17:12-16.
QUESTION 32
Which of the following may be beneficial in decreasing the deleterious effects of total muscle ischemia in a patient who has a compartment syndrome:
1
Systemic steroids
2
Hypothermia
3
Elevation of the extremity above the heart
4
Antihypertensive therapy
5
Anticoagulant therapy
Aside from performing a fasciotomy, little can be done for patients with a compartment syndrome. Hypothermia, systemic corticosteroids, and anticoagulation therapy may increase muscle tolerance to ischemia.
Steroids and anticoagulation are not reasonable options because there is an impaired blood supply to the muscle (ie, these agents cannot enter the muscle). Hypothermia can be used to gain some time if immediate fasciotomy cannot be performed.
Steroids and anticoagulation are not reasonable options because there is an impaired blood supply to the muscle (ie, these agents cannot enter the muscle). Hypothermia can be used to gain some time if immediate fasciotomy cannot be performed.
QUESTION 33
of 100
Figure 93
Figure 93
1
Chromosome 17 mutation
2
MYH3 mutation
3
Embryonic vascular interruption
4
Infantile vascular interruption
5
Chromosome 11 mutation
- Sporadic inheritance
QUESTION 34
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is


1
open reduction and internal fixation (ORIF).
2
a mallet splint.
3
repair of the terminal tendon.
4
arthrodesis.
Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
QUESTION 35
What is the most common pathogen for soft-tissue infection of the foot caused by a puncture wound?
1
Staphylococcus aureus
2
Pseudomonas aeruginosa
3
Eikenella corrodens
4
Pasteurella multocida
5
Vibrio species
Staphylococcus and Streptococcus species are the most common causes of soft-tissue infections in the foot due to punctures. Pseudomonas is the most common cause of osteomyelitis of the foot due to puncture wounds. Pasteurella and Eikenella are seen in animal and human bites, respectively.Vibrio species are found in marine environments.
QUESTION 36
Ultrasound therapy delivers superficial heat to the tissue and has a penetration depth of 5 mm.
1
True
2
False
Ultrasound is considered a deep heat modality and does not heat the superficial tissues.
QUESTION 37
Slide 1 Slide 2 Slide 3
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
1
Gram-positive cocci
2
Gram-negative rods
3
Normal joint fluid
4
Sodium monourate crystals
5
A high red cell count
This patient most likely has an acute attack of gout. The prior episodes of foot pain and the sudden onset lasting 5 days for each bout is characteristic. The ankle is not a common location for gout (the most frequent site is the hallux metatarsophalangeal joint). The treatment should consist of injection of a corticosteroid into the joint and administration of appropriate oral anti-inflammatory medication.
QUESTION 38
The thumb metacarpophalangeal (MCP) joint should be flexed to what degree to properly assess ligamentous stability?
1
30 degrees of flexion to test the proper collateral ligament and full extension to test the accessory collateral ligament and the palmar plate
2
30 degrees of flexion to test the accessory collateral ligament and full extension to test the proper collateral ligament and the palmar plate
3
45 degrees of flexion to test the accessory collateral ligament, the proper collateral ligament, and the palmar plate
4
90 degrees of flexion to test the proper collateral ligament and full extension to test the acces sory collateral ligament and the palmar plate
5
90 degrees of flexion to test the accessory collateral ligament and full extension to test the proper collateral ligament and the palmar plate
DISCUSSION: The collateral ligaments of the MCP joint of the thumb can be isolated by flexing the joint to 30 degrees. Full extension is best to assess the accessory collaterals and the palmar plate. The ulnar collateral ligament nearly always separates from the base of first phalanx of the thumb; it frequently becomes lodged between adductor pollicis aponeurosis and its normal position (Stener lesion). The creation of a Stener lesion requires significant radial deviation of the phalanx along with combined tears of the proper and accessory collateral ligaments in order for the ligament to be displaced above the adductor aponeurosis.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 339-358.
Stener B: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1962;44:869-879.
33 • American Academy of Orthopaedic Surgeons
QUESTION 39
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
1
Nonsurgical management with the use of a cast-brace
2
Nonsurgical management with skeletal traction
3
Open treatment with a locked plate with or without strut allograft
4
Revision of the femoral component to a cemented femoral component that bypasses the fracture site by two cortical diameters
5
Revision of the femoral component to a cementless femoral component that bypasses the fracture site by at least two cortical diameters
DISCUSSION: The patient has a Vancouver type B2 periprosthetic femoral fracture with a loose, cementless femoral component. Radiographs show subsidence of the femoral component and the patient reports pain in the thigh for several years prior to the fall. When the femoral component is loose, revision is mandated to treat both the loose component and the fracture. Nonsurgical management is associated with a high risk of medical complications related to extended recumbency as well as a high rate of malunion and nonunion. Cementless femoral component revision has been shown to fare better than cemented femoral components, particularly for treating periprosthetic fractures of the femur.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
1. ### Discontinuation of the epidural and serial neurologic exams
2. ### Loosening of the surgical bandages and elevation of the extremity
3. ### MRI of the spine to evaluate for an epidural hematoma
4. ### Return to the operating room for angiography and vascular bypass
5. ### Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
QUESTION 40
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of
1
wrist extension.
2
digital abduction.
3
thumb flexion.
4
thumb opposition.
5
thumb extension.
The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition.
REFERENCES: Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
REFERENCES: Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
QUESTION 41
Emery-Dreifuss muscular dystrophy is unique among the dystrophies because of the development of which deformity:
1
Neck extension contracture
2
Hip abduction
3
Knee flexion
4
Equinus contracture
5
Scoliosis
Emery-Dreifuss muscular dystrophy is an x-linked disorder of emerin, which is a cell-membrane protein. Symptoms and signs develop within the first decade in most cases. A unique deformity, neck extension contracture, develops, in addition to elbow flexion contractures and peroneal wasting. The other deformities listed above are common in many dystrophies.
QUESTION 42
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions? ](http://www.orthobullets.com/anatomy/10106/median-nerve)

1
Median nerve lesion in the arm
2
Radial nerve lesion in the arm
3
Anterior interosseous nerve syndrome
4
Posterior interosseous nerve syndrome
5
Median neuropathy at the wrist
QUESTION 43
What percentage of the human genome represents the actual genes:
1
80%
2
66%
3
50%
4
20%
5
5%
The percentage of the genome that represents the sequence of our genes is approximately 5%. The rest of the genome codes are for initiator and termination sequences, maintenance functions, and unknown functions.
QUESTION 44
A 5-year-old boy has had a limp for the past 4 weeks with intermittent pain at the foot. He remains normally active and has no history of trauma. He has no fevers, rashes, or swelling. Examination reveals tenderness at the mid-dorsum of the foot medially. Radiographs are seen in Figures la and lb. Treatment should include which of the following?

1
MRI of the foot with gadolinium
2
Open biopsy of the lesion
3
Needle aspiration and culture, followed by antibiotic treatment
4
Observation or an orthotic arch support
5
Steroid injection of the lesion
DISCUSSION: Osteochondrosis of the tarsal navicular is most commonly identified between the ages of 2 and 9 years. The condition is benign and self limited in nature. In patients with severe pain, a period of casting may be warranted, but otherwise management usually consists of observation or a supportive orthotic.
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
8 • American Academy of Orthopaedic Surgeons**
Figure 2
QUESTION 45
Figures 1 through 3 are the MRI scans of a 56-year-old woman in good health who reports a 6-month history of shoulder pain and external rotation weakness. Her radiographs are unremarkable. What is the diagnosis?
1
Rotator cuff tear
2
Anteroinferior labral tear
3
Suprascapular nerve compression
4
Quadrilateral space syndrome
31
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr
QUESTION 46
When compared with a conventional ultra-high molecular weight polyethylene (UHMWPE) -bearing surface in total hip arthroplasty, a highly cross-linked polyethylene (XLPE) -bearing surface is associated with
1
significantly reduced wear and greater mid-term implant survival.
2
increased wear and increased fracture rate of the liner.
3
decreased mid-term implant survival when compared with UHMWPE.
4
reduced wear, but increased osteolysis.
XLPE was developed to address the problem of wear and osteolysis associated with conventional UHMWPE-bearing surfaces. Data have shown, with randomized controlled trials, that XLPE liners have significantly reduced wear and are associated with greater implant survival at 10 years compared with UHMWPE-bearing surfaces.
QUESTION 47
Haversian bone is composed of vascular channels surrounded circumferentially by lamellar bone. Which of the following terms is used to describe the unit of bone composed of a neurovascular channel surrounded by a cell-permeated layer of bone matrix:
1
Bone remodeling unit
2
Plexiform bone
3
Osteon
4
Volkman unit
5
Canaliculi
The osteon is a unique arrangement of bone cells and matrix surrounding a blood vessel. The osteon is an irregular branching, anastomosing cylinder composed of a centrally placed neurovascular canal surrounded by cell-permeated layers of bone matrix.
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
The bone remodeling unit refers to the cutting cone of leading osteoclasts and following osteoblasts.
Plexiform bone is a structural type of bone found in large animals where rapid bone growth occurs. There are alternating layers of lamellar and woven bone.
Volkman canals are the channels connecting different osteons or Haversian units.
Canaliculi are small channels through which the cell processes of the osteocytes connect to each other. Correct Answer: Osteon
QUESTION 48
A 20-year-old male military recruit reports a 5-day history of progressive deep groin pain that is made worse with weight-bearing activities and running. His initial coronal T2-weighted MRI scan is shown in Figure 75. His initial treatment should consist of which of the following?
1
Bed rest with skeletal traction (distal femur traction pin)
2
Calcium supplements
3
Crutches with protected weight bearing
4
Open reduction and internal fixation
5
Pulsed ultrasound treatment
DISCUSSION: The MRI scan findings and patient history demonstrate a compression-sided femoral neck stress fracture. The stress fracture on the coronal MRI scan involves about one third of the width of the femoral neck. Surgical treatment would be recommended for tension-sided fractures of the femoral neck. The most appropriate initial treatment is protected weight bearing, with close examination and imaging follow-up. Skeletal traction is not currently used for nondisplaced femoral neck stress fractures, and there is no indication
for open reduction and internal fixation. There is no documented role for pulsed ultrasound or calcium supplements in the acute treatment of stress fractures.
REFERENCES: Shin AY, Morin WD, Gorman JD, et al: The superiority of magnetic resonance imaging in differentiating the cause of hip pain in endurance athletes. Am J Sports Med 1996;24:168-176.
Pihlajamaki HK, Ruohola JP, Weckstrom M, et al: Long-term outcome of undisplaced fatigue fractures of the
femoral neck in young male adults. J Bone Joint Surg Br 2006;88:1574-1579.
Valimaki VV, Alfthan H, Lehmuskallio E, et al: Risk factors for clinical stress fractures in male military recruits: A prospective cohort study. Bone 2005;37:267-273.
for open reduction and internal fixation. There is no documented role for pulsed ultrasound or calcium supplements in the acute treatment of stress fractures.
REFERENCES: Shin AY, Morin WD, Gorman JD, et al: The superiority of magnetic resonance imaging in differentiating the cause of hip pain in endurance athletes. Am J Sports Med 1996;24:168-176.
Pihlajamaki HK, Ruohola JP, Weckstrom M, et al: Long-term outcome of undisplaced fatigue fractures of the
femoral neck in young male adults. J Bone Joint Surg Br 2006;88:1574-1579.
Valimaki VV, Alfthan H, Lehmuskallio E, et al: Risk factors for clinical stress fractures in male military recruits: A prospective cohort study. Bone 2005;37:267-273.
QUESTION 49
of 100
Which treatment regimen for Ewing sarcoma most effectively controls disease?
Which treatment regimen for Ewing sarcoma most effectively controls disease?
1
Chemotherapy alone
2
Chemotherapy plus wide surgical resection
3
Chemotherapy plus radiation therapy
4
Surgery plus radiation therapy
Patients with Ewing sarcoma need chemotherapy to treat micrometastatic disease. Historical outcomes of patients who receive local control alone without chemotherapy are dismal. Chemotherapy alone, however, is not adequate to control local bulky disease. Local control options include radiation therapy or wide surgical resection. Historically, it was believed that surgery should be recommended for expendable bones to minimize morbidity. More recent data support improved outcomes (vs outcomes associated with radiation alone to the primary site of disease) for patients who undergo wide surgical resection; consequently, chemotherapy plus wide surgical resection is the most effective regimen.
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
RECOMMENDED READINGS
19. [Rodriguez-Galindo C, Spunt SL, Pappo AS. Treatment of Ewing sarcoma family of tumors: current status and outlook for the future. Med Pediatr Oncol. 2003 May;40(5):276-87. Review. Erratum in: Med Pediatr Oncol. 2003 Dec;41(6):594. PubMed PMID: 12652615. ](http://www.ncbi.nlm.nih.gov/pubmed/12652615)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12652615)
20. Bacci G, Toni A, Avella M, Manfrini M, Sudanese A, Ciaroni D, Boriani S, Emiliani E, Campanacci
[M. Long-term results in 144 localized Ewing's sarcoma patients treated with combined therapy. Cancer. 1989 Apr 15;63(8):1477-86. PubMed PMID: 2924256. ](http://www.ncbi.nlm.nih.gov/pubmed/2924256)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/2924256)
21. [Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID: 20118326. ](http://www.ncbi.nlm.nih.gov/pubmed/20118326)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20118326)
22. Weis L. Ewing’s Sarcoma. In: Simon MA, Springfield D, eds. _Surgery for Bone and Soft Tissue Tumors_. Philadelphia, PA: Lippincott-Raven; 1998:287-298.
23. DuBois SG, Krailo MD, Gebhardt MC, Donaldson SS, Marcus KJ, Dormans J, Shamberger RC, Sailer S, Nicholas RW, Healey JH, Tarbell NJ, Randall RL, Devidas M, Meyer JS, Granowetter L, Womer RB, Bernstein M, Marina N, Grier HE. Comparative evaluation of local control strategies in localized
Ewing sarcoma of bone: a report from the Children's Oncology Group. Cancer. 2015 Feb 1;121(3):467-
[75/. doi: 10.1002/cncr.29065. Epub 2014 Sep 23. PubMed PMID: 25251206. ](http://www.ncbi.nlm.nih.gov/pubmed/25251206)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25251206)
QUESTION 50
A 24-year-old man has a deep knife wound across the dorsal aspect of his wrist, transecting all of his wrist and finger extensor tendons. How does the surgeon determine which of the proximal tendon stumps in the fourth dorsal compartment is the extensor indicis proprius? ](http://www.orthobullets.com/anatomy/10040/extensor-indicis)Review Topic
1
The tendon runs in a separate compartment.
2
The tendon has a more circular cross section.
3
The tendon has the most distal muscle belly.
4
The tendon is the most radial and superficial.
5
The tendon has two separate slips.
QUESTION 51
Which of the following mutations occurs in patients with diastrophic dysplasia:
1
Type II collagen mutation
2
Type V collagen mutation
3
Type I collagen mutation
4
Sulfate transporter gene mutation
5
Fibrillin gene mutation
One should remember the important mutations that occur in musculoskeletal conditions: FGFR3 mutation: Achondroplasia
Type IX collagen mutation: Multiple epiphyseal dysplasia (MED)
WISP3 mutation: Spondyloepiphyseal dysplasia with progressive osteoarthropathy
Type II collagen mutation: Stickler syndrome
Sulfate transporter gene mutation: Diastrophic dysplasia
Fibrillin gene mutation: Marfanâs syndrome
Type V collagen mutation: Ehlers-Danlos syndrome
Type I collagen mutation: Osteogenesis imperfecta
C orrect Answer: Sulfate transporter gene mutation
Type IX collagen mutation: Multiple epiphyseal dysplasia (MED)
WISP3 mutation: Spondyloepiphyseal dysplasia with progressive osteoarthropathy
Type II collagen mutation: Stickler syndrome
Sulfate transporter gene mutation: Diastrophic dysplasia
Fibrillin gene mutation: Marfanâs syndrome
Type V collagen mutation: Ehlers-Danlos syndrome
Type I collagen mutation: Osteogenesis imperfecta
C orrect Answer: Sulfate transporter gene mutation
QUESTION 52
of 100
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure

A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure
1
She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management?

2
DEXA scan
3
Brace treatment with a Jewett hyperextension brace
4
Anterior lumbar corpectomy and arthrodesis with instrumentation
5
Posterior lumbar decompression and fusion
■
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
QUESTION 53
Figures A and B are radiographic images of an 85-year-old woman with isolated left hip pain. She describes a non-syncopal fall from standing 4 hours ago. Physical examination reveals pain with log-rolling the left thigh and the inability to bear weight on the affected leg. The radiologist reports no fracture in the left hip. What would be the next best step?


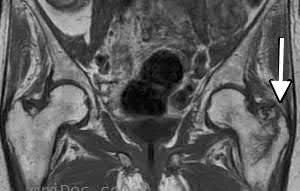
1
Stress view radiographs of the left hip
2
Non-weight bearing and pelvic bone scan in 7 days
3
Non-weight bearing and repeat the CT scan after 48 hours from injury
4
MRI hip and pelvis
5
Weight bearing activity as tolerated with close follow-up
The next best step would be an MRI hip and pelvis to investigate for an occult fracture of the left hip.
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were
negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
Answer 1: Stress view radiographs would not be recommended.
Answer 2: If MRI is contraindicated, for example if a pacemaker is present, then a bone scan at 72 hours is the next test of choice. Waiting 7 days would not be appropriate for this patient.
Answer 3: Repeating the CT scan will not help to identify fracture, unless the fracture becomes displaced. A delay in identifying a fracture pattern by 48 hours, while the patient is non-mobile, significantly increases their risk of complications.
Answer 5: Weight bearing activity as tolerated with close follow-up may be suggested if the patient is clinically able to walk and advanced imaging is negative for fracture. The best modality to rule-out occult fracture is MRI.
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were
negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
Answer 1: Stress view radiographs would not be recommended.
Answer 2: If MRI is contraindicated, for example if a pacemaker is present, then a bone scan at 72 hours is the next test of choice. Waiting 7 days would not be appropriate for this patient.
Answer 3: Repeating the CT scan will not help to identify fracture, unless the fracture becomes displaced. A delay in identifying a fracture pattern by 48 hours, while the patient is non-mobile, significantly increases their risk of complications.
Answer 5: Weight bearing activity as tolerated with close follow-up may be suggested if the patient is clinically able to walk and advanced imaging is negative for fracture. The best modality to rule-out occult fracture is MRI.
QUESTION 54
This patient developed a peripheral neuropathy of uncertain etiology. She has a partial peroneal nerve palsy with lack of extensor function of the hallux. She repeatedly stubs and catches the hallux when walking. Upon examination, she has good strength of the extensor digitorum longus tendon, as well as the anterior tibial tendon. Flexor strength of the foot is intact. All of the following are acceptable surgical alternatives except:
1
Arthrodesis of the hallux metatarsophalangeal (MP) joint
2
Tenodesis of the extensor hallucis longus tendon to the extensor digitorum longus tendon
3
Tenodesis of the extensor hallucis longus tendon to the anterior tibial tendon
4
Transfer of the peroneus tertius tendon to the extensor hallucis longus tendon
5
Transfer of a portion of the extensor digitorum longus tendon to the extensor hallucis longus tendon
When arthrodesis of the hallux MP joint is performed, it stabilizes the MP joint and continued flexion of the hallux with recurrent deformity occurs because the hallux interphalangel joint is not controlled with MP arthrodesis. All of the other procedures are satisfactory alternatives.
QUESTION 55
of 100
What is the most common complication following open reduction locking plate osteosynthesis of this injury?
What is the most common complication following open reduction locking plate osteosynthesis of this injury?
1
Intra-articular screw penetration
2
Posttraumatic avascular necrosis (AVN)
3
Nonunion
4
Subacromial plate impingement
- Intra-articular screw penetration_
QUESTION 56
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
1
Axillary nerve in the posterolateral space
2
Dorsal scapular nerve at the medial border of the scapula
3
Suprascapular nerve in the scapular notch
4
Suprascapular nerve in the spinoglenoid notch
5
Subscapular nerve at the rotator interval
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
QUESTION 57
Which of the following statements is true regarding soft tissue sarcomas:
1
Soft tissue sarcomas frequently metastasize to bone.
2
Patients with soft tissue sarcomas of the hand have worse prognosis than patients with similar tumors in other extremities.
3
Soft tissue sarcomas present as a painful mass in the hand.
4
Overall prognosis is better with radical resection than wide excision.
5
Soft tissue sarcomas can be "shelled out".
Soft tissue sarcomas in the hand present as painless lesions, do not metastasize to bone, and although local control is better with radical resection, there is no improvement in overall survival when compared to wide excision. Soft tissue sarcomas should not be "shelled out."
QUESTION 58
of 100
A patient undergoes excision of a presumed lipoma of the superficial thigh. Final pathology reveals synovial sarcoma without reference to the margins. What is the recommendation for definitive treatment?
A patient undergoes excision of a presumed lipoma of the superficial thigh. Final pathology reveals synovial sarcoma without reference to the margins. What is the recommendation for definitive treatment?
1
Observation
2
External beam radiation therapy alone
3
Wide resection of the tumor bed and radiation therapy
4
Radiation therapy and chemotherapy
An unplanned excision of a soft-tissue sarcoma occurs when a surgeon removes a soft-tissue mass while believing it is benign, and, upon pathologic examination, learns that it is malignant. These procedures often are performed without presurgical staging studies or appropriate oncologic surgical technique. Following an unplanned excision, patients usually are referred to a sarcoma center for definitive care. Definitive treatment is hindered by the lack of presurgical imaging, sophisticated pathologic examination findings, and a contaminated tumor bed larger than the original tumor. Further, as many as 50% of cases are associated with residual disease within the tumor bed, even when no tumor can be identified with imaging or an examination and the initial
surgical report indicates all gross disease has been removed. Most patients for whom an inadequate excision of an unsuspected sarcoma is performed are treated with reexcision of the tumor bed, and, very often, adjuvant radiotherapy.
RECOMMENDED READINGS
99. [Gutierrez JC, Perez EA, Moffat FL, Livingstone AS, Franceschi D, Koniaris LG. Should soft tissue sarcomas be treated at high-volume centers? An analysis of 4205 patients. Ann Surg. 2007 Jun;245(6):952-8. PubMed PMID: 17522521.](http://www.ncbi.nlm.nih.gov/pubmed/17522521)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17522521)
100. [Johnson GD, Smith G, Dramis A, Grimer RJ. Delays in referral of soft tissue sarcomas. Sarcoma. 2008;2008:378574. doi: 10.1155/2008/378574. PubMed PMID: 18317511. ](http://www.ncbi.nlm.nih.gov/pubmed/18317511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317511)
surgical report indicates all gross disease has been removed. Most patients for whom an inadequate excision of an unsuspected sarcoma is performed are treated with reexcision of the tumor bed, and, very often, adjuvant radiotherapy.
RECOMMENDED READINGS
99. [Gutierrez JC, Perez EA, Moffat FL, Livingstone AS, Franceschi D, Koniaris LG. Should soft tissue sarcomas be treated at high-volume centers? An analysis of 4205 patients. Ann Surg. 2007 Jun;245(6):952-8. PubMed PMID: 17522521.](http://www.ncbi.nlm.nih.gov/pubmed/17522521)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17522521)
100. [Johnson GD, Smith G, Dramis A, Grimer RJ. Delays in referral of soft tissue sarcomas. Sarcoma. 2008;2008:378574. doi: 10.1155/2008/378574. PubMed PMID: 18317511. ](http://www.ncbi.nlm.nih.gov/pubmed/18317511)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18317511)
QUESTION 59
When fracture step-off is greater than the accepted limits, which of the following complications is the most common:
1
Arthritis
2
Pain
3
Decreased range of motion
4
Decreased pinch strength
5
All of the above
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Pain, decreased range of motion, and decreased pinch strength also correlated with these poor outcomes.
QUESTION 60
Which of the following stress fractures is the most prone to nonunion and require surgical intervention:
1
Proximal posteromedial compression
2
Distal posteromedial compression
3
Anterior tibial cortex tension
4
Femoral shaft compression
5
Medial malleolus
The majority of stress fractures are treated with rest and protected weight-bearing. When the patient rests, strain on the affected bone is reduced and formation exceeds resorption, leading to bone healing.
An anterior tibial tension stress fracture is most prone to not healing. This fracture typically occurs in the anterior cortex and appears as a horizontal lucency â the dreaded black line.
Many patients with this fracture will not heal nonoperatively and will require intramedullary rod fixation. Correct Answe Anterior tibial cortex tension
An anterior tibial tension stress fracture is most prone to not healing. This fracture typically occurs in the anterior cortex and appears as a horizontal lucency â the dreaded black line.
Many patients with this fracture will not heal nonoperatively and will require intramedullary rod fixation. Correct Answe Anterior tibial cortex tension
QUESTION 61
A 56-year-old man has a chief complaint of leg weakness and inability to walk. Examination reveals 5out of 5 motor strength in all lower extremity muscle groups tested and normal sensation to light touch in
both lower extremities. The patient is slow in getting up from a seated position and has an unsteady widebased gait. An MRI scan of the lumbar spine is shown in Figure
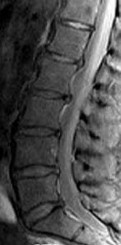
both lower extremities. The patient is slow in getting up from a seated position and has an unsteady widebased gait. An MRI scan of the lumbar spine is shown in Figure
1

What is the next most appropriate course of action?
2
Electromyography and nerve conduction velocity studies of bilateral lower extremities
3
Multilevel lumbar laminectomy
4
MRI of the thoracic and cervical spine
5
MRI of the brain
The patient is having gait problems suspicious for spinal cord compression. MRI of the thoracic and cervical spine should be performed to evaluate for spinal cord compression. Reports of leg
weakness in the absence of discrete motor weakness on manual testing, and the appearance of an unsteady wide-based gait are more consistent with myelopathy as a cause of the gait difficulty rather than lumbar stenosis. Although the MRI scan of the lumbar spine shows multilevel spinal stenosis that is mild to moderate, it does not clearly explain the patient’s signs and symptoms. Electromyography and nerve conduction velocity studies of the lower extremities are unlikely to add significantly to the diagnosis.Epidural steroid injections are not indicated. Lumbar decompression is unlikely to help the patient because the source of the patient’s problem does not originate in the lumbar spine. MRI of the brain could be considered as a secondary imaging study if the cervical and thoracic MRI scans fail to identify an obvious cause for gait instability.
weakness in the absence of discrete motor weakness on manual testing, and the appearance of an unsteady wide-based gait are more consistent with myelopathy as a cause of the gait difficulty rather than lumbar stenosis. Although the MRI scan of the lumbar spine shows multilevel spinal stenosis that is mild to moderate, it does not clearly explain the patient’s signs and symptoms. Electromyography and nerve conduction velocity studies of the lower extremities are unlikely to add significantly to the diagnosis.Epidural steroid injections are not indicated. Lumbar decompression is unlikely to help the patient because the source of the patient’s problem does not originate in the lumbar spine. MRI of the brain could be considered as a secondary imaging study if the cervical and thoracic MRI scans fail to identify an obvious cause for gait instability.
QUESTION 62
The increased radiographiCbone density in osteonecrosis is most likely secondary to:
1
Calcification of the necrotiCbone marrow
2
Insoluble soap from released calcium and free fatty acids
3
Creeping substitution on the dead trabeculae
4
Resorption of the Haversian canal bone
5
NecrotiCcortical bone
The majority of the increased radiographiCbone density in osteonecrosis is caused by new bone formation laid down on the necrotiCbone trabeculae. This occurs through the process of creeping substitution.
There is calcification of the necrotiCmarrow and insoluble soap formation from the combination of the free fatty acids and released calcium. However, this does not cause the majority of the increased radiodensity.
There is resorption of the Haversian canal bone, but this results in decreased radiodensity on the radiograph rather than increased radiodensity.
NecrotiCbone that has not gone through the repair process appears normal on the plain radiograph (neither bone resorption or creeping substitution has occurred).
There is calcification of the necrotiCmarrow and insoluble soap formation from the combination of the free fatty acids and released calcium. However, this does not cause the majority of the increased radiodensity.
There is resorption of the Haversian canal bone, but this results in decreased radiodensity on the radiograph rather than increased radiodensity.
NecrotiCbone that has not gone through the repair process appears normal on the plain radiograph (neither bone resorption or creeping substitution has occurred).
QUESTION 63
Emergent management of acute tooth displacement (luxation) includes
1
delaying replantation until a dentist is present.
2
scrubbing the root of the tooth clean with hydrogen peroxide.
3
transporting the tooth in a carbonated beverage.
4
emergency root canal.
§. immediate repositioning or replantation of the tooth.
DISCUSSION: Avulsed teeth must be replanted immediately to enhance viability of the periodontal ligament cells on the root. With the tooth in place, the athlete should bite down on a towel to maintain stability. The athlete should be taken emergently to a dentist’s office or emergency room. The avulsed tooth should not be handled by the root or scrubbed to remove debris. If immediate replantation is not possible, the tooth should be transported in saline solution, milk, or saliva on gauze.
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
DISCUSSION: Avulsed teeth must be replanted immediately to enhance viability of the periodontal ligament cells on the root. With the tooth in place, the athlete should bite down on a towel to maintain stability. The athlete should be taken emergently to a dentist’s office or emergency room. The avulsed tooth should not be handled by the root or scrubbed to remove debris. If immediate replantation is not possible, the tooth should be transported in saline solution, milk, or saliva on gauze.
REFERENCES: Flores MT, Andreasen JO, Bakland LK, et al: Guidelines for the evaluation and management of traumatic dental injuries. Dent Traumatol 2001; 17:97-102.
Ranalli DN, Demas PN: Orofacial injuries from sport preventive measures for sports medicine. Sports Med
2002;2:409-418.
QUESTION 64
What is the most well-documented advantage of computer-assisted navigation for total knee arthroplasty (TKA)?
1
Lowers risk for symptomatic fat embolization
2
Improves range of motion
3
Decreases radiographic outliers
4
Decreases blood loss
Studies of patients following TKA utilizing navigation have failed to show a significant difference in the degree of fat embolization or changes in cognition compared to standard instrumentation. Clinical results also have not changed following TKA with and without navigation in terms of range of motion or blood loss. Most studies do show a decreased incidence of radiographic outliers, however, at least in the coronal plane.
QUESTION 65
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
1
open reduction and internal fixation, followed by casting.
2
open reduction and internal fixation, followed by early range of motion.
3
open reduction and internal fixation, medial collateral ligament repair, and early range of motion.
4
open reduction and internal fixation of the ulna, application of a hinged external fixator, and early range of motion.
5
closed reduction and splinting, followed by early range of motion.
Transolecranon fracture-dislocations are most effectively managed with open reduction and internal fixation, followed by early aggressive range of motion. Concomitant injury to the collateral ligament is rare, and stability is achieved by anatomic reconstruction of the olecranon fracture with rigid fixation. The need for collateral ligament repair or a hinged external fixator is uncommon in this fracture pattern.
REFERENCE: Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
REFERENCE: Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
QUESTION 66
of 100
Recommendations for sports activity should include
Recommendations for sports activity should include
1
full participation without restrictions.
2
avoidance of contact or collision sports.
3
avoidance of racquet sports.
4
avoidance of throwing sports.
- avoidance of contact or collision sports.
QUESTION 67
In injured tissues, ischemia begins when the tissue pressure within the compartment comes within mm Hg of the diastolic pressure.
1
10
2
20
3
30
4
40
5
50
Normal tissues have adequate tissue perfusion with increases in compartment pressure to within 10 mm Hg of the diastolic pressure. In damaged tissue (eg, tibia fracture), perfusion can be impaired when the diastolic pressure reaches within 20 mm Hg of the diastolic pressure.
One should remember that hypotensive patients with extremity injuries are prone to compartment syndromes. Correct Answer: 20
One should remember that hypotensive patients with extremity injuries are prone to compartment syndromes. Correct Answer: 20
QUESTION 68
A 78-year-old woman undergoes a reverse total shoulder arthroplasty for cuff tear arthropathy. Her preoperative, 3-month postoperative, and
1
year postoperative radiographs are shown in Figures 1 through
2
What is the cause of the radiographic finding seen here?
17
3
Glenoid component malposition
4
Humeral component malposition
5
Over tensioning of the deltoid
The patient underwent a reverse arthroplasty for cuff tear arthropathy. Her preoperative radiograph shows some superior glenoid wear, which was not corrected at the time of surgery. This has resulted in superior tilt to the glenosphere, which has been identified as a risk factor for scapular notching. This occurs as a result of mechanical impingement between the medial humerus and scapular neck during arm adduction. The Beta angle and reverse shoulder angle have been proposed as measurements that can help identify pathologic glenoid tilt preoperatively. Risk factors for scapular notching include superior tilt of the glenosphere, superior placement of the glenoid baseplate on the glenoid, a 155° humeral implant angle, and incomplete lateralization of the construct.
The humeral component appears well-positioned in this radiograph. Over tensioning of the deltoid and excessive humeral lateralization would risk an acromial stress fracture and could limit shoulder range of motion. This is an inlay humeral stem, which does not lateralize the humerus.
The humeral component appears well-positioned in this radiograph. Over tensioning of the deltoid and excessive humeral lateralization would risk an acromial stress fracture and could limit shoulder range of motion. This is an inlay humeral stem, which does not lateralize the humerus.
QUESTION 69
A 35-year-old male sustains the fracture seen in Figures A and B. Which of the following substances has been shown to result in the least radiographic subsidence when combined with open reduction and internal fixation?


1
Cancellous allograft bone chips
2
Autograft iliac crest
3
Femoral intramedullary reamings
4
Calcium phosphate cement
5
Calcium sulfate cement
Figures A and B show a plateau fracture with a lateral split and depression of the articular surface. In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations due to its high compressive strength.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
QUESTION 70
A 16-year-old boy with type I Ehlers-Danlos syndrome has a spinal curvature that has progressed 18° in the past year. The curve is a double major type with a C obb angle of 60° in each curve. There is no associated kyphosis. The following treatment is recommend:
1
Observation
2
Bracing
3
Anterior fusion and instrumentation
4
Posterior fusion and instrumentation
5
Anterior and posterior fusion with instrumentation
Posterior fusion and instrumentation is the best-documented treatment. Although this form of treatment is followed by an increased incidence of wound healing problems, the problems can be treated.
Observation is not recommended because the curve is highly likely to increase and cause a decrease in pulmonary function.
Bracing has no role in large curves, and it is not known if bracing is successful in Ehlers-Danlos syndrome.
Anterior fusion with instrumentation would be difficult with a double curve. Anterior fusion carries an increased risk due to vascular fragility. It is not necessary because there is no increased risk of crankshaft or pseudarthrosis.
There is no particular reason for adding an anterior procedure in this situation in view of the vascular risk.
Observation is not recommended because the curve is highly likely to increase and cause a decrease in pulmonary function.
Bracing has no role in large curves, and it is not known if bracing is successful in Ehlers-Danlos syndrome.
Anterior fusion with instrumentation would be difficult with a double curve. Anterior fusion carries an increased risk due to vascular fragility. It is not necessary because there is no increased risk of crankshaft or pseudarthrosis.
There is no particular reason for adding an anterior procedure in this situation in view of the vascular risk.
QUESTION 71
Which of the following cell type-cell function pairings is false:
1
Pre-osteoblasts â stem cell for osteoblasts
2
Osteoblasts â synthesize organiCmatrix
3
Ostecytes â maintain mineral homeostatsis
4
Osteoclasts â synthesize organiCmatrix
5
Osteoblasts â receptors for PTH
Osteoclasts resorb bone by attaching to the bone surface, releasing enzymes, and dissolve the organiCmineral phases of bone. Osteoclasts do not have hormone receptors
QUESTION 72
..What is the most likely predictor of postsurgical pain following a coracoid transfer procedure for recurrent shoulder instability?
1
Suboptimal graft placement
2
Pain before surgery
3
Progression of osteoarthritis
4
Previous surgical treatment
DISCUSSION…Recurrent glenohumeral instability with anteroinferior glenoid bone loss is best treated with a coracoid transfer. Schmid and associates reported on 49 patients with these lesions and recurrent instability who underwent coracoid transfer procedures. Good and excellent outcomes were reported in 88% of patients, and there were no instances of recurrent instability.
With anteroinferior glenoid bone loss, capsular procedures—whether open or arthroscopic—are unlikely to provide stability. Remplissage is a procedure designed to address Hill-Sachs lesions rather than glenoid defects. The absolute indications to treat Hill-Sachs lesions surgically include a lesion associated with a humeral head fracture, a lesion involving more than 30% of the humeral head with chronic instability, and reverse Hill-Sachs lesions involving more than 20% of
the articular surface with symptoms of posterior instability. Lesions involving 20% to 35% with or without engagement on examination are relative indications, as are lesions exceeding 10% that do not remain centered in the glenoid following arthroscopic stabilization.
In Schmid and associates’ series of coracoid transfers for recurrent instability and anterior glenoid deficiency, patients who reported pain before surgery were 20 times more likely to have pain after surgery that compromised the functional outcome. Optimal graft placement correlated with better functional outcomes and less progression of arthrosis, but not with pain. Consequently, poor graft position, arthritis progression, and prior surgical treatment are not as consistently predictive of pain after surgery.
- Coracoid transfer
P R: 4- A lesion involving 40% of the humeral head with recurrent glenohumeral instability PREFERRED RESPONSE: 2- Pain before surgery
P R: 4- A lesion involving 40% of the humeral head with recurrent glenohumeral instability PREFERRED RESPONSE: 2- Pain before surgery
QUESTION 73
slide 1 slide 2
A patientâs upper extremity radiographs are shown in Slide 1 and Slide 2. What is the most likely inheritance pattern of this condition:
A patientâs upper extremity radiographs are shown in Slide 1 and Slide 2. What is the most likely inheritance pattern of this condition:
1
X-linked recessive
2
X-linked dominant
3
Autosomal recessive
4
Autosomal dominant
5
Sporadic
This patient has multiple hereditary exostoses. Note the multiple sessile osteochondromas on the humerus and ulna. A
characteristic bowing deformity of the forearm and pseudo-Madelung deformity of the wrist are also present.
Multiple hereditary exostoses is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring is approximately 10%.
In most patients, the forearm deformity does not cause a major problem and can be treated nonoperatively. Correct Answe Autosomal dominant
characteristic bowing deformity of the forearm and pseudo-Madelung deformity of the wrist are also present.
Multiple hereditary exostoses is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring is approximately 10%.
In most patients, the forearm deformity does not cause a major problem and can be treated nonoperatively. Correct Answe Autosomal dominant
QUESTION 74
A 25-year-old laborer sustains a transverse fracture of the proximal 25% of the scaphoid. CT reconstructions reveal a 1-mm fracture gap. What is the most appropriate treatment?
1
Above-elbow thumb spica cast
2
Short arm thumb spica cast
3
Scaphotrapezial-trapezoidal (STT) fusion
4
Excision of the proximal pole
5
Internal fixation of the fracture with a compression screw
A higher risk of nonunion and the need for prolonged immobilization is seen after nonsurgical management of proximal pole fractures of the scaphoid. Because of the relatively poor blood supply of the proximal pole, surgical treatment with a compression screw is advocated for fractures of the proximal third of the scaphoid.
REFERENCES: Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Ring D, Jupiter JB, Herndon JH: Acute fractures of the scaphoid. J Am Acad Orthop Surg 2000;8:225-231.
REFERENCES: Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Ring D, Jupiter JB, Herndon JH: Acute fractures of the scaphoid. J Am Acad Orthop Surg 2000;8:225-231.
QUESTION 75
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
1
arthroscopic synovectomy.
2
humeral arthroplasty.
3
unconstrained total shoulder arthroplasty.
4
constrained total shoulder arthroplasty with a fixed-fulcrum prosthesis.
5
glenohumeral arthrodesis.
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred.
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
QUESTION 76
of 100
Figures 58a through 58c are the radiograph, MR image, and sagittal CT scan of a 13-year-old boy with a 5-month history of a left hip injury. He has no current pain, but substantial, progressive limitations in hip flexion are present. What is the most likely diagnosis?

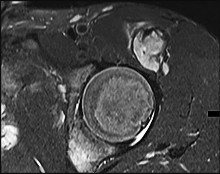

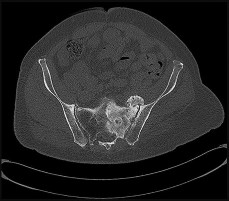
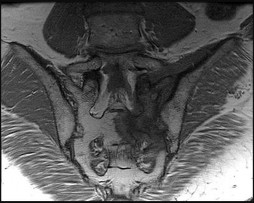
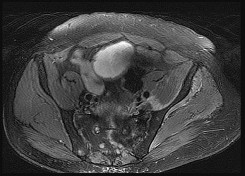
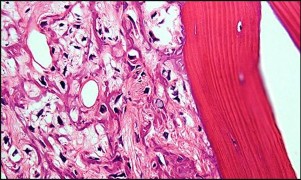
Figures 58a through 58c are the radiograph, MR image, and sagittal CT scan of a 13-year-old boy with a 5-month history of a left hip injury. He has no current pain, but substantial, progressive limitations in hip flexion are present. What is the most likely diagnosis?
1
Extraskeletal osteosarcoma
2
Myositis ossificans
3
Chondrosarcoma
4
Pelvic osteosarcoma
This patient has a mineralized mass in the soft tissues in the rectus femoris origin. The clinical history favors an avulsion injury with subsequent myositis ossificans, and the imaging is consistent with an ossified soft-tissue mass. Extraskeletal osteosarcoma is a rare soft-tissue sarcoma and is generally seen in adults. Chondrosarcoma is also generally seen in adults and would have a more chondroid matrix as opposed to mature-looking bone on a CT scan. Pelvic osteosarcoma could have this appearance on radiograph, but the CT scan and MR image confirm this is a soft-tissue process with mature mineralization.
RECOMMENDED READINGS
13. Tyler P, Saifuddin A. The imaging of myositis ossificans. Semin Musculoskelet Radiol. 2010 Jun;14(2):201-16. doi: 10.1055/s-0030-1253161. Epub 2010 May 18. Review. PubMed PMID:
[20486028/. ](http://www.ncbi.nlm.nih.gov/pubmed/20486028)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20486028)
14. [Colman MW, Lozano-Calderon S, Raskin KA, Hornicek FJ, Gebhardt M. Non-neoplastic soft tissue masses that mimic sarcoma. Orthop Clin North Am. 2014 Apr;45(2):245-55. doi: 10.1016/j.ocl.2013.12.006. Epub 2014 Feb 1. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24684918)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24684918)
CLINICAL SITUATION FOR QUESTIONS 59 THROUGH 61
Figures 59a through 59d are the CT scans and biopsy specimen of a 68-year-old man with progressive radicular symptoms in his left lower extremity. Four years previously he underwent treatment of colorectal cancer with surgery, chemotherapy, and radiotherapy.
RECOMMENDED READINGS
13. Tyler P, Saifuddin A. The imaging of myositis ossificans. Semin Musculoskelet Radiol. 2010 Jun;14(2):201-16. doi: 10.1055/s-0030-1253161. Epub 2010 May 18. Review. PubMed PMID:
[20486028/. ](http://www.ncbi.nlm.nih.gov/pubmed/20486028)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20486028)
14. [Colman MW, Lozano-Calderon S, Raskin KA, Hornicek FJ, Gebhardt M. Non-neoplastic soft tissue masses that mimic sarcoma. Orthop Clin North Am. 2014 Apr;45(2):245-55. doi: 10.1016/j.ocl.2013.12.006. Epub 2014 Feb 1. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24684918)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24684918)
CLINICAL SITUATION FOR QUESTIONS 59 THROUGH 61
Figures 59a through 59d are the CT scans and biopsy specimen of a 68-year-old man with progressive radicular symptoms in his left lower extremity. Four years previously he underwent treatment of colorectal cancer with surgery, chemotherapy, and radiotherapy.
QUESTION 77
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of
1
continued non-weight-bearing and a bone stimulator.
2
removal of the hardware, bone grafting of the femoral neck, and refixation.
3
removal of the hardware and hemiarthroplasty.
4
removal of the hardware and total hip arthroplasty.
5
removal of the hardware and a valgus osteotomy.
The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy.
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
QUESTION 78
A 45-year-old coach sustains a complete distal biceps tendon rupture at the elbow. Surgical repair is most indicated to
1
restore full supination strength.
2
restore full elbow flexion strength.
3
restore full range of motion.
4
improve cosmesis.
5
prevent degenerative changes of the elbow.
DISCUSSION: The biceps is primarily responsible for supination of the forearm. The brachialis muscle is primarily repsonsible for elbow flexion strength. Failure to repair the distal biceps tendon will result in loss of 40% supination strength and 10% loss in flexion strength. Therefore, surgical repair of a complete distal biceps tendon rupture is most indicated to maximize supination strength. Improved cosmesis should not be the primary indication for surgical repair. Degenerative changes of the elbow have no bearing on whether the distal biceps is repaired or not. Loss of terminal extension is common in distal biceps tendon repairs.
REFERENCES: Altcheck DW, Altcheck AJ: The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 288.
Morrey BF, Askew LJ, An KN, et al: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418^4-21.
REFERENCES: Altcheck DW, Altcheck AJ: The Athlete’s Elbow. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, p 288.
Morrey BF, Askew LJ, An KN, et al: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418^4-21.
QUESTION 79
A 24-year-old female soccer player has recurrent instability following noncontact injury to the right knee 2 years after anterior cruciate reconstruction using hamstring autograft. Physical examination reveals positive Lachman and pivot shift. Radiographs reveal well-preserved joint spaces with 13° of posterior tibial slope. MRI scan reveals failure of graft with small tear of the lateral meniscus. What is the most appropriate treatment?
1
Revision anterior cruciate ligament (ACL) reconstruction using patellar tendon autograft and lateral meniscal repair
2
Revision ACL reconstruction with proximal tibial osteotomy and lateral meniscal repair
3
Revision ACL reconstruction using autograft and meniscal transplant
4
Partial lateral meniscectomy and functional bracing
Increased tibial slope (>12°) may be a risk factor for noncontact ACL injury and subsequent failure of repair, and corrective proximal tibial osteotomy may be indicated combined with primary or revision ACL reconstruction. The indications for proximal tibial valgus osteotomy are generally isolated medial compartment degeneration in a knee with varus malalignment in a young, active individual. Factors associated with early failure include increased age (>55 years), increased BMI (10% greater than normal), preoperative flexion
<120° and under- or overcorrection. Inflammatory arthritis, including gout, would be a relative contraindication.
<120° and under- or overcorrection. Inflammatory arthritis, including gout, would be a relative contraindication.
QUESTION 80
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
1
Spiral fracture pattern
2
Low-energy mechanism
3
Amount of shortening
4
Fracture of the fibula at a different level
5
Ipsilateral femoral fracture
All the factors listed, with the exception of an ipsilateral femoral fracture, are representative of a low-energy stable tibial shaft fracture that will do well with closed reduction and immobilization in a long leg cast, followed by weight bearing as tolerated and then a functional brace or patellar tendon bearing cast until union is achieved. Shortening will not increase from that seen on these initial radiographs. The spiral fracture provides a broad surface for healing, and the fibular fracture at another level indicates a stable soft-tissue envelope which, with the immobilization device, will stabilize the fracture reduction. An ipsilateral femoral fracture is a strong indication to surgically stabilize both fractures.
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
QUESTION 81
A magnetic resonance image of a 7-year-old girl shows a line of high-signal intensity within the cord on T2 sequences that parallels the ventral surface of the cord and appears as a syrinx. However, on the axial images and on the T1 sequences, this finding is not evident. The most likely diagnosis is:
1
C ollapsing syrinx
2
Gibbs artifact
3
Motion artifact
4
Ependymoma
5
Astrocytoma
A Gibbs artifact is a linear focus in the cord on T2-weighted images that parallels the ventral aspect of the cord and mimics a syrinx. The Gibbs artifact is due to the linear interface between two tissues of differing signal intensity. It is not seen on axial images or T1-weighted images.
Motion artifact is a blurring of the image due to patient motion, respiration, or cerebral spinal fluid pulsation. Ependymoma and astrocytoma are seen on both the axial and the sagittal images.
Motion artifact is a blurring of the image due to patient motion, respiration, or cerebral spinal fluid pulsation. Ependymoma and astrocytoma are seen on both the axial and the sagittal images.
QUESTION 82
of 100
The floor of the acetabular fossa touches the ilioischial line
The floor of the acetabular fossa touches the ilioischial line
1
Figure 51a
2
Figure 51b
3
Figure 51c
4
Figure 51d
5
Figure 51e
- Figure 51e_
QUESTION 83
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?

