1
Middle glenohumeral ligament
5
Bankart tear
It is important to recognize that rotator cuff tears are a common finding in the setting of a dislocated long head of the biceps tendon (LHB) from the intertubercular groove of the shoulder. If a LHB tendon dislocation is found on examination or radiographic work-up (ultrasound or MRI), it is imperative to rule out associated rotator cuff pathology, specifically of the subscapularis tendon. Although very rare, injury to the lesser tuberosity should also be ruled out. There are a variety of methods to treat the dislocated biceps (tenotomy versus tenodesis); however, the entire rotator cuff, especially the subscapularis, should be carefully inspected and treated if necessary. The corollary is also true - if you find a tear of the subscapularis tendon insertion, especially the superior half, the LHB should be carefully inspected to ensure that it is not unstable as it exits the shoulder. If the LHB is unstable, this is also addressed surgically with either tenotomy or tenodesis. The middle glenohumeral ligament and Bankart tears are not stabilizers of the biceps.
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Tung GA, Yoo DC, Levine SM, et al: Subscapularis tendon tear: Primary and associated signs on MRI. J Comput Assist Tomogr 2001;25:417-424.
46 • American Academy of Orthopaedic Surgeons
Figure 57
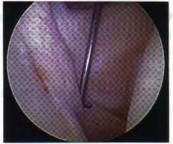
A 57-year-old man who plays recreational sports reports pain in his dominant shoulder. An MR arthrogram is shown in Figure 57. During arthroscopy of the shoulder, what pathology is most likely to be found?
The supplement is creatine. Approximately 17% of high school athletes and about 30% of high school football players use creatine. Creatine is a protein synthesized in the liver and the kidney, circulates in the bloodstream, and is incorporated into muscle. Its use is associated with increased muscle mass, short-term improvement in sprinting, and may allow for increased anaerobic resistance performance. Caffeine and ephedrine are taken orally but do not increase muscle mass. Testosterone and human growth hormone are both associated with increased body mass but must be injected.
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
An 11-year-old boy who is a Little League pitcher has a 3-month history of right elbow pain, made worse after several innings of pitching. The pain is in the posterior and medial aspect of the elbow joint but is without clicking or mechanical symptoms. There are no signs of infection or swelling, and range of motion is full.
There is tenderness over the medial aspect of the elbow distal to the humeral epicondyle over the proximal olecranon. Valgus stress testing of the elbow is normal. What is the most likely diagnosis?
1) Olecranon bursitis
2) Osteochondritis dissecans of the capitellum
3) Ulnar collateral ligament insufficiency
4) Medial epicondylitis
5) Olecranon stress fracture
The patient has an olecranon stress fracture due to overuse injury from pitching. The repetitive forceful contraction of the triceps coupled with varus and valgus torques about the elbow are felt to cause the olecranon epiphysis to separate from the adjacent epiphyseal plate as reported by Torg and Moyer. This may persist into late adolescence; Charlton and Chandler described five throwing athletes between the ages of 16 to 20 years with delayed closure of the olecranon epiphysis and inability to throw. The ulnar collateral ligament was intact in all. The patients in their study underwent open reduction and internal fixation with tension band wire, screw fixation, and autogenous bone graft in some of the cases.
At 32 months, all were asymptomatic despite a prolonged preoperative course (> 30 months) of limiting pain. It is important to recognize stress fractures about the elbow in a young pitching population and treat accordingly first with rest and cessation of throwing activities. If prolonged, surgical fixation provides reliable results.
REFERENCES: Charlton WP, Chandler RW: Persistence of the olecranon physis in baseball players: Results following operative management. J Shoulder Elbow Surg 2003;12:59-62.
Torg JS, Moyer RA: Non-union of a stress fracture through the olecranon epiphyseal plate observed in an
adolescent baseball pitcher. J Bone Joint Surg Am 1977;59:264-265.
Rettig AC, Wurth TR, Mieling P: Nonunion of olecranon stress fractures in adolescent baseball pitchers: A case series of 5 athletes. Am J Sports Med 2006;34:653-656.
What is the most common physical finding in a patient with femoroacetabular impingement (FAI)?
1) Increased external rotation
2) Increased abduction
3) Decreased external rotation
4) Decreased flexion and internal rotation
5) Decreased adduction
reproduction of symptoms. Occasionally, a posterior impingement test will be positive with extension and external rotation. There are a variety of causes of FAI; however, the pathology limits motion as the femur (cam) and acetabulum (pincer) contact one another. Also, only one location needs to be present, such as cam-type or pincer-type versus both cam-pincer lesions to cause symptoms.
REFERENCES: Philippon MJ, Stubbs AJ, Schenker ML, et al: Arthroscopic management of femoroacetabular impingement: Osteoplasty technique and literature review. Am J Sports Med 2007;35:1571 -1580, Siebenrock KA, Schoeniger R, Ganz R: Anterior femoroacetabular impingement due to acetabular retroversion: Treatment with periacetabular osteotomy. J Bone Joint Surg Am 2003;85:278 -286. Kubiak-Langer M, Tannast M, Murphy SB, et al: Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res 2007;458:117-124.
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
1) Tuberculosis
2) Hepatitis B
3) HIV
4) West Nile virus
5) Clostridium
The only reported cases of HIV transmission with tissue transplantation occurred more than 20 years ago. The only reported cases of tuberculosis and hepatitis B occurred more than 50 years ago. The donor-associated clostridium infection occurred in 2001. The facility was not AATB-accredited (American Association of Tissue Banks) and the local A ATB facility refused the graft. It is necessary for the surgeon using the allograft tissue to be aware of the current status of tissue regulation, and procurement and processing procedures.
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006.
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?