1
Tuberculosis
2
Hepatitis B
3
HIV
4
West Nile virus
5
Clostridium
DISCUSSION: The only reported cases of HIV transmission with tissue transplantation occurred more than 20 years ago. The only reported cases of tuberculosis and hepatitis B occurred more than 50 years ago. The donor-associated clostridium infection occurred in 2001. The facility was not AATB-accredited (American Association of Tissue Banks) and the local A ATB facility refused the graft. It is necessary for the surgeon using the allograft tissue to be aware of the current status of tissue regulation, and procurement and processing procedures.
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006. Question 74
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
1. #### Discoid meniscus
2. #### Posterolateral comer injury
3. #### Vertical meniscal tears
4. #### Middle third lateral meniscal tears
5. #### Popliteus tendon tears
PREFERRED RESPONSE: 4
DISCUSSION: Lateral meniscal cysts often arise from myxoid degeneration that progresses from the meniscal center and then outside the meniscus. Horizontal cleavage tears are commonly associated with the condition.
Cysts of the lateral meniscus are most commonly the consequence of a tear located in the medial third. If the
tear communicates with the joint, arthroscopic partial meniscectomy and cyst decompression are indicated. If the tear does not open into the joint, arthroscopy should be followed by an open cystectomy.
REFERENCES: Hulet C, Souquet D, Alexandre P, et al: Arthroscopic treatment of 105 lateral meniscal cysts with 5-year average follow-up. Arthroscopy 2004;20:831-836.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part I. Macroscopic and histologic findings. Clin Orthop
Relat Res 1980;146:289-300.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part II. Horizontal cleavages and lateral cysts. Clin Orthop Relat Res 1980:146:301-307.
Figure 75
QUESTION 84
.Figures 11a and 11b show the radiographs of the open fracture of a 46-year-old man who injured his elbow on his nondominant arm in a motorcycle crash. On the day of injury, he underwent irrigation and débridement of the fracture. He was also treated with antibiotics. Which of the following definitive treatment methods will most likely lead to the best functional outcome?

1
Cast immobilization
2
Intramedullary screw fixation
3
Open reduction and plate fixation
4
Open reduction and internal fixation with tension band wiring
5
Fragment excision and triceps advancement
QUESTION 85
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
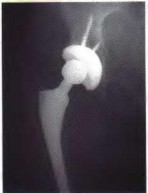

1
initiation of a first-generation cephalosporin while awaiting culture results.
2
initiation of broad-spectrum antibiotics while awaiting culture results.
3
ultrasound to evaluate for fluid collection around the knee.
4
surgical debridement of the knee before culture results are available.
5
inpatient observation and no antibiotics until culture results are available.
Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
Figure 3a Figure 3b
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
Figure 3a Figure 3b
QUESTION 86
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of
1
weight bearing as tolerated in a hard-soled shoe.
2
weight bearing as tolerated in an ankle lacer.
3
weight bearing as tolerated in a short leg cast.
4
non-weight-bearing in a hard-soled shoe.
5
non-weight-bearing in a short leg cast.
The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated.
REFERENCES: Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Lawrence SJ, Botte MJ: Jones’ fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.
REFERENCES: Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Lawrence SJ, Botte MJ: Jones’ fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.
QUESTION 87
ORTHOPEDIC MCQS BANK ONLINE OITE 21
For OITE 21 FIGURES CLICK OITE21FIG
For OITE 21 FIGURES CLICK OITE21FIG
1
01.1 A 49-year-old man has a persistent Trendelenburg gait after undergoing open
2
reduction and internal fixation of a posterior wall acetabular fracture 6 months
3
ago. The radiographs reveal a normal joint space with no heterotopic ossification
4
and no signs of osteonecrosis. Weakness in what muscle group is the most likely
5
cause of his limp?
for this finding?
6. 1- The arthritis has stabilized.
7. 2- The C1-2 joint has fused.
8. 3- The patient has been wearing a cervical collar.
9. 4- Medical advancements have been made in the management of arthritis.
10. 5- Basilar impression (atlantoaxial impaction) has developed.
1. answer
1. back
1. Question 01.87
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Oda T, Fujiwara K, Yonenobu K, Azuma B, Ochi T: Natural course of cervical spine lesions in rheumatoid arthritis. Spine 1995;20:1128-1135.
1. 01.88 A woman with degenerative arthritis and a fixed genu valgum deformity of 17°
2. undergoes primary total knee arthroplasty under general anesthesia. In the
3. recovery room, she is unable to dorsiflex her foot. Immediate management
4. should include
5. 1- fasciotomies.
6. 2- surgical nerve decompression.
7. 3- flexion of the knee.
8. 4- continuous passive motion.
9. 5- electromyography.
1. answer
1. back
1. Question 01.88
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mont MA, Dellon AL, Chen F, Hungerford MW, Krackow KA, Hungerford DS: The operative treatment of peroneal nerve palsy. J Bone Joint Surg Am 1996;78:863-869. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
1. 01.89 A 30-year-old professional soccer player sustains a midshaft fracture of the tibia
2. and fibula. History reveals that the patient underwent a successful anterior
3. cruciate ligament reconstruction with central one third bone-patellar tendon-bone
4. autograft and graft fixation with interference screws 2 years ago. Figures 22a and
5. 22b show the pre-and postoperative radiograph. What is the most likely
6. postoperative complication in this patient?
7. 1- Loss of graft fixation
8. 2- Fracture through the tibial
9. tunnel
10. 3- Galvanic corrosion
11. (battery effect)
12. 4- Anterior knee pain
13. 5- Saphenous neuralgia
1. answer
1. back
1. A
1. B
1. Figures 22
1. Question 01.89
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Keating JF, Orfaly R, O'Brien PJ: Knee pain after tibial nailing. J Orthop Trauma 1997;11:10-13. Roberts C, John C, Seligson D: Prior anterior cruciate ligament reconstruction complicating intramedullary nailing of a tibia fracture. Arthroscopy 1998;14:779-783.
1. 01.90 Which of the following muscles protracts the shoulder?
2. 1- Serratus anterior
3. 2- Rhomboid major
4. 3- Trapezius
5. 4- Latissimus dorsi
6. 5- Subscapularis
1. answer
1. back
1. Question 01.90
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Kahn JF, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
1. 01.91 Which of the following pharmacologic agents may antagonize the
2. anticoagulation effect of warfarin?
3. 1- Cefamandole
4. 2- Cimetidine
5. 3- Phenytoin
6. 4- Trimethoprim
7. 5- Phenobarbital
1. answer
1. back
1. Question 01.91
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 487-517.
1. 01.92 Figures 23a and 23b show an AP open mouth view and a CT scan at C1-2.
2. Because this is an acute injury with no neurologic deficit, the best course of
3. action should be
4. 1- acute occipital-cervical fusion with rigid instrumentation.
5. 2- use of a soft collar.
6. 3- use of a halo vest for 3 months, followed by assessment for C1-2 instability.
7. 4- a gradual return to activity with no restrictions.
8. 5- flexion-extension radiographs to help determine the need for surgery.
1. answer
1. back
1. A
1. B
1. Figures 23
1. Question 01.92
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Levine AM: Orthopaedic Knowledge Update: Trauma. Rosemont. IL. American Academy of Orthopaedic Surgeons, 1996, pp 317-322.
1. 01.93 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.94 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.95 Intradiscal pressure in the third lumbar disk is least in which of the following
2. positions?
3. 1- Sitting, flexed forward slightly
4. 2- Sitting, straight
5. 3- Laying, supine
6. 4- Standing, straight
7. 5- Standing, slightly extended
1. answer
1. back
1. Question 01.95
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Nachemson A: The lumbar spine: An orthopaedic challenge. Spine 1976;1:59-71. White AA II, Panjabi MM (eds): Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 454-461.
1. 01.96 A 35-year-old man who sustained a grade II open fracture of the right tibia 9
2. months ago underwent reamed intramedullary nailing. The patient continues to
3. have pain with weight bearing. Laboratory studies show a normal WBC and
4. erythrocyte sedimentation rate, and there has been no change in the radiographs
5. in the past 3 months. Current radiographs are shown in Figures 24a and 24b.
6. What is the most likely diagnosis?
7. 1- Delayed union
8. 2- Aseptic nonunion
9. 3- Infected nonunion
10. 4- Synovial pseudarthrosis
11. 5- Failure of the internal fixation device
1. answer
1. back
1. A
1. B
1. Figures 24
1. Question 01.96
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Browner BD, Jupiter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 68-72. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 25-35.
1. 01.97 Figure 25 shows the AP radiograph of a 20-year-old man who sustained a
2. twisting injury to his foot. An attempt at closed reduction is unsuccessful, most
3. likely because of
4. 1- buttonholing of the talar head through the extensor retinaculum.
5. 2- osteochondral fracture of the posterior facet of the talus.
6. 3- interpositioning of the peroneal tendons.
7. 4- interpositioning of the posterior tibial tendon.
8. 5- fracture of the talar neck.
1. answer
1. back
1. Figure 25
1. Question 01.97
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Bellabarba C, Sanders R: Dislocation of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1519-1573. Hansen ST 1r: Foot injuries, in Browner BD, Jupiter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 2405-2438. DeLee JC, Curtis R: Subtalar dislocation of the foot. J Bone Joint Surg Am 1982;64:433-437.
1. 01/. 98 A 65-year-old man has had progressively worsening pain and limited motion in
2. the left shoulder for the past year. History reveals that he sustained a
3. nondisplaced fracture of the surgical neck of the humerus 10 years ago. Plain
4. radiographs are shown in Figures 26a and 26b. What is the most likely
5. diagnosis?
6. 1- Osteonecrosis
7. 2- Posttraumatic osteoarthritis
8. 3- Rheumatoid arthritis
9. 4- Gouty arthritis
10. 5- Chondrocalcinosis
1. answer
1. back
1. A
1. B
1. Figures 26
1. Question 01.98
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Matsen FA III, Rock-wood CA Jr, Wirth MA, Lippitt SB: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III, Wirth MA, Harryman DT II (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, pp 840-964.
1. 01.99 A 14-year-old basketball player has had activity-related low back pain for the
2. past 6 weeks. Plain radiographs are unremarkable. Selected coronal single-
3. photon emission computed tomography scans are shown in Figure 27. The best
4. course of action should be
5. 1- bilateral facet blocks.
6. 2- brace immobilization for 3 to 6 months.
7. 3- instrumented posterior spinal fusion.
8. 4- a CT-guided needle biopsy.
9. 5- an open incisional biopsy.
1. answer
1. back
1. Figure 27
1. Question 01.99
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Loder RT, Hensinger RN: Fractures of the thoracic and lumbar spine, in Rockwood CA, Wilkins KE, Beaty 1H (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1062-1096. Lonstein JE: Spondylolysis and spondylolisthesis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 717-737. Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253. Lonstein JE: Spondylolisthesis in children: Cause. natural history, and management. Spine 19994:2640-2648. Anderson K, Sarwark JF, Conway JJ, Logue ES, Schafer WI: Quantitative assessment with SPELT imaging of stress injuries of the pats interarticularis and response to bracing. J Pediatr Orthop 2000;20:28-33.
1. 01.100 Which of the following is considered an advantage of the inside-out technique
2. for meniscal repairs compared with the outside-in technique?
3. 1- Improved ultimate knee motion
4. 2- Increased rate of healing
5. 3- Diminished infection rates
6. 4- The ability to achieve proper suture orientation in posterior horn tears
7. 5- Decreased risk of neurologic injury
1. answer
1. back
1. Question 01.100
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Rodeo SA: Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect 2000;49:195-206. Post WR, Akers SR, Kish V: Load to failure of common meniscal repair techniques: Effects of suture technique and suture material. Arthroscopy 1997;13:731-736.
1. 01.101 An anterior (Smith-Peterson) approach to the hip joint uses what internervous
2. plane?
3. 1- Superior gluteal and femoral
4. 2- Superior gluteal and inferior gluteal
5. 3- Femoral and obturator
6. 4- Sciatic and superior gluteal
7. 5- Sciatic and femoral
1. answer
1. back
1. Question 01.101
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp 303-32I.
1. 01.102 A 21-year-old man sustains the acetabular fracture shown in Figures 28a
2. through 28c. The best outcomes following surgical treatment of this fracture
3. have been reported with which
4. of the following surgical
5. approaches?
6. 1- Posterior (Kocher-Langenbeck)
7. 2- Triradiate
8. 3- Extended iliofemoral
9. 4- Modified extensile lateral
10. 5- Ilioinguinal
1. answer
1. back
1. A
1. B
1. Figures 28
1. C
1. Question 01.102
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clip Orthop 1993;292:62-76.
1. 01.103 What type of injury is shown in Figure 29?
2. 1- Compression fracture
3. 2- Burst fracture
4. 3- Flexion-distraction
5. 4- Extension injury
6. 5- Fracture-dislocation
1. answer
1. back
1. Figure 29 (all three)
1. Question 01.103
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Dents F: The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983;8:817-831.
1. 01.104 A 55-year-old patient underwent a total hip arthroplasty with a diaphyseal -
2. locking, fully porous-coated cementless femoral prosthesis 8 years ago.
3. Radiographs reveal a distally fixed stem with distal spot welds and proximal
4. bone loss. The femoral head is located concentrically within the acetabulum.
5. What is the most likely etiology of the bone loss?
6. 1- Bone hypertrophy
7. 2- Stress shielding
8. 3- Osteoporosis
9. 4- Osteolysis
10. 5- Osteonecrosis
1. answer
1. back
1. Question 01.104
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 1995, pp 127-138.
1. 01.105 Endurance strength training has been shown to have which of the following
2. demonstrated physiologic effects?
3. 1- Decreases aerobic capacity
4. 2- Decreases bone mineral density with weight-bearing activities
5. 3- Decreases type II muscle fiber cross-sectional area
6. 4- Increases heart rate at rest
7. 5- Improves blood lipid profiles
1. answer
1. back
1. Question 01.105
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Miszko T, Cress M: A lifetime of fitness, in Clinics in Sports Medicine. Philadelphia, PA, WB Saunders, 2000, vol 19, pp 215-232. Blumenthal JA, Emery CF, Madden DJ, et al: Cardiovascular and behavioral effects of aerobic exercise training in healthy older men and woman. J Gerontol
3. 1989;44:147-157.
1. 01.106 What organ secretes calcitonin?
2. 1- Parathyroid
3. 2- Thyroid
4. 3- Kidney
5. 4- Bone
6. 5- Skin
1. answer
1. back
1. Question 01.106
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Silver JJ, Majeska RJ, Einhorn TA: An update on bone cell biology. Curr Opin Orthop 1994;5:50-59.
1. 01.107 The volar radioscapholunate ligament (ligament of Testut) functions primarily
2. as a
3. 1- neurovascular conduit.
4. 2- stabilizing ligament of the scapholunate interval.
5. 3- stabilizing ligament of the radiocarpal joint.
6. 4- stabilizing ligament of the midcarpal joint.
7. 5- septal ligament contiguous with the interfossal ridge.
1. answer
1. back
1. Question 01.107
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Berger RA, Landsmeer JM: The palmar radiocarpal ligaments: A study of adult and fetal human wrist joints. J Hand Surg Am 1990;15:847-854. Hixson ML, Stewart C: Microvascular anatomy of the radioscapholunate ligament of the wrist. J Hand Surg Am 1990;15:279-282.
1. 01.108 A 19-year-old man reports groin pain after undergoing antegrade nailing of a
2. femoral shaft fracture 3 weeks ago. Figures 30a and 30b show the current
3. radiograph and tomogram. The next most appropriate step in management
4. should consist of
5. 1- observation.
6. 2- electrical stimulation.
7. 3- resection of
8. heterotopic
9. ossification.
10. 4- exchange nailing.
11. 5- screw fixation
12. around the nail.
1. answer
1. back
1. A
1. B
1. Figures 1
1. Question 01.108
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 177-190.
1. 01.109 What is the most common mechanism of injury to the adult spinal cord?
2. 1- Gunshot wounds
3. 2- Falls
4. 3- Motor vehicle accidents
5. 4- Sporting injuries
6. 5- Suicide attempts
1. answer
1. back
1. Question 01.109
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Slucky AV, Eismont FJ: Treatment of acute injury of the cervical spine. Instr Course Lect 1995;44:67-80. Vaccaro AR, An HS, Betz RR, Coder JM, Balderston RA: The management of acute spinal trauma: Prehospital and in-hospital emergency care. Instr Course Lect 1997;46:113-125.
1. 01.110 A 33-year-old woman has had progressive rheumatoid arthritis for the past 12
2. years. Figure 31 shows the postoperative radiograph. What is the most likely
3. long-term symptomatic complication following this procedure?
4. 1- Nonunion of the first metatarsophalangeal joint
5. 2- Chronic infection
6. 3- Plantar callosities
7. 4- Recurrent hammer toe deformity
8. 5- Interphalangeal joint arthritis of the great toe
1. answer
1. back
1. Figure 31
1. Question 01.110
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term follow-up study. J Bone Joint Surg Am 2000;82:322-341. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 293-303.
1. 01.111 A 12-year-old boy is referred for evaluation of a spinal deformity. Examination
2. and history reveal that he and one of his two sisters have numerous light brown
3. birthmarks distributed on all areas of the body. The radiograph shown in Figure
4. 32 reveals a curve that measures 70°. The best course of action should include
5. 1- MRI of the entire spine.
6. 2- brace treatment with a thoracolumbosacral
7. orthosis.
8. 3- posterior spinal fusion and observation for
9. possible crankshaft progression of the curve.
10. 4- a period of observation to determine whether the
11. curve may progress.
12. 5- a renal ultrasound and echocardiogram.
1. answer
1. back
1. Figure 32
1. Question 01.111
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Crawford AH: Neurofibromatosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 619-650. Crawford AH, Gabriel KR: Dysplastic scoliosis: Neurofibromatosis, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA,
3. Lippincott-Raven, 1997, pp 276-298.
1. 01.112 A 33-year-old man fell from a height of 25 feet and sustained a fracture-
2. dislocation of the right elbow. Following closed reduction of the elbow in the
3. emergency department, plain radiographs show a displaced radial neck and a
4. type II coronoid fracture. Examination reveals elbow swelling and wrist
5. tenderness. The neurologic examination is normal. Treatment of the elbow
6. should include
7. 1- excision of the radial head and coronoid fragment.
8. 2- excision of the radial head and open reduction and internal fixation of the coronoid.
9. 3- open reduction and internal fixation of the radial head and excision of the coronoid
10. fragment.
11. 4- open reduction and internal fixation of the radial head and coronoid.
12. 5- replacement of the radial head and excision of the coronoid fragment.
1. answer
1. back
1. Question 01.112
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? Am Acad Orthop Surg 1997;5:1-10. Money BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128. Began W, Money B: Fractures of the coronoid process of the ulna,. J Bone Joint Surg Am 1989;71:1348-1354.
1. 01.113 A 21-year-old patient sustains a fracture of the humeral shaft that is treated as
2. shown in Figures 33a and 33b. The reported incidence of shoulder problems
3. following this method of fracture stabilization is approximately what percent?
4. 1- 0% to 5%
5. 2- 6% to 10%
6. 3- 11% to 15%
7. 4- 16% to 20%
8. 5- 21 % to 25 %
1. answer
1. back
1. A
1. B
1. Figures 33
1. Question 01.113
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Chapman JR, Henley MB, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. McCormack RG, Briers D, Buckley RE, McKee MD, Powell J, Schemitsch EH: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective randomized trial. J Bone Joint Surg Br 2000;82:336-339.
1. 01.114 A revision total knee arthroplasty was performed on a patient who was
2. presumed to have aseptic loosening. Antibiotic-impregnated cement was used
3. at the time of reimplantation. Interface membrane cultures taken routinely at
4. the time of the revision revealed coagulase-negative staphylococci 2 days after
5. surgery. Appropriate management should consist of
6. 1- antibiotic therapy alone.
7. 2- surgical debridement with polyethylene exchange.
8. 3- one-staged exchange of both components.
9. 4- two-staged exchange of both components.
10. 5- knee fusion.
1. answer
1. back
1. Question 01.114
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Segawa H, Tsukayama DT, Kyle RF, Becker DA, Gustilo RB: Infection after total knee arthroplasry: A retrospective study of the treatment of eighty-one infections.
3. J Bone Joint Sur- Am 1999;81:1434-1445.
1. 01.115 A 38-year-old man underwent anterior cruciate ligament reconstruction 12
2. weeks ago. Examination of the knee now reveals active arc of motion from 15°
3. to 80°. Patellar mobility is limited. Radiographs reveal appropriate tunnel
4. placement. Management should now consist of
5. 1- physical therapy.
6. 2- continuous passive motion.
7. 3- open debridement.
8. 4- arthroscopic debridement.
9. 5- manipulation under anesthesia.
1. answer
1. back
1. Question 01.115
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Lindenfeld TN, Wojtys EM, Husain A: Surgical treatment of arthrofibrosis of the knee. Instr Course Lect 2000;49:211-221. Richmond JC, al Assal M: Arthroscopic management of arthrofibrosis of the knee, including infrapatellar contraction syndrome. Arthroscopy 1991;7:144-147.
1. 01.116 Which of the following radiographic findings is most helpful in differentiating
2. chordoma from chondrosarcoma of the sacrum?
3. 1- Bright signal intensity on T1-weighted MRI scan
4. 2- Lytic destruction
5. 3- Midline location
6. 4- Uptake on bone scan
7. 5- Soft-tissue extension
1. answer
1. back
1. Question 01.116
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Smith J, Ludwig RL, Marcove RC: Sacrococcygeal chordoma: A clinicoradiological study of 60 patients. Skeletal Radiol 1987: 16:37-44. Firooznia H, Pinto RS, Lin JP, Baruch HH, Zausner J: Chordoma: Radiologic evaluation of 20 cases. Am J Roentgenol 1976;127:797-805. Temple WJ: Sacral bone tumors. Can J Surg 1994;37:446.
1. 01.117 A 21-year-old student sustains a twisting injury to the ankle. Examination
2. reveals some tenderness over the anteromedial ankle and significant pain and
3. tenderness over the lateral malleolus. A stress radiograph in external rotation is
4. shown in Figure 34. Definitive treatment should consist of
5. 1- weight bearing as tolerated in a functional brace.
6. 2- a short leg cast with no weight bearing for 6 weeks.
7. 3- a long leg cast with no weight bearing for 6 weeks.
8. 4- open reduction and internal fixation of the lateral malleolus.
9. 5- open reduction and internal fixation of the lateral malleolus and repair of the deltoid
10. ligament.
1. answer
1. back
1. Figure 34
1. Question 01.117
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Principles of orthopaedic practice, in Dee R (ed): Ankle Injuries. New York, NY, McGraw Hill, 1997, pp 538-543. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 203-225.
1. 01.118 The mother of a 1-month-old infant reports that he seems to sniff and snort
2. persistently and his temperature has been very labile. Examination reveals a
3. depressed nasal bridge, mild jaundice, and hepatosplenomegaly. Radiographs
4. are shown in Figures 35a and 35b. To help confirm the diagnosis, the best
5. course of action would be to order
6. 1- a rapid plasma reagin (RPR) test.
7. 2- a technetium Tc 99m total body bone scan.
8. 3- CT of the skull and upper cervical spine.
9. 4- needle aspiration of both tibiae.
10. 5- bilateral hip ultrasound studies.
1. answer
1. back
1. A
1. B
1. Figures 35
1. Question 01.118
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 35-46. Brion LP, Manuli M, Rai B, Kresch MJ, Pavlov H, Glaser J: Long-bone radiographic abnormalities as a sign of active congenital syphilis in asymptomatic newborns. Pediatrics 1991;88:1037-1040
1. 01.119 Figure 36 shows an axial T1-weighted MRI scan at L4-5. The arrow is
2. pointing to what structure?
3. 1- Spinous process
4. 2- Herniated disk
5. 3- Epidural fat
6. 4- Ligamentum flavum
7. 5- Facet joint
1. answer
1. back
1. Question 01.119
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Author states there is no reference.
1. 01.120 What is the most severe side effect of doxorubicin (Adriamycin)?
2. 1- Neurotoxicity
3. 2- Ototoxicity
4. 3- Cardiac toxicity
5. 4- Hemorrhagic cystitis
6. 5- Pulmonary fibrosis
1. answer
1. back
1. Question 01.120
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty 1H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189. Burgert EO Jr, Nesbit ME, Garnsey LA, et al: Multimodal therapy for the management of nonpelvic, localized Ewing's sarcoma of bone: Intergroup study IESS-II J Clin Oncol 1990;8:1514-1524.
1. 01.121 Which of the following procedures is most likely to result in a hooked nail
2. deformity following fingertip amputation?
3. 1- Split-thickness skin grafting
4. 2- Reimplantation of the avulsed skin
5. 3- Local advancement flap
6. 4- Nail removal for associated nail bed repair
7. 5- Primary closure
1. answer
1. back
1. Question 01.121
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill
3. Livingstone, 1999, pp 1353-1380. Zook EG, Russell RC: Reconstruction of a functional and esthetic nail. Hand Clin 1990;6:59-68.
1. 01.122 Which of the following shoe insert (orthosis) materials has the greatest shock-
2. absorbing properties?
3. 1- Cross-linked polyethylene foam
4. 2- Rubberized cork
5. 3- Polypropylene
6. 4- Carbon epoxy resin
7. 5- Natural leather
1. answer
1. back
1. Question 01.122
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Shiba N, Kitaoka HB, Cahalan TD, Chao EY: Shock-absorbing effect of shoe insert materials commonly used in management of lower extremity disorders. Clin Orthop 1995;310:130-136. Wapner KL: Conservative treatment of the foot, in Coughlin MJ, Mann RA (eds): . Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 115-130.
1. 01.123 What type of major pelvic ring injury has the greatest average transfusion
2. requirement?
3. 1- Lateral compression
4. 2- Vertical shear
5. 3- Anteroposterior compression
6. 4- Fractures through the sacrum
7. 5- Fractures through the iliac wing
1. answer
1. back
1. Question 01.123
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Turen CH, Dube MA, LeCroy MC: Approach to the polytraumatized patient with musculoskeletal injuries. J Am Acad Orthop Surg 1999;7:154-165. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 1989;29:981-1002.
1. 01.124 Where does the nutrient artery to the tibia most commonly enter the bone?
2. 1- Anteriorly above the pes anserinus
3. 2- Anteriorly 4 cm above the ankle
4. 3- Laterally above the fibular head
5. 4- Posteriorly below the posterior cruciate ligament insertion
6. 5- Posteriorly in the medial malleolus
1. answer
1. back
1. Question 01.124
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Brinker MR, Cook SD, Dunlap IN, Christakis P, Elliott MN: Early changes in nutrient artery blood flow following tibial nailing with and without reaming: A preliminary study. J Orthop Trauma 1999;13:129-133.
1. 01.125 An 11-year-old soccer player has had left lateral ankle pain for the past 6
2. months. Examination shows increased heel valgus and decreased subtalar
3. motion on the left side. Ankle range of motion and stability are symmetric.
4. Radiographs of the foot and ankle are normal. The next most appropriate step
5. in management should consist of
6. 1- observation with follow-up in 6 months.
7. 2- a full shoe orthosis with medial heel posting left.
8. 3- left sinus tarsi injections with local anesthetic.
9. 4- comparative stress radiographs of both ankles.
10. 5- CT of the left foot.
1. answer
1. back
1. Question 01.125
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL., American Academy of Orthopaedic Surgeons, 1999, pp 583-595. Wechsler RJ, Schweitzer ME, Deely DM, Horn BD, Pizzutillo PD: Tarsal coalition: Depiction and characterization with CT and MR imaging. Radiology
3. 1994;193:447-452.
1. 01.126 What complication is significantly more common among octogenarians who
2. undergo concomitant bilateral total knee arthroplasty than those who undergo
3. unilateral total knee arthroplasty?
4. 1- Deep wound infection
5. 2- Aseptic loosening
6. 3- Periprosthetic fracture
7. 4- Congestive heart failure
8. 5- Pneumonia
1. answer
1. back
1. Question 01.126
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Lynch NM, Trousdale RT, Ilstrup DM: Complications after concomitant bilateral total knee arthroplasty in elderly patients. Mayo Clin Proc 1997;72:799-805. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
1. 01.127 A 53-year-old man has had low back pain
2. and perineal fullness for the past 18
3. months. A plain radiograph is shown in
4. Figure 37a, a CT scan is shown in Figure
5. 37b, and a biopsy specimen is shown in
6. Figure 37c. What is the most likely
7. diagnosis?
8. 1- Chordoma
9. 2- Plasmacytoma
10. 3- Fibrosarcoma
11. 4- Liposarcoma
12. 5- Metastatic carcinoma
1. answer
1. back
1. A
1. B
1. Figures 37
1. C
1. Question 01.127
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276. Bruckner 1D, Conrad EU: Spine, in Simon MA. Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 435-450.
1. 01.128 What is the most common soft-tissue tumor in children?
2. 1- Ganglion
3. 2- Hemangioma
4. 3- Fibroma
5. 4- Lipoma
6. 5- Sarcoma
1. answer
1. back
1. Question 01.128
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Conrad EU, Enneking WR: Clinical Symposium: Common Soft Tissue Tumors, ed 2. New York, NY, Ciba-Geigy, 1990.
1. 01.129 Which of the following is considered the most important factor in fracture
2. healing in adults?
3. 1- Age of the patient
4. 2- Gender of the patient
5. 3- Neurologic status of the extremity
6. 4- Blood supply
7. 5- Fracture pattern
1. answer
1. back
1. Question 01.129
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.130 A 67-year-old woman reports progressively worsening buttock pain.
2. Examination reveals a mass affixed to the region of the posterior ilium. Figures
3. 38a through 38d show a plain radiograph, a posterior view bone scan, a CT
4. scan, and a biopsy specimen. What is the most likely diagnosis?
5. 1- Dedifferentiated chondrosarcoma
6. 2- Malignant fibrous histiocytoma
7. 3- Fibrosarcoma
8. 4- Pagetoid osteosarcoma
9. 5- Osteomyelitis
1. back
1. A
1. B
1. Figures 38
1. Go to next slide for remaining
2. figures and
3. answer link
1. Figures 38
1. D
1. C
1. answer
1. back to question
1. Question 01.130
1. Question 01.130
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802. Harrington KD: Surgical management of neoplastic complications of Paget's disease. J Bone Miner Res 1999;2:45-48.
1. 01.131 A 23-year-old woman has had chronic swelling in the ankle for the past year
2. with no history of injury. Plain radiographs are normal. At ankle arthroscopy,
3. the articular surfaces appear normal. The synovial tissue is inflamed and friable;
4. a biopsy specimen of the synovium is shown in Figure 39. What is the most
5. likely diagnosis?
6. 1- Tuberculosis
7. 2- Synovial cell sarcoma
8. 3- Pigmented villonodular synovitis
9. 4- Rheumatoid arthritis
10. 5- Chondrocalcinosis
1. answer
1. back
1. Figure 39
1. Question 01.131
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Rao AS, Vigorita VJ: Pigmented villonodular synovitis (giant-cell tumor of the tendon sheath and synovial membrane): A review of eighty-one cases. J Bone Joint Surg Am 1984;66:76-94.
1. 01.132 Figure 40 shows the radiograph of a 24-year-old woman who has ulnar-sided
2. wrist pain. Nonsurgical management consisting of splinting, physical therapy,
3. and activity modifications has failed to provide relief. Examination reveals a
4. stable distal radioulnar joint and a negative triangular fibrocartilage complex
5. grind. Pain is reproduced when the wrist is dorsiflexed and the forearm is then
6. supinated but not when the forearm is
7. pronated. Treatment should now consist of
8. 1- partial ulnar styloidectomy.
9. 2- triangular fibrocartilage complex rim repair.
10. 3- debridement of the extensor carpi ulnaris tendon
11. sheath.
12. 4- a radial lengthening osteotomy.
13. 5- an ulnar shortening osteotomy.
1. answer
1. back
1. Figure 40
1. Question 01.132
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Topper SM, Wood MB, Ruby LK: Ulnar styloid impaction syndrome. J Hand Surg Am 19972:699-704. Topper SM, Wood MB, Ruby LK Ulnar styloid impaction syndrome, in Sulfar P, Amadio PC, Foucher G (eds): Current Practice in Hand Surgery. London, England, Martin Dunitz, 1997, pp 261-268.
1. 01.133 A patient with diabetes mellitus has an ulcer on the plantar aspect of the foot.
2. Which of these test results best correlates with the patient's ability to heal this
3. ulcer?
4. 1- Toe pressures of greater than 45 mm Hg
5. 2- An arterial brachial index of 0.40
6. 3- Capillary refill time in the toes of greater than 3 seconds
7. 4- Ability to detect greater than a 5.07 Semmes -Weinstein monofilament
8. 5- A hemoglobin A3 level of greater than 4%
1. answer
1. back
1. Question 01.133
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121. Brodsky JW: The diabetic foot. in Coughlin MJ. Mann RA (eds)- Surgery of the root and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 895-969.
1. 01.134 A 42-year-old woman who has had a low-grade aching pain in her forearm for
2. the past 4 years recently fell on the arm and now reports markedly increased
3. pain. A plain radiograph and biopsy specimen are shown in Figures 41a and
4. 41b. What is the most likely diagnosis?
5. 1- Chondroblastoma
6. 2- Chondrosarcoma
7. 3- Chondromyxoid fibroma
8. 4- Adamantinoma
9. 5- Enchondroma
1. answer
1. back
1. A
1. Figures 41
1. B
1. Question 01.134
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Weis L: Common malignant bone tumors: Chondrosarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 275-286. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276.
1. 01.135 To prevent abnormal patellofemoral contact loading after insertion of a
2. retrograde femoral nail through an intra-articular starting portal, the surgeon
3. should
4. 1- seat the nail beneath the articular surface.
5. 2- use a patellar tendon-splitting approach.
6. 3- use an unreamed technique.
7. 4- perform a lateral release.
8. 5- perform a medial parapatellar arthrotomy.
1. answer
1. back
1. Question 01.135
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Moed B, Watson JT: Retrograde nailing of the femoral shaft. J Am Acad Orthop Surg 1999;7:209-216. Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
1. 01.136 A woman who is in the 20th week of her pregnancy seeks an orthopaedic
2. consultation after undergoing an ultrasound. The findings reveal that the fetus
3. has bilateral clubfeet and both femurs measure less than two standard
4. deviations below normal. What is the most likely diagnosis?
5. 1- Myelomeningocele
6. 2- Bilateral proximal focal femoral deficiency
7. 3- Diastrophic dysplasia
8. 4- Achondroplasia
9. 5- Spondylometaphyseal dysplasia
1. answer
1. back
1. Question 01.136
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Horton WA, Hall JG, Scott CI, Pyeritz RE, Rimoin DL: Growth curves for height for diastrophic dysplasia, spondyloepiphyseal dysplasia congenita, and pseudoachondroplasia. Am J Dis Child 1982;136:316-319. Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-44.4.
1. 01.137 A 47-year old woman has right groin pain. An AP radiograph of the pelvis and
2. a biopsy specimen are shown in Figures 42a and 42b. What is the most likely
3. diagnosis?
4. 1- Ollier's disease
5. 2- Paget's disease
6. 3- Metastatic carcinoma
7. 4- Aneurysmal bone cyst
8. 5- Fibrous dysplasia
1. answer
1. back
1. A
1. B
1. Figures 42
1. Question 01.137
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276. Gitelis S, McDonald DJ: Common benign bone tumors and usual treatment, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 275-286.
1. 01.138 Acute hypotension, hypoxemia, cardiac arrest, and sudden death are events that
2. are most commonly encountered in what stage of total hip arthroplasty?
3. 1- Exposure
4. 2- Acetabular reaming
5. 3- Broaching the femur
6. 4- Impaction of the acetabular component
7. 5- Cementing of the femoral component
1. answer
1. back
1. Question 01.138
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasry: A
3. prospective, randomized clinical trial. J Bone Joint Surg Am 1999;81:831-843.
1. 01.139 A 35-year-old woman falls on the ice and sustains an isolated minimally
2. displaced radial head fracture. Management should include
3. 1- use of a posterior splint and sling at all times for 6 weeks.
4. 2- use of a sling until radiologic union is achieved.
5. 3- application of a cast in 7 to 10 days.
6. 4- application of a hinged elbow orthosis in 3 weeks.
7. 5- a program of active range of motion in 1 week.
1. answer
1. back
1. Question 01.139
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Morrey BF: Radial head fractures, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WE Saunders, 1985, pp 355-381. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 47-55.
1. 01.140 An asymptomatic 10-year-old boy is referred for evaluation of a limb-length
2. discrepancy that measures less than 2 cm. Examination reveals that the most
3. lateral ray of the ipsilateral foot is absent, and the ipsilateral knee is unstable to
4. Lachman and anterior drawer tests. Figure 43 shows an AP radiograph of the
5. ankle. Management of the knee should consist of
6. 1- anterior cruciate ligament reconstruction using a
7. quadruple hamstring technique.
8. 2- anterior cruciate ligament reconstruction using an
9. allograft in the over-the-top position.
10. 3- observation.
11. 4- an aggressive physical therapy program that
12. emphasizes open chain techniques.
13. 5- functional knee bracing until skeletal maturity,
14. followed by anterior cruciate ligament reconstruction.
1. answer
1. back
1. Figure 43
1. Question 01.140
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Achterman C, Kalamchi A: Congenital deficiency of the fibula. J Bone Joint Surg Br 1979;61:133-137. Roux MO, Cariioz H: Clinical examination and investigation of the cruciate ligaments in children with fibular hemimelia. J Pediatr Orthop 1999;19:247-251. Stevens PM, Arms D: Postaxial hypoplasia of the lower extremity. J Pediatr Orthop 2000;20:166-172.
1. 01.141 A nonrandomized prospective study of the efficacy of a new diagnostic test to
2. detect deep venous thrombosis has just been completed. Each patient had
3. venography as the definitive test to detect the thrombosis. Of the 100 patients
4. tested, 10 were true positives, 30 were false negatives, 40 were true negatives,
5. and 20 were false positives. What is the sensitivity of the new test?
6. 1- 25 %
7. 2- 30%
8. 3- 50 %
9. 4- 59%
10. 5- 67 %
1. answer
1. back
1. Question 01.141
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 2000, pp 308-316.
1. 01.142 When treating tibial plateau fractures, the most important reason that proximal
2. tibial transfixation wires should be placed at least 14 mm from the articular
3. surface is to
4. 1- obtain good fixation in subchondral bone.
5. 2- allow radiographic visualization of the joint reduction.
6. 3- minimize the risk that septic arthritis will develop.
7. 4- increase the range of knee flexion.
8. 5- compress the articular fragments.
1. answer
1. back
1. Question 01.142
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. DeCoster TA, Crawford M.K, Kraut VIA: Safe extracapsular placement of proximal tibia transfixation pins. J Orthop Trauma 1999;13:236-240. Reid JS, Van Slyke MA, Moulton MJ, Mann TA: Safe placement of proximal tibial transfixation wires with respect to intracapsular penetration. J Orthop Trauma 2001;15:10-17.
1. 01.143 A 17-year-old girl reports a 4-month history of progressively worsening left
2. arm pain. A plain radiograph and biopsy specimen are shown in Figures 44a
3. and 44b. After complete staging, management should consist of
4. 1- forequarter amputation alone.
5. 2- radiation therapy and chemotherapy.
6. 3- radiation therapy and wide surgical excision.
7. 4- chemotherapy and wide surgical excision.
8. 5- wide surgical excision alone.
1. answer
1. back
1. A
1. B
1. Figures 44
1. Question 01.143
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia., PA.
3. WB Saunders, 1998, pp 195-276. Weis L: Common malignant bone tumors: Osteosarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274. Goorin A: Chemotherapy for osteosarcoma and Ewing's sarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA,
4. Lippincott-Raven, 1998, pp 239-244.
1. 01.144 Figure 45 shows the initial clinical photograph of a 70-year-old woman. The
2. deformity of the second toe may recur after attempted surgical reconstruction.
3. Dysfunction of what structure allows for recurrence?
4. 1- Dorsal capsule
5. 2- Plantar plate
6. 3- Medial collateral ligament
7. 4- Lateral collateral ligament
8. 5- Transverse intermetatarsal ligament
1. answer
1. back
1. Figure 45
1. Question 01.144
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Yao L, Cracchiolo A, Farahani K, Seeger LL: Magnetic resonance imaging of plantar plate rupture. Foot Ankle Int 1996;17:33-36. Deland JT, Sung IH: The medial crossover toe: A cadaveric dissection. Foot Ankle Int 2000;21:375-378.
1. 01.145 A 25-year-old rugby player who sustained blunt trauma to the right dominant
2. long finger 2 days ago now reports pain over the dorsum of the digit and
3. clicking when he flexes and extends the digit. Examination reveals swelling
4. and ecchymosis over the metacarpophalangeal joint, as well as a palpable
5. subluxation of the extrinsic extensor tendon over the metacarpophalangeal
6. joint with joint flexion and extension. Management should consist of
7. 1- surgical repair of the sagittal band.
8. 2- surgical repair of the spiral oblique retinacular ligament.
9. 3- surgical repair of the triangular ligament.
10. 4- splinting the metacarpophalangeal joint at 70° of flexion.
11. 5- a program of early active motion with buddy taping.
1. answer
1. back
1. Question 01.145
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Ishizuki M: Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg Am 1990;15:967-972. Rayan GM, Murray D: Classification and treatment of closed sagittal band injuries. J Hand Surg Am 1994;19:590-594.
1. 01.146 When placing lateral mass screws in the midcervical spine, where is the
2. vertebral artery located in relation to the starting point for screw insertion?
3. 1- Medial
4. 2- Lateral
5. 3- Anterior
6. 4- Posterior
7. 5- Superior
1. answer
1. back
1. Question 01.146
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Levine AM: Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 335-339.
1. 01.147 A 30-year-old man underwent an arthroscopic Bankart repair with suture
2. anchors 6 months ago. While the patient reports that the shoulder is stable, he
3. notes anterior shoulder pain and crepitation. Figure 46 shows an arthroscopic
4. view of the anterior shoulder joint. The next most appropriate step in
5. management should consist of
6. 1- an intra-articular culture.
7. 2- rotator cuff repair.
8. 3- removal of the anchors.
9. 4- arthroscopic releases.
10. 5- exchange of the metallic
11. anchor for a bioabsorbable
12. device.
1. answer
1. back
1. Figure 46
1. Question 01.147
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Kaar TY, Schenck RC Jr, Worth MA, Rockwood CA Jr.- Complications of metallic suture anchors in shoulder surgery: A report of 8 cases. Arthroscopy 2001;17:31-37. Zuckerman JD, Matsen FA III: Complications about the glenohumeral joint related to the use of screws and staples. J Bone Joint Surg Am 1984;66:175-180
1. 01.148 A 32-year-old man notes a lump on the side of his neck and undergoes a lymph
2. node biopsy. Following the procedure, the patient reports pain in the shoulder
3. girdle and is unable to elevate his shoulder. Which of the following structures
4. has most likely been injured?
5. 1- Trapezius muscle
6. 2- Sternocleidomastoid muscle
7. 3- Axillary nerve
8. 4- Cranial nerve XI
9. 5- Suprascapular nerve
1. answer
1. back
1. Question 01.148
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Leffert RD: Neurologic problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, p 759. Bigliani LU, Perez-Sanz JR, Wolfe IN: Treatment of trapezius paralysis. J Bone Joint Surg Am 1985;67:871-877.
1. 01.149 A 40-year-old woman with steroid-dependent Crohn's disease has had pain and swelling
2. of the left ankle for the past 5 days. She has a plugged central line for parenteral feeding.
3. Examination of the ankle reveals focal inflammation and limited range of motion. She is
4. sensitive to the 4.17 Semmes-Weinstein monofilament test. Radiographs are shown in
5. Figures 47a and 47b. The next most appropriate step in management should consist of
6. 1- a biopsy of the talus.
7. 2- a bone scan.
8. 3- aspiration and culture of the ankle.
9. 4- no weight bearing and a total contact cast for 1 week.
10. 5- a brace with calipers.
1. answer
1. back
1. A
1. B
1. Figures 47
1. Question 01.149
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mielants H, Veys EM: The gut in the pondyloarthropathies. J Rheumatol 1990;17:7-10. Myerson M: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1215-1216.
1. 01.150 What structures are located within the femoral canal as it passes beneath the
2. inguinal ligament?
3. 1- Femoral artery, femoral vein, and femoral nerve
4. 2- Femoral artery and femoral vein
5. 3- Femoral artery, femoral vein, and lymphatics
6. 4- Femoral artery, femoral vein, femoral nerve, and lymphatics
7. 5- Internal iliac artery, internal iliac vein, and femoral nerve
1. answer
1. back
1. Question 01.150
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. ed 2. Philadelphia. PA. JB Lippincott, 1994. pp 362-275.
1. 01.151 A 6-month-old boy with L1 myelomeningocele has bilateral dislocated hips.
2. Examination reveals that the hips are clinically reducible, and there are no
3. significant hip or knee joint contractures. The best course of action for both
4. hips should consist of
5. 1- observation.
6. 2- application of a Pavlik harness.
7. 3- application of a rigid hip abduction orthosis.
8. 4- closed reduction with a hip spica cast.
9. 5- open reduction via an adductor approach.
1. answer
1. back
1. Question 01.151
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spins bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436. Broughton NS, Menelaus MB, Cole WG, Shurtleff DB: The natural history of hip deformity in myelomeningocele. J Bone Joint Surg Br 1993;75:760-763.
1. 01.152 Sterilization of ultra-high molecular-weight polyethylene by irradiation in an
2. inert environment (argon, nitrogen, or vacuum) is recommended because it
3. 1- increases crystallinity.
4. 2- prevents free radical formation.
5. 3- prevents immediate oxidative degradation.
6. 4- prevents component shrinkage.
7. 5- provides better sterility.
1. answer
1. back
1. Question 01.152
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53. Deng M, Shalaby SW: Lang-term gamma irradiation effects on ultrahigh molecular weight polyethylene. J Biomed Mater Res 2001;54:428-435.
1. 01.153 A 13-year-old girl reports activity-related pain in her left leg with no history of
2. trauma. Figures 48a through 48d show a plain radiograph, T1- and T2-weighted
3. MRI scans, and a biopsy specimen. What is the most likely diagnosis?
4. 1- Ewing's sarcoma
5. 2- Osteomyelitis
6. 3- Fibrous dysplasia
7. 4- Adamantinoma
8. 5- Tibial stress fracture
1. back
1. A
1. B
1. Figures 48
1. Go to next slide for remaining figures and answer link
1. Figures 48
1. D
1. C
1. answer
1. back to question
1. Question 01.153
1. Question 01.153
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Jeske JM, Lomasney LM, Demos TC, Vade A, Bielski RJ: Longitudinal tibial stress fracture. Orthopedics 1996;19:263,66,68,70. Shearman CM, Brandser EA, Parman LM, et al: Longitudinal tibial stress fractures: A report of eight cases and review of the literature. J Comput Assist Tomogr 1998;22:265-269.
1. 01.154 A 30-year-old woman who underwent total hip arthroplasty for osteonecrosis 6
2. months ago is now seeking a second opinion for her limp. What is the most
3. significant radiographic finding shown in Figure 49?
4. 1- Contralateral osteonecrosis
5. 2- Prosthetic loosening
6. 3- Heterotopic ossification
7. 4- Stress shielding
8. 5- Limb-length inequality
1. answer
1. back
1. Figure 49
1. Question 01.154
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Woolson ST: Leg length equalization during total hip replacement. Orthopedics 1990;13:17-21. Shaw JA, Greet RB III: Complications of total hip replacement, in Epps CH Jr (ed): Complication in Orthopaedic Surgery. Philadelphia, PA, JB Lippincott,
3. 1994, pp 1013-1056.
1. 01.155 Figure 50 shows the radiograph of a 24-year-old patient who has a slightly painful swollen distal finger. What is the most likely diagnosis?
2. 1- Glomus tumor
3. 2- Giant cell tumor
4. 3- Intraosseous ganglion
5. 4- Foreign body granuloma
6. 5- Inclusion cyst
1. answer
1. back
1. Question 01.155
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Schajowicz F, Aiello CL, Slullitel I: Cystic and pseudocystic lesions of the terminal phalanx with special reference to epidermoid cysts. Clip Orthop 1970;68:84-92. Athanasian EA: Bone and soft-tissue tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2223-2253.
1. 01.156 A 4-year-old boy has a painful spinal deformity. Figures 51a through 51d show
2. a lateral spine radiograph, whole body bone scan, a lateral T1-weighted MRI
3. scan, and a needle biopsy specimen. What is the most likely diagnosis?
4. 1- Tuberculosis
5. 2- Metastatic neuroblastoma
6. 3- Chordoma
7. 4- Diskitis
8. 5- Ewing's sarcoma
1. back
1. A
1. B
1. Figures 51
1. Go to next slide
2. for remaining
3. figures and
4. answer link
1. Figures 51
1. D
1. C
1. answer
1. back to question
1. Question 01.156
1. Question 01.156
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Mushkin AY, Kovalenko KN: Neurological complications of spinal tuberculosis in children. Int Orthop 1999;23:210-212. Sudarshan K: Tuberculosis of bones and joints. J Bone Joint Surg Am 1997;79:1891.
1. 01.157 A 19-year-old man sustained a fracture-dislocation of the ankle and a talar neck
2. and body fracture when his foot was run over by a truck. Examination reveals
3. no pulse in the ankle and an ischemic foot. The anterior and posterior tibial
4. arteries are transected. He has no other injuries. A clinical photograph is shown
5. in Figure 52. Treatment should consist of
6. 1- repair of the posterior tibial artery and ankle fusion.
7. 2- repair of the anterior tibial artery and pantalar fusion.
8. 3- repair of both tibial arteries and internal fixation of the talus.
9. 4- repair of the posterior tibial artery and nerve and external fixation.
10. 5- amputation.
1. answer
1. back
1. Figure 52
1. Question 01.157
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Gregory P, Sanders R: The management of severe fractures of the lower extremities. Clip Orthop 1995;318:95-105.
3. Tornetta P III, Olson SA (eds): Amputation versus limb salvage. Instr Course Lect 1997;46:511-518.
1. 01.158 In an animal model, the use of anabolic steroids on muscle contusion injury has
2. been shown to
3. 1- be similar to placebo controls.
4. 2- be similar to corticosteroids with respect to muscle strength recovery in the long
5. term.
6. 3- be more effective than corticosteroids with respect to muscle strength recovery in the
7. long term.
8. 4- be less effective than corticosteroids with respect to muscle strength recovery in the
9. long term.
10. 5- result in severely disorganized muscle fiber architecture.
1. answer
1. back
1. Question 01.158
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beiner JM, Jokl P, Cholewicki J, Panjabi MM: The effect of anabolic steroids and corticosteroids on healing of muscle contusion injury. Am J Sports Med 1999;27:2-9. Tingus SJ, Carlsen RC: Effect of continuous infusion of an anabolic steroid on marine skeletal muscle. Med Sci Sports Exert 1993;25:485-494.
1. 01.159 When performing a surgical debridement for a painful irreparable rotator cuff
2. tear, it is important to
3. 1- tenodese the biceps.
4. 2- excise the distal clavicle (Mumford procedure).
5. 3- preserve the coracohumeral ligament.
6. 4- preserve the coracoacromial ligament.
7. 5- advance the deltoid origin.
1. answer
1. back
1. Question 01.159
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Ellman H, Hanker G, Bayer M: Repair of the rotator cuff: End-result study of factors influencing reconstruction. J Bone Joint Surg Am 1986;68:1136-1144. Hanyman DT II, Mack LA. Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of
3. the cuff. J Bone Joint Surg Am 1991;73:982-989.
1. 01.160 A patient with developmental dysplasia of the hip is undergoing open
2. reduction. Which of the following is considered an advantage of using a medial
3. approach compared with an anterior approach?
4. 1- A lower incidence of osteonecrosis
5. 2- Access for performance of capsulorrhaphy
6. 3- Access to the transverse acetabular ligament
7. 4- Better ability to reduce an inverted labrum
8. 5- Better visualization of the lateral femoral cutaneous nerve
1. answer
1. back
1. Question 01.160
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Turner Y, Ward WT, Grudziak J: Medial open reduction in the treatment of developmental dislocation of the hip. J Pediatr Orthop 1997;17:176-180. Mankey MG, Arntz GT, Staheli LT: Open reduction through a medial approach for congenital dislocation of the hip: A critical review of the Ludloff approach in sixty-six hips. J Bone Joint Surg Am 1993;75:1334-1345.
1. 01.161 A 35-year-old laborer sustains a irreparable fracture of the radial head after
2. falling 12 feet. Examination reveals tenderness at the elbow and wrist and pain
3. with manipulation of the distal radioulnar joint. In addition to resection of the
4. radial head, management should include
5. 1- hinged bracing of the elbow.
6. 2- immobilization in a long arm cast.
7. 3- prosthetic replacement of the radial head.
8. 4- repair of the distal radioulnar joint.
9. 5- application of a hinged external fixator.
1. answer
1. back
1. Question 01.161
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL,, American Academy of Orthopaedic Surgeons, 2000, pp 39-51. Hotchkiss RN: An KN, Sowa DT, Banta S, Weiland AJ: An anatomic and mechanical study of the interosseous membrane of the forearm: Pathomechanics of proximal migration of the radius. J Hand Surg Am 1989;14:256-261.
1. 01.162 Which of the following treatments has been shown to prevent the formation of
2. heterotopic ossification after total hip arthroplasty in patients who are at high
3. risk?
4. 1- Alendronate
5. 2- Acetaminophen
6. 3- Preoperative radiation
7. 4- Calcitonin
8. 5- Parathormone
1. answer
1. back
1. Question 01.162
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Knelles D, Barthel T, Karrer A, Kraus U, Eulert J, Kolbl O: Prevention of heterotopic ossification after total hip replacement: A prospective, randomised study using acetylsalicylic acid, indomethacin and fractional or single-dose, irradiation. J Bone Joint Surg Br 1997;79:596-602. Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Sung Am 1996;78:870-881.
1. 01.163 A 38-year-old landscaper was treated with internal and external fixation for a
2. severe pilon fracture. Radiographs obtained at 3 months and 1 year are shown
3. in Figures 53a and 53b. He now reports increasing pain over the past 4 months
4. and is unable to walk uphill or stand for more than 2 hours. Examination
5. reveals range of motion from neutral to 5° of plantar flexion. Use of a short leg
6. brace with a rocker bottom sole after screw removal provides some pain relief,
7. but he still has too much pain to work. Management should now consist of
8. 1- manipulation of the ankle under anesthesia.
9. 2- arthroscopic debridement of the ankle.
10. 3- ankle arthroplasty.
11. 4- ankle fusion.
12. 5- subtalar fusion.
1. answer
1. back
1. A
1. B
1. Figures 53
1. Question 01.163
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 191-202.
1. 01.164 Which of the following factors best predicts the increased risk for development
2. of a foot ulcer in a patient with diabetes mellitus?
3. 1- A history of a previous foot ulcer
4. 2- A history of poor blood glucose control
5. 3- Type I diabetes for more than 10 years
6. 4- Ability to detect a 5.07 Semmes-Weinstein monofilament, on the plantar surface of
7. the foot
8. 5- Nonpalpable pulses with an ankle-brachial index (ABI) of greater than 0.5
1. answer
1. back
1. Question 01.164
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. McDermott JE (ed): The Diabetic Foot. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 1-12. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 113-12I. Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 895-969.
1. 01.165 A study is being designed to compare the results of two new drugs on bone
2. mineral density. The number of subjects needed for this study should be
3. determined by
4. 1- Student's t test.
5. 2- power analysis.
6. 3- probability distribution.
7. 4- regression analysis.
8. 5- Spearman rank correlation.
1. answer
1. back
1. Question 01.165
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 2-17.
1. 01.166 A 17-year-old basketball player sustains an ankle eversion injury on a fast
2. break. She notes immediate anteromedial ankle pain and swelling and is unable
3. to bear weight. The next most appropriate step in management should consist
4. of
5. 1- ice and protected weight bearing.
6. 2- functional ankle bracing treatment.
7. 3- a short leg cast.
8. 4- radiographs.
9. 5- MRI.
1. answer
1. back
1. Question 01.166
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Roberts CS, DeMaio M, Larkin JJ, Paine R: Eversion ankle sprains. Orthopedics 1995;18:299-304. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons 1999, pp 597-612.
1. 01.167 Following reinsertion of the distal biceps tendon, early rehabilitation should
2. include
3. 1- active elbow flexion and active forearm supination.
4. 2- active elbow flexion and passive forearm supination.
5. 3- active elbow extension and active forearm supination.
6. 4- passive elbow extension and active forearm supination.
7. 5- passive elbow flexion and passive forearm supination.
1. answer
1. back
1. Question 01.167
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Money BF: Tendon injuries about the elbow, in Moray BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Sounders, 1993, pp 492-504. Sotereanos DG, Pierce TD, Varitimidis SE: A simplified method for repair of distal biceps tendon ruptures. J Shoulder Elbow Sung 2000;9:227-233.
1. 01.168 In the absence of a visible fracture on radiographs, the presence of a positive
2. posterior fat pad sign following trauma of the elbow in a 5-year-old child most
3. likely represents
4. 1- a normal radiographic finding.
5. 2- a soft-tissue contusion.
6. 3- nursemaid's elbow.
7. 4- an occult fracture.
8. 5- synovial hypertrophy.
1. answer
1. back
1. Question 01.168
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Sung Am 1999;81:1429-1433. Donnelly LF, Klostermeier TT, Klosterman LA: Traumatic elbow effusions in pediatric patients: Are occult fractures the rule? Am J Roentgenol 1998;171:243-245.
1. 01.169 Thumb adduction in low ulnar nerve palsy is provided by the
2. 1- extensor pollicis longus.
3. 2- extensor pollicis brevis.
4. 3- flexor pollicis brevis.
5. 4- first dorsal interosseous.
6. 5- accessory head of the flexor pollicis longus (Gantzer's muscle).
1. answer
1. back
1. Question 01.169
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Smith RJ: Tendon Transfers of the Hand and Forearm. Boston, MA, Little Brown, 1987, pp 85-102. Hamlin C, Littler JW: Restoration of power pinch. J Hand Surg Am 1980;5:396-401.
1. 01.170 The parents of a 6-month-old infant report that she has been unwilling to move
2. her left upper extremity for the past 5 hours. An AP radiograph and an MRI
3. scan are shown in Figures 54a and 54b. Based on these findings and after
4. initial treatment, a consultation should be arranged with
5. 1- child protection services.
6. 2- a geneticist.
7. 3- a nephrologist.
8. 4- a rheumatologist.
9. 5- an infectious disease
10. specialist.
1. answer
1. back
1. A
1. B
1. Figures 54
1. Question 01.170
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. DeLee JC, Wilkins KE, Rogers LF, Rockwood CA: Fracture-separation of the distal humeral epiphysis. J Bone Joint Surg Am 1980;62:46-51. Cramer KE, Green NE: Child abuse, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Sounders, 1998, pp 577-594. Nimkin K, Kleinman PK. Teeger S, Spevak MR: Distal humeral physeal injuries in child abuse: MR imaging and ultrasonography findings. Pediatr Radiol 1995;25:562-565. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
1. 01.171 Where are the sacral roots located within the canal at the L1-2 disk level?
2. 1- Random pattern
3. 2- Anterior
4. 3- Central
5. 4- Lateral
6. 5- Posterior
1. answer
1. back
1. Question 01.171
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Wall E1, Cohen MS, Abitbol JJ, Garfin SR: Organization of intrathecal nerve roots at the level of the conus medullaris. J Bone Joint Surg Am 1990;72:1495-1499. Wall FJ, Cohen MS, Massie JB, Rydevik B, Garfin SR: Cauda equina anatomy: L Intrathecal nerve root organization. Spine 1990;15:1244-1247.
1. 01.172 University of California Biomechanics Laboratory (UCBL) lower extremity
2. orthoses are thought to work by
3. 1- supporting the forefoot in rigid deformities.
4. 2- supporting the midfoot in rigid deformities.
5. 3- controlling the hindfoot in flexible deformities.
6. 4- controlling the ankle when instability is present.
7. 5- accommodating a forefoot deformity.
1. answer
1. back
1. Question 01.172
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64. Wapner KL: Conservative treatment of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 115-130.
1. 01.173 What portion of the calcaneus typically maintains a normal relationship to the
2. talus in displaced intra-articular calcaneus fractures?
3. 1- Sustentaculum tali
4. 2- Tuberosity
5. 3- Anterolateral
6. 4- Posterior facet
7. 5- Lateral wall
1. answer
1. back
1. Question 01.173
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Olexa TA, Ebraheim NA, Haman SP: The sustentaculum tall: Anatomic, radiographic, and surgical considerations. Foot Ankle Int 2000;21:400-403. Sanders R: Intro articular fractures of the calcaneus: Present state of the art. J Orthop Trauma 1992;6:252-265.
1. 01.174 The linear relationship between an applied stress and the resultant deformation
2. defines a material's
3. 1- modulus of elasticity.
4. 2- brittleness.
5. 3- yield strength.
6. 4- ultimate strength.
7. 5- toughness.
1. answer
1. back
1. Question 01.174
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 447-486.
1. 01.175 In total hip arthroplasty, which of the following characterizes the clinical pain
2. pattern seen with a loose femoral component?
3. 1- Gluteal
4. 2- Night
5. 3- Start-up
6. 4- Back
7. 5- At rest
1. answer
1. back
1. Question 01.175
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Katz RP, Callaghan JJ, Sullivan PM, Johnston RC: Long-term results of revision total hip arthroplasty with improved cementing technique. J Bone Joint Sung Br 1997;79:322-326. Krishnamurthy AB, MacDonald SJ, Paprosky WG: 5- to 13-year follow-up study on cementless femoral components in revision surgery. J Arthroplasty 1997;12:839-847.
1. 01.176 What is the natural history of a nonossifying fibroma?
2. 1- Gradual enlargement after skeletal maturity
3. 2- Spontaneous resolution with skeletal maturity
4. 3- Chronic pain
5. 4- Late malignant degeneration
6. 5- Angular deformity
1. answer
1. back
1. Question 01.176
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Jaffe HL, Lichtenstein L: Non-osteogenic fibroma of bane. Am J Pathol 1942;18:205. Unni KK: Conditions that commonly simulate primary neoplasms of bone, in Dahlin's Bone Tumors, ed 5. Philadelphia, PA, 1996, pp 355-432.
1. 01.177 What structure is outlined and lies at the tip of the arrow shown in Figure 55?
2. 1- Inferior articular facet
3. 2- Superior articular facet
4. 3- Pedicle
5. 4- Lamina
6. 5- Spinous process
1. answer
1. back
1. Figure 55
1. Question 01.177
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Parke WW: Applied Anatomy of the Spine, in Herkowitz HN, Eismont FJ, Garfin SR, Bell GR, Balderston RA, Wiesel SW (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 27-73. Netter FH (ed): The Ciba Collection of Medical Illustrations: Musculoskeletal System, Part L Anatomy, Physiology, and Metabolic Disorders. Summit, NJ,
3. Ciba-Geigy, 1987, vol 8, pp 9-19.
1. 01.178 Which of the following systemic conditions is associated with a genetic defect
2. in skeletal formation that does not involve abnormal collagen?
3. 1- Osteogenesis imperfecta
4. 2- Spondyloepiphyseal dysplasia congenita
5. 3- Achondroplasia
6. 4- Multiple epiphyseal dysplasia
7. 5- Kneist dysplasia
1. answer
1. back
1. Question 01.178
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Dietz FR, Matthews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Bone Joint Surg Am 1996;78:1583-1598.
1. 01.179 What is the most likely cause of mortality within the first 48 hours in patients
2. who sustain a pelvic fracture from a lateral compression mechanism?
3. 1- Aortic rupture
4. 2- Pelvic arterial injury
5. 3- Pelvic venous injury
6. 4- Hollow viscous injury
7. 5- Head injury
1. answer
1. back
1. Question 01.179
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Dalal SA, Burgess AR, Siegel 3H, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 1989;29;981-1002.
1. 01.180 Following total hip arthroplasty, examination of the patient reveals an ischemic
2. leg. A radiograph obtained in the recovery room is shown in Figure 56a, and a
3. subtraction arteriogram is shown in Figure 56b. What artery has been injured?
4. 1- Profunda femoris
5. 2- External iliac
6. 3- Obturator
7. 4- Superior gluteal
8. 5- Inferior gluteal
1. answer
1. back
1. A
1. B
1. Figures 56
1. Question 01.180
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Wasielewski RC, Cooperstein LA, Kruger MP, Rubash HE: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508. Shaw JA, Greer RB III: Complications of total hip replacement, in Epps CH Jr (ed): Complication in Orthopaedic Surgery. Philadelphia, PA, JB Lippincott,
3. 1994, pp 1013-1056.
1. 01.181 Which of the following axial pattern flaps is best used to repair fingertip
2. amputations?
3. 1- Axial flag
4. 2- First dorsal metacarpal artery
5. 3- Second dorsal metacarpal artery
6. 4- Reversed dorsal metacarpal artery
7. 5- Digital artery island
1. answer
1. back
1. Question 01.181
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Lai CS, Lin SD, Yang CC: The reverse digital artery flap for fingertip reconstruction. Ann Plant Surg 1989;22:495-500. Lister GD, Pederson WC: Skin flaps, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1783-1850.
1. 01.182 What is the most common complication seen in patients undergoing surgery on
2. the Achilles tendon for chronic refractory tendinitis?
3. 1- Deep vein thrombosis
4. 2- Partial/complete tendon rupture
5. 3- Skin edge necrosis
6. 4- Infection
7. 5- Complex regional pain syndrome
1. answer
1. back
1. Question 01.182
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Paavola M, Orava S, Leppilahti J, Kannus P, Jarvinen M: Chronic Achilles tendon overuse injury: Complications after surgical treatment: An analysis of 432 consecutive patients. Am J Sports Med 2000;28:77-82. Williams J: Achilles tendon lesions in sport. Sports Med 1986;3:114-135.
1. 01.183 Figures 57a and 57b show the radiographs of a college basketball player who
2. has had lateral foot pain for the past 3 weeks. Management should consist of
3. 1- weight bearing as tolerated with continued play.
4. 2- weight bearing as tolerated in a short leg cast.
5. 3- restricted weight bearing for 4 weeks, followed by an early return to play.
6. 4- electrical bone stimulation.
7. 5- percutaneous screw fixation.
1. answer
1. back
1. A
1. B
1. Figures 57
1. Question 01.183
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mindrebo N, Shelboume KD, Van Meter CD, Rettig AC: Outpatient percutaneous screw fixation of the acute Jones fracture. Am J Sports Med 1993;21:720-723. Weinfeld SB, Haddad SL, Myerson MS: Metatarsal stress fractures. Clip Sports Med 1997;16:319-338.
1. 01.184 A 62-year-old man has pain with overhead activities and shoulder weakness.
2. History reveals that he sustained an anterior dislocation of the right shoulder 18
3. months ago and underwent open repair of the subscapularis, supraspinatus, and
4. infraspinatus tendons 2 weeks after the injury. Examination reveals active total
5. elevation of 160°, active external rotation of 50°, and passive internal rotation
6. to T9. He has 5/5 deltoid, 4-/5 external rotation, and 5/5 internal rotation
7. strength. What is the most likely cause of his symptoms?
8. 1- Residual rotator cuff tear
9. 2- Adhesive capsulitis
10. 3- Glenohumeral instability
11. 4- Axillary neuropathy
12. 5- Suprascapular neuropathy
1. answer
1. back
1. Question 01.184
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Gerber C, Fucks B, Holler J: The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am 2000;82:505-515. Harryman DT II, Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am 1991;73:982-989.
1. 01.185 A 6-year-old girl has a right genu varum that has progressed over the last 6
2. months. Plain radiographs of the knee reveal a sloping medial joint line with an
3. obvious bony bar at the medial proximal tibial physis. A CT scan shows that
4. this bar involves about 20% of the physis. Treatment at this time should include
5. 1- epiphyseodesis of the proximal tibial physis.
6. 2- corrective osteotomy of the tibia and fibula.
7. 3- corrective osteotomy of the tibia and epiphyseodesis of the left proximal tibial
8. physis.
9. 4- proximal tibial physeal bar resection and corrective osteotomy of the tibia and fibula.
10. 5- elevating osteotomy of the proximal tibial medial plateau.
1. answer
1. back
1. Question 01.185
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520. Tachdjian MA: Tibia vara, in Pediatric Orthopaedics. Philadelphia, PA, WB Saunders, 1990, p 2846. Greene WB: Infantile tibia vara. Instr Course Lect 1993;42:525-538.
1. 01.186 An 18-year-old patient has the painful lesion shown in Figure 58a. A biopsy
2. specimen is shown in Figure 58b. Management should consist of
3. 1- preoperative chemotherapy and wide resection.
4. 2- wide resection only.
5. 3- marginal distal ulna resection.
6. 4- curettage and bone grafting.
7. 5- low-dose radiation.
1. answer
1. back
1. A
1. B
1. Figures 58
1. Question 01.186
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Martinet V, Sissons HA: Aneurysmal bone cyst: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-2304. Biesecker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cysts: A clinicopathologic study of 66 cases. Cancer 1970;26:615-625. Gibbs CP Jr, Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
1. 01.187 The value of intercondylar notch visualization of the posterior compartment
2. during anterior cruciate ligament reconstruction is to identify
3. 1- a loose body.
4. 2- a popliteus injury.
5. 3- meniscal root tears.
6. 4- an injury to the ligament of Wrisberg.
7. 5- an osteochondral injury.
1. answer
1. back
1. Question 01.187
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Amin KB, Cosgarea AJ, Kaeding CC: The value of intercondylar notch visualization of the posteromedial and posterolateral compartments during knee arthroscopy. Arthroscopy 1999;15:813-817. Boytim MJ, Smith JP, Fischer DA, Quick DC: Arthroscopic posteromedial visualization of the knee. Clip Orthop 1995;310:82-86.
1. 01.188 Figures 59a and 59b show the radiographs of an 8-year-old boy who has
2. atraumatic recurrent lateral dislocation of the left patella. Examination reveals
3. no fixed genu varum or valgum, and the lower extremity lengths are equal. The
4. Q angle is 25°. The extended hips show internal rotation of 40° and external
5. rotation of 60°, with a neutral thigh-foot angle. There is no generalized
6. ligamentous laxity. Treatment should consist of
7. 1- femoral rotational osteotomy.
8. 2- tibial rotational osteotomy.
9. 3- tibial tuberosity transfer (Fulkerson, Elmslie-Trillat,
10. or Hauser).
11. 4- tenodesis of the semitendinosus to the patella.
12. 5- patellectomy and vastus medialis advancement.
1. answer
1. back
1. A
1. B
1. Figures 59
1. Question 01.188
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hall JE, Micheli LJ, McManama GB Jr- Semitendinosus tenodesis for recurrent subluxation or dislocation of the patella. Clin Orthop 1979;144:31-35. Sponseller PD, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1231-1329. Tolo V: Fractures and dislocations about the knee, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 431-458. Lefts RM, Davidson D, Beaule P: Semitendinosus tenodesis for repair of recurrent dislocation of the patella in children. J Pediatr Orthop 1999;19:742-747.
1. 01.189 The posterior (Thompson) approach to the proximal radial shaft lies between
2. the
3. 1- extensor carpi ulnaris and anconeus.
4. 2- extensor carpi ulnaris and extensor carpi radialis longus.
5. 3- extensor carpi radialis longus and extensor carpi radialis brevis.
6. 4- extensor carpi radialis brevis and extensor digitorum communis.
7. 5- brachioradialis and extensor carpi radialis longus.
1. answer
1. back
1. Question 01.189
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp 109-139. Thompson BE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309.
1. 01.190 Concurrent injuries to which of the following structures results in an increased
2. osteogenic response to fracture?
3. 1- Head
4. 2- Liver
5. 3- Chest
6. 4- Major artery
7. 5- Bladder
1. answer
1. back
1. Question 01.190
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Kushwaha VP, Garland DG: Extremity fractures in the patient with a traumatic brain injury. J Am Acad Orthop Surg 1998;6:298-307. Spencer RF: The effect of head injury on fracture healing: A quantitative assessment. J Bone Joint Surg Br 1987;69:525-528.
1. 01.191 A 29-year-old man sustained a talar neck fracture with an associated
2. dislocation of the body of the talus from the subtalar and tibiotalar joints. He
3. was treated with immediate open reduction and internal fixation. Twelve weeks
4. later, the fracture has united, and lucency is observed in the superior
5. subchondral bone of the talar body. The next most appropriate step in
6. management should consist of
7. 1- bone grafting of the talar neck and body.
8. 2- application of an ultrasound bone stimulator.
9. 3- a brace with calipers.
10. 4- MRI to assess body viability.
11. 5- protected weight bearing.
1. answer
1. back
1. Question 01.191
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 201-213. Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, p 1176.
1. 01.192 Within the normal healthy lumbar disk of a young person, proteoglycans
2. constitute a
3. 1- low percent of dry weight within the annulus, a high percent of dry weight within the
4. nucleus, and interact with H2O to primarily resist compression.
5. 2- low percent of dry weight within the annulus, a high percent of dry weight within the
6. nucleus, and interact with H2O to primarily resist tension.
7. 3- high percent of dry weight within the annulus, a low percent of dry weight within the
8. nucleus, and interact with H2O to primarily resist compression.
9. 4- high percent of dry weight within the annulus, a low percent of dry weight within the
10. nucleus, and interact with H2O to primarily resist tension.
11. 5- high percent of dry weight within the annulus, a low percent of dry weight within the
12. nucleus, and have no interaction with H2O.
1. answer
1. back
1. Question 01.192
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 548-556. Buckwalter JA, Pedrini-Mille A, Pedrini V, Tudisco C: Proteoglycans of human infant intervertebral disc: Electron microscopic and biochemical studies. J Bone Joint Surg Am 1985;67:284-294.
1. 01.193 A 40-year-old woman has right shoulder pain and limited range of motion.
2. History reveals that she sustained a right proximal humerus fracture 10 years
3. ago and was treated with a sling and physical therapy. Examination reveals
4. active forward elevation of 100°, active external rotation of 0°, and passive
5. internal rotation to L5. Passive shoulder motion is the same. Plain radiographs
6. of the shoulder are shown in Figures 60a and 60b. Treatment should now
7. consist of
8. 1- arthroscopic debridement.
9. 2- humeral osteotomy.
10. 3- core decompression.
11. 4- humeral head replacement.
12. 5- capsular release.
1. answer
1. back
1. A
1. B
1. Figures 60
1. Question 01.193
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Norris TR, Green A, McGuigan FX: Late prosthetic arthroplasty for displaced proximal humerus fractures. J Shoulder Elbow Surg 1995;4:271-280. Schlegel TF, Hawkins RJ: Displaced proximal humeral fractures: Evaluation and treatment. J Am Acad Orthop Surg 1994;2:54-78.
1. 01.194 The lateral crista of the trochlea develops from what secondary ossification
2. center?
3. 1- Medial condylar epiphysis
4. 2- Lateral condylar epiphysis
5. 3- Medial epicondylar apophysis
6. 4- Lateral epicondylar apophysis
7. 5- Olecranon apophysis
1. answer
1. back
1. Question 01.194
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Wilkins KE: Fractures and dislocations of the elbow region: Part L The elbow region: General concepts in the pediatric patient, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 653-669.
1. 01.195 A 40-year-old man sustains a rupture of the Achilles tendon while playing
2. recreational basketball. If he undergoes surgical repair rather than nonsurgical
3. management, the patient should be told to expect a
4. 1- lower skin complication rate and a longer period of rehabilitation.
5. 2- lower re-rupture rate and a longer period of rehabilitation.
6. 3- higher re-rupture rate and a shorter rehabilitation.
7. 4- higher skin complication rate and a higher re-rupture rate.
8. 5- higher skin complication rate and a lower re-rupture rate.
1. answer
1. back
1. Question 01.195
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 786-861. Troop RL, Losse GM, Lane JG, Robertson DB, Hastings PS, Howard ME: Early motion after repair of Achilles tendon ruptures. Foot Ankle Int 1995;16:705-709.
1. 01.196 Which of the following is considered the most sensitive sensory test for
2. detecting early carpal tunnel syndrome?
3. 1- Light touch sensation
4. 2- Pinprick sensation
5. 3- Two-point discrimination
6. 4- Moving two-point discrimination
7. 5- Semmes-Weinstein monofilament
1. answer
1. back
1. Question 01.196
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, B., American Academy of Orthopaedic Surgeons, 1996, pp 221-231. Szabo RM, Gelberman RH, Dimick MD: Sensibility testing in patients with carpal tunnel syndrome. J Bone Joint Surg Am 1984;66:60-64.
1. 01.197 A 16-year-old boy has had pain in the lateral ankle and hindfoot after sustaining
2. a minor ankle sprain 6 months ago. The pain is worse with any twisting activity
3. of the foot. Examination reveals normal alignment of the foot and ankle. An AP
4. radiograph of the ankle and foot is normal. A lateral radiograph is shown in
5. Figure 61. What is the most likely cause of his persistent pain?
6. 1- Fracture of the lateral process of the talus
7. 2- Fracture of the anterior process of the calcaneus
8. 3- Fracture of the tibial plafond
9. 4- Talocalcaneal coalition
10. 5- Stress fracture of the calcaneus
1. answer
1. back
1. Figure 61
1. Question 01.197
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Richardson EG: Flatfoot in children and adults, in Coughlin MJ, Mate RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science,
3. 1999, pp 702-733. Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
1. 01.198 A patient who underwent total knee arthroplasty 2 years ago has a range of
2. motion of 0° to 60°. The implants are well fixed, and the knee is well aligned
3. on AP radiographs. Lateral .radiographs show that the femoral component is
4. appropriately sized and the tibial component is in 5° of anterior tilt. Treatment
5. should consist of
6. 1- revision of the femoral component.
7. 2- revision of the tibial component.
8. 3- closed knee manipulation.
9. 4- open lysis of adhesions.
10. 5- open quadricepsplasty.
1. answer
1. back
1. Question 01.198
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
1. 01.199 When compared to plate fixation, antegrade intramedullary nailing of humeral
2. shaft fractures results in
3. 1- better elbow function.
4. 2- a higher rate of union.
5. 3- a higher rate of complications.
6. 4- a higher rate of infection.
7. 5- longer surgical time.
1. answer
1. back
1. Question 01.199
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267. McCormack RG, Brien D, Buckley RE, McKee MD, Powell J, Schemitsch EH: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective randomized trial. J Bone Joint Surg Br 2000;82:336-339.
1. 01.200 Which of the following groups is most at risk for osteoporosis?
2. 1- Caucasian men
3. 2- Caucasian women
4. 3- African-American women
5. 4- Hispanic men
6. 5- Hispanic women
1. answer
1. back
1. Question 01.200
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Lane JM, Nydick M: Osteoporosis: Current modes of prevention and treatment. J Am Acad Orthop Surg 1999;7:19-31. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-115
1. 01.201 A 49-year-old man with advanced glenohumeral arthritis undergoes total
2. shoulder replacement. Following surgery, he reports pain relief but now has
3. weakness when using his arm for activities in front of his body. He is unable to
4. hold the dorsum of his hand away from his back. The weakness is most likely
5. related to what muscle?
6. 1- Supraspinatus
7. 2- Subscapularis
8. 3- Infraspinatus
9. 4- Deltoid
10. 5- Pectoralis major
1. answer
1. back
1. Question 01.201
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Gerber C, Farrow MD: Isolated tears of the subscapularis tendon. Orthop Trans 1995;19:457. Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
1. 01.202 An ankle fracture heals with an anatomically aligned mortise and 2 mm of
2. displacement of the distal fibula fracture. What affect will these findings have
3. on the tibiotalar joint?
4. 1- Decreased contact loading
5. 2- Increased contact loading
6. 3- Increased external rotation
7. 4- Increased medial-lateral translation
8. 5- Normal loading, rotation, and translation
1. answer
1. back
1. Question 01.202
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Brown TD, Hurlbut PT, Hale JE, et a1: Effects of imposed hindfoot constraint on ankle contact mechanics for displaced lateral malleolar fractures. J Orthop Trauma 1994;8:511-519. Michelson JD: Fractures about the ankle. J Bone Joint Surg Am 1995;77:142-152.
1. 01.203 Figure 62 shows the MRI scan of a 30-year-old male volleyball player who has
2. had shoulder pain for the past 6 months. Which of the following physical
3. findings in the shoulder would be most consistent with this lesion?
4. 1- Weakness of internal rotation
5. 2- Weakness of external rotation
6. 3- Weakness of abduction
7. 4- Positive impingement sign
8. 5- Positive apprehension sign
1. answer
1. back
1. Figure 62
1. Question 01.203
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Thompson RC Jr, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
1. 01.204 In cemented polyethylene acetabular components, the reported average
2. polyethylene wear rate on a yearly basis is how many millimeters?
3. 1- 0.01
4. 2- 0.05
5. 3- 0.1
6. 4- 1.0
7. 5- 2.0
1. answer
1. back
1. Question 01.204
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Jasty M, Goetz DD, Bragdon CP, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
1. 01.205 The Lisfranc ligament connects what two bones?
2. 1- Middle cuneiform and first metatarsal
3. 2- Middle cuneiform and second metatarsal
4. 3- Medial cuneiform and first metatarsal
5. 4- Medial cuneiform and second metatarsal
6. 5- Medial cuneiform and middle cuneiform
1. answer
1. back
1. Question 01.205
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Sanafian SK: Osteology, in Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 37-112. Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. SL Louis, MO, Harcourt Health Science, 1999, pp 1090-1209.
1. 01.206 The arrow in the axial MRI scan shown in Figure 63 is pointing to what
2. muscle?
3. 1- Gracilis
4. 2- Adductor brevis
5. 3- Sartorius
6. 4- Semitendinosus
7. 5- Pectineus
1. answer
1. back
1. Figure 63
1. Question 01.206
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 401-429.
1. 01.207 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.208 Which of the following conditions will most likely cause disability at some
2. point in the life of a patient with achondroplasia?
3. 1- Degenerative joint disease of the knees
4. 2- Cervical instability with myelopathy
5. 3- Scoliosis of the thoracic or lumbar spine
6. 4- Spinal stenosis
7. 5- Progressive contractures of the limbs
1. answer
1. back
1. Question 01.208
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Pyeritz RE, Sack GH Jr, Udvarhelyi GB: Thoracolumbosacral laminectomy in achondroplasia: Long-term results in 22 patients. Am J Med Genet 1987;28:433-444. Tolo VT: Spinal deformity in skeletal dysplasia, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 369-393.
1. 01.209 The use of calcium supplements should be
2. 1- encouraged in girls at puberty to help prevent osteoporosis.
3. 2- restricted until menopause to decrease the risk of renal stones.
4. 3- left to individual preference until perimenopause, then started routinely.
5. 4- started only after a bone mineral density study indicates a deficiency of 2 standard
6. deviations.
7. 5- started only after a bone mineral density study indicates a deficiency of 1 standard
8. deviation.
1. answer
1. back
1. Question 01.209
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
1. 01.210 The bending strength of fractured long bones fixed with an experimental
2. compression plate is compared with unfractured controls. What statistical test
3. should be used to compare the mean bending strength of the two groups?
4. 1- Student's t test
5. 2- Analysis of variance
6. 3- Regression analysis
7. 4- Chi-square test
8. 5- Wilcoxon two-sample test
1. answer
1. back
1. Question 01.210
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 397-446.
1. 01.211 Which of the following factors has been shown to be an independent risk factor
2. for infection after open reduction and internal fixation of the calcaneus through
3. an extensile lateral incision?
4. 1- Age of greater than 50 years
5. 2- History of smoking
6. 3- A comminuted posterior facet
7. 4- Extension of the fracture into the sustentaculum
8. 5- Use of phenytoin
1. answer
1. back
1. Question 01.211
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Folk JW, Stan AJ, Early JS: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999;13:369-372.
1. 01.212 Examination of a 65-year-old woman who sustained a stroke 18 months ago
2. reveals a clenched fist deformity that is causing significant hygiene problems
3. because of skin maceration and malodor. She has no observed voluntary motor
4. control of the hand or forearm. Management should consist of
5. 1- open phenol blocks.
6. 2- botulinum toxin blocks.
7. 3- proximal interphalangeal and distal interphalangeal arthrodesis.
8. 4- flexor tenotomies.
9. 5- a superficialis-to-profundus tendon transfer.
1. answer
1. back
1. Question 01.212
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Braun RN, Vise GT, Roger B: Preliminary experience with superficialis-to profundus tendon transfer in the hemiplegic upper extremity. J Bone Joint Surg Am 1974;56:466-472. Hisex MS, Keenan MAE: Orthopaedic management of upper extremity dysfunction following stroke or brain injury, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 287-324.
1. 01.213 Revision of a failed acetabular component with a bipolar endoprosthesis and
2. acetabular bone grafting is most likely to fail because of what mechanism?
3. 1- Osteolysis
4. 2- Femoral stem loosening
5. 3- Recurrent dislocation
6. 4- Bipolar head migration
7. 5- Bipolar head disengagement
1. answer
1. back
1. Question 01.213
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Brien WW, Bruce WJ, Salvati EA, Wilson PD 1r, Pellicci PM: Acetabular reconstruction with a bipolar prosthesis and morseled bone grafts. J Bone Joint Surg Am 1990;72:1230-1235. McFarland EG, Lewallen DG, CabaneIa ME: Use of bipolar endoprosthesis and.bone grafting for acetabular reconstruction. Clin Orthop 1991; 268:128-129. Papagelopoulus PJ, Lewallen DG, Cabanela ME, McFarland EG, Wallnichs SL: Acetabular reconstruction using bipolar endoprosthesis and bone grafting in patients with severe bone deficiency. Clin Orthop 1995;314:170-184.
1. 01.214 An 18-year-old man sustains the proximal femur fracture shown in Figures 64a
2. and 64b. Definitive management should consist of
3. 1- traction for 6 weeks.
4. 2- a functional brace.
5. 3- a 135° angle sliding hip screw.
6. 4- a 95° fixed angle plate.
7. 5- antegrade nailing with transverse screws.
1. answer
1. back
1. A
1. B
1. Figures 64
1. Question 01.214
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kinast C, Bolhofner BR, Mast 1W, Ganz R: Subtrochanteric fractures of the femur: Results of treatment with the 95 degrees blade-plate. Clin Orthop 1989;238:122-130.
1. 01.215 In the treatment of femoral shaft fractures, the lowest union rate has been
2. reported after which of the following types of nailing?
3. 1- Reamed antegrade locked
4. 2- Reamed antegrade unlocked
5. 3- Reamed retrograde locked
6. 4- Unreamed antegrade locked
7. 5- Unreamed retrograde locked
1. answer
1. back
1. Question 01.215
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Moed BR, Watson JT, Cramer KE, Karges DE, Teefey JS: Unreamed retrograde intramedullary nailing of fractures of the femoral shaft. J Orthop Trauma 1998;12334-342. Moed BR, Watson JT: Retrograde intramedullary nailing, without reaming, of fractures of the femoral shaft in multiply injured patients. J Bone Joint Surg Am 1995;77:1520-1527.
1. 01.216 A 36-year-old man has pain in the metatarsophalangeal (MTP) joint of the
2. great toe with all weight-bearing activities, and management consisting of shoe
3. modification and an insert has failed to provide relief. Examination reveals a
4. painful 10° arc of motion. Radiographs show degenerative changes with dorsal
5. and medial osteophytes and joint narrowing. Treatment should now consist of
6. 1- excision of the osteophytes and the dorsal third of the metatarsal head.
7. 2- a dorsiflexion osteotomy of the metatarsal head.
8. 3- resection arthroplasty of the MTP joint.
9. 4- a Silastic implant of the MTP joint.
10. 5- arthrodesis of the MTP joint.
1. answer
1. back
1. Question 01.216
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mann RA, Clanton TO: Hallux rigidus: Treatment by cheilectomy. J Bone Joint Surg Am 1988;70:400-406. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 151-161. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 605-633.
1. 01.217 A 14-year-old boy who plays football sustains a valgus force to his knee.
2. Examination reveals a 1+ effusion and decreased range of motion. Lachman
3. test results are negative. He has no joint line tenderness, but he does have
4. tenderness over the proximal origin of the medial collateral ligament and pain
5. with valgus stressing. Initial plain radiographs of the knee are normal. Further
6. evaluation should include
7. 1- arthrography.
8. 2- MRI.
9. 3- a bone scan.
10. 4- emergent arthroscopy.
11. 5- stress radiographs.
1. answer
1. back
1. Question 01.217
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Sponseller PD, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1231-1329. Cook PC, Leit ME: Issues in the pediatric athlete. Orthop Clin North Am 1995;26:453-464.
1. 01.218 A 35-year-old man sustained an isolated closed displaced bicondylar tibial
2. plateau fracture after being struck by a car. Reduction and internal fixation of
3. both condyles can be most safely achieved using which of the following
4. surgical approaches?
5. 1- Isolated anterior midline
6. 2- Isolated lateral parapatellar
7. 3- Isolated posteromedial
8. 4- Combined anterolateral and posteromedial
9. 5- Combined anterior midline and posterior transpopliteal
1. answer
1. back
1. Question 01.218
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Georgiadis GM: Combined anterior and posterior approaches for complex tibial plateau fixations. J Bone Joint Surg Br 1994;76:285-289.
1. 01.219 Which of the following conditions is most commonly associated with
2. congenital fibular hemimelia?
3. 1- Congenital absence of the patella
4. 2- Congenital absence of the first ray
5. 3- Genu varum
6. 4- Equinovarus ankle
7. 5- Talocalcaneal coalition
1. answer
1. back
1. Question 01.219
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Grogan DP, Holt GR, Ogden JA: Talocalcaneal coalition in patients who have fibular hemimelia or proximal femoral focal deficiency: A comparison of the radiographic and pathological findings. J Bone Joint Surg Am 1994;76:1363-1370. Epps CH Jr, Schneider PL: Treatment of hemimelias of the lower extremity: Long term results. J Bone Joint Surg Am 1989;71273-277.
1. 01.220 A 58-year-old woman has severe neck pain after falling at home. Examination
2. reveals intact deltoid strength, 2/5 weakness in the rest of the right upper
3. extremity, and 2/5 weakness in the left upper extremity, except for a grip
4. strength of 3/5. She has 4/5 strength in both lower extremities, good rectal
5. tone, and an intact bulbocavernosus reflex. Sensation is intact. Which of the
6. following conditions best characterizes her neurologic injury?
7. 1- A complete spinal cord injury
8. 2- Bilateral brachial plexopathies
9. 3- Multilevel cervical radiculopathy
10. 4- Anterior cord syndrome
11. 5- Central cord syndrome
1. answer
1. back
1. Question 01.220
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. McGuire RA: Physical examination in spinal trauma, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA. WB Saunders, 1998, pp 17-27. Bohiman HH, Docker TB: Spine trauma in adults: Spine and spinal cord injuries, in Herkowitz HN, Eismont FJ, Garfin SR, Bell GR, Balderston RA, Wiesel SW (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 889-914.
1. 01.221 A 25-year-old construction worker reports a mass on the dorsum of his hand
2. that is painful with strenuous use. Examination reveals a 4 x 2 x 1 cm soft mass
3. that overlies the proximal portions of the index and middle metacarpals. It
4. moves with flexion and extension of those digits, becomes firmer with forceful
5. grasp, and does not transilluminate. What is the most likely diagnosis?
6. 1- Dorsal wrist ganglion
7. 2- Extensor tenosynovitis
8. 3- Giant cell tumor of the tendon sheath
9. 4- Carpal boss
10. 5- Anomalous extensor muscle
1. answer
1. back
1. Question 01.221
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Tan ST, Smith PJ: Anomalous extensor muscles of the hand: A review. J Hand Sung Am 1999;24:449-455. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1950-1987.
1. 01.222 Which of the following cytokines have been implicated in the pathogenesis of
2. rheumatoid arthritis?
3. 1- Fibroblastic growth factor and transforming growth factor
4. 2- Parathyroid hormone-related protein and interferon-gamma
5. 3- Interleukin- 1 and tumor necrosis factor
6. 4- Interleukin-4 and granulocyte-macrophage colony-stimulating factor
7. 5- Interleukin- 10 and vascular endothelial growth factor
1. answer
1. back
1. Question 01.222
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty 3H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 205-216. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 490-530.
1. 01.223 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.224 An 11-year-old girl has had progressive medial midfoot pain bilaterally for the
2. past 6 months. Her mother states that the child's feet appeared normal until the
3. pain started, and she is concerned about the development of flatfeet. What is
4. the most likely diagnosis?
5. 1- Physiologic pes planus
6. 2- Charcot foot
7. 3- Posterior tibial tendon insufficiency
8. 4- Congenital vertical talus
9. 5- Accessory navicular
1. answer
1. back
1. Question 01.224
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Prichasuk S, Sinphurmsuksknl O: Kidner procedure for symptomatic accessory navicular and its relation to pes planus. Foot Ankle Int 1995;16:500-503.
1. 01.225 Which of the following is considered the most important factor in preventing
2. failure of fixation of displaced femoral neck fractures?
3. 1- Use of a compression screw and side plate
4. 2- Use of cannulated screws
5. 3- Accuracy of reduction
6. 4- Reduction on a traction table
7. 5- Release of a capsular hematoma
1. answer
1. back
1. Question 01.225
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Chug D, Jaglal SB, Schatzker J: Predictors of early failure of fixation in the treatment of displaced subcapital hip fractures. J Orthop Trauma 1998;12:230-234. Swiontkowski MF: Intracapsular fractures of the hip. J Bone Joint Surg Am 1994;76:129-138.
1. 01.226 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.227 The process of host repair following osteonecrosis is referred to as
2. 1- haversian remodeling.
3. 2- osteogenesis.
4. 3- osteoinduction.
5. 4- fracture healing.
6. 5- creeping substitution.
1. answer
1. back
1. Question 01.227
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds)- Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.228 What type of knee dislocation is most likely to be irreducible by closed means?
2. 1- Posterior
3. 2- Anterior
4. 3- Lateral
5. 4- Posterolateral
6. 5- Posteromedial
1. answer
1. back
1. Question 01.228
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 151-155. Quinlan AG, Sharrard WJW: Posterolateral dislocation of the knee with capsular interposition. J Bone Joint Surg Br 1958;40:660-663.
1. 01.229 A 16-year-old boy who is 5 ft 4 in tall reports pain in the knees and ankles.
2. Examination reveals that his knees are in 15° of valgus. The articular surfaces
3. of the knees and ankles are irregular, and the femoral heads are slightly
4. flattened. A lateral radiograph shows that the patellae have a double layer.
5. What is the most likely diagnosis?
6. 1- Kneist syndrome
7. 2- Spondyloepiphyseal dysplasia congenita
8. 3- Multiple epiphyseal dysplasia
9. 4- Achondroplasia
10. 5- Dyschondrosteosis
1. answer
1. back
1. Question 01.229
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Dietz FR, Matthews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Bone Joint Surg Am 1996;78:1583-1598. Spranger J: The epiphyseal dysplasias. Clip Orthop 1976;114:46-59. Sheffield EG: Double-layered patella in multiple epiphyseal dysplasia: A valuable clue in the diagnosis. J Pediatr Orthop 1998;18:123-128.
1. 01.230 What is the most common primary malignancy that metastasizes to the bones
2. of the hand?
3. 1- Breast
4. 2- Prostate
5. 3- Renal
6. 4- Colon
7. 5- Lung
1. answer
1. back
1. Question 01.230
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 369-376. Athanasian EA: Bone and soft-tissue tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2223-2253.
1. 01.231 A 14-year-old girl has been limping and has had pain with weight bearing on
2. the right lower leg for the past 48 hours. She has a temperature of 100°F
3. (37.7°C). She prefers a prone position with the right hip and knee extended.
4. Pain is produced by placing the hip in flexion, abduction, and external rotation.
5. Which of the following studies will best confirm the diagnosis?
6. 1- Hip joint aspiration
7. 2- AP radiograph of the pelvis
8. 3- Oblique radiograph of the lumbar spine
9. 4- CT of the abdomen
10. 5- MRI of the pelvis
1. answer
1. back
1. Question 01.231
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Bollow M, Braun 1, Biedermann T, et al: Use of contrast-enhanced MR imaging to detect sacroiliitis in children. Skeletal Radiol 1998;27:606-616. Tisserant R, Loeuille D, Pere P, Gancher A, Ponrel J, Blum A: Septic sacroiliitis during the postpartal period: Diagnostic contribution of magnetic resonance imaging. Rev Rheum Engl Ed 1999;66:512-515.
1. 01.232 A surgeon who is planning a total elbow arthroplasty would like to use a
2. prosthesis that he helped to develop. A royalty payment is received each time
3. the prosthesis is used. What is the surgeon's ethical responsibility?
4. 1- The prosthesis should not be used.
5. 2- The prosthesis can be used, but the royalty payment information should not be
6. discussed with the patient.
7. 3- The royalty payment information should be included on the informed consent
8. document but not discussed with the patient.
9. 4- The patient should be informed that the surgeon receives a royalty payment for using
10. the prosthesis.
11. 5- The surgeon should offer to split the royalty payment with the patient.
1. answer
1. back
1. Question 01.232
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Wenger NS, Liu H, Lieberman JR: Teaching medical ethics to orthopaedic surgery residents. J Bone Joint Surg Am 1998;80:1125-1131.
1. 01.233 In trauma patients older than age 60 years, mortality most closely correlates
2. with
3. 1- the injury severity score (ISS).
4. 2- the extremity abbreviated injury score (AIS).
5. 3- the need for orthopaedic surgery.
6. 4- the timing of orthopaedic surgery.
7. 5- a history of type I diabetes mellitus.
1. answer
1. back
1. Question 01.233
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Tornetta P BI, Mostafavi H, Riina J, et al: Morbidity and mortality in elderly trauma patients. J Trauma 1999;46:702-706.
1. 01.234 A 46-year-old woman has had plantar heel pain for the past 5 months. She
2. reports that the pain is most severe when she arises out of bed in the morning
3. and when she stands after being seated for a period of time. Initial management
4. should consist of
5. 1- surgical lengthening of the Achilles tendon.
6. 2- surgical release of the plantar fascia.
7. 3- a custom orthosis.
8. 4- a stretching program and a cushioned heel insert.
9. 5- a corticosteroid injection.
1. answer
1. back
1. Question 01.234
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Pfeffer G, Bacchetti P, Deland J, et al: Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int 1999;20:214-221. Richardson EG: Heel pain, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1090-1209.
1. 01.235 The triceps reflex is largely a function of what neurologic level?
2. 1- C5
3. 2- C6
4. 3- C7
5. 4- C8
6. 5- T1
1. answer
1. back
1. Question 01.235
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Snider RK (ed): Essentials of Musculoskeletal Care. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 491-546.
1. 01.236 A 19-year-old female swimmer has had right shoulder pain for the past 5 years.
2. Although she had responded previously to physical therapy, she has been in
3. rehabilitation for the past 6 months without improvement. Examination reveals
4. active total elevation of 170°, active external rotation of 70°, and passive
5. internal rotation to T3. There is symmetric 2+ glenohumeral translation in the
6. anterior, posterior, and inferior directions and a positive Neer impingement
7. sign. Treatment should consist of
8. 1- open Bankart repair.
9. 2- an inferior capsular shift.
10. 3- arthroscopic coracoacromial ligament resection.
11. 4- arthroscopic acromioplasty.
12. 5- arthroscopic Bankart repair.
1. answer
1. back
1. Question 01.236
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multi-directional instability of the shoulder. A preliminary report J Bone Joint Surg Am 1980;62:897-908. Schenk TJ, Brems JJ: Multi-directional instability of the shoulder Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1998;6:65-72.
1. 01.237 What is the most common complication at a minimum of 1 year after treatment
2. with a reamed antegrade nail for a femoral shaft fracture?
3. 1- Nonunion
4. 2- Malunion
5. 3- Trendelenburg gait
6. 4- Hip discomfort
7. 5- Osteonecrosis of the femoral head
1. answer
1. back
1. Question 01.237
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Bain GI, Zacest AC, Paterson DC, Middleton J, Pohl AP: Abduction strength following intramedullary nailing of the femur. J Orthop Trauma 1997;11:93-97.
1. 01.238 A 13-year-old boy has nonrigid Scheuermann's kyphosis. Weight-bearing
2. radiographs show a kyphosis of 70° from T7 to L1, with scoliosis that
3. measures 10° at Risser 2 maturity. Management should consist of
4. 1- postural exercises and analgesics.
5. 2- a Charleston bending brace.
6. 3- an extension-type spinal orthosis.
7. 4- posterior spinal fusion with instrumentation.
8. 5- anterior spinal release and posterior spinal instrumentation.
1. answer
1. back
1. Question 01.238
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Lowe TG: Scheuermann disease. J Bone Joint Surg Am 1990;72:940-945. Tribes CB: Scheuermann's kyphosis in adolescents and adults: Diagnosis and management. J Am Acad Orthop Surg 1998;6:36-43.
1. 01.239 A 21-year-old male wrestler sustained a right posterolateral elbow dislocation
2. with an associated type I coronoid fracture 2 years ago. Management at the
3. time of injury consisted of application of a splint for 2 weeks. He now reports
4. recurrent elbow subluxation and pain. What is the most likely cause of the
5. instability?
6. 1- Displaced coronoid process fracture
7. 2- Insufficiency of the lateral ulnar collateral ligament
8. 3- Insufficiency of the anterior band of the medial collateral ligament
9. 4- Insufficiency of the posterior band of the medial collateral ligament
10. 5- Anterior capsular insufficiency
1. answer
1. back
1. Question 01.239
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Josefsson PO, Johnell O, Gentz CF: Long-term sequelae of simple dislocation of the elbow. J Bone Joint Surg Am 1984;66:927-930. Nestor BJ, O'Driscoll SW, Morrey BF: Ligamentous reconstruction for posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1992;74:1235-1241. O'Driscoll SW, Money BF, Korinek S, An KN: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
1. 01.240 The degree of ulnar variance is best defined by
2. 1- arthrography.
3. 2- MRI.
4. 3- cineradiographs.
5. 4- stress radiographs.
6. 5- plain radiographs.
1. answer
1. back
1. Question 01.240
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Nagle DJ: Evaluation of chronic wrist pain. J Am Acad Orthop Surg 2000;8:45-55. Epner RA, Bowers WH, Guilford WB: Ulnar variance: The effect of wrist positioning and roentgen filming technique. J Hand Surg Am 1982;7:298-305.
1. 01.241 An 18-year-old woman has had left hip pain for the past 2 months.
2. Examination reveals audible snapping with extension of a flexed, abducted,
3. and externally rotated hip. What study is most likely to establish the diagnosis?
4. 1- Bone scan
5. 2- Iliopsoas bursography
6. 3- Plain radiography
7. 4- Hip arthrography
8. 5- Hip arthroscopy
1. answer
1. back
1. Question 01.241
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Schaberg JF, Harper MC, Allen WC: The snapping hip syndrome. Am J Sports Med 1984;12:361-365. Jacobson T, Allen WC: Surgical correction of the snapping iliopsoas tendon. Am J Sports Med 1990;18:470-474.
1. 01.242 What metabolic bone disease is associated with abnormal osteoclastic
2. function?
3. 1- X-linked hypophosphatemic rickets
4. 2- Fanconi's syndrome
5. 3- Osteopetrosis
6. 4- Osteomalacia
7. 5- Paget's disease of bone
1. answer
1. back
1. Question 01.242
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL. American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Shapiro F: Osteopetrosis: Current clinical considerations. Clin Orthop 1993;294:344.
1. 01.243 The Glasgow Coma Scale categorizes the neurologic status of a multiply
2. injured patient by assessing verbal response, motor response, and
3. 1- orientation.
4. 2- response to commands.
5. 3- pupillary response.
6. 4- withdrawal to pain.
7. 5- eye opening response.
1. answer
1. back
1. Question 01.243
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Turen CH, Dube MA, LeCroy MC: Approach to the polytraumatized patient with musculoskeletal injuries. J Am Acad Orthop Surg 1999;7:154-165. Teasdale G, Jennett B: Assessment of coma and impaired consciousness: A practical scale. Lancet 1974;2:81-84.
1. 01.244 Which of the following is considered the preferred total knee design for a
2. patient with a history of a patellectomy?
3. 1- Posterior cruciate ligament-retaining
4. 2- Posterior cruciate ligament-substituting
5. 3- Rotating hinge
6. 4- Unicondylar
7. 5- Meniscal bearing
1. answer
1. back
1. Question 01.244
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582. Paletta GA Jr, Laskin RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
1. 01.245 A child with chronic recurrent multifocal osteomyelitis has painful swelling
2. and tenderness in the right medial clavicle with no fluctuance. She has a
3. temperature of 99°F (37.2°C). The palms and soles show pustular lesions.
4. Radiographs reveal periosteal new bone formation in the medial clavicle.
5. Management should consist of
6. 1- a steroid injection into the medial clavicle.
7. 2- oral nonsteroidal anti-inflammatory drugs.
8. 3- IV administration of oxacillin for 4 weeks.
9. 4- IV administration of gamma globulin.
10. 5- incision and drainage of the medial clavicle.
1. answer
1. back
1. Question 01.245
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Godette GA, Murray DP, Gruel CR, Leonard 1C: Chronic recurrent multifocal osteomyelitis. Orthopedics 1992;15:520-521, 525-526. Bjorksten B, Gustavson K-H, Eriksson B, Lindholm A, Nordstrom S: Chronic recurrent multifocal osteomyelitis and pustulosis palmoplantaris. J Pediatr 1978;93:227-231. Stanton RP, Lopez-Sosa FH, Doidge R: Chronic recurrent multifocal osteomyelitis. Orthop Rev 1993;22:229-233.
1. 01.246 A 32-year-old woman reports right shoulder pain and has difficulty with
2. overhead activities. History reveals that she underwent an open anterior labral
3. repair and capsular shift to treat anterior glenohumeral instability 3 years ago.
4. Examination reveals tenderness over the anterior shoulder, active and passive
5. total elevation of 120°, and external rotation of 30°. Shoulder strength is
6. normal. Plain radiographs are normal. Physical therapy has failed to provide
7. relief. Treatment should now consist of
8. 1- arthroscopic acromioplasty.
9. 2- biceps tenodesis.
10. 3- open subscapularis lengthening and capsular release.
11. 4- humeral head replacement.
12. 5- derotational humeral osteotomy.
1. answer
1. back
1. Question 01.246
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Bigliani LU: Glenohumeral instability repairs: Complications and failures, in Bigliani LU (ed): The Unstable Shoulder. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 99-106. MacDonald PB, Hawkins RJ, Fowler PJ, Miniaci A: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
1. 01.247 What statistical test should be used to determine whether a significant
2. difference exists between the means of more than two independent samples
3. with normal distributions?
4. 1- Student's t test
5. 2- Analysis of variance
6. 3- Regression analysis
7. 4- Chi-square test
8. 5- Kruskal-Wallis test
1. answer
1. back
1. Question 01.247
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 623-665. Freedman KB, Bernstein J: Sample size and statistical power in clinical orthopaedic research. J Bone Joint Surg Am 1999;81:1454-1460.
1. 01.248 A female patient is most likely the victim of domestic abuse when the
2. 1- injury is inconsistent with the offered explanation.
3. 2- spouse does not express any interest in the patient's injuries.
4. 3- patient expresses an overly animated affect.
5. 4- patient has a lower socioeconomic status.
6. 5- patient is eager to leave the hospital or clinic.
1. answer
1. back
1. Question 01.248
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Zillmer DA: Domestic violence: The role of the orthopaedic surgeon in identification and treatment. J Am Acad Orthop Surg 2000;8:91-96.
1. 01.249 A varus malreduction of a comminuted talar neck fracture will result in
2. 1- varus hindfoot and decreased subtalar motion.
3. 2- increased contact loading of the posterior facet.
4. 3- subtalar instability.
5. 4- anterior ankle impingement.
6. 5- talonavicular subluxation.
1. answer
1. back
1. Question 01.249
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect in the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567. Sangeorzan BJ, Wagner UA, Harrington RIM, Tencer AF: Contact characteristics of the subtalar joint: The effect of talar neck misalignment. J Orthop Res 1992;10:544.-551.
1. 01.250 While performing a revision total knee replacement with a trial component in
2. place, it is noted that the knee has full extension but is loose in flexion. To
3. resolve this flexion-extension discrepancy, the surgeon should
4. 1- use a thicker polyethylene insert.
5. 2- use a larger femoral component with posterior condyle metallic wedges.
6. 3- use a more constrained polyethylene insert.
7. 4- release the posterior capsule.
8. 5- cut more posterior slope on the tibia.
1. answer
1. back
1. Question 01.250
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 323-327.
1. 01.251 During harvest of an anterior iliac crest bone graft, what nerve is at greatest
2. risk for injury?
3. 1- Lateral femoral cutaneous
4. 2- Inguinal
5. 3- Genitofemoral
6. 4- Ilioinguinal
7. 5- Femoral
1. answer
1. back
1. Question 01.251
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, p 1736.
1. 01.252 What structure is at greatest risk for injury when the anterolateral portal is used
2. for ankle arthroscopy?
3. 1- Superficial peroneal nerve
4. 2- Saphenous nerve
5. 3- Sural nerve
6. 4- Deep peroneal nerve
7. 5- Peroneal artery
1. answer
1. back
1. Question 01.252
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Ferkel RD: Arthroscopy of the foot and ankle, in Coughlin MJ, Mate RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1257-1268.
1. 01.253 A 53-year-old patient sustains a traumatic anterior dislocation of the
2. glenohumeral joint. The glenohumeral joint is reduced, and postreduction
3. radiographs show a concentric reduction and no evidence of fracture. One
4. week later, the patient cannot actively abduct his arm; however, passive
5. abduction is normal. What is the most likely cause for the lack of active
6. shoulder abduction?
7. 1- Axillary nerve injury
8. 2- Brachial plexus injury
9. 3- Deltoid muscle avulsion
10. 4- Rotator cuff tear
11. 5- Glenoid labral tear
1. answer
1. back
1. Question 01.253
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Stayner LR, Cummings J, Andersen J, Jobe CM: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
1. 01.254 What patient-related risk factor is associated with an increased risk of
2. dislocation in total hip arthroplasty?
3. 1- Obesity
4. 2- Smoking
5. 3- Alcohol intake
6. 4- Male gender
7. 5- Use of systemic steroids
1. answer
1. back
1. Question 01.254
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Espehaug B, Havelin LL Engesaester LB, Langeland N, Vollset SE: Patient related risk factors for early revision of total hip replacements: A population register-based case-control study of 674 revised hips. Acts Orthop Scand 1997;68:207-215. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
1. 01.255 The poor results following surgical treatment of posterior wall acetabular
2. fractures are most commonly associated with
3. 1- sciatic nerve injury.
4. 2- articular comminution.
5. 3- heterotopic ossification.
6. 4- deep venous thrombosis.
7. 5- osteonecrosis of the femoral head.
1. answer
1. back
1. Question 01.255
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Browner BD, Jupiter JB, Levine AM Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders 1998, pp 1204-1208. Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78:1632-1645. Saterbak AM, Marsh JL, Nepola JV, Brandser EA, Turbett T: Clinical failure after posterior wall acetabular fractures: The influence of initial fracture patterns. J Orthop Trauma 2000;14:230-237.
1. 01.256 Which of the following conditions is considered a common clinical
2. manifestation of multiple hereditary exostoses?
3. 1- Radial bowing
4. 2- Scoliosis
5. 3- Acetabular dysplasia
6. 4- Genu varum
7. 5- Dwarfism
1. answer
1. back
1. Question 01.256
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Stanton RP, Hansen MO: Function of the upper extremities in hereditary multiple exostoses. J Bone Joint Surg Am 1969;78:68-573. Arms DM, Strecker WB, Manske PR, Schoenecker PL: Management of forearm deformity in multiple hereditary osteochondromatosis. J Pediatr Orthop 1997;17:450-454. Schmale GA, Conrad EU III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
1. 01.257 When comparing women who sustained a pelvic ring fracture with women
2. who have multiple injuries without a pelvic ring fracture, those with a pelvic
3. fracture have been found to have a higher subsequent rate of
4. 1- miscarriage.
5. 2- infertility.
6. 3- depression.
7. 4- failure to achieve physiologic sexual arousal.
8. 5- urinary difficulties.
1. answer
1. back
1. Question 01.257
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Copeland CE, Bosse MJ, McCarthy ML, et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
1. 01.258 When performing palmar fasciectomy for Dupuytren's contracture, what other
2. procedure should not be performed at the same time?
3. 1- Trigger finger release
4. 2- Intraoperative digital nerve laceration repair
5. 3- Knuckle pad excision
6. 4- Proximal interphalangeal joint arthrodesis
7. 5- Carpal tunnel release
1. answer
1. back
1. Question 01.258
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 271-279. Nissenbaum M, Kleinert HE: Treatment considerations in carpal tunnel syndrome with coexistent Dnpuytren's disease. J Hand Surg Am 1980;5:544-547.
1. 01.259 A 44-year-old man has persistent anteromedial joint line pain after sustaining
2. multiple ankle sprains. At the time of surgery, thickening of the deltoid
3. ligament on its most anterior aspect is noted. What fascicle of the deltoid
4. ligament is involved with this anterior impingement?
5. 1- Anterior tibial
6. 2- Anterior tibiotalar
7. 3- Tibionavicular
8. 4- Tibiocalcaneal
9. 5- Talonavicular
1. answer
1. back
1. Question 01.259
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Egol KA, Parisian JS: Impingement syndrome of the ankle caused by a medial meniscoid lesion. Arthroscopy 1997;13:522-525. Mosier-La Clair SM, Monroe MT, Manoli A: Medial impingement syndrome of the anterior tibiotalar fascicle of the deltoid ligament on the talus. Foot Ankle Int 2000;21:385-391.
1. 01.260 What metabolic bone disease is associated with the presence of virus-like
2. inclusion bodies found in the osteoclast?
3. 1- X-linked hypophosphatemic rickets
4. 2- Fanconi's syndrome
5. 3- Osteopetrosis
6. 4- Osteomalacia
7. 5- Paget's disease of bone
1. answer
1. back
1. Question 01.260
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Beaty 1H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Hadjipavlou A, Lander P: Paget disease of the spine. J Bone Joint Surg Am 1991;73:1376-1381. Delmas PD, Mennier P1: The management of Paget's disease of bone. N Engl J Med 1997;336:58-566.
1. 01.261 Pseudoachondroplasia, characterized by disproportionate short-limbed
2. dwarfism and ligamentous laxity, is caused by a deletion or alteration in the
3. gene encoding what protein?
4. 1- Fibroblast growth factor receptor
5. 2- Cartilage oligomeric matrix protein
6. 3- Type 11 collagen
7. 4- Type IX collagen
8. 5- Parathyroid hormone receptor
1. answer
1. back
1. Question 01.261
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 112-131.
1. 01.262 Semmes-Weinstein monofilaments are used to test the foot for abnormal
2. sensory threshold in patients with diabetes mellitus. Loss of protective
3. sensation is the inability to feel
4. 1- the 4.17 filament.
5. 2- the 5.07 filament.
6. 3- the 6.10 filament.
7. 4- 5 g of pressure.
8. 5- 15 g of pressure.
1. answer
1. back
1. Question 01.262
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Jeng C, Michelson J, Mizel M: Sensory thresholds of normal human feet. Foot Ankle Int 2000;21:501-504. Rith-Najarian SJ, Stolusky T, Gohdes DM: Identifying diabetic patients at him risk for lower-extremity amputation in a primary health care setting: A prospective evaluation of simple screening criteria. Diabetes Care 1992;15:1386-1389.
1. 01.263 A 13-year-old girl with scoliosis has mild intermittent back pain. A bone scan,
2. CT scan, and an MRI scan would most likely reveal which of the following
3. conditions?
4. 1- Spondylolysis
5. 2- Spondylolisthesis
6. 3- Scheuermann's disorder
7. 4- Slipped vertebral apophysis
8. 5- No other condition
1. answer
1. back
1. Question 01.263
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368.
1. 01.264 What is the most common cause of failure of the pars interarticularis in
2. spondylolysis?
3. 1- Repetitive hyperextension
4. 2- Repetitive axial loading
5. 3- Repetitive torsion
6. 4- Single-load extension
7. 5- Single-load flexion
1. answer
1. back
1. Question 01.264
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Bradford D.S: Spondylolysis and spondylolisthesis in children and adolescents: Current concepts in management, in Bradford DS, Hensinger RM (eds): The Pediatric Spine. New York, NY, Thieme, 1985, pp 403-423. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 1337-1347.
1. 01.265 What is the advantage of impaction allografting during femoral revision hip
2. arthroplasty?
3. 1- Lower cost
4. 2- Lower incidence of femoral component subsidence
5. 3- Lower risk of femoral fracture and perforation
6. 4- Ability to reconstitute bone stock
7. 5- Delivery of depot antibiotics
1. answer
1. back
1. Question 01.265
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Inst Course Lect 2000;49:111-118.
1. 01.266 Which of the following is considered a characteristic of a prosthesis used for a
2. Syme's amputation?
3. 1- No auxiliary suspension mechanisms
4. 2- Posterior window
5. 3- Non-weight-bearing distal portion
6. 4- Patellar tendon bearing
7. 5- Availability of multiple foot prostheses
1. answer
1. back
1. Question 01.266
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1003-1004.
1. 01.267 A 62-year-old woman who plays tennis underwent an acromioplasty and
2. rotator cuff repair using four suture anchors 1 month ago. Three days ago, she
3. was allowed to begin using her arm to lift light weights, but she now reports a
4. dramatic increase in pain and is unable to elevate the arm. The next most
5. appropriate step in management should consist of
6. 1- further immobilization and discontinuation of physical therapy.
7. 2- plain radiography.
8. 3- MRI.
9. 4- arthrography.
10. 5- electromyography of the axillary and suprascapular nerves.
1. answer
1. back
1. Question 01.267
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Hanyman DT II: Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am 1991;73:982-989. Barber FA, Herbert MA, Click JN: The ultimate strength of suture anchors. Arthroscopy 1995;11:21-28.
1. 01.268 Which of the following factors will increase the rigidity of an external fixator?
2. 1- Decreased pin diameter
3. 2- Decreased pin number
4. 3- Increased pin spread within a segment
5. 4- Increased bone-to-rod distance
6. 5- Increased distance between fragment pin sets
1. answer
1. back
1. Question 01.268
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA. Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.269 The likelihood of a contralateral slip occurring in a boy with a unilateral
2. slipped capital femoral epiphysis is greatest when combined with which of the
3. following risk factors?
4. 1- An unstable slip
5. 2- A chronic slip
6. 3- A grade III slip
7. 4- Patient age of 11 years
8. 5- Patient age of 13 years
1. answer
1. back
1. Question 01.269
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Stasikelis PJ, Sullivan CM, Phillips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155. Loder RT, Aronson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.
1. 01.270 During intramedullary tibial nailing, compartment pressures in the leg are most
2. elevated by the use of
3. 1- reaming.
4. 2- continuous traction.
5. 3- a medial starting point.
6. 4- a lateral starting point.
7. 5- a solid nail.
1. answer
1. back
1. Question 01.270
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Shakespeare DT, Henderson NJ: Compartmental pressure changes during calcaneal traction in tibial fractures. J Bone Joint Surg Br 1982;64:498-499. McQueen MM, Christie J, Court-Brown CM: Compartment pressures after intramedullary nailing of the tibia. J Bone Joint Surg Br 1990;72:395-397.
1. 01.271 Surgical intervention is first indicated for Dupuytren's disease when which of
2. the following findings is present?
3. 1- A metacarpophalangeal joint contracture that is greater than 60° and a proximal
4. interphalangeal joint contracture of any degree
5. 2- A metacarpophalangeal joint contracture and a proximal interphalangeal joint
6. contracture that are each greater than 40°
7. 3- A metacarpophalangeal joint contracture of 30° and a proximal interphalangeal joint
8. contracture of any degree
9. 4- A metacarpophalangeal joint contracture of any degree and a proximal
10. interphalangeal joint contracture that is greater than or equal to 30°
11. 5- Any contracture of either the metacarpophalangeal or proximal interphalangeal joints
1. answer
1. back
1. Question 01.271
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. McFarlane RM, Botz JS: The results of treatment, in McFarlane RM, McGrouther DA, Flint MA (eds): Dupuytren's Disease: Biology and Treatment (The hand and upper limb series, vol 5). Edinburgh, Scotland, 1990, pp 387-412.
1. 01.272 Following a left-sided approach for surgery on the anterior cervical spine, the
2. patient reports a drooping left upper eyelid and dryness on the left side of the
3. face. Which of the following structures has most likely been injured?
4. 1- Recurrent laryngeal nerve
5. 2- Superior laryngeal nerve
6. 3- Hypoglossal nerve
7. 4- Phrenic nerve
8. 5- Sympathetic chain
1. answer
1. back
1. Question 01.272
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 1427-1438. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
1. 01.273 An 18-year-old man with recurrent bilateral ankle instability reports that his
2. symptoms have been slowly progressing. He denies problems with
3. coordination, but he notes easy fatigability when he types. History reveals that
4. his grandmother had "disfigured feet." Examination reveals bilateral cavovarus
5. feet and peroneal weakness. He has intrinsic muscular weakness in his hands.
6. To confirm the diagnosis, which of the following studies should be obtained?
7. 1- Radiographs of the spine
8. 2- Electrocardiography
9. 3- Electromyography
10. 4- MRI of the feet
11. 5- CBC
1. answer
1. back
1. Question 01.273
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
1. 01.274 Which of the following is considered the most common complication of an
2. extensive medial release for resistant medial epicondylitis?
3. 1- Ulnar palsy
4. 2- Medial elbow instability
5. 3- Wrist flexion weakness
6. 4- Forearm pronation weakness
7. 5- Elbow flexor weakness
1. answer
1. back
1. Question 01.274
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaway GH, Field LD, Deng ML et al: Biomechanical evaluation of the medial collateral ligament of the elbow. J Bone Joint Surg Am 1997;79:1223-1231. Vangsness CT Jr, Jobe FW: Surgical treatment of medial epicondylitis: Results in 35 elbows. J Bone Joint Surg Br 1991;73:409-411.
1. 01.275 What neurosensory receptor is responsible for detecting the sensation of a
2. vibration?
3. 1- Merkel cells
4. 2- Pacinian corpuscles
5. 3- Ruffini end organs
6. 4- Meissner corpuscles
7. 5- Free-ending nerve fibers
1. answer
1. back
1. Question 01.275
2. Answer = 3
1. back to this question
1. End of 2001 Exam
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 325-396.
[**for more mcqs in the bank**](https://hutaifortho.com/942#content)
**[ORTHOPEDIC MCQS ONLINE BANK OITE 20](http://www.hutaifortho.com/1179)**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 97](http://www.hutaifortho.com/1178)**
**[ORTHOPEDIC MCQS BANK OITE 96](http://www.hutaifortho.com/1177)**
**[ORTHOPEDIC MCQS BANK OITE 99](http://www.hutaifortho.com/1176)**
**[ORTHOPEDIC MCQS BANK OITE98](http://www.hutaifortho.com/1175)**
[ORTHOPEDIC MCQS ONLINE OB PATHOLOGY 1A](http://www.hutaifortho.com/1080)
**[ORTHOPEDIC MCQS ONLINE OB HAND 1A](http://www.hutaifortho.com/1078)**
[Links For. ORTHOPEDICS MCQS QUESTION BANK](http://www.hutaifortho.com/942)
**[ortho mcqs](http://www.hutaifortho.com/934)**
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1D](http://www.hutaifortho.com/933)
[ORTHOPEDIC MCQS ADULT RECONSTRUCTIVE OB 20 1C](http://www.hutaifortho.com/932)
[ORTHOPEDIC MCQS ONLINE OB 20 2B RECONSTRUCTION](http://www.hutaifortho.com/929)
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1A](http://www.hutaifortho.com/928)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2D](http://www.hutaifortho.com/927)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B](http://www.hutaifortho.com/925)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 2A](http://www.hutaifortho.com/924)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D](http://www.hutaifortho.com/923)
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1C](http://www.hutaifortho.com/922)**
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1B](http://www.hutaifortho.com/921)**
**[ORTHOPEDIC MCQS 20OB TRAUMA 1A](http://www.hutaifortho.com/920)**
**[ORTHOPEDIC MCQS ONLINE 010 PEDIATRIC](http://www.hutaifortho.com/919)**
**[ORTHOPEDIC MCQS 010 ONLINE](http://www.hutaifortho.com/918)**
[ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery...](http://www.hutaifortho.com/917)
[ORTHOPEDIC MCQS ONLINE 011 RECONSTRUCTION](http://www.hutaifortho.com/916)
**[ORTHOPEDIC MCQS ONLINE 011 PATHOLOGY](http://www.hutaifortho.com/915)**
**[ORTHOPEDIC MCQS 011 ANATOMY IMAGING](http://www.hutaifortho.com/914)**
**[ORTHOPEDIC MCQS O11 UPPER EXTREMITY](http://www.hutaifortho.com/913)**
**[ORTHOPEDIC MCQS ONLINE 012 SPINE](http://www.hutaifortho.com/912)**
**[ORTHOPEDIC MCQS ONLINE 012 TRAUMA](http://www.hutaifortho.com/911)**
[Orthopedic MCQS online 012 FOOT AND ANKLE](http://www.hutaifortho.com/910)
**[ORTHOPEDIC MCQS ONLINE 013 PEDIATRIC](http://www.hutaifortho.com/909)**
**[ORTHOPEDIC MCQS ONLINE 013 SPORT](http://www.hutaifortho.com/908)**
**[ORTHOPEDIC MCQS ONLINE 013 BASIC](http://www.hutaifortho.com/906)**
[ORTHOPEDIC MCQS ONLINE 014 ANATOMY IMAGING](http://www.hutaifortho.com/905)
[ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY](http://www.hutaifortho.com/904)
**[ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY](http://www.hutaifortho.com/903)**
**[ORTHOPEDIC MCQS ONLINE 015 TRAUMA](http://www.hutaifortho.com/902)**
[ORTHOPEDIC MCQS ONLINE 015 FOOT AND ANKLE e](http://www.hutaifortho.com/901)
**[ORTHOPEDIC MCQS ONLINE 015Spine](http://www.hutaifortho.com/900)**
**[ORTHOPEDIC MCQS ONLINE PEDIATRIC 016](http://www.hutaifortho.com/899)**
[ORTHOPEDIC MCQS ONLINE RECONSTRUCTION 016](http://www.hutaifortho.com/898)
**[ORTHOPEDIC MCQS ONLINE SPORT016](http://www.hutaifortho.com/897)**
**[ORTHOPEDIC MCQS ONLINE HAND 017](http://www.hutaifortho.com/896)**
**[ORTHOPEDIC MCQS ONLINE PATHOLOGY 017](http://www.hutaifortho.com/895)**
[Orthopedic MCQS online Shoulder and Elbow 017](http://www.hutaifortho.com/894)
**[Orthopedic MCQS online Anatomy 017](http://www.hutaifortho.com/893)**
**[Orthopedic MCQS online Basic 018](http://www.hutaifortho.com/892)**
**[Orthopedic MCQS online Spine 0018](http://www.hutaifortho.com/891)**
**[Orthopedic MCQS Trauma 0018](http://www.hutaifortho.com/890)**
**[Orthopedic MCQS RECON0019](http://www.hutaifortho.com/889)**
**[Orthopedic Mcqs Sport 0019](http://www.hutaifortho.com/888)**
**[Orthopedics Mcqs Hand0019](http://www.hutaifortho.com/887)**
**[ORTHO MCQS RECON019](http://www.hutaifortho.com/886)**
**[HAND AND WRIST MCQS 019](http://www.hutaifortho.com/885)**
**[ORTHO MCQS Shoulder and Elbow 0192](http://www.hutaifortho.com/884)**
**[ORTHO MCQS Shoulder and Elbow 019](http://www.hutaifortho.com/883)**
**[ORTHO MCQS PEDS 10](http://www.hutaifortho.com/882)**
**[ORTHO MCQS SPORT 10](http://www.hutaifortho.com/881)**
**[ORTHO MCQS BANK 011 FREE 04](http://www.hutaifortho.com/880)**
**[ORTHO MCQS BANK 011 FREE 03](http://www.hutaifortho.com/879)**
**[ORTHO MCQS 011 FREE BANK 02](http://www.hutaifortho.com/878)**
**[ORTHO MCQS 011 FREE BANK](http://www.hutaifortho.com/877)**
[Orthopedic MCQS online Hip and knee ADULT...](http://www.hutaifortho.com/876)
**[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://www.hutaifortho.com/875)**
**[ORTHOPEDIC MCQS OB 20 BASIC5](http://www.hutaifortho.com/874)**
**[ORTHOPEDIC MCQS OB 20 BASIC7](http://www.hutaifortho.com/873)**
**[ORTHOPEDIC MCQS OB 20 BASIC 6](http://www.hutaifortho.com/872)**
**[ORTHOPEDIC MCQS OB 20 BASIC 44](http://www.hutaifortho.com/871)**
**[ORTHOPEDIC MCQS OB 20 BASIC 4](http://www.hutaifortho.com/870)**
**[ORTHOPEDIC MCQS OB 20 BASIC 3](http://www.hutaifortho.com/869)**
**[ORTHOPEDIC MCQS OB 20 BASIC 2](http://www.hutaifortho.com/868)**
**[ORTHOPEDIC MCQS OB 20 BASIC 1](http://www.hutaifortho.com/867)**
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://www.hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://www.hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://www.hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://www.hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://www.hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://www.hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://www.hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02](http://www.hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://www.hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://www.hutaifortho.com/856)
**[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://www.hutaifortho.com/855)**
**[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://www.hutaifortho.com/854)**
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://www.hutaifortho.com/853)
**[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://www.hutaifortho.com/852)**
**[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://www.hutaifortho.com/851)**
**[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://www.hutaifortho.com/850)**
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://www.hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://www.hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://www.hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://www.hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://www.hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://www.hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://www.hutaifortho.com/843)
**[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://www.hutaifortho.com/842)**
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://www.hutaifortho.com/841)
**[ONLINE ORTHOPEDIC MCQS SPORT07](http://www.hutaifortho.com/840)**
**[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://www.hutaifortho.com/839)**
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://www.hutaifortho.com/838)
**[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://www.hutaifortho.com/837)**
**[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://www.hutaifortho.com/836)**
**[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://www.hutaifortho.com/835)**
**[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://www.hutaifortho.com/834)**
[Orthopedic MCQS online sports Medicine](http://www.hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://www.hutaifortho.com/832)
**[Orthopedic MCQS online Hip and knee](http://www.hutaifortho.com/831)**
**[online orthopedic mcqs](http://www.hutaifortho.com/830)**
[Shoulder and elbow: Mcqs AND EMQS Answers](http://www.hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://www.hutaifortho.com/765)
**[Hand and wrist: Answers MCQS EMQS](http://www.hutaifortho.com/764)**
[Hand and wrist: MCQ AND EMQ Questions](http://www.hutaifortho.com/763)
**[2021 SHOULDER AND ELBOW MCQS FREE](http://www.hutaifortho.com/689)**
[Pediatric Orthopaedic MCQS Self-Assessment...](http://www.hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://www.hutaifortho.com/684)
**[Foot and Ankle free MCQS2020 Online](http://www.hutaifortho.com/681)**
**[UPDATED ORTHOPEDIC MCQS](http://www.hutaifortho.com/680)**
[FREE Orthopedics MCQS 2022 1951.-2000.](http://www.hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://www.hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://www.hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://www.hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://www.hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://www.hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://www.hutaifortho.com/668)
**[FREE Orthopedics MCQS 2022 1651-1700](http://www.hutaifortho.com/667)**
[FREE Orthopedics MCQS 2022 1601-1650.](http://www.hutaifortho.com/666)
**[ORTHOPEDIC MCQS FREE 2023](http://www.hutaifortho.com/665)**
**[FREE Orthopedics MCQS 2022 1551-1600](http://www.hutaifortho.com/664)**
**[FREE Orthopedics MCQS 2022 1501-1550](http://www.hutaifortho.com/663)**
**[FREE Orthopedics MCQS 2022 1451-1500](http://www.hutaifortho.com/662)**
**[FREE Orthopedics MCQS 2022 1401-1450](http://www.hutaifortho.com/661)**
[FREE Orthopedics MCQS 2022 1351 -1400](http://www.hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://www.hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://www.hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://www.hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://www.hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://www.hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://www.hutaifortho.com/653)
**[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://www.hutaifortho.com/652)**
**[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://www.hutaifortho.com/651)**
**[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://www.hutaifortho.com/650)**
**[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://www.hutaifortho.com/649)**
**[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://www.hutaifortho.com/647)**
**[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://www.hutaifortho.com/646)**
**[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://www.hutaifortho.com/645)**
**[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://www.hutaifortho.com/644)**
**[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://www.hutaifortho.com/643)**
**[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://www.hutaifortho.com/642)**
**[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://www.hutaifortho.com/641)**
**[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://www.hutaifortho.com/640)**
**[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://www.hutaifortho.com/639)**
**[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://www.hutaifortho.com/638)**
**[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://www.hutaifortho.com/637)**
**[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://www.hutaifortho.com/636)**
**[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://www.hutaifortho.com/635)**
**[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://www.hutaifortho.com/634)**
**[FREE Orthopedics MCQS 2022 51-100](http://www.hutaifortho.com/633)**
**[Orthopedics Hyperguide MCQ 1-50](http://www.hutaifortho.com/631)**
**for more mcqs in the bank**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 20](http://www.hutaifortho.com/1179)**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 97](http://www.hutaifortho.com/1178)**
**[ORTHOPEDIC MCQS BANK OITE 96](http://www.hutaifortho.com/1177)**
**[ORTHOPEDIC MCQS BANK OITE 99](http://www.hutaifortho.com/1176)**
**[ORTHOPEDIC MCQS BANK OITE98](http://www.hutaifortho.com/1175)**
[ORTHOPEDIC MCQS ONLINE OB PATHOLOGY 1A](http://www.hutaifortho.com/1080)
**[ORTHOPEDIC MCQS ONLINE OB HAND 1A](http://www.hutaifortho.com/1078)**
[Links For. ORTHOPEDICS MCQS QUESTION BANK](http://www.hutaifortho.com/942)
**[ortho mcqs](http://www.hutaifortho.com/934)**
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1D](http://www.hutaifortho.com/933)
[ORTHOPEDIC MCQS ADULT RECONSTRUCTIVE OB 20 1C](http://www.hutaifortho.com/932)
[ORTHOPEDIC MCQS ONLINE OB 20 2B RECONSTRUCTION](http://www.hutaifortho.com/929)
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1A](http://www.hutaifortho.com/928)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2D](http://www.hutaifortho.com/927)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B](http://www.hutaifortho.com/925)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 2A](http://www.hutaifortho.com/924)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D](http://www.hutaifortho.com/923)
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1C](http://www.hutaifortho.com/922)**
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1B](http://www.hutaifortho.com/921)**
**[ORTHOPEDIC MCQS 20OB TRAUMA 1A](http://www.hutaifortho.com/920)**
**[ORTHOPEDIC MCQS ONLINE 010 PEDIATRIC](http://www.hutaifortho.com/919)**
**[ORTHOPEDIC MCQS 010 ONLINE](http://www.hutaifortho.com/918)**
[ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery...](http://www.hutaifortho.com/917)
[ORTHOPEDIC MCQS ONLINE 011 RECONSTRUCTION](http://www.hutaifortho.com/916)
**[ORTHOPEDIC MCQS ONLINE 011 PATHOLOGY](http://www.hutaifortho.com/915)**
**[ORTHOPEDIC MCQS 011 ANATOMY IMAGING](http://www.hutaifortho.com/914)**
**[ORTHOPEDIC MCQS O11 UPPER EXTREMITY](http://www.hutaifortho.com/913)**
**[ORTHOPEDIC MCQS ONLINE 012 SPINE](http://www.hutaifortho.com/912)**
**[ORTHOPEDIC MCQS ONLINE 012 TRAUMA](http://www.hutaifortho.com/911)**
[Orthopedic MCQS online 012 FOOT AND ANKLE](http://www.hutaifortho.com/910)
**[ORTHOPEDIC MCQS ONLINE 013 PEDIATRIC](http://www.hutaifortho.com/909)**
**[ORTHOPEDIC MCQS ONLINE 013 SPORT](http://www.hutaifortho.com/908)**
**[ORTHOPEDIC MCQS ONLINE 013 BASIC](http://www.hutaifortho.com/906)**
[ORTHOPEDIC MCQS ONLINE 014 ANATOMY IMAGING](http://www.hutaifortho.com/905)
[ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY](http://www.hutaifortho.com/904)
**[ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY](http://www.hutaifortho.com/903)**
**[ORTHOPEDIC MCQS ONLINE 015 TRAUMA](http://www.hutaifortho.com/902)**
[ORTHOPEDIC MCQS ONLINE 015 FOOT AND ANKLE e](http://www.hutaifortho.com/901)
**[ORTHOPEDIC MCQS ONLINE 015Spine](http://www.hutaifortho.com/900)**
**[ORTHOPEDIC MCQS ONLINE PEDIATRIC 016](http://www.hutaifortho.com/899)**
[ORTHOPEDIC MCQS ONLINE RECONSTRUCTION 016](http://www.hutaifortho.com/898)
**[ORTHOPEDIC MCQS ONLINE SPORT016](http://www.hutaifortho.com/897)**
**[ORTHOPEDIC MCQS ONLINE HAND 017](http://www.hutaifortho.com/896)**
**[ORTHOPEDIC MCQS ONLINE PATHOLOGY 017](http://www.hutaifortho.com/895)**
[Orthopedic MCQS online Shoulder and Elbow 017](http://www.hutaifortho.com/894)
**[Orthopedic MCQS online Anatomy 017](http://www.hutaifortho.com/893)**
**[Orthopedic MCQS online Basic 018](http://www.hutaifortho.com/892)**
**[Orthopedic MCQS online Spine 0018](http://www.hutaifortho.com/891)**
**[Orthopedic MCQS Trauma 0018](http://www.hutaifortho.com/890)**
**[Orthopedic MCQS RECON0019](http://www.hutaifortho.com/889)**
**[Orthopedic Mcqs Sport 0019](http://www.hutaifortho.com/888)**
**[Orthopedics Mcqs Hand0019](http://www.hutaifortho.com/887)**
**[ORTHO MCQS RECON019](http://www.hutaifortho.com/886)**
**[HAND AND WRIST MCQS 019](http://www.hutaifortho.com/885)**
**[ORTHO MCQS Shoulder and Elbow 0192](http://www.hutaifortho.com/884)**
**[ORTHO MCQS Shoulder and Elbow 019](http://www.hutaifortho.com/883)**
**[ORTHO MCQS PEDS 10](http://www.hutaifortho.com/882)**
**[ORTHO MCQS SPORT 10](http://www.hutaifortho.com/881)**
**[ORTHO MCQS BANK 011 FREE 04](http://www.hutaifortho.com/880)**
**[ORTHO MCQS BANK 011 FREE 03](http://www.hutaifortho.com/879)**
**[ORTHO MCQS 011 FREE BANK 02](http://www.hutaifortho.com/878)**
**[ORTHO MCQS 011 FREE BANK](http://www.hutaifortho.com/877)**
[Orthopedic MCQS online Hip and knee ADULT...](http://www.hutaifortho.com/876)
**[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://www.hutaifortho.com/875)**
**[ORTHOPEDIC MCQS OB 20 BASIC5](http://www.hutaifortho.com/874)**
**[ORTHOPEDIC MCQS OB 20 BASIC7](http://www.hutaifortho.com/873)**
**[ORTHOPEDIC MCQS OB 20 BASIC 6](http://www.hutaifortho.com/872)**
**[ORTHOPEDIC MCQS OB 20 BASIC 44](http://www.hutaifortho.com/871)**
**[ORTHOPEDIC MCQS OB 20 BASIC 4](http://www.hutaifortho.com/870)**
**[ORTHOPEDIC MCQS OB 20 BASIC 3](http://www.hutaifortho.com/869)**
**[ORTHOPEDIC MCQS OB 20 BASIC 2](http://www.hutaifortho.com/868)**
**[ORTHOPEDIC MCQS OB 20 BASIC 1](http://www.hutaifortho.com/867)**
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://www.hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://www.hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://www.hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://www.hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://www.hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://www.hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://www.hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02](http://www.hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://www.hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://www.hutaifortho.com/856)
**[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://www.hutaifortho.com/855)**
**[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://www.hutaifortho.com/854)**
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://www.hutaifortho.com/853)
**[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://www.hutaifortho.com/852)**
**[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://www.hutaifortho.com/851)**
**[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://www.hutaifortho.com/850)**
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://www.hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://www.hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://www.hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://www.hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://www.hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://www.hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://www.hutaifortho.com/843)
**[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://www.hutaifortho.com/842)**
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://www.hutaifortho.com/841)
**[ONLINE ORTHOPEDIC MCQS SPORT07](http://www.hutaifortho.com/840)**
**[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://www.hutaifortho.com/839)**
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://www.hutaifortho.com/838)
**[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://www.hutaifortho.com/837)**
**[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://www.hutaifortho.com/836)**
**[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://www.hutaifortho.com/835)**
**[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://www.hutaifortho.com/834)**
[Orthopedic MCQS online sports Medicine](http://www.hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://www.hutaifortho.com/832)
**[Orthopedic MCQS online Hip and knee](http://www.hutaifortho.com/831)**
**[online orthopedic mcqs](http://www.hutaifortho.com/830)**
[Shoulder and elbow: Mcqs AND EMQS Answers](http://www.hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://www.hutaifortho.com/765)
**[Hand and wrist: Answers MCQS EMQS](http://www.hutaifortho.com/764)**
[Hand and wrist: MCQ AND EMQ Questions](http://www.hutaifortho.com/763)
**[2021 SHOULDER AND ELBOW MCQS FREE](http://www.hutaifortho.com/689)**
[Pediatric Orthopaedic MCQS Self-Assessment...](http://www.hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://www.hutaifortho.com/684)
**[Foot and Ankle free MCQS2020 Online](http://www.hutaifortho.com/681)**
**[UPDATED ORTHOPEDIC MCQS](http://www.hutaifortho.com/680)**
[FREE Orthopedics MCQS 2022 1951.-2000.](http://www.hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://www.hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://www.hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://www.hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://www.hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://www.hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://www.hutaifortho.com/668)
**[FREE Orthopedics MCQS 2022 1651-1700](http://www.hutaifortho.com/667)**
[FREE Orthopedics MCQS 2022 1601-1650.](http://www.hutaifortho.com/666)
**[ORTHOPEDIC MCQS FREE 2023](http://www.hutaifortho.com/665)**
**[FREE Orthopedics MCQS 2022 1551-1600](http://www.hutaifortho.com/664)**
**[FREE Orthopedics MCQS 2022 1501-1550](http://www.hutaifortho.com/663)**
**[FREE Orthopedics MCQS 2022 1451-1500](http://www.hutaifortho.com/662)**
**[FREE Orthopedics MCQS 2022 1401-1450](http://www.hutaifortho.com/661)**
[FREE Orthopedics MCQS 2022 1351 -1400](http://www.hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://www.hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://www.hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://www.hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://www.hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://www.hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://www.hutaifortho.com/653)
**[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://www.hutaifortho.com/652)**
**[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://www.hutaifortho.com/651)**
**[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://www.hutaifortho.com/650)**
**[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://www.hutaifortho.com/649)**
**[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://www.hutaifortho.com/647)**
**[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://www.hutaifortho.com/646)**
**[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://www.hutaifortho.com/645)**
**[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://www.hutaifortho.com/644)**
**[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://www.hutaifortho.com/643)**
**[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://www.hutaifortho.com/642)**
**[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://www.hutaifortho.com/641)**
**[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://www.hutaifortho.com/640)**
**[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://www.hutaifortho.com/639)**
**[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://www.hutaifortho.com/638)**
**[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://www.hutaifortho.com/637)**
**[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://www.hutaifortho.com/636)**
**[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://www.hutaifortho.com/635)**
**[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://www.hutaifortho.com/634)**
**[FREE Orthopedics MCQS 2022 51-100](http://www.hutaifortho.com/633)**
**[Orthopedics Hyperguide](http://www.hutaifortho.com/631)**
6. 1- The arthritis has stabilized.
7. 2- The C1-2 joint has fused.
8. 3- The patient has been wearing a cervical collar.
9. 4- Medical advancements have been made in the management of arthritis.
10. 5- Basilar impression (atlantoaxial impaction) has developed.
1. answer
1. back
1. Question 01.87
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Oda T, Fujiwara K, Yonenobu K, Azuma B, Ochi T: Natural course of cervical spine lesions in rheumatoid arthritis. Spine 1995;20:1128-1135.
1. 01.88 A woman with degenerative arthritis and a fixed genu valgum deformity of 17°
2. undergoes primary total knee arthroplasty under general anesthesia. In the
3. recovery room, she is unable to dorsiflex her foot. Immediate management
4. should include
5. 1- fasciotomies.
6. 2- surgical nerve decompression.
7. 3- flexion of the knee.
8. 4- continuous passive motion.
9. 5- electromyography.
1. answer
1. back
1. Question 01.88
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mont MA, Dellon AL, Chen F, Hungerford MW, Krackow KA, Hungerford DS: The operative treatment of peroneal nerve palsy. J Bone Joint Surg Am 1996;78:863-869. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
1. 01.89 A 30-year-old professional soccer player sustains a midshaft fracture of the tibia
2. and fibula. History reveals that the patient underwent a successful anterior
3. cruciate ligament reconstruction with central one third bone-patellar tendon-bone
4. autograft and graft fixation with interference screws 2 years ago. Figures 22a and
5. 22b show the pre-and postoperative radiograph. What is the most likely
6. postoperative complication in this patient?
7. 1- Loss of graft fixation
8. 2- Fracture through the tibial
9. tunnel
10. 3- Galvanic corrosion
11. (battery effect)
12. 4- Anterior knee pain
13. 5- Saphenous neuralgia
1. answer
1. back
1. A
1. B
1. Figures 22
1. Question 01.89
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Keating JF, Orfaly R, O'Brien PJ: Knee pain after tibial nailing. J Orthop Trauma 1997;11:10-13. Roberts C, John C, Seligson D: Prior anterior cruciate ligament reconstruction complicating intramedullary nailing of a tibia fracture. Arthroscopy 1998;14:779-783.
1. 01.90 Which of the following muscles protracts the shoulder?
2. 1- Serratus anterior
3. 2- Rhomboid major
4. 3- Trapezius
5. 4- Latissimus dorsi
6. 5- Subscapularis
1. answer
1. back
1. Question 01.90
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Kahn JF, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
1. 01.91 Which of the following pharmacologic agents may antagonize the
2. anticoagulation effect of warfarin?
3. 1- Cefamandole
4. 2- Cimetidine
5. 3- Phenytoin
6. 4- Trimethoprim
7. 5- Phenobarbital
1. answer
1. back
1. Question 01.91
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 487-517.
1. 01.92 Figures 23a and 23b show an AP open mouth view and a CT scan at C1-2.
2. Because this is an acute injury with no neurologic deficit, the best course of
3. action should be
4. 1- acute occipital-cervical fusion with rigid instrumentation.
5. 2- use of a soft collar.
6. 3- use of a halo vest for 3 months, followed by assessment for C1-2 instability.
7. 4- a gradual return to activity with no restrictions.
8. 5- flexion-extension radiographs to help determine the need for surgery.
1. answer
1. back
1. A
1. B
1. Figures 23
1. Question 01.92
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Levine AM: Orthopaedic Knowledge Update: Trauma. Rosemont. IL. American Academy of Orthopaedic Surgeons, 1996, pp 317-322.
1. 01.93 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.94 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.95 Intradiscal pressure in the third lumbar disk is least in which of the following
2. positions?
3. 1- Sitting, flexed forward slightly
4. 2- Sitting, straight
5. 3- Laying, supine
6. 4- Standing, straight
7. 5- Standing, slightly extended
1. answer
1. back
1. Question 01.95
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Nachemson A: The lumbar spine: An orthopaedic challenge. Spine 1976;1:59-71. White AA II, Panjabi MM (eds): Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 454-461.
1. 01.96 A 35-year-old man who sustained a grade II open fracture of the right tibia 9
2. months ago underwent reamed intramedullary nailing. The patient continues to
3. have pain with weight bearing. Laboratory studies show a normal WBC and
4. erythrocyte sedimentation rate, and there has been no change in the radiographs
5. in the past 3 months. Current radiographs are shown in Figures 24a and 24b.
6. What is the most likely diagnosis?
7. 1- Delayed union
8. 2- Aseptic nonunion
9. 3- Infected nonunion
10. 4- Synovial pseudarthrosis
11. 5- Failure of the internal fixation device
1. answer
1. back
1. A
1. B
1. Figures 24
1. Question 01.96
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Browner BD, Jupiter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 68-72. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 25-35.
1. 01.97 Figure 25 shows the AP radiograph of a 20-year-old man who sustained a
2. twisting injury to his foot. An attempt at closed reduction is unsuccessful, most
3. likely because of
4. 1- buttonholing of the talar head through the extensor retinaculum.
5. 2- osteochondral fracture of the posterior facet of the talus.
6. 3- interpositioning of the peroneal tendons.
7. 4- interpositioning of the posterior tibial tendon.
8. 5- fracture of the talar neck.
1. answer
1. back
1. Figure 25
1. Question 01.97
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Bellabarba C, Sanders R: Dislocation of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1519-1573. Hansen ST 1r: Foot injuries, in Browner BD, Jupiter JB, Levine AM, Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 2405-2438. DeLee JC, Curtis R: Subtalar dislocation of the foot. J Bone Joint Surg Am 1982;64:433-437.
1. 01/. 98 A 65-year-old man has had progressively worsening pain and limited motion in
2. the left shoulder for the past year. History reveals that he sustained a
3. nondisplaced fracture of the surgical neck of the humerus 10 years ago. Plain
4. radiographs are shown in Figures 26a and 26b. What is the most likely
5. diagnosis?
6. 1- Osteonecrosis
7. 2- Posttraumatic osteoarthritis
8. 3- Rheumatoid arthritis
9. 4- Gouty arthritis
10. 5- Chondrocalcinosis
1. answer
1. back
1. A
1. B
1. Figures 26
1. Question 01.98
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Matsen FA III, Rock-wood CA Jr, Wirth MA, Lippitt SB: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III, Wirth MA, Harryman DT II (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, pp 840-964.
1. 01.99 A 14-year-old basketball player has had activity-related low back pain for the
2. past 6 weeks. Plain radiographs are unremarkable. Selected coronal single-
3. photon emission computed tomography scans are shown in Figure 27. The best
4. course of action should be
5. 1- bilateral facet blocks.
6. 2- brace immobilization for 3 to 6 months.
7. 3- instrumented posterior spinal fusion.
8. 4- a CT-guided needle biopsy.
9. 5- an open incisional biopsy.
1. answer
1. back
1. Figure 27
1. Question 01.99
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Loder RT, Hensinger RN: Fractures of the thoracic and lumbar spine, in Rockwood CA, Wilkins KE, Beaty 1H (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1062-1096. Lonstein JE: Spondylolysis and spondylolisthesis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 717-737. Congeni J, McCulloch J, Swanson K: Lumbar spondylolysis: A study of natural progression in athletes. Am J Sports Med 1997;25:248-253. Lonstein JE: Spondylolisthesis in children: Cause. natural history, and management. Spine 19994:2640-2648. Anderson K, Sarwark JF, Conway JJ, Logue ES, Schafer WI: Quantitative assessment with SPELT imaging of stress injuries of the pats interarticularis and response to bracing. J Pediatr Orthop 2000;20:28-33.
1. 01.100 Which of the following is considered an advantage of the inside-out technique
2. for meniscal repairs compared with the outside-in technique?
3. 1- Improved ultimate knee motion
4. 2- Increased rate of healing
5. 3- Diminished infection rates
6. 4- The ability to achieve proper suture orientation in posterior horn tears
7. 5- Decreased risk of neurologic injury
1. answer
1. back
1. Question 01.100
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Rodeo SA: Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect 2000;49:195-206. Post WR, Akers SR, Kish V: Load to failure of common meniscal repair techniques: Effects of suture technique and suture material. Arthroscopy 1997;13:731-736.
1. 01.101 An anterior (Smith-Peterson) approach to the hip joint uses what internervous
2. plane?
3. 1- Superior gluteal and femoral
4. 2- Superior gluteal and inferior gluteal
5. 3- Femoral and obturator
6. 4- Sciatic and superior gluteal
7. 5- Sciatic and femoral
1. answer
1. back
1. Question 01.101
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp 303-32I.
1. 01.102 A 21-year-old man sustains the acetabular fracture shown in Figures 28a
2. through 28c. The best outcomes following surgical treatment of this fracture
3. have been reported with which
4. of the following surgical
5. approaches?
6. 1- Posterior (Kocher-Langenbeck)
7. 2- Triradiate
8. 3- Extended iliofemoral
9. 4- Modified extensile lateral
10. 5- Ilioinguinal
1. answer
1. back
1. A
1. B
1. Figures 28
1. C
1. Question 01.102
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clip Orthop 1993;292:62-76.
1. 01.103 What type of injury is shown in Figure 29?
2. 1- Compression fracture
3. 2- Burst fracture
4. 3- Flexion-distraction
5. 4- Extension injury
6. 5- Fracture-dislocation
1. answer
1. back
1. Figure 29 (all three)
1. Question 01.103
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Dents F: The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983;8:817-831.
1. 01.104 A 55-year-old patient underwent a total hip arthroplasty with a diaphyseal -
2. locking, fully porous-coated cementless femoral prosthesis 8 years ago.
3. Radiographs reveal a distally fixed stem with distal spot welds and proximal
4. bone loss. The femoral head is located concentrically within the acetabulum.
5. What is the most likely etiology of the bone loss?
6. 1- Bone hypertrophy
7. 2- Stress shielding
8. 3- Osteoporosis
9. 4- Osteolysis
10. 5- Osteonecrosis
1. answer
1. back
1. Question 01.104
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 1995, pp 127-138.
1. 01.105 Endurance strength training has been shown to have which of the following
2. demonstrated physiologic effects?
3. 1- Decreases aerobic capacity
4. 2- Decreases bone mineral density with weight-bearing activities
5. 3- Decreases type II muscle fiber cross-sectional area
6. 4- Increases heart rate at rest
7. 5- Improves blood lipid profiles
1. answer
1. back
1. Question 01.105
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Miszko T, Cress M: A lifetime of fitness, in Clinics in Sports Medicine. Philadelphia, PA, WB Saunders, 2000, vol 19, pp 215-232. Blumenthal JA, Emery CF, Madden DJ, et al: Cardiovascular and behavioral effects of aerobic exercise training in healthy older men and woman. J Gerontol
3. 1989;44:147-157.
1. 01.106 What organ secretes calcitonin?
2. 1- Parathyroid
3. 2- Thyroid
4. 3- Kidney
5. 4- Bone
6. 5- Skin
1. answer
1. back
1. Question 01.106
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Silver JJ, Majeska RJ, Einhorn TA: An update on bone cell biology. Curr Opin Orthop 1994;5:50-59.
1. 01.107 The volar radioscapholunate ligament (ligament of Testut) functions primarily
2. as a
3. 1- neurovascular conduit.
4. 2- stabilizing ligament of the scapholunate interval.
5. 3- stabilizing ligament of the radiocarpal joint.
6. 4- stabilizing ligament of the midcarpal joint.
7. 5- septal ligament contiguous with the interfossal ridge.
1. answer
1. back
1. Question 01.107
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Berger RA, Landsmeer JM: The palmar radiocarpal ligaments: A study of adult and fetal human wrist joints. J Hand Surg Am 1990;15:847-854. Hixson ML, Stewart C: Microvascular anatomy of the radioscapholunate ligament of the wrist. J Hand Surg Am 1990;15:279-282.
1. 01.108 A 19-year-old man reports groin pain after undergoing antegrade nailing of a
2. femoral shaft fracture 3 weeks ago. Figures 30a and 30b show the current
3. radiograph and tomogram. The next most appropriate step in management
4. should consist of
5. 1- observation.
6. 2- electrical stimulation.
7. 3- resection of
8. heterotopic
9. ossification.
10. 4- exchange nailing.
11. 5- screw fixation
12. around the nail.
1. answer
1. back
1. A
1. B
1. Figures 1
1. Question 01.108
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 177-190.
1. 01.109 What is the most common mechanism of injury to the adult spinal cord?
2. 1- Gunshot wounds
3. 2- Falls
4. 3- Motor vehicle accidents
5. 4- Sporting injuries
6. 5- Suicide attempts
1. answer
1. back
1. Question 01.109
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Slucky AV, Eismont FJ: Treatment of acute injury of the cervical spine. Instr Course Lect 1995;44:67-80. Vaccaro AR, An HS, Betz RR, Coder JM, Balderston RA: The management of acute spinal trauma: Prehospital and in-hospital emergency care. Instr Course Lect 1997;46:113-125.
1. 01.110 A 33-year-old woman has had progressive rheumatoid arthritis for the past 12
2. years. Figure 31 shows the postoperative radiograph. What is the most likely
3. long-term symptomatic complication following this procedure?
4. 1- Nonunion of the first metatarsophalangeal joint
5. 2- Chronic infection
6. 3- Plantar callosities
7. 4- Recurrent hammer toe deformity
8. 5- Interphalangeal joint arthritis of the great toe
1. answer
1. back
1. Figure 31
1. Question 01.110
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term follow-up study. J Bone Joint Surg Am 2000;82:322-341. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 293-303.
1. 01.111 A 12-year-old boy is referred for evaluation of a spinal deformity. Examination
2. and history reveal that he and one of his two sisters have numerous light brown
3. birthmarks distributed on all areas of the body. The radiograph shown in Figure
4. 32 reveals a curve that measures 70°. The best course of action should include
5. 1- MRI of the entire spine.
6. 2- brace treatment with a thoracolumbosacral
7. orthosis.
8. 3- posterior spinal fusion and observation for
9. possible crankshaft progression of the curve.
10. 4- a period of observation to determine whether the
11. curve may progress.
12. 5- a renal ultrasound and echocardiogram.
1. answer
1. back
1. Figure 32
1. Question 01.111
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Crawford AH: Neurofibromatosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 619-650. Crawford AH, Gabriel KR: Dysplastic scoliosis: Neurofibromatosis, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA,
3. Lippincott-Raven, 1997, pp 276-298.
1. 01.112 A 33-year-old man fell from a height of 25 feet and sustained a fracture-
2. dislocation of the right elbow. Following closed reduction of the elbow in the
3. emergency department, plain radiographs show a displaced radial neck and a
4. type II coronoid fracture. Examination reveals elbow swelling and wrist
5. tenderness. The neurologic examination is normal. Treatment of the elbow
6. should include
7. 1- excision of the radial head and coronoid fragment.
8. 2- excision of the radial head and open reduction and internal fixation of the coronoid.
9. 3- open reduction and internal fixation of the radial head and excision of the coronoid
10. fragment.
11. 4- open reduction and internal fixation of the radial head and coronoid.
12. 5- replacement of the radial head and excision of the coronoid fragment.
1. answer
1. back
1. Question 01.112
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? Am Acad Orthop Surg 1997;5:1-10. Money BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128. Began W, Money B: Fractures of the coronoid process of the ulna,. J Bone Joint Surg Am 1989;71:1348-1354.
1. 01.113 A 21-year-old patient sustains a fracture of the humeral shaft that is treated as
2. shown in Figures 33a and 33b. The reported incidence of shoulder problems
3. following this method of fracture stabilization is approximately what percent?
4. 1- 0% to 5%
5. 2- 6% to 10%
6. 3- 11% to 15%
7. 4- 16% to 20%
8. 5- 21 % to 25 %
1. answer
1. back
1. A
1. B
1. Figures 33
1. Question 01.113
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Chapman JR, Henley MB, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. McCormack RG, Briers D, Buckley RE, McKee MD, Powell J, Schemitsch EH: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective randomized trial. J Bone Joint Surg Br 2000;82:336-339.
1. 01.114 A revision total knee arthroplasty was performed on a patient who was
2. presumed to have aseptic loosening. Antibiotic-impregnated cement was used
3. at the time of reimplantation. Interface membrane cultures taken routinely at
4. the time of the revision revealed coagulase-negative staphylococci 2 days after
5. surgery. Appropriate management should consist of
6. 1- antibiotic therapy alone.
7. 2- surgical debridement with polyethylene exchange.
8. 3- one-staged exchange of both components.
9. 4- two-staged exchange of both components.
10. 5- knee fusion.
1. answer
1. back
1. Question 01.114
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Segawa H, Tsukayama DT, Kyle RF, Becker DA, Gustilo RB: Infection after total knee arthroplasry: A retrospective study of the treatment of eighty-one infections.
3. J Bone Joint Sur- Am 1999;81:1434-1445.
1. 01.115 A 38-year-old man underwent anterior cruciate ligament reconstruction 12
2. weeks ago. Examination of the knee now reveals active arc of motion from 15°
3. to 80°. Patellar mobility is limited. Radiographs reveal appropriate tunnel
4. placement. Management should now consist of
5. 1- physical therapy.
6. 2- continuous passive motion.
7. 3- open debridement.
8. 4- arthroscopic debridement.
9. 5- manipulation under anesthesia.
1. answer
1. back
1. Question 01.115
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Lindenfeld TN, Wojtys EM, Husain A: Surgical treatment of arthrofibrosis of the knee. Instr Course Lect 2000;49:211-221. Richmond JC, al Assal M: Arthroscopic management of arthrofibrosis of the knee, including infrapatellar contraction syndrome. Arthroscopy 1991;7:144-147.
1. 01.116 Which of the following radiographic findings is most helpful in differentiating
2. chordoma from chondrosarcoma of the sacrum?
3. 1- Bright signal intensity on T1-weighted MRI scan
4. 2- Lytic destruction
5. 3- Midline location
6. 4- Uptake on bone scan
7. 5- Soft-tissue extension
1. answer
1. back
1. Question 01.116
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Smith J, Ludwig RL, Marcove RC: Sacrococcygeal chordoma: A clinicoradiological study of 60 patients. Skeletal Radiol 1987: 16:37-44. Firooznia H, Pinto RS, Lin JP, Baruch HH, Zausner J: Chordoma: Radiologic evaluation of 20 cases. Am J Roentgenol 1976;127:797-805. Temple WJ: Sacral bone tumors. Can J Surg 1994;37:446.
1. 01.117 A 21-year-old student sustains a twisting injury to the ankle. Examination
2. reveals some tenderness over the anteromedial ankle and significant pain and
3. tenderness over the lateral malleolus. A stress radiograph in external rotation is
4. shown in Figure 34. Definitive treatment should consist of
5. 1- weight bearing as tolerated in a functional brace.
6. 2- a short leg cast with no weight bearing for 6 weeks.
7. 3- a long leg cast with no weight bearing for 6 weeks.
8. 4- open reduction and internal fixation of the lateral malleolus.
9. 5- open reduction and internal fixation of the lateral malleolus and repair of the deltoid
10. ligament.
1. answer
1. back
1. Figure 34
1. Question 01.117
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Principles of orthopaedic practice, in Dee R (ed): Ankle Injuries. New York, NY, McGraw Hill, 1997, pp 538-543. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 203-225.
1. 01.118 The mother of a 1-month-old infant reports that he seems to sniff and snort
2. persistently and his temperature has been very labile. Examination reveals a
3. depressed nasal bridge, mild jaundice, and hepatosplenomegaly. Radiographs
4. are shown in Figures 35a and 35b. To help confirm the diagnosis, the best
5. course of action would be to order
6. 1- a rapid plasma reagin (RPR) test.
7. 2- a technetium Tc 99m total body bone scan.
8. 3- CT of the skull and upper cervical spine.
9. 4- needle aspiration of both tibiae.
10. 5- bilateral hip ultrasound studies.
1. answer
1. back
1. A
1. B
1. Figures 35
1. Question 01.118
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 35-46. Brion LP, Manuli M, Rai B, Kresch MJ, Pavlov H, Glaser J: Long-bone radiographic abnormalities as a sign of active congenital syphilis in asymptomatic newborns. Pediatrics 1991;88:1037-1040
1. 01.119 Figure 36 shows an axial T1-weighted MRI scan at L4-5. The arrow is
2. pointing to what structure?
3. 1- Spinous process
4. 2- Herniated disk
5. 3- Epidural fat
6. 4- Ligamentum flavum
7. 5- Facet joint
1. answer
1. back
1. Question 01.119
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Author states there is no reference.
1. 01.120 What is the most severe side effect of doxorubicin (Adriamycin)?
2. 1- Neurotoxicity
3. 2- Ototoxicity
4. 3- Cardiac toxicity
5. 4- Hemorrhagic cystitis
6. 5- Pulmonary fibrosis
1. answer
1. back
1. Question 01.120
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty 1H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189. Burgert EO Jr, Nesbit ME, Garnsey LA, et al: Multimodal therapy for the management of nonpelvic, localized Ewing's sarcoma of bone: Intergroup study IESS-II J Clin Oncol 1990;8:1514-1524.
1. 01.121 Which of the following procedures is most likely to result in a hooked nail
2. deformity following fingertip amputation?
3. 1- Split-thickness skin grafting
4. 2- Reimplantation of the avulsed skin
5. 3- Local advancement flap
6. 4- Nail removal for associated nail bed repair
7. 5- Primary closure
1. answer
1. back
1. Question 01.121
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill
3. Livingstone, 1999, pp 1353-1380. Zook EG, Russell RC: Reconstruction of a functional and esthetic nail. Hand Clin 1990;6:59-68.
1. 01.122 Which of the following shoe insert (orthosis) materials has the greatest shock-
2. absorbing properties?
3. 1- Cross-linked polyethylene foam
4. 2- Rubberized cork
5. 3- Polypropylene
6. 4- Carbon epoxy resin
7. 5- Natural leather
1. answer
1. back
1. Question 01.122
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Shiba N, Kitaoka HB, Cahalan TD, Chao EY: Shock-absorbing effect of shoe insert materials commonly used in management of lower extremity disorders. Clin Orthop 1995;310:130-136. Wapner KL: Conservative treatment of the foot, in Coughlin MJ, Mann RA (eds): . Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 115-130.
1. 01.123 What type of major pelvic ring injury has the greatest average transfusion
2. requirement?
3. 1- Lateral compression
4. 2- Vertical shear
5. 3- Anteroposterior compression
6. 4- Fractures through the sacrum
7. 5- Fractures through the iliac wing
1. answer
1. back
1. Question 01.123
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Turen CH, Dube MA, LeCroy MC: Approach to the polytraumatized patient with musculoskeletal injuries. J Am Acad Orthop Surg 1999;7:154-165. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 1989;29:981-1002.
1. 01.124 Where does the nutrient artery to the tibia most commonly enter the bone?
2. 1- Anteriorly above the pes anserinus
3. 2- Anteriorly 4 cm above the ankle
4. 3- Laterally above the fibular head
5. 4- Posteriorly below the posterior cruciate ligament insertion
6. 5- Posteriorly in the medial malleolus
1. answer
1. back
1. Question 01.124
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Brinker MR, Cook SD, Dunlap IN, Christakis P, Elliott MN: Early changes in nutrient artery blood flow following tibial nailing with and without reaming: A preliminary study. J Orthop Trauma 1999;13:129-133.
1. 01.125 An 11-year-old soccer player has had left lateral ankle pain for the past 6
2. months. Examination shows increased heel valgus and decreased subtalar
3. motion on the left side. Ankle range of motion and stability are symmetric.
4. Radiographs of the foot and ankle are normal. The next most appropriate step
5. in management should consist of
6. 1- observation with follow-up in 6 months.
7. 2- a full shoe orthosis with medial heel posting left.
8. 3- left sinus tarsi injections with local anesthetic.
9. 4- comparative stress radiographs of both ankles.
10. 5- CT of the left foot.
1. answer
1. back
1. Question 01.125
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL., American Academy of Orthopaedic Surgeons, 1999, pp 583-595. Wechsler RJ, Schweitzer ME, Deely DM, Horn BD, Pizzutillo PD: Tarsal coalition: Depiction and characterization with CT and MR imaging. Radiology
3. 1994;193:447-452.
1. 01.126 What complication is significantly more common among octogenarians who
2. undergo concomitant bilateral total knee arthroplasty than those who undergo
3. unilateral total knee arthroplasty?
4. 1- Deep wound infection
5. 2- Aseptic loosening
6. 3- Periprosthetic fracture
7. 4- Congestive heart failure
8. 5- Pneumonia
1. answer
1. back
1. Question 01.126
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Lynch NM, Trousdale RT, Ilstrup DM: Complications after concomitant bilateral total knee arthroplasty in elderly patients. Mayo Clin Proc 1997;72:799-805. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
1. 01.127 A 53-year-old man has had low back pain
2. and perineal fullness for the past 18
3. months. A plain radiograph is shown in
4. Figure 37a, a CT scan is shown in Figure
5. 37b, and a biopsy specimen is shown in
6. Figure 37c. What is the most likely
7. diagnosis?
8. 1- Chordoma
9. 2- Plasmacytoma
10. 3- Fibrosarcoma
11. 4- Liposarcoma
12. 5- Metastatic carcinoma
1. answer
1. back
1. A
1. B
1. Figures 37
1. C
1. Question 01.127
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276. Bruckner 1D, Conrad EU: Spine, in Simon MA. Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 435-450.
1. 01.128 What is the most common soft-tissue tumor in children?
2. 1- Ganglion
3. 2- Hemangioma
4. 3- Fibroma
5. 4- Lipoma
6. 5- Sarcoma
1. answer
1. back
1. Question 01.128
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Conrad EU, Enneking WR: Clinical Symposium: Common Soft Tissue Tumors, ed 2. New York, NY, Ciba-Geigy, 1990.
1. 01.129 Which of the following is considered the most important factor in fracture
2. healing in adults?
3. 1- Age of the patient
4. 2- Gender of the patient
5. 3- Neurologic status of the extremity
6. 4- Blood supply
7. 5- Fracture pattern
1. answer
1. back
1. Question 01.129
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.130 A 67-year-old woman reports progressively worsening buttock pain.
2. Examination reveals a mass affixed to the region of the posterior ilium. Figures
3. 38a through 38d show a plain radiograph, a posterior view bone scan, a CT
4. scan, and a biopsy specimen. What is the most likely diagnosis?
5. 1- Dedifferentiated chondrosarcoma
6. 2- Malignant fibrous histiocytoma
7. 3- Fibrosarcoma
8. 4- Pagetoid osteosarcoma
9. 5- Osteomyelitis
1. back
1. A
1. B
1. Figures 38
1. Go to next slide for remaining
2. figures and
3. answer link
1. Figures 38
1. D
1. C
1. answer
1. back to question
1. Question 01.130
1. Question 01.130
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802. Harrington KD: Surgical management of neoplastic complications of Paget's disease. J Bone Miner Res 1999;2:45-48.
1. 01.131 A 23-year-old woman has had chronic swelling in the ankle for the past year
2. with no history of injury. Plain radiographs are normal. At ankle arthroscopy,
3. the articular surfaces appear normal. The synovial tissue is inflamed and friable;
4. a biopsy specimen of the synovium is shown in Figure 39. What is the most
5. likely diagnosis?
6. 1- Tuberculosis
7. 2- Synovial cell sarcoma
8. 3- Pigmented villonodular synovitis
9. 4- Rheumatoid arthritis
10. 5- Chondrocalcinosis
1. answer
1. back
1. Figure 39
1. Question 01.131
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Rao AS, Vigorita VJ: Pigmented villonodular synovitis (giant-cell tumor of the tendon sheath and synovial membrane): A review of eighty-one cases. J Bone Joint Surg Am 1984;66:76-94.
1. 01.132 Figure 40 shows the radiograph of a 24-year-old woman who has ulnar-sided
2. wrist pain. Nonsurgical management consisting of splinting, physical therapy,
3. and activity modifications has failed to provide relief. Examination reveals a
4. stable distal radioulnar joint and a negative triangular fibrocartilage complex
5. grind. Pain is reproduced when the wrist is dorsiflexed and the forearm is then
6. supinated but not when the forearm is
7. pronated. Treatment should now consist of
8. 1- partial ulnar styloidectomy.
9. 2- triangular fibrocartilage complex rim repair.
10. 3- debridement of the extensor carpi ulnaris tendon
11. sheath.
12. 4- a radial lengthening osteotomy.
13. 5- an ulnar shortening osteotomy.
1. answer
1. back
1. Figure 40
1. Question 01.132
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Topper SM, Wood MB, Ruby LK: Ulnar styloid impaction syndrome. J Hand Surg Am 19972:699-704. Topper SM, Wood MB, Ruby LK Ulnar styloid impaction syndrome, in Sulfar P, Amadio PC, Foucher G (eds): Current Practice in Hand Surgery. London, England, Martin Dunitz, 1997, pp 261-268.
1. 01.133 A patient with diabetes mellitus has an ulcer on the plantar aspect of the foot.
2. Which of these test results best correlates with the patient's ability to heal this
3. ulcer?
4. 1- Toe pressures of greater than 45 mm Hg
5. 2- An arterial brachial index of 0.40
6. 3- Capillary refill time in the toes of greater than 3 seconds
7. 4- Ability to detect greater than a 5.07 Semmes -Weinstein monofilament
8. 5- A hemoglobin A3 level of greater than 4%
1. answer
1. back
1. Question 01.133
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121. Brodsky JW: The diabetic foot. in Coughlin MJ. Mann RA (eds)- Surgery of the root and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 895-969.
1. 01.134 A 42-year-old woman who has had a low-grade aching pain in her forearm for
2. the past 4 years recently fell on the arm and now reports markedly increased
3. pain. A plain radiograph and biopsy specimen are shown in Figures 41a and
4. 41b. What is the most likely diagnosis?
5. 1- Chondroblastoma
6. 2- Chondrosarcoma
7. 3- Chondromyxoid fibroma
8. 4- Adamantinoma
9. 5- Enchondroma
1. answer
1. back
1. A
1. Figures 41
1. B
1. Question 01.134
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Weis L: Common malignant bone tumors: Chondrosarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 275-286. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276.
1. 01.135 To prevent abnormal patellofemoral contact loading after insertion of a
2. retrograde femoral nail through an intra-articular starting portal, the surgeon
3. should
4. 1- seat the nail beneath the articular surface.
5. 2- use a patellar tendon-splitting approach.
6. 3- use an unreamed technique.
7. 4- perform a lateral release.
8. 5- perform a medial parapatellar arthrotomy.
1. answer
1. back
1. Question 01.135
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Moed B, Watson JT: Retrograde nailing of the femoral shaft. J Am Acad Orthop Surg 1999;7:209-216. Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
1. 01.136 A woman who is in the 20th week of her pregnancy seeks an orthopaedic
2. consultation after undergoing an ultrasound. The findings reveal that the fetus
3. has bilateral clubfeet and both femurs measure less than two standard
4. deviations below normal. What is the most likely diagnosis?
5. 1- Myelomeningocele
6. 2- Bilateral proximal focal femoral deficiency
7. 3- Diastrophic dysplasia
8. 4- Achondroplasia
9. 5- Spondylometaphyseal dysplasia
1. answer
1. back
1. Question 01.136
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Horton WA, Hall JG, Scott CI, Pyeritz RE, Rimoin DL: Growth curves for height for diastrophic dysplasia, spondyloepiphyseal dysplasia congenita, and pseudoachondroplasia. Am J Dis Child 1982;136:316-319. Ryoppy S, Poussa M, Merikanto J, Marttinen E, Kaitila I: Foot deformities in diastrophic dysplasia: An analysis of 102 patients. J Bone Joint Surg Br 1992;74:441-44.4.
1. 01.137 A 47-year old woman has right groin pain. An AP radiograph of the pelvis and
2. a biopsy specimen are shown in Figures 42a and 42b. What is the most likely
3. diagnosis?
4. 1- Ollier's disease
5. 2- Paget's disease
6. 3- Metastatic carcinoma
7. 4- Aneurysmal bone cyst
8. 5- Fibrous dysplasia
1. answer
1. back
1. A
1. B
1. Figures 42
1. Question 01.137
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, pp 195-276. Gitelis S, McDonald DJ: Common benign bone tumors and usual treatment, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 275-286.
1. 01.138 Acute hypotension, hypoxemia, cardiac arrest, and sudden death are events that
2. are most commonly encountered in what stage of total hip arthroplasty?
3. 1- Exposure
4. 2- Acetabular reaming
5. 3- Broaching the femur
6. 4- Impaction of the acetabular component
7. 5- Cementing of the femoral component
1. answer
1. back
1. Question 01.138
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Pitto RP, Koessler M, Kuehle JW: Comparison of fixation of the femoral component without cement and fixation with use of a bone-vacuum cementing technique for the prevention of fat embolism during total hip arthroplasry: A
3. prospective, randomized clinical trial. J Bone Joint Surg Am 1999;81:831-843.
1. 01.139 A 35-year-old woman falls on the ice and sustains an isolated minimally
2. displaced radial head fracture. Management should include
3. 1- use of a posterior splint and sling at all times for 6 weeks.
4. 2- use of a sling until radiologic union is achieved.
5. 3- application of a cast in 7 to 10 days.
6. 4- application of a hinged elbow orthosis in 3 weeks.
7. 5- a program of active range of motion in 1 week.
1. answer
1. back
1. Question 01.139
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Morrey BF: Radial head fractures, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WE Saunders, 1985, pp 355-381. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 47-55.
1. 01.140 An asymptomatic 10-year-old boy is referred for evaluation of a limb-length
2. discrepancy that measures less than 2 cm. Examination reveals that the most
3. lateral ray of the ipsilateral foot is absent, and the ipsilateral knee is unstable to
4. Lachman and anterior drawer tests. Figure 43 shows an AP radiograph of the
5. ankle. Management of the knee should consist of
6. 1- anterior cruciate ligament reconstruction using a
7. quadruple hamstring technique.
8. 2- anterior cruciate ligament reconstruction using an
9. allograft in the over-the-top position.
10. 3- observation.
11. 4- an aggressive physical therapy program that
12. emphasizes open chain techniques.
13. 5- functional knee bracing until skeletal maturity,
14. followed by anterior cruciate ligament reconstruction.
1. answer
1. back
1. Figure 43
1. Question 01.140
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Achterman C, Kalamchi A: Congenital deficiency of the fibula. J Bone Joint Surg Br 1979;61:133-137. Roux MO, Cariioz H: Clinical examination and investigation of the cruciate ligaments in children with fibular hemimelia. J Pediatr Orthop 1999;19:247-251. Stevens PM, Arms D: Postaxial hypoplasia of the lower extremity. J Pediatr Orthop 2000;20:166-172.
1. 01.141 A nonrandomized prospective study of the efficacy of a new diagnostic test to
2. detect deep venous thrombosis has just been completed. Each patient had
3. venography as the definitive test to detect the thrombosis. Of the 100 patients
4. tested, 10 were true positives, 30 were false negatives, 40 were true negatives,
5. and 20 were false positives. What is the sensitivity of the new test?
6. 1- 25 %
7. 2- 30%
8. 3- 50 %
9. 4- 59%
10. 5- 67 %
1. answer
1. back
1. Question 01.141
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American
3. Academy of Orthopaedic Surgeons, 2000, pp 308-316.
1. 01.142 When treating tibial plateau fractures, the most important reason that proximal
2. tibial transfixation wires should be placed at least 14 mm from the articular
3. surface is to
4. 1- obtain good fixation in subchondral bone.
5. 2- allow radiographic visualization of the joint reduction.
6. 3- minimize the risk that septic arthritis will develop.
7. 4- increase the range of knee flexion.
8. 5- compress the articular fragments.
1. answer
1. back
1. Question 01.142
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. DeCoster TA, Crawford M.K, Kraut VIA: Safe extracapsular placement of proximal tibia transfixation pins. J Orthop Trauma 1999;13:236-240. Reid JS, Van Slyke MA, Moulton MJ, Mann TA: Safe placement of proximal tibial transfixation wires with respect to intracapsular penetration. J Orthop Trauma 2001;15:10-17.
1. 01.143 A 17-year-old girl reports a 4-month history of progressively worsening left
2. arm pain. A plain radiograph and biopsy specimen are shown in Figures 44a
3. and 44b. After complete staging, management should consist of
4. 1- forequarter amputation alone.
5. 2- radiation therapy and chemotherapy.
6. 3- radiation therapy and wide surgical excision.
7. 4- chemotherapy and wide surgical excision.
8. 5- wide surgical excision alone.
1. answer
1. back
1. A
1. B
1. Figures 44
1. Question 01.143
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Primary bone tumors, in McCarthy EF, Frassica FJ (eds): Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia., PA.
3. WB Saunders, 1998, pp 195-276. Weis L: Common malignant bone tumors: Osteosarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274. Goorin A: Chemotherapy for osteosarcoma and Ewing's sarcoma, in Simon MA, Springfield D (eds): Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA,
4. Lippincott-Raven, 1998, pp 239-244.
1. 01.144 Figure 45 shows the initial clinical photograph of a 70-year-old woman. The
2. deformity of the second toe may recur after attempted surgical reconstruction.
3. Dysfunction of what structure allows for recurrence?
4. 1- Dorsal capsule
5. 2- Plantar plate
6. 3- Medial collateral ligament
7. 4- Lateral collateral ligament
8. 5- Transverse intermetatarsal ligament
1. answer
1. back
1. Figure 45
1. Question 01.144
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Yao L, Cracchiolo A, Farahani K, Seeger LL: Magnetic resonance imaging of plantar plate rupture. Foot Ankle Int 1996;17:33-36. Deland JT, Sung IH: The medial crossover toe: A cadaveric dissection. Foot Ankle Int 2000;21:375-378.
1. 01.145 A 25-year-old rugby player who sustained blunt trauma to the right dominant
2. long finger 2 days ago now reports pain over the dorsum of the digit and
3. clicking when he flexes and extends the digit. Examination reveals swelling
4. and ecchymosis over the metacarpophalangeal joint, as well as a palpable
5. subluxation of the extrinsic extensor tendon over the metacarpophalangeal
6. joint with joint flexion and extension. Management should consist of
7. 1- surgical repair of the sagittal band.
8. 2- surgical repair of the spiral oblique retinacular ligament.
9. 3- surgical repair of the triangular ligament.
10. 4- splinting the metacarpophalangeal joint at 70° of flexion.
11. 5- a program of early active motion with buddy taping.
1. answer
1. back
1. Question 01.145
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Ishizuki M: Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg Am 1990;15:967-972. Rayan GM, Murray D: Classification and treatment of closed sagittal band injuries. J Hand Surg Am 1994;19:590-594.
1. 01.146 When placing lateral mass screws in the midcervical spine, where is the
2. vertebral artery located in relation to the starting point for screw insertion?
3. 1- Medial
4. 2- Lateral
5. 3- Anterior
6. 4- Posterior
7. 5- Superior
1. answer
1. back
1. Question 01.146
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Levine AM: Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 335-339.
1. 01.147 A 30-year-old man underwent an arthroscopic Bankart repair with suture
2. anchors 6 months ago. While the patient reports that the shoulder is stable, he
3. notes anterior shoulder pain and crepitation. Figure 46 shows an arthroscopic
4. view of the anterior shoulder joint. The next most appropriate step in
5. management should consist of
6. 1- an intra-articular culture.
7. 2- rotator cuff repair.
8. 3- removal of the anchors.
9. 4- arthroscopic releases.
10. 5- exchange of the metallic
11. anchor for a bioabsorbable
12. device.
1. answer
1. back
1. Figure 46
1. Question 01.147
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Kaar TY, Schenck RC Jr, Worth MA, Rockwood CA Jr.- Complications of metallic suture anchors in shoulder surgery: A report of 8 cases. Arthroscopy 2001;17:31-37. Zuckerman JD, Matsen FA III: Complications about the glenohumeral joint related to the use of screws and staples. J Bone Joint Surg Am 1984;66:175-180
1. 01.148 A 32-year-old man notes a lump on the side of his neck and undergoes a lymph
2. node biopsy. Following the procedure, the patient reports pain in the shoulder
3. girdle and is unable to elevate his shoulder. Which of the following structures
4. has most likely been injured?
5. 1- Trapezius muscle
6. 2- Sternocleidomastoid muscle
7. 3- Axillary nerve
8. 4- Cranial nerve XI
9. 5- Suprascapular nerve
1. answer
1. back
1. Question 01.148
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Leffert RD: Neurologic problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, p 759. Bigliani LU, Perez-Sanz JR, Wolfe IN: Treatment of trapezius paralysis. J Bone Joint Surg Am 1985;67:871-877.
1. 01.149 A 40-year-old woman with steroid-dependent Crohn's disease has had pain and swelling
2. of the left ankle for the past 5 days. She has a plugged central line for parenteral feeding.
3. Examination of the ankle reveals focal inflammation and limited range of motion. She is
4. sensitive to the 4.17 Semmes-Weinstein monofilament test. Radiographs are shown in
5. Figures 47a and 47b. The next most appropriate step in management should consist of
6. 1- a biopsy of the talus.
7. 2- a bone scan.
8. 3- aspiration and culture of the ankle.
9. 4- no weight bearing and a total contact cast for 1 week.
10. 5- a brace with calipers.
1. answer
1. back
1. A
1. B
1. Figures 47
1. Question 01.149
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mielants H, Veys EM: The gut in the pondyloarthropathies. J Rheumatol 1990;17:7-10. Myerson M: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1215-1216.
1. 01.150 What structures are located within the femoral canal as it passes beneath the
2. inguinal ligament?
3. 1- Femoral artery, femoral vein, and femoral nerve
4. 2- Femoral artery and femoral vein
5. 3- Femoral artery, femoral vein, and lymphatics
6. 4- Femoral artery, femoral vein, femoral nerve, and lymphatics
7. 5- Internal iliac artery, internal iliac vein, and femoral nerve
1. answer
1. back
1. Question 01.150
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. ed 2. Philadelphia. PA. JB Lippincott, 1994. pp 362-275.
1. 01.151 A 6-month-old boy with L1 myelomeningocele has bilateral dislocated hips.
2. Examination reveals that the hips are clinically reducible, and there are no
3. significant hip or knee joint contractures. The best course of action for both
4. hips should consist of
5. 1- observation.
6. 2- application of a Pavlik harness.
7. 3- application of a rigid hip abduction orthosis.
8. 4- closed reduction with a hip spica cast.
9. 5- open reduction via an adductor approach.
1. answer
1. back
1. Question 01.151
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spins bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436. Broughton NS, Menelaus MB, Cole WG, Shurtleff DB: The natural history of hip deformity in myelomeningocele. J Bone Joint Surg Br 1993;75:760-763.
1. 01.152 Sterilization of ultra-high molecular-weight polyethylene by irradiation in an
2. inert environment (argon, nitrogen, or vacuum) is recommended because it
3. 1- increases crystallinity.
4. 2- prevents free radical formation.
5. 3- prevents immediate oxidative degradation.
6. 4- prevents component shrinkage.
7. 5- provides better sterility.
1. answer
1. back
1. Question 01.152
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53. Deng M, Shalaby SW: Lang-term gamma irradiation effects on ultrahigh molecular weight polyethylene. J Biomed Mater Res 2001;54:428-435.
1. 01.153 A 13-year-old girl reports activity-related pain in her left leg with no history of
2. trauma. Figures 48a through 48d show a plain radiograph, T1- and T2-weighted
3. MRI scans, and a biopsy specimen. What is the most likely diagnosis?
4. 1- Ewing's sarcoma
5. 2- Osteomyelitis
6. 3- Fibrous dysplasia
7. 4- Adamantinoma
8. 5- Tibial stress fracture
1. back
1. A
1. B
1. Figures 48
1. Go to next slide for remaining figures and answer link
1. Figures 48
1. D
1. C
1. answer
1. back to question
1. Question 01.153
1. Question 01.153
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Jeske JM, Lomasney LM, Demos TC, Vade A, Bielski RJ: Longitudinal tibial stress fracture. Orthopedics 1996;19:263,66,68,70. Shearman CM, Brandser EA, Parman LM, et al: Longitudinal tibial stress fractures: A report of eight cases and review of the literature. J Comput Assist Tomogr 1998;22:265-269.
1. 01.154 A 30-year-old woman who underwent total hip arthroplasty for osteonecrosis 6
2. months ago is now seeking a second opinion for her limp. What is the most
3. significant radiographic finding shown in Figure 49?
4. 1- Contralateral osteonecrosis
5. 2- Prosthetic loosening
6. 3- Heterotopic ossification
7. 4- Stress shielding
8. 5- Limb-length inequality
1. answer
1. back
1. Figure 49
1. Question 01.154
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Woolson ST: Leg length equalization during total hip replacement. Orthopedics 1990;13:17-21. Shaw JA, Greet RB III: Complications of total hip replacement, in Epps CH Jr (ed): Complication in Orthopaedic Surgery. Philadelphia, PA, JB Lippincott,
3. 1994, pp 1013-1056.
1. 01.155 Figure 50 shows the radiograph of a 24-year-old patient who has a slightly painful swollen distal finger. What is the most likely diagnosis?
2. 1- Glomus tumor
3. 2- Giant cell tumor
4. 3- Intraosseous ganglion
5. 4- Foreign body granuloma
6. 5- Inclusion cyst
1. answer
1. back
1. Question 01.155
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Schajowicz F, Aiello CL, Slullitel I: Cystic and pseudocystic lesions of the terminal phalanx with special reference to epidermoid cysts. Clip Orthop 1970;68:84-92. Athanasian EA: Bone and soft-tissue tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2223-2253.
1. 01.156 A 4-year-old boy has a painful spinal deformity. Figures 51a through 51d show
2. a lateral spine radiograph, whole body bone scan, a lateral T1-weighted MRI
3. scan, and a needle biopsy specimen. What is the most likely diagnosis?
4. 1- Tuberculosis
5. 2- Metastatic neuroblastoma
6. 3- Chordoma
7. 4- Diskitis
8. 5- Ewing's sarcoma
1. back
1. A
1. B
1. Figures 51
1. Go to next slide
2. for remaining
3. figures and
4. answer link
1. Figures 51
1. D
1. C
1. answer
1. back to question
1. Question 01.156
1. Question 01.156
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Mushkin AY, Kovalenko KN: Neurological complications of spinal tuberculosis in children. Int Orthop 1999;23:210-212. Sudarshan K: Tuberculosis of bones and joints. J Bone Joint Surg Am 1997;79:1891.
1. 01.157 A 19-year-old man sustained a fracture-dislocation of the ankle and a talar neck
2. and body fracture when his foot was run over by a truck. Examination reveals
3. no pulse in the ankle and an ischemic foot. The anterior and posterior tibial
4. arteries are transected. He has no other injuries. A clinical photograph is shown
5. in Figure 52. Treatment should consist of
6. 1- repair of the posterior tibial artery and ankle fusion.
7. 2- repair of the anterior tibial artery and pantalar fusion.
8. 3- repair of both tibial arteries and internal fixation of the talus.
9. 4- repair of the posterior tibial artery and nerve and external fixation.
10. 5- amputation.
1. answer
1. back
1. Figure 52
1. Question 01.157
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Gregory P, Sanders R: The management of severe fractures of the lower extremities. Clip Orthop 1995;318:95-105.
3. Tornetta P III, Olson SA (eds): Amputation versus limb salvage. Instr Course Lect 1997;46:511-518.
1. 01.158 In an animal model, the use of anabolic steroids on muscle contusion injury has
2. been shown to
3. 1- be similar to placebo controls.
4. 2- be similar to corticosteroids with respect to muscle strength recovery in the long
5. term.
6. 3- be more effective than corticosteroids with respect to muscle strength recovery in the
7. long term.
8. 4- be less effective than corticosteroids with respect to muscle strength recovery in the
9. long term.
10. 5- result in severely disorganized muscle fiber architecture.
1. answer
1. back
1. Question 01.158
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beiner JM, Jokl P, Cholewicki J, Panjabi MM: The effect of anabolic steroids and corticosteroids on healing of muscle contusion injury. Am J Sports Med 1999;27:2-9. Tingus SJ, Carlsen RC: Effect of continuous infusion of an anabolic steroid on marine skeletal muscle. Med Sci Sports Exert 1993;25:485-494.
1. 01.159 When performing a surgical debridement for a painful irreparable rotator cuff
2. tear, it is important to
3. 1- tenodese the biceps.
4. 2- excise the distal clavicle (Mumford procedure).
5. 3- preserve the coracohumeral ligament.
6. 4- preserve the coracoacromial ligament.
7. 5- advance the deltoid origin.
1. answer
1. back
1. Question 01.159
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Ellman H, Hanker G, Bayer M: Repair of the rotator cuff: End-result study of factors influencing reconstruction. J Bone Joint Surg Am 1986;68:1136-1144. Hanyman DT II, Mack LA. Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of
3. the cuff. J Bone Joint Surg Am 1991;73:982-989.
1. 01.160 A patient with developmental dysplasia of the hip is undergoing open
2. reduction. Which of the following is considered an advantage of using a medial
3. approach compared with an anterior approach?
4. 1- A lower incidence of osteonecrosis
5. 2- Access for performance of capsulorrhaphy
6. 3- Access to the transverse acetabular ligament
7. 4- Better ability to reduce an inverted labrum
8. 5- Better visualization of the lateral femoral cutaneous nerve
1. answer
1. back
1. Question 01.160
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Turner Y, Ward WT, Grudziak J: Medial open reduction in the treatment of developmental dislocation of the hip. J Pediatr Orthop 1997;17:176-180. Mankey MG, Arntz GT, Staheli LT: Open reduction through a medial approach for congenital dislocation of the hip: A critical review of the Ludloff approach in sixty-six hips. J Bone Joint Surg Am 1993;75:1334-1345.
1. 01.161 A 35-year-old laborer sustains a irreparable fracture of the radial head after
2. falling 12 feet. Examination reveals tenderness at the elbow and wrist and pain
3. with manipulation of the distal radioulnar joint. In addition to resection of the
4. radial head, management should include
5. 1- hinged bracing of the elbow.
6. 2- immobilization in a long arm cast.
7. 3- prosthetic replacement of the radial head.
8. 4- repair of the distal radioulnar joint.
9. 5- application of a hinged external fixator.
1. answer
1. back
1. Question 01.161
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL,, American Academy of Orthopaedic Surgeons, 2000, pp 39-51. Hotchkiss RN: An KN, Sowa DT, Banta S, Weiland AJ: An anatomic and mechanical study of the interosseous membrane of the forearm: Pathomechanics of proximal migration of the radius. J Hand Surg Am 1989;14:256-261.
1. 01.162 Which of the following treatments has been shown to prevent the formation of
2. heterotopic ossification after total hip arthroplasty in patients who are at high
3. risk?
4. 1- Alendronate
5. 2- Acetaminophen
6. 3- Preoperative radiation
7. 4- Calcitonin
8. 5- Parathormone
1. answer
1. back
1. Question 01.162
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Knelles D, Barthel T, Karrer A, Kraus U, Eulert J, Kolbl O: Prevention of heterotopic ossification after total hip replacement: A prospective, randomised study using acetylsalicylic acid, indomethacin and fractional or single-dose, irradiation. J Bone Joint Surg Br 1997;79:596-602. Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Sung Am 1996;78:870-881.
1. 01.163 A 38-year-old landscaper was treated with internal and external fixation for a
2. severe pilon fracture. Radiographs obtained at 3 months and 1 year are shown
3. in Figures 53a and 53b. He now reports increasing pain over the past 4 months
4. and is unable to walk uphill or stand for more than 2 hours. Examination
5. reveals range of motion from neutral to 5° of plantar flexion. Use of a short leg
6. brace with a rocker bottom sole after screw removal provides some pain relief,
7. but he still has too much pain to work. Management should now consist of
8. 1- manipulation of the ankle under anesthesia.
9. 2- arthroscopic debridement of the ankle.
10. 3- ankle arthroplasty.
11. 4- ankle fusion.
12. 5- subtalar fusion.
1. answer
1. back
1. A
1. B
1. Figures 53
1. Question 01.163
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic
3. Surgeons, 2000, pp 191-202.
1. 01.164 Which of the following factors best predicts the increased risk for development
2. of a foot ulcer in a patient with diabetes mellitus?
3. 1- A history of a previous foot ulcer
4. 2- A history of poor blood glucose control
5. 3- Type I diabetes for more than 10 years
6. 4- Ability to detect a 5.07 Semmes-Weinstein monofilament, on the plantar surface of
7. the foot
8. 5- Nonpalpable pulses with an ankle-brachial index (ABI) of greater than 0.5
1. answer
1. back
1. Question 01.164
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. McDermott JE (ed): The Diabetic Foot. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 1-12. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 113-12I. Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 895-969.
1. 01.165 A study is being designed to compare the results of two new drugs on bone
2. mineral density. The number of subjects needed for this study should be
3. determined by
4. 1- Student's t test.
5. 2- power analysis.
6. 3- probability distribution.
7. 4- regression analysis.
8. 5- Spearman rank correlation.
1. answer
1. back
1. Question 01.165
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 2-17.
1. 01.166 A 17-year-old basketball player sustains an ankle eversion injury on a fast
2. break. She notes immediate anteromedial ankle pain and swelling and is unable
3. to bear weight. The next most appropriate step in management should consist
4. of
5. 1- ice and protected weight bearing.
6. 2- functional ankle bracing treatment.
7. 3- a short leg cast.
8. 4- radiographs.
9. 5- MRI.
1. answer
1. back
1. Question 01.166
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Roberts CS, DeMaio M, Larkin JJ, Paine R: Eversion ankle sprains. Orthopedics 1995;18:299-304. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons 1999, pp 597-612.
1. 01.167 Following reinsertion of the distal biceps tendon, early rehabilitation should
2. include
3. 1- active elbow flexion and active forearm supination.
4. 2- active elbow flexion and passive forearm supination.
5. 3- active elbow extension and active forearm supination.
6. 4- passive elbow extension and active forearm supination.
7. 5- passive elbow flexion and passive forearm supination.
1. answer
1. back
1. Question 01.167
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Money BF: Tendon injuries about the elbow, in Moray BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Sounders, 1993, pp 492-504. Sotereanos DG, Pierce TD, Varitimidis SE: A simplified method for repair of distal biceps tendon ruptures. J Shoulder Elbow Sung 2000;9:227-233.
1. 01.168 In the absence of a visible fracture on radiographs, the presence of a positive
2. posterior fat pad sign following trauma of the elbow in a 5-year-old child most
3. likely represents
4. 1- a normal radiographic finding.
5. 2- a soft-tissue contusion.
6. 3- nursemaid's elbow.
7. 4- an occult fracture.
8. 5- synovial hypertrophy.
1. answer
1. back
1. Question 01.168
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Sung Am 1999;81:1429-1433. Donnelly LF, Klostermeier TT, Klosterman LA: Traumatic elbow effusions in pediatric patients: Are occult fractures the rule? Am J Roentgenol 1998;171:243-245.
1. 01.169 Thumb adduction in low ulnar nerve palsy is provided by the
2. 1- extensor pollicis longus.
3. 2- extensor pollicis brevis.
4. 3- flexor pollicis brevis.
5. 4- first dorsal interosseous.
6. 5- accessory head of the flexor pollicis longus (Gantzer's muscle).
1. answer
1. back
1. Question 01.169
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Smith RJ: Tendon Transfers of the Hand and Forearm. Boston, MA, Little Brown, 1987, pp 85-102. Hamlin C, Littler JW: Restoration of power pinch. J Hand Surg Am 1980;5:396-401.
1. 01.170 The parents of a 6-month-old infant report that she has been unwilling to move
2. her left upper extremity for the past 5 hours. An AP radiograph and an MRI
3. scan are shown in Figures 54a and 54b. Based on these findings and after
4. initial treatment, a consultation should be arranged with
5. 1- child protection services.
6. 2- a geneticist.
7. 3- a nephrologist.
8. 4- a rheumatologist.
9. 5- an infectious disease
10. specialist.
1. answer
1. back
1. A
1. B
1. Figures 54
1. Question 01.170
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. DeLee JC, Wilkins KE, Rogers LF, Rockwood CA: Fracture-separation of the distal humeral epiphysis. J Bone Joint Surg Am 1980;62:46-51. Cramer KE, Green NE: Child abuse, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Sounders, 1998, pp 577-594. Nimkin K, Kleinman PK. Teeger S, Spevak MR: Distal humeral physeal injuries in child abuse: MR imaging and ultrasonography findings. Pediatr Radiol 1995;25:562-565. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
1. 01.171 Where are the sacral roots located within the canal at the L1-2 disk level?
2. 1- Random pattern
3. 2- Anterior
4. 3- Central
5. 4- Lateral
6. 5- Posterior
1. answer
1. back
1. Question 01.171
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Wall E1, Cohen MS, Abitbol JJ, Garfin SR: Organization of intrathecal nerve roots at the level of the conus medullaris. J Bone Joint Surg Am 1990;72:1495-1499. Wall FJ, Cohen MS, Massie JB, Rydevik B, Garfin SR: Cauda equina anatomy: L Intrathecal nerve root organization. Spine 1990;15:1244-1247.
1. 01.172 University of California Biomechanics Laboratory (UCBL) lower extremity
2. orthoses are thought to work by
3. 1- supporting the forefoot in rigid deformities.
4. 2- supporting the midfoot in rigid deformities.
5. 3- controlling the hindfoot in flexible deformities.
6. 4- controlling the ankle when instability is present.
7. 5- accommodating a forefoot deformity.
1. answer
1. back
1. Question 01.172
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 55-64. Wapner KL: Conservative treatment of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 115-130.
1. 01.173 What portion of the calcaneus typically maintains a normal relationship to the
2. talus in displaced intra-articular calcaneus fractures?
3. 1- Sustentaculum tali
4. 2- Tuberosity
5. 3- Anterolateral
6. 4- Posterior facet
7. 5- Lateral wall
1. answer
1. back
1. Question 01.173
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Olexa TA, Ebraheim NA, Haman SP: The sustentaculum tall: Anatomic, radiographic, and surgical considerations. Foot Ankle Int 2000;21:400-403. Sanders R: Intro articular fractures of the calcaneus: Present state of the art. J Orthop Trauma 1992;6:252-265.
1. 01.174 The linear relationship between an applied stress and the resultant deformation
2. defines a material's
3. 1- modulus of elasticity.
4. 2- brittleness.
5. 3- yield strength.
6. 4- ultimate strength.
7. 5- toughness.
1. answer
1. back
1. Question 01.174
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 447-486.
1. 01.175 In total hip arthroplasty, which of the following characterizes the clinical pain
2. pattern seen with a loose femoral component?
3. 1- Gluteal
4. 2- Night
5. 3- Start-up
6. 4- Back
7. 5- At rest
1. answer
1. back
1. Question 01.175
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Katz RP, Callaghan JJ, Sullivan PM, Johnston RC: Long-term results of revision total hip arthroplasty with improved cementing technique. J Bone Joint Sung Br 1997;79:322-326. Krishnamurthy AB, MacDonald SJ, Paprosky WG: 5- to 13-year follow-up study on cementless femoral components in revision surgery. J Arthroplasty 1997;12:839-847.
1. 01.176 What is the natural history of a nonossifying fibroma?
2. 1- Gradual enlargement after skeletal maturity
3. 2- Spontaneous resolution with skeletal maturity
4. 3- Chronic pain
5. 4- Late malignant degeneration
6. 5- Angular deformity
1. answer
1. back
1. Question 01.176
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Jaffe HL, Lichtenstein L: Non-osteogenic fibroma of bane. Am J Pathol 1942;18:205. Unni KK: Conditions that commonly simulate primary neoplasms of bone, in Dahlin's Bone Tumors, ed 5. Philadelphia, PA, 1996, pp 355-432.
1. 01.177 What structure is outlined and lies at the tip of the arrow shown in Figure 55?
2. 1- Inferior articular facet
3. 2- Superior articular facet
4. 3- Pedicle
5. 4- Lamina
6. 5- Spinous process
1. answer
1. back
1. Figure 55
1. Question 01.177
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Parke WW: Applied Anatomy of the Spine, in Herkowitz HN, Eismont FJ, Garfin SR, Bell GR, Balderston RA, Wiesel SW (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 27-73. Netter FH (ed): The Ciba Collection of Medical Illustrations: Musculoskeletal System, Part L Anatomy, Physiology, and Metabolic Disorders. Summit, NJ,
3. Ciba-Geigy, 1987, vol 8, pp 9-19.
1. 01.178 Which of the following systemic conditions is associated with a genetic defect
2. in skeletal formation that does not involve abnormal collagen?
3. 1- Osteogenesis imperfecta
4. 2- Spondyloepiphyseal dysplasia congenita
5. 3- Achondroplasia
6. 4- Multiple epiphyseal dysplasia
7. 5- Kneist dysplasia
1. answer
1. back
1. Question 01.178
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Dietz FR, Matthews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Bone Joint Surg Am 1996;78:1583-1598.
1. 01.179 What is the most likely cause of mortality within the first 48 hours in patients
2. who sustain a pelvic fracture from a lateral compression mechanism?
3. 1- Aortic rupture
4. 2- Pelvic arterial injury
5. 3- Pelvic venous injury
6. 4- Hollow viscous injury
7. 5- Head injury
1. answer
1. back
1. Question 01.179
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Dalal SA, Burgess AR, Siegel 3H, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome. J Trauma 1989;29;981-1002.
1. 01.180 Following total hip arthroplasty, examination of the patient reveals an ischemic
2. leg. A radiograph obtained in the recovery room is shown in Figure 56a, and a
3. subtraction arteriogram is shown in Figure 56b. What artery has been injured?
4. 1- Profunda femoris
5. 2- External iliac
6. 3- Obturator
7. 4- Superior gluteal
8. 5- Inferior gluteal
1. answer
1. back
1. A
1. B
1. Figures 56
1. Question 01.180
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Wasielewski RC, Cooperstein LA, Kruger MP, Rubash HE: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508. Shaw JA, Greer RB III: Complications of total hip replacement, in Epps CH Jr (ed): Complication in Orthopaedic Surgery. Philadelphia, PA, JB Lippincott,
3. 1994, pp 1013-1056.
1. 01.181 Which of the following axial pattern flaps is best used to repair fingertip
2. amputations?
3. 1- Axial flag
4. 2- First dorsal metacarpal artery
5. 3- Second dorsal metacarpal artery
6. 4- Reversed dorsal metacarpal artery
7. 5- Digital artery island
1. answer
1. back
1. Question 01.181
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Lai CS, Lin SD, Yang CC: The reverse digital artery flap for fingertip reconstruction. Ann Plant Surg 1989;22:495-500. Lister GD, Pederson WC: Skin flaps, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1783-1850.
1. 01.182 What is the most common complication seen in patients undergoing surgery on
2. the Achilles tendon for chronic refractory tendinitis?
3. 1- Deep vein thrombosis
4. 2- Partial/complete tendon rupture
5. 3- Skin edge necrosis
6. 4- Infection
7. 5- Complex regional pain syndrome
1. answer
1. back
1. Question 01.182
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Paavola M, Orava S, Leppilahti J, Kannus P, Jarvinen M: Chronic Achilles tendon overuse injury: Complications after surgical treatment: An analysis of 432 consecutive patients. Am J Sports Med 2000;28:77-82. Williams J: Achilles tendon lesions in sport. Sports Med 1986;3:114-135.
1. 01.183 Figures 57a and 57b show the radiographs of a college basketball player who
2. has had lateral foot pain for the past 3 weeks. Management should consist of
3. 1- weight bearing as tolerated with continued play.
4. 2- weight bearing as tolerated in a short leg cast.
5. 3- restricted weight bearing for 4 weeks, followed by an early return to play.
6. 4- electrical bone stimulation.
7. 5- percutaneous screw fixation.
1. answer
1. back
1. A
1. B
1. Figures 57
1. Question 01.183
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mindrebo N, Shelboume KD, Van Meter CD, Rettig AC: Outpatient percutaneous screw fixation of the acute Jones fracture. Am J Sports Med 1993;21:720-723. Weinfeld SB, Haddad SL, Myerson MS: Metatarsal stress fractures. Clip Sports Med 1997;16:319-338.
1. 01.184 A 62-year-old man has pain with overhead activities and shoulder weakness.
2. History reveals that he sustained an anterior dislocation of the right shoulder 18
3. months ago and underwent open repair of the subscapularis, supraspinatus, and
4. infraspinatus tendons 2 weeks after the injury. Examination reveals active total
5. elevation of 160°, active external rotation of 50°, and passive internal rotation
6. to T9. He has 5/5 deltoid, 4-/5 external rotation, and 5/5 internal rotation
7. strength. What is the most likely cause of his symptoms?
8. 1- Residual rotator cuff tear
9. 2- Adhesive capsulitis
10. 3- Glenohumeral instability
11. 4- Axillary neuropathy
12. 5- Suprascapular neuropathy
1. answer
1. back
1. Question 01.184
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Gerber C, Fucks B, Holler J: The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am 2000;82:505-515. Harryman DT II, Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am 1991;73:982-989.
1. 01.185 A 6-year-old girl has a right genu varum that has progressed over the last 6
2. months. Plain radiographs of the knee reveal a sloping medial joint line with an
3. obvious bony bar at the medial proximal tibial physis. A CT scan shows that
4. this bar involves about 20% of the physis. Treatment at this time should include
5. 1- epiphyseodesis of the proximal tibial physis.
6. 2- corrective osteotomy of the tibia and fibula.
7. 3- corrective osteotomy of the tibia and epiphyseodesis of the left proximal tibial
8. physis.
9. 4- proximal tibial physeal bar resection and corrective osteotomy of the tibia and fibula.
10. 5- elevating osteotomy of the proximal tibial medial plateau.
1. answer
1. back
1. Question 01.185
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520. Tachdjian MA: Tibia vara, in Pediatric Orthopaedics. Philadelphia, PA, WB Saunders, 1990, p 2846. Greene WB: Infantile tibia vara. Instr Course Lect 1993;42:525-538.
1. 01.186 An 18-year-old patient has the painful lesion shown in Figure 58a. A biopsy
2. specimen is shown in Figure 58b. Management should consist of
3. 1- preoperative chemotherapy and wide resection.
4. 2- wide resection only.
5. 3- marginal distal ulna resection.
6. 4- curettage and bone grafting.
7. 5- low-dose radiation.
1. answer
1. back
1. A
1. B
1. Figures 58
1. Question 01.186
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Martinet V, Sissons HA: Aneurysmal bone cyst: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-2304. Biesecker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cysts: A clinicopathologic study of 66 cases. Cancer 1970;26:615-625. Gibbs CP Jr, Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
1. 01.187 The value of intercondylar notch visualization of the posterior compartment
2. during anterior cruciate ligament reconstruction is to identify
3. 1- a loose body.
4. 2- a popliteus injury.
5. 3- meniscal root tears.
6. 4- an injury to the ligament of Wrisberg.
7. 5- an osteochondral injury.
1. answer
1. back
1. Question 01.187
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Amin KB, Cosgarea AJ, Kaeding CC: The value of intercondylar notch visualization of the posteromedial and posterolateral compartments during knee arthroscopy. Arthroscopy 1999;15:813-817. Boytim MJ, Smith JP, Fischer DA, Quick DC: Arthroscopic posteromedial visualization of the knee. Clip Orthop 1995;310:82-86.
1. 01.188 Figures 59a and 59b show the radiographs of an 8-year-old boy who has
2. atraumatic recurrent lateral dislocation of the left patella. Examination reveals
3. no fixed genu varum or valgum, and the lower extremity lengths are equal. The
4. Q angle is 25°. The extended hips show internal rotation of 40° and external
5. rotation of 60°, with a neutral thigh-foot angle. There is no generalized
6. ligamentous laxity. Treatment should consist of
7. 1- femoral rotational osteotomy.
8. 2- tibial rotational osteotomy.
9. 3- tibial tuberosity transfer (Fulkerson, Elmslie-Trillat,
10. or Hauser).
11. 4- tenodesis of the semitendinosus to the patella.
12. 5- patellectomy and vastus medialis advancement.
1. answer
1. back
1. A
1. B
1. Figures 59
1. Question 01.188
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hall JE, Micheli LJ, McManama GB Jr- Semitendinosus tenodesis for recurrent subluxation or dislocation of the patella. Clin Orthop 1979;144:31-35. Sponseller PD, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1231-1329. Tolo V: Fractures and dislocations about the knee, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 431-458. Lefts RM, Davidson D, Beaule P: Semitendinosus tenodesis for repair of recurrent dislocation of the patella in children. J Pediatr Orthop 1999;19:742-747.
1. 01.189 The posterior (Thompson) approach to the proximal radial shaft lies between
2. the
3. 1- extensor carpi ulnaris and anconeus.
4. 2- extensor carpi ulnaris and extensor carpi radialis longus.
5. 3- extensor carpi radialis longus and extensor carpi radialis brevis.
6. 4- extensor carpi radialis brevis and extensor digitorum communis.
7. 5- brachioradialis and extensor carpi radialis longus.
1. answer
1. back
1. Question 01.189
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, Lippincott Williams & Wilkins, 1984, pp 109-139. Thompson BE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309.
1. 01.190 Concurrent injuries to which of the following structures results in an increased
2. osteogenic response to fracture?
3. 1- Head
4. 2- Liver
5. 3- Chest
6. 4- Major artery
7. 5- Bladder
1. answer
1. back
1. Question 01.190
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Kushwaha VP, Garland DG: Extremity fractures in the patient with a traumatic brain injury. J Am Acad Orthop Surg 1998;6:298-307. Spencer RF: The effect of head injury on fracture healing: A quantitative assessment. J Bone Joint Surg Br 1987;69:525-528.
1. 01.191 A 29-year-old man sustained a talar neck fracture with an associated
2. dislocation of the body of the talus from the subtalar and tibiotalar joints. He
3. was treated with immediate open reduction and internal fixation. Twelve weeks
4. later, the fracture has united, and lucency is observed in the superior
5. subchondral bone of the talar body. The next most appropriate step in
6. management should consist of
7. 1- bone grafting of the talar neck and body.
8. 2- application of an ultrasound bone stimulator.
9. 3- a brace with calipers.
10. 4- MRI to assess body viability.
11. 5- protected weight bearing.
1. answer
1. back
1. Question 01.191
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998,
3. pp 201-213. Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, p 1176.
1. 01.192 Within the normal healthy lumbar disk of a young person, proteoglycans
2. constitute a
3. 1- low percent of dry weight within the annulus, a high percent of dry weight within the
4. nucleus, and interact with H2O to primarily resist compression.
5. 2- low percent of dry weight within the annulus, a high percent of dry weight within the
6. nucleus, and interact with H2O to primarily resist tension.
7. 3- high percent of dry weight within the annulus, a low percent of dry weight within the
8. nucleus, and interact with H2O to primarily resist compression.
9. 4- high percent of dry weight within the annulus, a low percent of dry weight within the
10. nucleus, and interact with H2O to primarily resist tension.
11. 5- high percent of dry weight within the annulus, a low percent of dry weight within the
12. nucleus, and have no interaction with H2O.
1. answer
1. back
1. Question 01.192
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 548-556. Buckwalter JA, Pedrini-Mille A, Pedrini V, Tudisco C: Proteoglycans of human infant intervertebral disc: Electron microscopic and biochemical studies. J Bone Joint Surg Am 1985;67:284-294.
1. 01.193 A 40-year-old woman has right shoulder pain and limited range of motion.
2. History reveals that she sustained a right proximal humerus fracture 10 years
3. ago and was treated with a sling and physical therapy. Examination reveals
4. active forward elevation of 100°, active external rotation of 0°, and passive
5. internal rotation to L5. Passive shoulder motion is the same. Plain radiographs
6. of the shoulder are shown in Figures 60a and 60b. Treatment should now
7. consist of
8. 1- arthroscopic debridement.
9. 2- humeral osteotomy.
10. 3- core decompression.
11. 4- humeral head replacement.
12. 5- capsular release.
1. answer
1. back
1. A
1. B
1. Figures 60
1. Question 01.193
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Norris TR, Green A, McGuigan FX: Late prosthetic arthroplasty for displaced proximal humerus fractures. J Shoulder Elbow Surg 1995;4:271-280. Schlegel TF, Hawkins RJ: Displaced proximal humeral fractures: Evaluation and treatment. J Am Acad Orthop Surg 1994;2:54-78.
1. 01.194 The lateral crista of the trochlea develops from what secondary ossification
2. center?
3. 1- Medial condylar epiphysis
4. 2- Lateral condylar epiphysis
5. 3- Medial epicondylar apophysis
6. 4- Lateral epicondylar apophysis
7. 5- Olecranon apophysis
1. answer
1. back
1. Question 01.194
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Wilkins KE: Fractures and dislocations of the elbow region: Part L The elbow region: General concepts in the pediatric patient, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 653-669.
1. 01.195 A 40-year-old man sustains a rupture of the Achilles tendon while playing
2. recreational basketball. If he undergoes surgical repair rather than nonsurgical
3. management, the patient should be told to expect a
4. 1- lower skin complication rate and a longer period of rehabilitation.
5. 2- lower re-rupture rate and a longer period of rehabilitation.
6. 3- higher re-rupture rate and a shorter rehabilitation.
7. 4- higher skin complication rate and a higher re-rupture rate.
8. 5- higher skin complication rate and a lower re-rupture rate.
1. answer
1. back
1. Question 01.195
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ: Disorders of tendons, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 786-861. Troop RL, Losse GM, Lane JG, Robertson DB, Hastings PS, Howard ME: Early motion after repair of Achilles tendon ruptures. Foot Ankle Int 1995;16:705-709.
1. 01.196 Which of the following is considered the most sensitive sensory test for
2. detecting early carpal tunnel syndrome?
3. 1- Light touch sensation
4. 2- Pinprick sensation
5. 3- Two-point discrimination
6. 4- Moving two-point discrimination
7. 5- Semmes-Weinstein monofilament
1. answer
1. back
1. Question 01.196
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, B., American Academy of Orthopaedic Surgeons, 1996, pp 221-231. Szabo RM, Gelberman RH, Dimick MD: Sensibility testing in patients with carpal tunnel syndrome. J Bone Joint Surg Am 1984;66:60-64.
1. 01.197 A 16-year-old boy has had pain in the lateral ankle and hindfoot after sustaining
2. a minor ankle sprain 6 months ago. The pain is worse with any twisting activity
3. of the foot. Examination reveals normal alignment of the foot and ankle. An AP
4. radiograph of the ankle and foot is normal. A lateral radiograph is shown in
5. Figure 61. What is the most likely cause of his persistent pain?
6. 1- Fracture of the lateral process of the talus
7. 2- Fracture of the anterior process of the calcaneus
8. 3- Fracture of the tibial plafond
9. 4- Talocalcaneal coalition
10. 5- Stress fracture of the calcaneus
1. answer
1. back
1. Figure 61
1. Question 01.197
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Richardson EG: Flatfoot in children and adults, in Coughlin MJ, Mate RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science,
3. 1999, pp 702-733. Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
1. 01.198 A patient who underwent total knee arthroplasty 2 years ago has a range of
2. motion of 0° to 60°. The implants are well fixed, and the knee is well aligned
3. on AP radiographs. Lateral .radiographs show that the femoral component is
4. appropriately sized and the tibial component is in 5° of anterior tilt. Treatment
5. should consist of
6. 1- revision of the femoral component.
7. 2- revision of the tibial component.
8. 3- closed knee manipulation.
9. 4- open lysis of adhesions.
10. 5- open quadricepsplasty.
1. answer
1. back
1. Question 01.198
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 317-322.
1. 01.199 When compared to plate fixation, antegrade intramedullary nailing of humeral
2. shaft fractures results in
3. 1- better elbow function.
4. 2- a higher rate of union.
5. 3- a higher rate of complications.
6. 4- a higher rate of infection.
7. 5- longer surgical time.
1. answer
1. back
1. Question 01.199
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267. McCormack RG, Brien D, Buckley RE, McKee MD, Powell J, Schemitsch EH: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective randomized trial. J Bone Joint Surg Br 2000;82:336-339.
1. 01.200 Which of the following groups is most at risk for osteoporosis?
2. 1- Caucasian men
3. 2- Caucasian women
4. 3- African-American women
5. 4- Hispanic men
6. 5- Hispanic women
1. answer
1. back
1. Question 01.200
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Lane JM, Nydick M: Osteoporosis: Current modes of prevention and treatment. J Am Acad Orthop Surg 1999;7:19-31. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-115
1. 01.201 A 49-year-old man with advanced glenohumeral arthritis undergoes total
2. shoulder replacement. Following surgery, he reports pain relief but now has
3. weakness when using his arm for activities in front of his body. He is unable to
4. hold the dorsum of his hand away from his back. The weakness is most likely
5. related to what muscle?
6. 1- Supraspinatus
7. 2- Subscapularis
8. 3- Infraspinatus
9. 4- Deltoid
10. 5- Pectoralis major
1. answer
1. back
1. Question 01.201
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Gerber C, Farrow MD: Isolated tears of the subscapularis tendon. Orthop Trans 1995;19:457. Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
1. 01.202 An ankle fracture heals with an anatomically aligned mortise and 2 mm of
2. displacement of the distal fibula fracture. What affect will these findings have
3. on the tibiotalar joint?
4. 1- Decreased contact loading
5. 2- Increased contact loading
6. 3- Increased external rotation
7. 4- Increased medial-lateral translation
8. 5- Normal loading, rotation, and translation
1. answer
1. back
1. Question 01.202
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Brown TD, Hurlbut PT, Hale JE, et a1: Effects of imposed hindfoot constraint on ankle contact mechanics for displaced lateral malleolar fractures. J Orthop Trauma 1994;8:511-519. Michelson JD: Fractures about the ankle. J Bone Joint Surg Am 1995;77:142-152.
1. 01.203 Figure 62 shows the MRI scan of a 30-year-old male volleyball player who has
2. had shoulder pain for the past 6 months. Which of the following physical
3. findings in the shoulder would be most consistent with this lesion?
4. 1- Weakness of internal rotation
5. 2- Weakness of external rotation
6. 3- Weakness of abduction
7. 4- Positive impingement sign
8. 5- Positive apprehension sign
1. answer
1. back
1. Figure 62
1. Question 01.203
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Thompson RC Jr, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187. Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
1. 01.204 In cemented polyethylene acetabular components, the reported average
2. polyethylene wear rate on a yearly basis is how many millimeters?
3. 1- 0.01
4. 2- 0.05
5. 3- 0.1
6. 4- 1.0
7. 5- 2.0
1. answer
1. back
1. Question 01.204
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Jasty M, Goetz DD, Bragdon CP, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
1. 01.205 The Lisfranc ligament connects what two bones?
2. 1- Middle cuneiform and first metatarsal
3. 2- Middle cuneiform and second metatarsal
4. 3- Medial cuneiform and first metatarsal
5. 4- Medial cuneiform and second metatarsal
6. 5- Medial cuneiform and middle cuneiform
1. answer
1. back
1. Question 01.205
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Sanafian SK: Osteology, in Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 37-112. Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. SL Louis, MO, Harcourt Health Science, 1999, pp 1090-1209.
1. 01.206 The arrow in the axial MRI scan shown in Figure 63 is pointing to what
2. muscle?
3. 1- Gracilis
4. 2- Adductor brevis
5. 3- Sartorius
6. 4- Semitendinosus
7. 5- Pectineus
1. answer
1. back
1. Figure 63
1. Question 01.206
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Hoppenfeld S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 401-429.
1. 01.207 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.208 Which of the following conditions will most likely cause disability at some
2. point in the life of a patient with achondroplasia?
3. 1- Degenerative joint disease of the knees
4. 2- Cervical instability with myelopathy
5. 3- Scoliosis of the thoracic or lumbar spine
6. 4- Spinal stenosis
7. 5- Progressive contractures of the limbs
1. answer
1. back
1. Question 01.208
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Pyeritz RE, Sack GH Jr, Udvarhelyi GB: Thoracolumbosacral laminectomy in achondroplasia: Long-term results in 22 patients. Am J Med Genet 1987;28:433-444. Tolo VT: Spinal deformity in skeletal dysplasia, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY, Raven Press, 1994, pp 369-393.
1. 01.209 The use of calcium supplements should be
2. 1- encouraged in girls at puberty to help prevent osteoporosis.
3. 2- restricted until menopause to decrease the risk of renal stones.
4. 3- left to individual preference until perimenopause, then started routinely.
5. 4- started only after a bone mineral density study indicates a deficiency of 2 standard
6. deviations.
7. 5- started only after a bone mineral density study indicates a deficiency of 1 standard
8. deviation.
1. answer
1. back
1. Question 01.209
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 127-139.
1. 01.210 The bending strength of fractured long bones fixed with an experimental
2. compression plate is compared with unfractured controls. What statistical test
3. should be used to compare the mean bending strength of the two groups?
4. 1- Student's t test
5. 2- Analysis of variance
6. 3- Regression analysis
7. 4- Chi-square test
8. 5- Wilcoxon two-sample test
1. answer
1. back
1. Question 01.210
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 397-446.
1. 01.211 Which of the following factors has been shown to be an independent risk factor
2. for infection after open reduction and internal fixation of the calcaneus through
3. an extensile lateral incision?
4. 1- Age of greater than 50 years
5. 2- History of smoking
6. 3- A comminuted posterior facet
7. 4- Extension of the fracture into the sustentaculum
8. 5- Use of phenytoin
1. answer
1. back
1. Question 01.211
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Folk JW, Stan AJ, Early JS: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999;13:369-372.
1. 01.212 Examination of a 65-year-old woman who sustained a stroke 18 months ago
2. reveals a clenched fist deformity that is causing significant hygiene problems
3. because of skin maceration and malodor. She has no observed voluntary motor
4. control of the hand or forearm. Management should consist of
5. 1- open phenol blocks.
6. 2- botulinum toxin blocks.
7. 3- proximal interphalangeal and distal interphalangeal arthrodesis.
8. 4- flexor tenotomies.
9. 5- a superficialis-to-profundus tendon transfer.
1. answer
1. back
1. Question 01.212
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Braun RN, Vise GT, Roger B: Preliminary experience with superficialis-to profundus tendon transfer in the hemiplegic upper extremity. J Bone Joint Surg Am 1974;56:466-472. Hisex MS, Keenan MAE: Orthopaedic management of upper extremity dysfunction following stroke or brain injury, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 287-324.
1. 01.213 Revision of a failed acetabular component with a bipolar endoprosthesis and
2. acetabular bone grafting is most likely to fail because of what mechanism?
3. 1- Osteolysis
4. 2- Femoral stem loosening
5. 3- Recurrent dislocation
6. 4- Bipolar head migration
7. 5- Bipolar head disengagement
1. answer
1. back
1. Question 01.213
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Brien WW, Bruce WJ, Salvati EA, Wilson PD 1r, Pellicci PM: Acetabular reconstruction with a bipolar prosthesis and morseled bone grafts. J Bone Joint Surg Am 1990;72:1230-1235. McFarland EG, Lewallen DG, CabaneIa ME: Use of bipolar endoprosthesis and.bone grafting for acetabular reconstruction. Clin Orthop 1991; 268:128-129. Papagelopoulus PJ, Lewallen DG, Cabanela ME, McFarland EG, Wallnichs SL: Acetabular reconstruction using bipolar endoprosthesis and bone grafting in patients with severe bone deficiency. Clin Orthop 1995;314:170-184.
1. 01.214 An 18-year-old man sustains the proximal femur fracture shown in Figures 64a
2. and 64b. Definitive management should consist of
3. 1- traction for 6 weeks.
4. 2- a functional brace.
5. 3- a 135° angle sliding hip screw.
6. 4- a 95° fixed angle plate.
7. 5- antegrade nailing with transverse screws.
1. answer
1. back
1. A
1. B
1. Figures 64
1. Question 01.214
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kinast C, Bolhofner BR, Mast 1W, Ganz R: Subtrochanteric fractures of the femur: Results of treatment with the 95 degrees blade-plate. Clin Orthop 1989;238:122-130.
1. 01.215 In the treatment of femoral shaft fractures, the lowest union rate has been
2. reported after which of the following types of nailing?
3. 1- Reamed antegrade locked
4. 2- Reamed antegrade unlocked
5. 3- Reamed retrograde locked
6. 4- Unreamed antegrade locked
7. 5- Unreamed retrograde locked
1. answer
1. back
1. Question 01.215
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Moed BR, Watson JT, Cramer KE, Karges DE, Teefey JS: Unreamed retrograde intramedullary nailing of fractures of the femoral shaft. J Orthop Trauma 1998;12334-342. Moed BR, Watson JT: Retrograde intramedullary nailing, without reaming, of fractures of the femoral shaft in multiply injured patients. J Bone Joint Surg Am 1995;77:1520-1527.
1. 01.216 A 36-year-old man has pain in the metatarsophalangeal (MTP) joint of the
2. great toe with all weight-bearing activities, and management consisting of shoe
3. modification and an insert has failed to provide relief. Examination reveals a
4. painful 10° arc of motion. Radiographs show degenerative changes with dorsal
5. and medial osteophytes and joint narrowing. Treatment should now consist of
6. 1- excision of the osteophytes and the dorsal third of the metatarsal head.
7. 2- a dorsiflexion osteotomy of the metatarsal head.
8. 3- resection arthroplasty of the MTP joint.
9. 4- a Silastic implant of the MTP joint.
10. 5- arthrodesis of the MTP joint.
1. answer
1. back
1. Question 01.216
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Mann RA, Clanton TO: Hallux rigidus: Treatment by cheilectomy. J Bone Joint Surg Am 1988;70:400-406. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 151-161. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 605-633.
1. 01.217 A 14-year-old boy who plays football sustains a valgus force to his knee.
2. Examination reveals a 1+ effusion and decreased range of motion. Lachman
3. test results are negative. He has no joint line tenderness, but he does have
4. tenderness over the proximal origin of the medial collateral ligament and pain
5. with valgus stressing. Initial plain radiographs of the knee are normal. Further
6. evaluation should include
7. 1- arthrography.
8. 2- MRI.
9. 3- a bone scan.
10. 4- emergent arthroscopy.
11. 5- stress radiographs.
1. answer
1. back
1. Question 01.217
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Sponseller PD, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1231-1329. Cook PC, Leit ME: Issues in the pediatric athlete. Orthop Clin North Am 1995;26:453-464.
1. 01.218 A 35-year-old man sustained an isolated closed displaced bicondylar tibial
2. plateau fracture after being struck by a car. Reduction and internal fixation of
3. both condyles can be most safely achieved using which of the following
4. surgical approaches?
5. 1- Isolated anterior midline
6. 2- Isolated lateral parapatellar
7. 3- Isolated posteromedial
8. 4- Combined anterolateral and posteromedial
9. 5- Combined anterior midline and posterior transpopliteal
1. answer
1. back
1. Question 01.218
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Georgiadis GM: Combined anterior and posterior approaches for complex tibial plateau fixations. J Bone Joint Surg Br 1994;76:285-289.
1. 01.219 Which of the following conditions is most commonly associated with
2. congenital fibular hemimelia?
3. 1- Congenital absence of the patella
4. 2- Congenital absence of the first ray
5. 3- Genu varum
6. 4- Equinovarus ankle
7. 5- Talocalcaneal coalition
1. answer
1. back
1. Question 01.219
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Grogan DP, Holt GR, Ogden JA: Talocalcaneal coalition in patients who have fibular hemimelia or proximal femoral focal deficiency: A comparison of the radiographic and pathological findings. J Bone Joint Surg Am 1994;76:1363-1370. Epps CH Jr, Schneider PL: Treatment of hemimelias of the lower extremity: Long term results. J Bone Joint Surg Am 1989;71273-277.
1. 01.220 A 58-year-old woman has severe neck pain after falling at home. Examination
2. reveals intact deltoid strength, 2/5 weakness in the rest of the right upper
3. extremity, and 2/5 weakness in the left upper extremity, except for a grip
4. strength of 3/5. She has 4/5 strength in both lower extremities, good rectal
5. tone, and an intact bulbocavernosus reflex. Sensation is intact. Which of the
6. following conditions best characterizes her neurologic injury?
7. 1- A complete spinal cord injury
8. 2- Bilateral brachial plexopathies
9. 3- Multilevel cervical radiculopathy
10. 4- Anterior cord syndrome
11. 5- Central cord syndrome
1. answer
1. back
1. Question 01.220
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. McGuire RA: Physical examination in spinal trauma, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA. WB Saunders, 1998, pp 17-27. Bohiman HH, Docker TB: Spine trauma in adults: Spine and spinal cord injuries, in Herkowitz HN, Eismont FJ, Garfin SR, Bell GR, Balderston RA, Wiesel SW (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 889-914.
1. 01.221 A 25-year-old construction worker reports a mass on the dorsum of his hand
2. that is painful with strenuous use. Examination reveals a 4 x 2 x 1 cm soft mass
3. that overlies the proximal portions of the index and middle metacarpals. It
4. moves with flexion and extension of those digits, becomes firmer with forceful
5. grasp, and does not transilluminate. What is the most likely diagnosis?
6. 1- Dorsal wrist ganglion
7. 2- Extensor tenosynovitis
8. 3- Giant cell tumor of the tendon sheath
9. 4- Carpal boss
10. 5- Anomalous extensor muscle
1. answer
1. back
1. Question 01.221
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Tan ST, Smith PJ: Anomalous extensor muscles of the hand: A review. J Hand Sung Am 1999;24:449-455. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1950-1987.
1. 01.222 Which of the following cytokines have been implicated in the pathogenesis of
2. rheumatoid arthritis?
3. 1- Fibroblastic growth factor and transforming growth factor
4. 2- Parathyroid hormone-related protein and interferon-gamma
5. 3- Interleukin- 1 and tumor necrosis factor
6. 4- Interleukin-4 and granulocyte-macrophage colony-stimulating factor
7. 5- Interleukin- 10 and vascular endothelial growth factor
1. answer
1. back
1. Question 01.222
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty 3H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 205-216. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 490-530.
1. 01.223 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.224 An 11-year-old girl has had progressive medial midfoot pain bilaterally for the
2. past 6 months. Her mother states that the child's feet appeared normal until the
3. pain started, and she is concerned about the development of flatfeet. What is
4. the most likely diagnosis?
5. 1- Physiologic pes planus
6. 2- Charcot foot
7. 3- Posterior tibial tendon insufficiency
8. 4- Congenital vertical talus
9. 5- Accessory navicular
1. answer
1. back
1. Question 01.224
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Prichasuk S, Sinphurmsuksknl O: Kidner procedure for symptomatic accessory navicular and its relation to pes planus. Foot Ankle Int 1995;16:500-503.
1. 01.225 Which of the following is considered the most important factor in preventing
2. failure of fixation of displaced femoral neck fractures?
3. 1- Use of a compression screw and side plate
4. 2- Use of cannulated screws
5. 3- Accuracy of reduction
6. 4- Reduction on a traction table
7. 5- Release of a capsular hematoma
1. answer
1. back
1. Question 01.225
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Chug D, Jaglal SB, Schatzker J: Predictors of early failure of fixation in the treatment of displaced subcapital hip fractures. J Orthop Trauma 1998;12:230-234. Swiontkowski MF: Intracapsular fractures of the hip. J Bone Joint Surg Am 1994;76:129-138.
1. 01.226 Item deleted after statistical review
2. (and no answer or references cited)
1. back
1. next question
1. 01.227 The process of host repair following osteonecrosis is referred to as
2. 1- haversian remodeling.
3. 2- osteogenesis.
4. 3- osteoinduction.
5. 4- fracture healing.
6. 5- creeping substitution.
1. answer
1. back
1. Question 01.227
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds)- Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.228 What type of knee dislocation is most likely to be irreducible by closed means?
2. 1- Posterior
3. 2- Anterior
4. 3- Lateral
5. 4- Posterolateral
6. 5- Posteromedial
1. answer
1. back
1. Question 01.228
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 151-155. Quinlan AG, Sharrard WJW: Posterolateral dislocation of the knee with capsular interposition. J Bone Joint Surg Br 1958;40:660-663.
1. 01.229 A 16-year-old boy who is 5 ft 4 in tall reports pain in the knees and ankles.
2. Examination reveals that his knees are in 15° of valgus. The articular surfaces
3. of the knees and ankles are irregular, and the femoral heads are slightly
4. flattened. A lateral radiograph shows that the patellae have a double layer.
5. What is the most likely diagnosis?
6. 1- Kneist syndrome
7. 2- Spondyloepiphyseal dysplasia congenita
8. 3- Multiple epiphyseal dysplasia
9. 4- Achondroplasia
10. 5- Dyschondrosteosis
1. answer
1. back
1. Question 01.229
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Dietz FR, Matthews KD: Update on the genetic bases of disorders with orthopaedic manifestations. J Bone Joint Surg Am 1996;78:1583-1598. Spranger J: The epiphyseal dysplasias. Clip Orthop 1976;114:46-59. Sheffield EG: Double-layered patella in multiple epiphyseal dysplasia: A valuable clue in the diagnosis. J Pediatr Orthop 1998;18:123-128.
1. 01.230 What is the most common primary malignancy that metastasizes to the bones
2. of the hand?
3. 1- Breast
4. 2- Prostate
5. 3- Renal
6. 4- Colon
7. 5- Lung
1. answer
1. back
1. Question 01.230
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 369-376. Athanasian EA: Bone and soft-tissue tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2223-2253.
1. 01.231 A 14-year-old girl has been limping and has had pain with weight bearing on
2. the right lower leg for the past 48 hours. She has a temperature of 100°F
3. (37.7°C). She prefers a prone position with the right hip and knee extended.
4. Pain is produced by placing the hip in flexion, abduction, and external rotation.
5. Which of the following studies will best confirm the diagnosis?
6. 1- Hip joint aspiration
7. 2- AP radiograph of the pelvis
8. 3- Oblique radiograph of the lumbar spine
9. 4- CT of the abdomen
10. 5- MRI of the pelvis
1. answer
1. back
1. Question 01.231
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Bollow M, Braun 1, Biedermann T, et al: Use of contrast-enhanced MR imaging to detect sacroiliitis in children. Skeletal Radiol 1998;27:606-616. Tisserant R, Loeuille D, Pere P, Gancher A, Ponrel J, Blum A: Septic sacroiliitis during the postpartal period: Diagnostic contribution of magnetic resonance imaging. Rev Rheum Engl Ed 1999;66:512-515.
1. 01.232 A surgeon who is planning a total elbow arthroplasty would like to use a
2. prosthesis that he helped to develop. A royalty payment is received each time
3. the prosthesis is used. What is the surgeon's ethical responsibility?
4. 1- The prosthesis should not be used.
5. 2- The prosthesis can be used, but the royalty payment information should not be
6. discussed with the patient.
7. 3- The royalty payment information should be included on the informed consent
8. document but not discussed with the patient.
9. 4- The patient should be informed that the surgeon receives a royalty payment for using
10. the prosthesis.
11. 5- The surgeon should offer to split the royalty payment with the patient.
1. answer
1. back
1. Question 01.232
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Wenger NS, Liu H, Lieberman JR: Teaching medical ethics to orthopaedic surgery residents. J Bone Joint Surg Am 1998;80:1125-1131.
1. 01.233 In trauma patients older than age 60 years, mortality most closely correlates
2. with
3. 1- the injury severity score (ISS).
4. 2- the extremity abbreviated injury score (AIS).
5. 3- the need for orthopaedic surgery.
6. 4- the timing of orthopaedic surgery.
7. 5- a history of type I diabetes mellitus.
1. answer
1. back
1. Question 01.233
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Tornetta P BI, Mostafavi H, Riina J, et al: Morbidity and mortality in elderly trauma patients. J Trauma 1999;46:702-706.
1. 01.234 A 46-year-old woman has had plantar heel pain for the past 5 months. She
2. reports that the pain is most severe when she arises out of bed in the morning
3. and when she stands after being seated for a period of time. Initial management
4. should consist of
5. 1- surgical lengthening of the Achilles tendon.
6. 2- surgical release of the plantar fascia.
7. 3- a custom orthosis.
8. 4- a stretching program and a cushioned heel insert.
9. 5- a corticosteroid injection.
1. answer
1. back
1. Question 01.234
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Pfeffer G, Bacchetti P, Deland J, et al: Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int 1999;20:214-221. Richardson EG: Heel pain, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1090-1209.
1. 01.235 The triceps reflex is largely a function of what neurologic level?
2. 1- C5
3. 2- C6
4. 3- C7
5. 4- C8
6. 5- T1
1. answer
1. back
1. Question 01.235
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Snider RK (ed): Essentials of Musculoskeletal Care. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 491-546.
1. 01.236 A 19-year-old female swimmer has had right shoulder pain for the past 5 years.
2. Although she had responded previously to physical therapy, she has been in
3. rehabilitation for the past 6 months without improvement. Examination reveals
4. active total elevation of 170°, active external rotation of 70°, and passive
5. internal rotation to T3. There is symmetric 2+ glenohumeral translation in the
6. anterior, posterior, and inferior directions and a positive Neer impingement
7. sign. Treatment should consist of
8. 1- open Bankart repair.
9. 2- an inferior capsular shift.
10. 3- arthroscopic coracoacromial ligament resection.
11. 4- arthroscopic acromioplasty.
12. 5- arthroscopic Bankart repair.
1. answer
1. back
1. Question 01.236
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multi-directional instability of the shoulder. A preliminary report J Bone Joint Surg Am 1980;62:897-908. Schenk TJ, Brems JJ: Multi-directional instability of the shoulder Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1998;6:65-72.
1. 01.237 What is the most common complication at a minimum of 1 year after treatment
2. with a reamed antegrade nail for a femoral shaft fracture?
3. 1- Nonunion
4. 2- Malunion
5. 3- Trendelenburg gait
6. 4- Hip discomfort
7. 5- Osteonecrosis of the femoral head
1. answer
1. back
1. Question 01.237
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Bain GI, Zacest AC, Paterson DC, Middleton J, Pohl AP: Abduction strength following intramedullary nailing of the femur. J Orthop Trauma 1997;11:93-97.
1. 01.238 A 13-year-old boy has nonrigid Scheuermann's kyphosis. Weight-bearing
2. radiographs show a kyphosis of 70° from T7 to L1, with scoliosis that
3. measures 10° at Risser 2 maturity. Management should consist of
4. 1- postural exercises and analgesics.
5. 2- a Charleston bending brace.
6. 3- an extension-type spinal orthosis.
7. 4- posterior spinal fusion with instrumentation.
8. 5- anterior spinal release and posterior spinal instrumentation.
1. answer
1. back
1. Question 01.238
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Lowe TG: Scheuermann disease. J Bone Joint Surg Am 1990;72:940-945. Tribes CB: Scheuermann's kyphosis in adolescents and adults: Diagnosis and management. J Am Acad Orthop Surg 1998;6:36-43.
1. 01.239 A 21-year-old male wrestler sustained a right posterolateral elbow dislocation
2. with an associated type I coronoid fracture 2 years ago. Management at the
3. time of injury consisted of application of a splint for 2 weeks. He now reports
4. recurrent elbow subluxation and pain. What is the most likely cause of the
5. instability?
6. 1- Displaced coronoid process fracture
7. 2- Insufficiency of the lateral ulnar collateral ligament
8. 3- Insufficiency of the anterior band of the medial collateral ligament
9. 4- Insufficiency of the posterior band of the medial collateral ligament
10. 5- Anterior capsular insufficiency
1. answer
1. back
1. Question 01.239
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Josefsson PO, Johnell O, Gentz CF: Long-term sequelae of simple dislocation of the elbow. J Bone Joint Surg Am 1984;66:927-930. Nestor BJ, O'Driscoll SW, Morrey BF: Ligamentous reconstruction for posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1992;74:1235-1241. O'Driscoll SW, Money BF, Korinek S, An KN: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
1. 01.240 The degree of ulnar variance is best defined by
2. 1- arthrography.
3. 2- MRI.
4. 3- cineradiographs.
5. 4- stress radiographs.
6. 5- plain radiographs.
1. answer
1. back
1. Question 01.240
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Nagle DJ: Evaluation of chronic wrist pain. J Am Acad Orthop Surg 2000;8:45-55. Epner RA, Bowers WH, Guilford WB: Ulnar variance: The effect of wrist positioning and roentgen filming technique. J Hand Surg Am 1982;7:298-305.
1. 01.241 An 18-year-old woman has had left hip pain for the past 2 months.
2. Examination reveals audible snapping with extension of a flexed, abducted,
3. and externally rotated hip. What study is most likely to establish the diagnosis?
4. 1- Bone scan
5. 2- Iliopsoas bursography
6. 3- Plain radiography
7. 4- Hip arthrography
8. 5- Hip arthroscopy
1. answer
1. back
1. Question 01.241
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Schaberg JF, Harper MC, Allen WC: The snapping hip syndrome. Am J Sports Med 1984;12:361-365. Jacobson T, Allen WC: Surgical correction of the snapping iliopsoas tendon. Am J Sports Med 1990;18:470-474.
1. 01.242 What metabolic bone disease is associated with abnormal osteoclastic
2. function?
3. 1- X-linked hypophosphatemic rickets
4. 2- Fanconi's syndrome
5. 3- Osteopetrosis
6. 4- Osteomalacia
7. 5- Paget's disease of bone
1. answer
1. back
1. Question 01.242
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL. American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Shapiro F: Osteopetrosis: Current clinical considerations. Clin Orthop 1993;294:344.
1. 01.243 The Glasgow Coma Scale categorizes the neurologic status of a multiply
2. injured patient by assessing verbal response, motor response, and
3. 1- orientation.
4. 2- response to commands.
5. 3- pupillary response.
6. 4- withdrawal to pain.
7. 5- eye opening response.
1. answer
1. back
1. Question 01.243
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Turen CH, Dube MA, LeCroy MC: Approach to the polytraumatized patient with musculoskeletal injuries. J Am Acad Orthop Surg 1999;7:154-165. Teasdale G, Jennett B: Assessment of coma and impaired consciousness: A practical scale. Lancet 1974;2:81-84.
1. 01.244 Which of the following is considered the preferred total knee design for a
2. patient with a history of a patellectomy?
3. 1- Posterior cruciate ligament-retaining
4. 2- Posterior cruciate ligament-substituting
5. 3- Rotating hinge
6. 4- Unicondylar
7. 5- Meniscal bearing
1. answer
1. back
1. Question 01.244
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582. Paletta GA Jr, Laskin RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
1. 01.245 A child with chronic recurrent multifocal osteomyelitis has painful swelling
2. and tenderness in the right medial clavicle with no fluctuance. She has a
3. temperature of 99°F (37.2°C). The palms and soles show pustular lesions.
4. Radiographs reveal periosteal new bone formation in the medial clavicle.
5. Management should consist of
6. 1- a steroid injection into the medial clavicle.
7. 2- oral nonsteroidal anti-inflammatory drugs.
8. 3- IV administration of oxacillin for 4 weeks.
9. 4- IV administration of gamma globulin.
10. 5- incision and drainage of the medial clavicle.
1. answer
1. back
1. Question 01.245
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Godette GA, Murray DP, Gruel CR, Leonard 1C: Chronic recurrent multifocal osteomyelitis. Orthopedics 1992;15:520-521, 525-526. Bjorksten B, Gustavson K-H, Eriksson B, Lindholm A, Nordstrom S: Chronic recurrent multifocal osteomyelitis and pustulosis palmoplantaris. J Pediatr 1978;93:227-231. Stanton RP, Lopez-Sosa FH, Doidge R: Chronic recurrent multifocal osteomyelitis. Orthop Rev 1993;22:229-233.
1. 01.246 A 32-year-old woman reports right shoulder pain and has difficulty with
2. overhead activities. History reveals that she underwent an open anterior labral
3. repair and capsular shift to treat anterior glenohumeral instability 3 years ago.
4. Examination reveals tenderness over the anterior shoulder, active and passive
5. total elevation of 120°, and external rotation of 30°. Shoulder strength is
6. normal. Plain radiographs are normal. Physical therapy has failed to provide
7. relief. Treatment should now consist of
8. 1- arthroscopic acromioplasty.
9. 2- biceps tenodesis.
10. 3- open subscapularis lengthening and capsular release.
11. 4- humeral head replacement.
12. 5- derotational humeral osteotomy.
1. answer
1. back
1. Question 01.246
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Bigliani LU: Glenohumeral instability repairs: Complications and failures, in Bigliani LU (ed): The Unstable Shoulder. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 99-106. MacDonald PB, Hawkins RJ, Fowler PJ, Miniaci A: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
1. 01.247 What statistical test should be used to determine whether a significant
2. difference exists between the means of more than two independent samples
3. with normal distributions?
4. 1- Student's t test
5. 2- Analysis of variance
6. 3- Regression analysis
7. 4- Chi-square test
8. 5- Kruskal-Wallis test
1. answer
1. back
1. Question 01.247
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 623-665. Freedman KB, Bernstein J: Sample size and statistical power in clinical orthopaedic research. J Bone Joint Surg Am 1999;81:1454-1460.
1. 01.248 A female patient is most likely the victim of domestic abuse when the
2. 1- injury is inconsistent with the offered explanation.
3. 2- spouse does not express any interest in the patient's injuries.
4. 3- patient expresses an overly animated affect.
5. 4- patient has a lower socioeconomic status.
6. 5- patient is eager to leave the hospital or clinic.
1. answer
1. back
1. Question 01.248
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Zillmer DA: Domestic violence: The role of the orthopaedic surgeon in identification and treatment. J Am Acad Orthop Surg 2000;8:91-96.
1. 01.249 A varus malreduction of a comminuted talar neck fracture will result in
2. 1- varus hindfoot and decreased subtalar motion.
3. 2- increased contact loading of the posterior facet.
4. 3- subtalar instability.
5. 4- anterior ankle impingement.
6. 5- talonavicular subluxation.
1. answer
1. back
1. Question 01.249
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect in the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567. Sangeorzan BJ, Wagner UA, Harrington RIM, Tencer AF: Contact characteristics of the subtalar joint: The effect of talar neck misalignment. J Orthop Res 1992;10:544.-551.
1. 01.250 While performing a revision total knee replacement with a trial component in
2. place, it is noted that the knee has full extension but is loose in flexion. To
3. resolve this flexion-extension discrepancy, the surgeon should
4. 1- use a thicker polyethylene insert.
5. 2- use a larger femoral component with posterior condyle metallic wedges.
6. 3- use a more constrained polyethylene insert.
7. 4- release the posterior capsule.
8. 5- cut more posterior slope on the tibia.
1. answer
1. back
1. Question 01.250
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 323-327.
1. 01.251 During harvest of an anterior iliac crest bone graft, what nerve is at greatest
2. risk for injury?
3. 1- Lateral femoral cutaneous
4. 2- Inguinal
5. 3- Genitofemoral
6. 4- Ilioinguinal
7. 5- Femoral
1. answer
1. back
1. Question 01.251
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, p 1736.
1. 01.252 What structure is at greatest risk for injury when the anterolateral portal is used
2. for ankle arthroscopy?
3. 1- Superficial peroneal nerve
4. 2- Saphenous nerve
5. 3- Sural nerve
6. 4- Deep peroneal nerve
7. 5- Peroneal artery
1. answer
1. back
1. Question 01.252
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Ferkel RD: Arthroscopy of the foot and ankle, in Coughlin MJ, Mate RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Harcourt Health Science, 1999, pp 1257-1268.
1. 01.253 A 53-year-old patient sustains a traumatic anterior dislocation of the
2. glenohumeral joint. The glenohumeral joint is reduced, and postreduction
3. radiographs show a concentric reduction and no evidence of fracture. One
4. week later, the patient cannot actively abduct his arm; however, passive
5. abduction is normal. What is the most likely cause for the lack of active
6. shoulder abduction?
7. 1- Axillary nerve injury
8. 2- Brachial plexus injury
9. 3- Deltoid muscle avulsion
10. 4- Rotator cuff tear
11. 5- Glenoid labral tear
1. answer
1. back
1. Question 01.253
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Stayner LR, Cummings J, Andersen J, Jobe CM: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
1. 01.254 What patient-related risk factor is associated with an increased risk of
2. dislocation in total hip arthroplasty?
3. 1- Obesity
4. 2- Smoking
5. 3- Alcohol intake
6. 4- Male gender
7. 5- Use of systemic steroids
1. answer
1. back
1. Question 01.254
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Espehaug B, Havelin LL Engesaester LB, Langeland N, Vollset SE: Patient related risk factors for early revision of total hip replacements: A population register-based case-control study of 674 revised hips. Acts Orthop Scand 1997;68:207-215. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
1. 01.255 The poor results following surgical treatment of posterior wall acetabular
2. fractures are most commonly associated with
3. 1- sciatic nerve injury.
4. 2- articular comminution.
5. 3- heterotopic ossification.
6. 4- deep venous thrombosis.
7. 5- osteonecrosis of the femoral head.
1. answer
1. back
1. Question 01.255
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Browner BD, Jupiter JB, Levine AM Trafton PB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders 1998, pp 1204-1208. Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78:1632-1645. Saterbak AM, Marsh JL, Nepola JV, Brandser EA, Turbett T: Clinical failure after posterior wall acetabular fractures: The influence of initial fracture patterns. J Orthop Trauma 2000;14:230-237.
1. 01.256 Which of the following conditions is considered a common clinical
2. manifestation of multiple hereditary exostoses?
3. 1- Radial bowing
4. 2- Scoliosis
5. 3- Acetabular dysplasia
6. 4- Genu varum
7. 5- Dwarfism
1. answer
1. back
1. Question 01.256
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Stanton RP, Hansen MO: Function of the upper extremities in hereditary multiple exostoses. J Bone Joint Surg Am 1969;78:68-573. Arms DM, Strecker WB, Manske PR, Schoenecker PL: Management of forearm deformity in multiple hereditary osteochondromatosis. J Pediatr Orthop 1997;17:450-454. Schmale GA, Conrad EU III, Raskind WH: The natural history of hereditary multiple exostoses. J Bone Joint Surg Am 1994;76:986-992.
1. 01.257 When comparing women who sustained a pelvic ring fracture with women
2. who have multiple injuries without a pelvic ring fracture, those with a pelvic
3. fracture have been found to have a higher subsequent rate of
4. 1- miscarriage.
5. 2- infertility.
6. 3- depression.
7. 4- failure to achieve physiologic sexual arousal.
8. 5- urinary difficulties.
1. answer
1. back
1. Question 01.257
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Copeland CE, Bosse MJ, McCarthy ML, et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function. J Orthop Trauma 1997;11:73-81.
1. 01.258 When performing palmar fasciectomy for Dupuytren's contracture, what other
2. procedure should not be performed at the same time?
3. 1- Trigger finger release
4. 2- Intraoperative digital nerve laceration repair
5. 3- Knuckle pad excision
6. 4- Proximal interphalangeal joint arthrodesis
7. 5- Carpal tunnel release
1. answer
1. back
1. Question 01.258
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. American Society for Surgery of the Hand: Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 271-279. Nissenbaum M, Kleinert HE: Treatment considerations in carpal tunnel syndrome with coexistent Dnpuytren's disease. J Hand Surg Am 1980;5:544-547.
1. 01.259 A 44-year-old man has persistent anteromedial joint line pain after sustaining
2. multiple ankle sprains. At the time of surgery, thickening of the deltoid
3. ligament on its most anterior aspect is noted. What fascicle of the deltoid
4. ligament is involved with this anterior impingement?
5. 1- Anterior tibial
6. 2- Anterior tibiotalar
7. 3- Tibionavicular
8. 4- Tibiocalcaneal
9. 5- Talonavicular
1. answer
1. back
1. Question 01.259
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Egol KA, Parisian JS: Impingement syndrome of the ankle caused by a medial meniscoid lesion. Arthroscopy 1997;13:522-525. Mosier-La Clair SM, Monroe MT, Manoli A: Medial impingement syndrome of the anterior tibiotalar fascicle of the deltoid ligament on the talus. Foot Ankle Int 2000;21:385-391.
1. 01.260 What metabolic bone disease is associated with the presence of virus-like
2. inclusion bodies found in the osteoclast?
3. 1- X-linked hypophosphatemic rickets
4. 2- Fanconi's syndrome
5. 3- Osteopetrosis
6. 4- Osteomalacia
7. 5- Paget's disease of bone
1. answer
1. back
1. Question 01.260
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Beaty 1H (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 149-165. Hadjipavlou A, Lander P: Paget disease of the spine. J Bone Joint Surg Am 1991;73:1376-1381. Delmas PD, Mennier P1: The management of Paget's disease of bone. N Engl J Med 1997;336:58-566.
1. 01.261 Pseudoachondroplasia, characterized by disproportionate short-limbed
2. dwarfism and ligamentous laxity, is caused by a deletion or alteration in the
3. gene encoding what protein?
4. 1- Fibroblast growth factor receptor
5. 2- Cartilage oligomeric matrix protein
6. 3- Type 11 collagen
7. 4- Type IX collagen
8. 5- Parathyroid hormone receptor
1. answer
1. back
1. Question 01.261
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 112-131.
1. 01.262 Semmes-Weinstein monofilaments are used to test the foot for abnormal
2. sensory threshold in patients with diabetes mellitus. Loss of protective
3. sensation is the inability to feel
4. 1- the 4.17 filament.
5. 2- the 5.07 filament.
6. 3- the 6.10 filament.
7. 4- 5 g of pressure.
8. 5- 15 g of pressure.
1. answer
1. back
1. Question 01.262
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Jeng C, Michelson J, Mizel M: Sensory thresholds of normal human feet. Foot Ankle Int 2000;21:501-504. Rith-Najarian SJ, Stolusky T, Gohdes DM: Identifying diabetic patients at him risk for lower-extremity amputation in a primary health care setting: A prospective evaluation of simple screening criteria. Diabetes Care 1992;15:1386-1389.
1. 01.263 A 13-year-old girl with scoliosis has mild intermittent back pain. A bone scan,
2. CT scan, and an MRI scan would most likely reveal which of the following
3. conditions?
4. 1- Spondylolysis
5. 2- Spondylolisthesis
6. 3- Scheuermann's disorder
7. 4- Slipped vertebral apophysis
8. 5- No other condition
1. answer
1. back
1. Question 01.263
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Ramirez N, Johnston CE, Browne RH: The prevalence of back pain in children who have idiopathic scoliosis. J Bone Joint Surg Am 1997;79:364-368.
1. 01.264 What is the most common cause of failure of the pars interarticularis in
2. spondylolysis?
3. 1- Repetitive hyperextension
4. 2- Repetitive axial loading
5. 3- Repetitive torsion
6. 4- Single-load extension
7. 5- Single-load flexion
1. answer
1. back
1. Question 01.264
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Bradford D.S: Spondylolysis and spondylolisthesis in children and adolescents: Current concepts in management, in Bradford DS, Hensinger RM (eds): The Pediatric Spine. New York, NY, Thieme, 1985, pp 403-423. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 1337-1347.
1. 01.265 What is the advantage of impaction allografting during femoral revision hip
2. arthroplasty?
3. 1- Lower cost
4. 2- Lower incidence of femoral component subsidence
5. 3- Lower risk of femoral fracture and perforation
6. 4- Ability to reconstitute bone stock
7. 5- Delivery of depot antibiotics
1. answer
1. back
1. Question 01.265
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Inst Course Lect 2000;49:111-118.
1. 01.266 Which of the following is considered a characteristic of a prosthesis used for a
2. Syme's amputation?
3. 1- No auxiliary suspension mechanisms
4. 2- Posterior window
5. 3- Non-weight-bearing distal portion
6. 4- Patellar tendon bearing
7. 5- Availability of multiple foot prostheses
1. answer
1. back
1. Question 01.266
2. Answer = 1
1. back to this question
1. next question
1. Reference(s)
2. Coughlin MJ, Mann RA: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1003-1004.
1. 01.267 A 62-year-old woman who plays tennis underwent an acromioplasty and
2. rotator cuff repair using four suture anchors 1 month ago. Three days ago, she
3. was allowed to begin using her arm to lift light weights, but she now reports a
4. dramatic increase in pain and is unable to elevate the arm. The next most
5. appropriate step in management should consist of
6. 1- further immobilization and discontinuation of physical therapy.
7. 2- plain radiography.
8. 3- MRI.
9. 4- arthrography.
10. 5- electromyography of the axillary and suprascapular nerves.
1. answer
1. back
1. Question 01.267
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Hanyman DT II: Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA III: Repairs of the rotator cuff: Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am 1991;73:982-989. Barber FA, Herbert MA, Click JN: The ultimate strength of suture anchors. Arthroscopy 1995;11:21-28.
1. 01.268 Which of the following factors will increase the rigidity of an external fixator?
2. 1- Decreased pin diameter
3. 2- Decreased pin number
4. 3- Increased pin spread within a segment
5. 4- Increased bone-to-rod distance
6. 5- Increased distance between fragment pin sets
1. answer
1. back
1. Question 01.268
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Buckwalter JA. Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 372-399.
1. 01.269 The likelihood of a contralateral slip occurring in a boy with a unilateral
2. slipped capital femoral epiphysis is greatest when combined with which of the
3. following risk factors?
4. 1- An unstable slip
5. 2- A chronic slip
6. 3- A grade III slip
7. 4- Patient age of 11 years
8. 5- Patient age of 13 years
1. answer
1. back
1. Question 01.269
2. Answer = 4
1. back to this question
1. next question
1. Reference(s)
2. Stasikelis PJ, Sullivan CM, Phillips WA, Polard JA: Slipped capital femoral epiphysis: Prediction of contralateral involvement. J Bone Joint Surg Am 1996;78:1149-1155. Loder RT, Aronson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147.
1. 01.270 During intramedullary tibial nailing, compartment pressures in the leg are most
2. elevated by the use of
3. 1- reaming.
4. 2- continuous traction.
5. 3- a medial starting point.
6. 4- a lateral starting point.
7. 5- a solid nail.
1. answer
1. back
1. Question 01.270
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Shakespeare DT, Henderson NJ: Compartmental pressure changes during calcaneal traction in tibial fractures. J Bone Joint Surg Br 1982;64:498-499. McQueen MM, Christie J, Court-Brown CM: Compartment pressures after intramedullary nailing of the tibia. J Bone Joint Surg Br 1990;72:395-397.
1. 01.271 Surgical intervention is first indicated for Dupuytren's disease when which of
2. the following findings is present?
3. 1- A metacarpophalangeal joint contracture that is greater than 60° and a proximal
4. interphalangeal joint contracture of any degree
5. 2- A metacarpophalangeal joint contracture and a proximal interphalangeal joint
6. contracture that are each greater than 40°
7. 3- A metacarpophalangeal joint contracture of 30° and a proximal interphalangeal joint
8. contracture of any degree
9. 4- A metacarpophalangeal joint contracture of any degree and a proximal
10. interphalangeal joint contracture that is greater than or equal to 30°
11. 5- Any contracture of either the metacarpophalangeal or proximal interphalangeal joints
1. answer
1. back
1. Question 01.271
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. McFarlane RM, Botz JS: The results of treatment, in McFarlane RM, McGrouther DA, Flint MA (eds): Dupuytren's Disease: Biology and Treatment (The hand and upper limb series, vol 5). Edinburgh, Scotland, 1990, pp 387-412.
1. 01.272 Following a left-sided approach for surgery on the anterior cervical spine, the
2. patient reports a drooping left upper eyelid and dryness on the left side of the
3. face. Which of the following structures has most likely been injured?
4. 1- Recurrent laryngeal nerve
5. 2- Superior laryngeal nerve
6. 3- Hypoglossal nerve
7. 4- Phrenic nerve
8. 5- Sympathetic chain
1. answer
1. back
1. Question 01.272
2. Answer = 5
1. back to this question
1. next question
1. Reference(s)
2. Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 1427-1438. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
1. 01.273 An 18-year-old man with recurrent bilateral ankle instability reports that his
2. symptoms have been slowly progressing. He denies problems with
3. coordination, but he notes easy fatigability when he types. History reveals that
4. his grandmother had "disfigured feet." Examination reveals bilateral cavovarus
5. feet and peroneal weakness. He has intrinsic muscular weakness in his hands.
6. To confirm the diagnosis, which of the following studies should be obtained?
7. 1- Radiographs of the spine
8. 2- Electrocardiography
9. 3- Electromyography
10. 4- MRI of the feet
11. 5- CBC
1. answer
1. back
1. Question 01.273
2. Answer = 3
1. back to this question
1. next question
1. Reference(s)
2. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
1. 01.274 Which of the following is considered the most common complication of an
2. extensive medial release for resistant medial epicondylitis?
3. 1- Ulnar palsy
4. 2- Medial elbow instability
5. 3- Wrist flexion weakness
6. 4- Forearm pronation weakness
7. 5- Elbow flexor weakness
1. answer
1. back
1. Question 01.274
2. Answer = 2
1. back to this question
1. next question
1. Reference(s)
2. Callaway GH, Field LD, Deng ML et al: Biomechanical evaluation of the medial collateral ligament of the elbow. J Bone Joint Surg Am 1997;79:1223-1231. Vangsness CT Jr, Jobe FW: Surgical treatment of medial epicondylitis: Results in 35 elbows. J Bone Joint Surg Br 1991;73:409-411.
1. 01.275 What neurosensory receptor is responsible for detecting the sensation of a
2. vibration?
3. 1- Merkel cells
4. 2- Pacinian corpuscles
5. 3- Ruffini end organs
6. 4- Meissner corpuscles
7. 5- Free-ending nerve fibers
1. answer
1. back
1. Question 01.275
2. Answer = 3
1. back to this question
1. End of 2001 Exam
1. Reference(s)
2. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 325-396.
[**for more mcqs in the bank**](https://hutaifortho.com/942#content)
**[ORTHOPEDIC MCQS ONLINE BANK OITE 20](http://www.hutaifortho.com/1179)**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 97](http://www.hutaifortho.com/1178)**
**[ORTHOPEDIC MCQS BANK OITE 96](http://www.hutaifortho.com/1177)**
**[ORTHOPEDIC MCQS BANK OITE 99](http://www.hutaifortho.com/1176)**
**[ORTHOPEDIC MCQS BANK OITE98](http://www.hutaifortho.com/1175)**
[ORTHOPEDIC MCQS ONLINE OB PATHOLOGY 1A](http://www.hutaifortho.com/1080)
**[ORTHOPEDIC MCQS ONLINE OB HAND 1A](http://www.hutaifortho.com/1078)**
[Links For. ORTHOPEDICS MCQS QUESTION BANK](http://www.hutaifortho.com/942)
**[ortho mcqs](http://www.hutaifortho.com/934)**
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1D](http://www.hutaifortho.com/933)
[ORTHOPEDIC MCQS ADULT RECONSTRUCTIVE OB 20 1C](http://www.hutaifortho.com/932)
[ORTHOPEDIC MCQS ONLINE OB 20 2B RECONSTRUCTION](http://www.hutaifortho.com/929)
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1A](http://www.hutaifortho.com/928)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2D](http://www.hutaifortho.com/927)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B](http://www.hutaifortho.com/925)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 2A](http://www.hutaifortho.com/924)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D](http://www.hutaifortho.com/923)
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1C](http://www.hutaifortho.com/922)**
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1B](http://www.hutaifortho.com/921)**
**[ORTHOPEDIC MCQS 20OB TRAUMA 1A](http://www.hutaifortho.com/920)**
**[ORTHOPEDIC MCQS ONLINE 010 PEDIATRIC](http://www.hutaifortho.com/919)**
**[ORTHOPEDIC MCQS 010 ONLINE](http://www.hutaifortho.com/918)**
[ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery...](http://www.hutaifortho.com/917)
[ORTHOPEDIC MCQS ONLINE 011 RECONSTRUCTION](http://www.hutaifortho.com/916)
**[ORTHOPEDIC MCQS ONLINE 011 PATHOLOGY](http://www.hutaifortho.com/915)**
**[ORTHOPEDIC MCQS 011 ANATOMY IMAGING](http://www.hutaifortho.com/914)**
**[ORTHOPEDIC MCQS O11 UPPER EXTREMITY](http://www.hutaifortho.com/913)**
**[ORTHOPEDIC MCQS ONLINE 012 SPINE](http://www.hutaifortho.com/912)**
**[ORTHOPEDIC MCQS ONLINE 012 TRAUMA](http://www.hutaifortho.com/911)**
[Orthopedic MCQS online 012 FOOT AND ANKLE](http://www.hutaifortho.com/910)
**[ORTHOPEDIC MCQS ONLINE 013 PEDIATRIC](http://www.hutaifortho.com/909)**
**[ORTHOPEDIC MCQS ONLINE 013 SPORT](http://www.hutaifortho.com/908)**
**[ORTHOPEDIC MCQS ONLINE 013 BASIC](http://www.hutaifortho.com/906)**
[ORTHOPEDIC MCQS ONLINE 014 ANATOMY IMAGING](http://www.hutaifortho.com/905)
[ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY](http://www.hutaifortho.com/904)
**[ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY](http://www.hutaifortho.com/903)**
**[ORTHOPEDIC MCQS ONLINE 015 TRAUMA](http://www.hutaifortho.com/902)**
[ORTHOPEDIC MCQS ONLINE 015 FOOT AND ANKLE e](http://www.hutaifortho.com/901)
**[ORTHOPEDIC MCQS ONLINE 015Spine](http://www.hutaifortho.com/900)**
**[ORTHOPEDIC MCQS ONLINE PEDIATRIC 016](http://www.hutaifortho.com/899)**
[ORTHOPEDIC MCQS ONLINE RECONSTRUCTION 016](http://www.hutaifortho.com/898)
**[ORTHOPEDIC MCQS ONLINE SPORT016](http://www.hutaifortho.com/897)**
**[ORTHOPEDIC MCQS ONLINE HAND 017](http://www.hutaifortho.com/896)**
**[ORTHOPEDIC MCQS ONLINE PATHOLOGY 017](http://www.hutaifortho.com/895)**
[Orthopedic MCQS online Shoulder and Elbow 017](http://www.hutaifortho.com/894)
**[Orthopedic MCQS online Anatomy 017](http://www.hutaifortho.com/893)**
**[Orthopedic MCQS online Basic 018](http://www.hutaifortho.com/892)**
**[Orthopedic MCQS online Spine 0018](http://www.hutaifortho.com/891)**
**[Orthopedic MCQS Trauma 0018](http://www.hutaifortho.com/890)**
**[Orthopedic MCQS RECON0019](http://www.hutaifortho.com/889)**
**[Orthopedic Mcqs Sport 0019](http://www.hutaifortho.com/888)**
**[Orthopedics Mcqs Hand0019](http://www.hutaifortho.com/887)**
**[ORTHO MCQS RECON019](http://www.hutaifortho.com/886)**
**[HAND AND WRIST MCQS 019](http://www.hutaifortho.com/885)**
**[ORTHO MCQS Shoulder and Elbow 0192](http://www.hutaifortho.com/884)**
**[ORTHO MCQS Shoulder and Elbow 019](http://www.hutaifortho.com/883)**
**[ORTHO MCQS PEDS 10](http://www.hutaifortho.com/882)**
**[ORTHO MCQS SPORT 10](http://www.hutaifortho.com/881)**
**[ORTHO MCQS BANK 011 FREE 04](http://www.hutaifortho.com/880)**
**[ORTHO MCQS BANK 011 FREE 03](http://www.hutaifortho.com/879)**
**[ORTHO MCQS 011 FREE BANK 02](http://www.hutaifortho.com/878)**
**[ORTHO MCQS 011 FREE BANK](http://www.hutaifortho.com/877)**
[Orthopedic MCQS online Hip and knee ADULT...](http://www.hutaifortho.com/876)
**[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://www.hutaifortho.com/875)**
**[ORTHOPEDIC MCQS OB 20 BASIC5](http://www.hutaifortho.com/874)**
**[ORTHOPEDIC MCQS OB 20 BASIC7](http://www.hutaifortho.com/873)**
**[ORTHOPEDIC MCQS OB 20 BASIC 6](http://www.hutaifortho.com/872)**
**[ORTHOPEDIC MCQS OB 20 BASIC 44](http://www.hutaifortho.com/871)**
**[ORTHOPEDIC MCQS OB 20 BASIC 4](http://www.hutaifortho.com/870)**
**[ORTHOPEDIC MCQS OB 20 BASIC 3](http://www.hutaifortho.com/869)**
**[ORTHOPEDIC MCQS OB 20 BASIC 2](http://www.hutaifortho.com/868)**
**[ORTHOPEDIC MCQS OB 20 BASIC 1](http://www.hutaifortho.com/867)**
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://www.hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://www.hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://www.hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://www.hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://www.hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://www.hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://www.hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02](http://www.hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://www.hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://www.hutaifortho.com/856)
**[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://www.hutaifortho.com/855)**
**[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://www.hutaifortho.com/854)**
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://www.hutaifortho.com/853)
**[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://www.hutaifortho.com/852)**
**[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://www.hutaifortho.com/851)**
**[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://www.hutaifortho.com/850)**
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://www.hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://www.hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://www.hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://www.hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://www.hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://www.hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://www.hutaifortho.com/843)
**[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://www.hutaifortho.com/842)**
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://www.hutaifortho.com/841)
**[ONLINE ORTHOPEDIC MCQS SPORT07](http://www.hutaifortho.com/840)**
**[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://www.hutaifortho.com/839)**
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://www.hutaifortho.com/838)
**[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://www.hutaifortho.com/837)**
**[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://www.hutaifortho.com/836)**
**[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://www.hutaifortho.com/835)**
**[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://www.hutaifortho.com/834)**
[Orthopedic MCQS online sports Medicine](http://www.hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://www.hutaifortho.com/832)
**[Orthopedic MCQS online Hip and knee](http://www.hutaifortho.com/831)**
**[online orthopedic mcqs](http://www.hutaifortho.com/830)**
[Shoulder and elbow: Mcqs AND EMQS Answers](http://www.hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://www.hutaifortho.com/765)
**[Hand and wrist: Answers MCQS EMQS](http://www.hutaifortho.com/764)**
[Hand and wrist: MCQ AND EMQ Questions](http://www.hutaifortho.com/763)
**[2021 SHOULDER AND ELBOW MCQS FREE](http://www.hutaifortho.com/689)**
[Pediatric Orthopaedic MCQS Self-Assessment...](http://www.hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://www.hutaifortho.com/684)
**[Foot and Ankle free MCQS2020 Online](http://www.hutaifortho.com/681)**
**[UPDATED ORTHOPEDIC MCQS](http://www.hutaifortho.com/680)**
[FREE Orthopedics MCQS 2022 1951.-2000.](http://www.hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://www.hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://www.hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://www.hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://www.hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://www.hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://www.hutaifortho.com/668)
**[FREE Orthopedics MCQS 2022 1651-1700](http://www.hutaifortho.com/667)**
[FREE Orthopedics MCQS 2022 1601-1650.](http://www.hutaifortho.com/666)
**[ORTHOPEDIC MCQS FREE 2023](http://www.hutaifortho.com/665)**
**[FREE Orthopedics MCQS 2022 1551-1600](http://www.hutaifortho.com/664)**
**[FREE Orthopedics MCQS 2022 1501-1550](http://www.hutaifortho.com/663)**
**[FREE Orthopedics MCQS 2022 1451-1500](http://www.hutaifortho.com/662)**
**[FREE Orthopedics MCQS 2022 1401-1450](http://www.hutaifortho.com/661)**
[FREE Orthopedics MCQS 2022 1351 -1400](http://www.hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://www.hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://www.hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://www.hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://www.hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://www.hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://www.hutaifortho.com/653)
**[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://www.hutaifortho.com/652)**
**[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://www.hutaifortho.com/651)**
**[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://www.hutaifortho.com/650)**
**[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://www.hutaifortho.com/649)**
**[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://www.hutaifortho.com/647)**
**[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://www.hutaifortho.com/646)**
**[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://www.hutaifortho.com/645)**
**[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://www.hutaifortho.com/644)**
**[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://www.hutaifortho.com/643)**
**[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://www.hutaifortho.com/642)**
**[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://www.hutaifortho.com/641)**
**[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://www.hutaifortho.com/640)**
**[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://www.hutaifortho.com/639)**
**[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://www.hutaifortho.com/638)**
**[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://www.hutaifortho.com/637)**
**[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://www.hutaifortho.com/636)**
**[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://www.hutaifortho.com/635)**
**[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://www.hutaifortho.com/634)**
**[FREE Orthopedics MCQS 2022 51-100](http://www.hutaifortho.com/633)**
**[Orthopedics Hyperguide MCQ 1-50](http://www.hutaifortho.com/631)**
**for more mcqs in the bank**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 20](http://www.hutaifortho.com/1179)**
**[ORTHOPEDIC MCQS ONLINE BANK OITE 97](http://www.hutaifortho.com/1178)**
**[ORTHOPEDIC MCQS BANK OITE 96](http://www.hutaifortho.com/1177)**
**[ORTHOPEDIC MCQS BANK OITE 99](http://www.hutaifortho.com/1176)**
**[ORTHOPEDIC MCQS BANK OITE98](http://www.hutaifortho.com/1175)**
[ORTHOPEDIC MCQS ONLINE OB PATHOLOGY 1A](http://www.hutaifortho.com/1080)
**[ORTHOPEDIC MCQS ONLINE OB HAND 1A](http://www.hutaifortho.com/1078)**
[Links For. ORTHOPEDICS MCQS QUESTION BANK](http://www.hutaifortho.com/942)
**[ortho mcqs](http://www.hutaifortho.com/934)**
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1D](http://www.hutaifortho.com/933)
[ORTHOPEDIC MCQS ADULT RECONSTRUCTIVE OB 20 1C](http://www.hutaifortho.com/932)
[ORTHOPEDIC MCQS ONLINE OB 20 2B RECONSTRUCTION](http://www.hutaifortho.com/929)
[ORTHOPEDIC MCQS ONLINE OB 20 RECONSTRUCTION 1A](http://www.hutaifortho.com/928)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2D](http://www.hutaifortho.com/927)
[ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2B](http://www.hutaifortho.com/925)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 2A](http://www.hutaifortho.com/924)
[ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D](http://www.hutaifortho.com/923)
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1C](http://www.hutaifortho.com/922)**
**[ORTHOPEDIC MCQS 20 OB TRAUMA 1B](http://www.hutaifortho.com/921)**
**[ORTHOPEDIC MCQS 20OB TRAUMA 1A](http://www.hutaifortho.com/920)**
**[ORTHOPEDIC MCQS ONLINE 010 PEDIATRIC](http://www.hutaifortho.com/919)**
**[ORTHOPEDIC MCQS 010 ONLINE](http://www.hutaifortho.com/918)**
[ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery...](http://www.hutaifortho.com/917)
[ORTHOPEDIC MCQS ONLINE 011 RECONSTRUCTION](http://www.hutaifortho.com/916)
**[ORTHOPEDIC MCQS ONLINE 011 PATHOLOGY](http://www.hutaifortho.com/915)**
**[ORTHOPEDIC MCQS 011 ANATOMY IMAGING](http://www.hutaifortho.com/914)**
**[ORTHOPEDIC MCQS O11 UPPER EXTREMITY](http://www.hutaifortho.com/913)**
**[ORTHOPEDIC MCQS ONLINE 012 SPINE](http://www.hutaifortho.com/912)**
**[ORTHOPEDIC MCQS ONLINE 012 TRAUMA](http://www.hutaifortho.com/911)**
[Orthopedic MCQS online 012 FOOT AND ANKLE](http://www.hutaifortho.com/910)
**[ORTHOPEDIC MCQS ONLINE 013 PEDIATRIC](http://www.hutaifortho.com/909)**
**[ORTHOPEDIC MCQS ONLINE 013 SPORT](http://www.hutaifortho.com/908)**
**[ORTHOPEDIC MCQS ONLINE 013 BASIC](http://www.hutaifortho.com/906)**
[ORTHOPEDIC MCQS ONLINE 014 ANATOMY IMAGING](http://www.hutaifortho.com/905)
[ORTHOPEDIC MCQS ONLINE 014 UPPER EXTREMITY](http://www.hutaifortho.com/904)
**[ORTHOPEDIC MCQS ONLINE 014 PATHOLOGY](http://www.hutaifortho.com/903)**
**[ORTHOPEDIC MCQS ONLINE 015 TRAUMA](http://www.hutaifortho.com/902)**
[ORTHOPEDIC MCQS ONLINE 015 FOOT AND ANKLE e](http://www.hutaifortho.com/901)
**[ORTHOPEDIC MCQS ONLINE 015Spine](http://www.hutaifortho.com/900)**
**[ORTHOPEDIC MCQS ONLINE PEDIATRIC 016](http://www.hutaifortho.com/899)**
[ORTHOPEDIC MCQS ONLINE RECONSTRUCTION 016](http://www.hutaifortho.com/898)
**[ORTHOPEDIC MCQS ONLINE SPORT016](http://www.hutaifortho.com/897)**
**[ORTHOPEDIC MCQS ONLINE HAND 017](http://www.hutaifortho.com/896)**
**[ORTHOPEDIC MCQS ONLINE PATHOLOGY 017](http://www.hutaifortho.com/895)**
[Orthopedic MCQS online Shoulder and Elbow 017](http://www.hutaifortho.com/894)
**[Orthopedic MCQS online Anatomy 017](http://www.hutaifortho.com/893)**
**[Orthopedic MCQS online Basic 018](http://www.hutaifortho.com/892)**
**[Orthopedic MCQS online Spine 0018](http://www.hutaifortho.com/891)**
**[Orthopedic MCQS Trauma 0018](http://www.hutaifortho.com/890)**
**[Orthopedic MCQS RECON0019](http://www.hutaifortho.com/889)**
**[Orthopedic Mcqs Sport 0019](http://www.hutaifortho.com/888)**
**[Orthopedics Mcqs Hand0019](http://www.hutaifortho.com/887)**
**[ORTHO MCQS RECON019](http://www.hutaifortho.com/886)**
**[HAND AND WRIST MCQS 019](http://www.hutaifortho.com/885)**
**[ORTHO MCQS Shoulder and Elbow 0192](http://www.hutaifortho.com/884)**
**[ORTHO MCQS Shoulder and Elbow 019](http://www.hutaifortho.com/883)**
**[ORTHO MCQS PEDS 10](http://www.hutaifortho.com/882)**
**[ORTHO MCQS SPORT 10](http://www.hutaifortho.com/881)**
**[ORTHO MCQS BANK 011 FREE 04](http://www.hutaifortho.com/880)**
**[ORTHO MCQS BANK 011 FREE 03](http://www.hutaifortho.com/879)**
**[ORTHO MCQS 011 FREE BANK 02](http://www.hutaifortho.com/878)**
**[ORTHO MCQS 011 FREE BANK](http://www.hutaifortho.com/877)**
[Orthopedic MCQS online Hip and knee ADULT...](http://www.hutaifortho.com/876)
**[ORTHOPEDIC MCQS OB 20 TRAUMA1](http://www.hutaifortho.com/875)**
**[ORTHOPEDIC MCQS OB 20 BASIC5](http://www.hutaifortho.com/874)**
**[ORTHOPEDIC MCQS OB 20 BASIC7](http://www.hutaifortho.com/873)**
**[ORTHOPEDIC MCQS OB 20 BASIC 6](http://www.hutaifortho.com/872)**
**[ORTHOPEDIC MCQS OB 20 BASIC 44](http://www.hutaifortho.com/871)**
**[ORTHOPEDIC MCQS OB 20 BASIC 4](http://www.hutaifortho.com/870)**
**[ORTHOPEDIC MCQS OB 20 BASIC 3](http://www.hutaifortho.com/869)**
**[ORTHOPEDIC MCQS OB 20 BASIC 2](http://www.hutaifortho.com/868)**
**[ORTHOPEDIC MCQS OB 20 BASIC 1](http://www.hutaifortho.com/867)**
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW4](http://www.hutaifortho.com/865)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW3](http://www.hutaifortho.com/864)
[ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW 2](http://www.hutaifortho.com/863)
[1ORTHOPEDIC MCQS OB 20 SHOULDER AND ELBOW](http://www.hutaifortho.com/862)
[ORTHOPEDIC MCQS BANK WITH ANSWER HIP 01](http://www.hutaifortho.com/861)
[ORTHOPEDIC MCQS BANK WITH ANSWER PEDS 01](http://www.hutaifortho.com/860)
[ORTHOPEDIC MCQS BANK WITH ANSWER SPORT 01](http://www.hutaifortho.com/859)
[ORTHOPEDIC MCQS BANK WITH ANSWER ANATOMY 02](http://www.hutaifortho.com/858)
[ORTHOPEDIC MCQS BANK WITH ANSWER PATHOLOGY 02](http://www.hutaifortho.com/857)
[ORTHOPEDIC MCQS BANK WITH ANSWER SHOULDER 02](http://www.hutaifortho.com/856)
**[ORTHOPEDIC MCQS WITH ANSWER FOOT 03](http://www.hutaifortho.com/855)**
**[ORTHOPEDIC MCQS WITH ANSWER SPINE 03](http://www.hutaifortho.com/854)**
[ORTHOPEDIC MCQS WITH ANSWER TRAUMA 03](http://www.hutaifortho.com/853)
**[ORTHOPEDIC MCQS WITH ANSWER HIP 04](http://www.hutaifortho.com/852)**
**[ORTHOPEDIC MCQS WITH ANSWER PEDS 04](http://www.hutaifortho.com/851)**
**[ORTHOPEDIC MCQS WITH ANSWER SPORT 04](http://www.hutaifortho.com/850)**
[ORTHOPEDIC MCQS WITH ANSWER ANATOMY 05](http://www.hutaifortho.com/849)
[ORTHOPEDIC MCQS WITH ANSWER TUMOR/ONCOLOGY 05](http://www.hutaifortho.com/848)
[ORTHOPEDIC MCQS WITH ANSWER UPPER LIMB 05](http://www.hutaifortho.com/847)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE SPINE 06](http://www.hutaifortho.com/846)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE FOOT AND ANKLE...](http://www.hutaifortho.com/845)
[ORTHOPEDIC MCQS WITH ANSWERS ONLINE TRAUMA 06](http://www.hutaifortho.com/844)
[ORTHOPEDIC MCQS with Answers ONLINE BASIC 06](http://www.hutaifortho.com/843)
**[ORTHOPEDIC MCQS ONLINE PEDIATRICS 07](http://www.hutaifortho.com/842)**
[ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07](http://www.hutaifortho.com/841)
**[ONLINE ORTHOPEDIC MCQS SPORT07](http://www.hutaifortho.com/840)**
**[ONLINE ORTHOPEDIC MCQS UPPER LIMB08](http://www.hutaifortho.com/839)**
[ONLINE ORTHOPEDIC MCQS ONCOLOGY/TUMOR08](http://www.hutaifortho.com/838)
**[ONLINE ORTHOPEDIC MCQS ANATOMY08](http://www.hutaifortho.com/837)**
**[ONLINE ORTHOPEDIC MCQS FOOT0 9](http://www.hutaifortho.com/836)**
**[ONLINE ORTHOPEDIC MCQS SPINE0 9](http://www.hutaifortho.com/835)**
**[ONLINE ORTHOPEDIC MCQS TRAUMA 9](http://www.hutaifortho.com/834)**
[Orthopedic MCQS online sports Medicine](http://www.hutaifortho.com/833)
[Orthopedic MCQS online Shoulder and Elbow](http://www.hutaifortho.com/832)
**[Orthopedic MCQS online Hip and knee](http://www.hutaifortho.com/831)**
**[online orthopedic mcqs](http://www.hutaifortho.com/830)**
[Shoulder and elbow: Mcqs AND EMQS Answers](http://www.hutaifortho.com/766)
[Shoulder And Elbow: Questions Mcqs AND EMQS](http://www.hutaifortho.com/765)
**[Hand and wrist: Answers MCQS EMQS](http://www.hutaifortho.com/764)**
[Hand and wrist: MCQ AND EMQ Questions](http://www.hutaifortho.com/763)
**[2021 SHOULDER AND ELBOW MCQS FREE](http://www.hutaifortho.com/689)**
[Pediatric Orthopaedic MCQS Self-Assessment...](http://www.hutaifortho.com/685)
[Self-Assessment Examination 2020 Adult Spine MCQS](http://www.hutaifortho.com/684)
**[Foot and Ankle free MCQS2020 Online](http://www.hutaifortho.com/681)**
**[UPDATED ORTHOPEDIC MCQS](http://www.hutaifortho.com/680)**
[FREE Orthopedics MCQS 2022 1951.-2000.](http://www.hutaifortho.com/677)
[FREE Orthopedics MCQS 2022 1901.-1950.](http://www.hutaifortho.com/676)
[FREE Orthopedics MCQS 2022 1851-1900.](http://www.hutaifortho.com/675)
[FREE Orthopedics MCQS 2022 1751-1850..](http://www.hutaifortho.com/674)
[FREE Orthopedics MCQS 2022 1751-1800..](http://www.hutaifortho.com/673)
[Foot and Ankle FREE ORTHOPEDICS MCQS Question 11](http://www.hutaifortho.com/672)
[FREE Orthopedics MCQS 2022 1701-1750.](http://www.hutaifortho.com/668)
**[FREE Orthopedics MCQS 2022 1651-1700](http://www.hutaifortho.com/667)**
[FREE Orthopedics MCQS 2022 1601-1650.](http://www.hutaifortho.com/666)
**[ORTHOPEDIC MCQS FREE 2023](http://www.hutaifortho.com/665)**
**[FREE Orthopedics MCQS 2022 1551-1600](http://www.hutaifortho.com/664)**
**[FREE Orthopedics MCQS 2022 1501-1550](http://www.hutaifortho.com/663)**
**[FREE Orthopedics MCQS 2022 1451-1500](http://www.hutaifortho.com/662)**
**[FREE Orthopedics MCQS 2022 1401-1450](http://www.hutaifortho.com/661)**
[FREE Orthopedics MCQS 2022 1351 -1400](http://www.hutaifortho.com/660)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1301-1350](http://www.hutaifortho.com/659)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1251-1300](http://www.hutaifortho.com/658)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1151-1200](http://www.hutaifortho.com/656)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ-1101 1150](http://www.hutaifortho.com/655)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1051-1100](http://www.hutaifortho.com/654)
[ORTHOPEDICS HYPERGUIDE 2022 MCQ1001-1051](http://www.hutaifortho.com/653)
**[ORTHOPEDICS HYPERGUIDE MCQ 951-1000](http://www.hutaifortho.com/652)**
**[ORTHOPEDICS HYPERGUIDE MCQ 901-950](http://www.hutaifortho.com/651)**
**[ORTHOPEDICS HYPERGUIDE MCQ 851-900](http://www.hutaifortho.com/650)**
**[ORTHOPEDICS HYPERGUIDE MCQ 800-850](http://www.hutaifortho.com/649)**
**[ORTHOPEDICS HYPERGUIDE MCQ 751-800](http://www.hutaifortho.com/647)**
**[ORTHOPEDICS HYPERGUIDE MCQ 701-750](http://www.hutaifortho.com/646)**
**[ORTHOPEDICS HYPERGUIDE MCQ 651-700](http://www.hutaifortho.com/645)**
**[ORTHOPEDICS HYPERGUIDE MCQ 601-650](http://www.hutaifortho.com/644)**
**[ORTHOPEDICS HYPERGUIDE MCQ 551-600](http://www.hutaifortho.com/643)**
**[ORTHOPEDICS HYPERGUIDE MCQ 501-550](http://www.hutaifortho.com/642)**
**[ORTHOPEDICS HYPERGUIDE MCQ 451-500](http://www.hutaifortho.com/641)**
**[ORTHOPEDICS HYPERGUIDE MCQ 401-450](http://www.hutaifortho.com/640)**
**[ORTHOPEDICS HYPERGUIDE MCQ 351-400](http://www.hutaifortho.com/639)**
**[ORTHOPEDICS HYPERGUIDE MCQ 301-350](http://www.hutaifortho.com/638)**
**[ORTHOPEDICS HYPERGUIDE MCQ 251-300](http://www.hutaifortho.com/637)**
**[ORTHOPEDICS HYPERGUIDE MCQ 201-250](http://www.hutaifortho.com/636)**
**[ORTHOPEDICS HYPERGUIDE MCQ 151-200](http://www.hutaifortho.com/635)**
**[ORTHOPEDICS HYPERGUIDE MCQ 101-150](http://www.hutaifortho.com/634)**
**[FREE Orthopedics MCQS 2022 51-100](http://www.hutaifortho.com/633)**
**[Orthopedics Hyperguide](http://www.hutaifortho.com/631)**
QUESTION 88
A healthy 39-year-old male presents to clinic with posttraumatic elbow stiffness after a minimally displaced radial head fracture. His injury occurred 4 months ago with no improvement in range of motion despite 10 weeks of supervised physiotherapy. Follow-up radiographs reveal normal osseous anatomy. What is the next best step in treatment?

1
Intra-articular and extra-capsular cortisone injection
2
Closed manipulation under anesthesia
3
Aggressive home exercise program
4
Continuous passive motion device
5
Static or dynamic progressive elbow splinting
Supervised exercise therapy with static or dynamic progressive elbow splinting over a 6 month period has shown to have the greatest improvement on DASH scores and functional range of motion (ROM) in patients with post-traumatic elbow stiffness.
The goal of treatment in post-traumatic stiffness is to restore a functional range of elbow motion (30° to 130°). Non-operative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static or dynamic progressive elbow splinting with a turnbuckle has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Gelinas et al. treated 22 patients with an elbow contracture using a static progressive turnbuckle splint for a mean of 4.5 +/- 1.8 months. The mean range of motion improved from 32 - 108, to 26 - 127 degrees (p = 0.0001). Their results suggest that static progressive splinting is an effective modality for postoperative elbow stiffness.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Illustration A shows an image of a static progressive elbow splint.
Incorrect Answers:
Answer 1: Intra-articular and extra-capsular cortisone injection have not shown to improve ROM in this scenario.
Answer 2: Closed manipulation under anesthesia may worsen elbow stiffness and cause intra-articular damage. Manipulation causes significant swelling and inflammation with tearing of soft tissues, causing hemarthrosis and additional fibrosis in the joint.
Answer 3: Aggressive home exercise program are not effective when formal physiotherapy has failed.
Answer 4: Continuous passive motion machines have a limited role in treating established contractures. They do not seem to improve end-range mobility in these patients.
The goal of treatment in post-traumatic stiffness is to restore a functional range of elbow motion (30° to 130°). Non-operative modalities are considered the first-line of treatment. Aggressive physical therapy has traditionally been advocated. However, the use of static or dynamic progressive elbow splinting with a turnbuckle has shown to provide better functional outcomes. Treatment is usually maintained over a period of 6-12 months. Surgery is considered when nonoperative therapy fails.
Gelinas et al. treated 22 patients with an elbow contracture using a static progressive turnbuckle splint for a mean of 4.5 +/- 1.8 months. The mean range of motion improved from 32 - 108, to 26 - 127 degrees (p = 0.0001). Their results suggest that static progressive splinting is an effective modality for postoperative elbow stiffness.
Lindenhovius et al. randomized sixty-six patients with post-traumatic elbow stiffness into static progressive elbow splint therapy or dynamic elbow splinting over a 12 month period. There was no significant difference in outcomes between treatment modalities. ROM increased by 40° vs. 39° at six months, respectively. DASH scores improved from 50 vs 45 at enrollment to 32 vs. 25 at six months, respectively.
Illustration A shows an image of a static progressive elbow splint.
Incorrect Answers:
Answer 1: Intra-articular and extra-capsular cortisone injection have not shown to improve ROM in this scenario.
Answer 2: Closed manipulation under anesthesia may worsen elbow stiffness and cause intra-articular damage. Manipulation causes significant swelling and inflammation with tearing of soft tissues, causing hemarthrosis and additional fibrosis in the joint.
Answer 3: Aggressive home exercise program are not effective when formal physiotherapy has failed.
Answer 4: Continuous passive motion machines have a limited role in treating established contractures. They do not seem to improve end-range mobility in these patients.
QUESTION 89
A 22-year-old male sustains the injury seen in Figures A and B as the result of a motor vehicle collision. He subsequently undergoes the procedure shown in Figures C and D with a 12 millimeter nail. When would full weight-bearing be allowed after surgery?




1
Immediately
2
4-6 weeks
3
8 weeks
4
12 weeks
5
After consolidation is seen
Comminuted femoral shaft fractures treated with statically locked intramedullary nails of appropriate diameter can be treated with immediate weight-bearing, with little risk of nail/screw breakage or deformity. Immediate range of motion and weight-bearing can be extremely beneficial to short-term patient outcomes, especially in polytrauma patients.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
Brumback et al.(1988) reviewed 133 dynamically locked femoral nails and report that 10.5% lost fixation and/or reduction postoperatively. They recommend reviewing high-quality radiographs to determine fracture characteristics, and note that dynamic fixation only be considered for transverse fracture patterns.
Brumback et al.(1988) performed a prospective series of 97 patients with statically locked femoral nails, and they report that 98% of these went on to successful union without additional procedures, and the 2% with nonunions were successfully treated with later conversion to dynamic interlocking. They also found that no implant failure or deformity occurred with early walking or weight-bearing.
Brumback et al.(1999) reviewed the biomechanics of immediate weightbearing after statically locked intramedullary nails are used in a segmental femur model, and they found that it would be safe. They then looked at immediate weight-bearing of these fractures after statically locked nail insertion in a series of 35 patients, and found no loss of reduction or implant failure with immediate weight-bearing.
Figures A and B show a comminuted, segmental femoral shaft fracture, while Figures C and D show the immediate postoperative radiographs of this patient after intramedullary nailing.
Incorrect Answers:
Answers 2-5: Delay in weight-bearing is not required for this injury pattern, if treated with an appropriate diameter statically locked intramedullary nail.
QUESTION 90
of 100
Figure 26 is a radiograph of an 11-year-old boy with insidious-onset anterior knee pain.
Figure 26 is a radiograph of an 11-year-old boy with insidious-onset anterior knee pain.
1
Plain radiographs
2
CT scan
3
MRI
4
Arthrogram
- MRI
QUESTION 91
C orrection of the congenital gibbus in spina bifida must follow which of these surgical principles:
1
Long instrumentation
2
Short instrumentation
3
Avoidance of instrumentation
4
Avoidance of bony resection
5
Anterior approach to deformity
The leverage provided by long instrumentation prevents loss of correction and junctional deformity.
Short instrumentation poses a risk of junctional kyphosis or loss of fixation.
Because of the severe angular deformity, fusion in situ without correction will be followed by increasing deformity. Resection of one to three of the vertebrae on the lower limb of the kyphosis is essential to allow safe correction without excessive tension on vessels and viscera.
The anterior approach to the gibbus is deep and impractical. This approach does not allow mechanically efficient instrumentation.
Short instrumentation poses a risk of junctional kyphosis or loss of fixation.
Because of the severe angular deformity, fusion in situ without correction will be followed by increasing deformity. Resection of one to three of the vertebrae on the lower limb of the kyphosis is essential to allow safe correction without excessive tension on vessels and viscera.
The anterior approach to the gibbus is deep and impractical. This approach does not allow mechanically efficient instrumentation.
QUESTION 92
of 100
Figures 34a through 34c are the radiographs and MR image of a 15-year-old, right-hand-dominant boy who was playing ice hockey and was checked into the boards. He had immediate anterior right shoulder pain and was unable to return to play. He was seen in the emergency department, and radiograph findings reportedly were normal. A sling is placed and he is seen in the office 3 days later. An examination reveals forward flexion of 90 degrees, abduction of 50 degrees, and external rotation of 0 degrees; all are painful. Belly-press test findings also are painful and abnormal. What is the most likely diagnosis?



Figures 34a through 34c are the radiographs and MR image of a 15-year-old, right-hand-dominant boy who was playing ice hockey and was checked into the boards. He had immediate anterior right shoulder pain and was unable to return to play. He was seen in the emergency department, and radiograph findings reportedly were normal. A sling is placed and he is seen in the office 3 days later. An examination reveals forward flexion of 90 degrees, abduction of 50 degrees, and external rotation of 0 degrees; all are painful. Belly-press test findings also are painful and abnormal. What is the most likely diagnosis?
1
Lesser tuberosity fracture
2
Acromioclavicular separation
3
Coracoid fracture
4
Salter 1 fracture of the proximal humerus
Apophyseal injuries of the lesser tuberosity are rare. If missed, these injuries can have devastating implications for return to normal function. The subscapularis tendon inserts on the lesser tuberosity, and injury to this structure is diagnosed with an examination and direct imaging. Delay in diagnosis is not uncommon. There is no evidence of acromioclavicular separation on radiographs. The coracoid and proximal humerus have a normal appearance for a 15-year-old with an unfused apophysis, and there is no irregularity or widening. Loss of motion can occur with any of the responses.
RECOMMENDED READINGS
11. [Sugalski MT, Hyman JE, Ahmad CS. Avulsion fracture of the lesser tuberosity in an adolescent baseball pitcher: a case report. Am J Sports Med. 2004 Apr-May;32(3):793-6. PubMed PMID: 15090399. ](http://www.ncbi.nlm.nih.gov/pubmed/15090399)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15090399)
12. [Harper DK, Craig JG, van Holsbeeck MT. Apophyseal injuries of the lesser tuberosity in adolescents: a series of five cases. Emerg Radiol. 2013 Jan;20(1):33-7. doi: 10.1007/s10140-012-1064-x. Epub 2012 Aug 16. PubMed PMID: 22895662. ](http://www.ncbi.nlm.nih.gov/pubmed/22895662)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22895662)
RESPONSES FOR QUESTIONS 35 THROUGH 38
1. Open reduction and internal fixation (ORIF)
2. Walking boot and weight bearing as tolerated until pain subsides
3. Nonweight-bearing cast for 6 weeks
4. Physical therapy
5. Closed reduction and weight bearing as tolerated
6. Closed reduction and percutaneous fixation
A 23-year-old man sustains an inversion ankle injury. For each figure(s) shown below, select the most appropriate treatment listed above.
RECOMMENDED READINGS
11. [Sugalski MT, Hyman JE, Ahmad CS. Avulsion fracture of the lesser tuberosity in an adolescent baseball pitcher: a case report. Am J Sports Med. 2004 Apr-May;32(3):793-6. PubMed PMID: 15090399. ](http://www.ncbi.nlm.nih.gov/pubmed/15090399)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15090399)
12. [Harper DK, Craig JG, van Holsbeeck MT. Apophyseal injuries of the lesser tuberosity in adolescents: a series of five cases. Emerg Radiol. 2013 Jan;20(1):33-7. doi: 10.1007/s10140-012-1064-x. Epub 2012 Aug 16. PubMed PMID: 22895662. ](http://www.ncbi.nlm.nih.gov/pubmed/22895662)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22895662)
RESPONSES FOR QUESTIONS 35 THROUGH 38
1. Open reduction and internal fixation (ORIF)
2. Walking boot and weight bearing as tolerated until pain subsides
3. Nonweight-bearing cast for 6 weeks
4. Physical therapy
5. Closed reduction and weight bearing as tolerated
6. Closed reduction and percutaneous fixation
A 23-year-old man sustains an inversion ankle injury. For each figure(s) shown below, select the most appropriate treatment listed above.
QUESTION 93
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
1
Abductor pollicis brevis and extensor pollicis brevis
2
Abductor pollicis brevis and extensor pollicis longus
3
Abductor pollicis longus and extensor pollicis brevis
4
Abductor pollicis longus and extensor pollicis longus
5
Adductor pollicis and extensor pollicis longus
DISCUSSION: Intersection syndrome is also known as “squeakers wrist,” “oarsmen wrist,” and crossover tendinitis. It occurs where the first and second dorsal wrist compartment structures pass over one another, resulting in fibrosis, muscular changes, and inflammation of the bursa in this area. The structures involved are the abductor pollicis longus and extensor pollicis brevis (first dorsal compartment) that pass across the second compartment structures (extensor carpi radialis brevis and extensor carpi radialis longus). An audible “squeak” is occasiona**l** y heard at the intersection point, which is approximately 4 to 5 cm proximal to the proximal dorsal wrist crease.
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
QUESTION 94
of 100 When performing a shoulder hemiarthroplasty for an unreconstructable proximal humerus fracture, the relationship of the repaired greater tuberosity to the prosthetic humeral head should be
1
6 mm to 8 mm superior to the top of the humeral head.
2
6 mm to 8 mm inferior to the top of the humeral head.
3
1.5 cm inferior to the top of the humeral head.
4
at the same height as the top of the humeral head.
DISCUSSION
The greater tuberosity lies anatomically 6 mm to 8 mm inferior to the top of the humeral head. Normal proximal humeral anatomy must be recreated when performing a hemiarthroplasty for fracture so as to minimize the complications associated with the greater tuberosity and maximize functional outcomes. Tuberosity malunion and nonunion are considered the most common reasons for poor clinical outcomes following this procedure. Placing the tuberosity too proximal can lead to issues with impingement during shoulder abduction, and placement too distal can increase the tension on the rotator cuff as it courses over the
prosthetic humeral head.
QUESTION 95
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
1
Quadrigia
2
Intrinsic tightness
3
Lumbrical plus deformity
4
Disruption of the tendon repair
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit. Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon
repair causes limited flexion of the injured finger.
repair causes limited flexion of the injured finger.
QUESTION 96
of 100
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
1
Primary lumbar disk herniation
2
Adolescent idiopathic scoliosis
3
Cervical spondylotic myelopathy
4
No conditions; there are no official guidelines
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
[Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. ](http://www.ncbi.nlm.nih.gov/pubmed/23116090)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23116090) [Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[View ](http://www.ncbi.nlm.nih.gov/pubmed/20858377)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20858377)
[Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[View](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[ ](http://www.ncbi.nlm.nih.gov/pubmed/24688334)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24688334)
QUESTION 97
Figure 64 shows the radiograph of a 61-year-old man with ankylosing spondylitis. He is scheduled to undergo left total hip arthroplasty. Which of the following perioperative interventions should be considered?
1
Intraoperative sciatic nerve monitoring
2
Preoperative radiation therapy with 700 centigray
3
Postoperative radiation therapy with 1,500 centigray
4
Postoperative continuous passive motion
5
Soft cervical collar during postoperative physical therapy
Patients with ankylosing spondylitis are at high risk for heterotopic ossification after total hip arthroplasty, and perioperative prophylaxis with nonsteroidal anti-inflammatory drugs or radiation therapy has been effective at reducing the risk. Radiation prophylaxis given within 24 hours preoperatively has been shown to be as effective as radiation given postoperatively. Doses of 700 to 800 centigray have been shown to be as effective as higher doses with less potential risk. Continuous passive motion has not been shown to improve the postoperative flexibility of these patients. Although these patients may have stiff spines and may be at risk for neurologic injury in the event of spinal fracture, a soft cervical collar is not expected to alter the risk should a catastrophic spinal injury occur. Since there has been no shortening of the limb, the sciatic nerve should not be at significantly higher risk for neurapraxia than with a more routine hip arthroplasty.
REFERENCES: Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;8:870-881.
Pellegrini VD Jr, Konski AA, Gastel JA, et al: Prevention of heterotopic ossification with irradiation after total
hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
REFERENCES: Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;8:870-881.
Pellegrini VD Jr, Konski AA, Gastel JA, et al: Prevention of heterotopic ossification with irradiation after total
hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
QUESTION 98
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
1
Enhanced neurogenic adaptations
2
Advanced myogenic adaptations
3
Increased contractile proteins
4
Increased short-term energy sources
5
Thickening of the connective tissue
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate.
REFERENCES: Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Micheli LJ: Strength training, in Sullivan JA, Grana WA (eds): The Pediatric Athlete. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 17-20.
REFERENCES: Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Micheli LJ: Strength training, in Sullivan JA, Grana WA (eds): The Pediatric Athlete. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 17-20.
QUESTION 99
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
1
Acute aortic dissection
2
Pulmonary contusion
3
Commotio cordis
4
Acute cardiac tamponade
5
Splenic rupture
Sudden cardiac arrest following a blow to the chest in young athletes has been termed “commotio cordis.” It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate.
REFERENCES: Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Link MS, Maron BJ, Estes NAM III: Commotio cordis, in Estes NAM III, Salem DN, Wang PJ (eds): Sudden Cardiac Death in the Athlete. Armonk, NY, Futura, 1998, pp 515-528.
REFERENCES: Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Link MS, Maron BJ, Estes NAM III: Commotio cordis, in Estes NAM III, Salem DN, Wang PJ (eds): Sudden Cardiac Death in the Athlete. Armonk, NY, Futura, 1998, pp 515-528.
QUESTION 100
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
1
steroid injection
2
stretching of the heel cord
3
surgical release of the plantar fascia
4
application of a short leg cast for 6 to 8 weeks
5
wearing dorsiflexion night splints
This question refers to plantar fascitis. Heel spurs are noted in approximately 50% of the cases of subcalcaneal pain syndrome. In this patient, diagnosis should rule out lumbar radiculopathy since the symptoms are bilateral.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
