Orthopedic Adult Reconstructiv Review | Dr Hutaif Hip & -...
Updated: Feb 2026
40 Views
Key Medical Takeaway
Discover the latest medical recommendations for ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery of the Hip and Knee Examination 7. Eds orthopaedic knowledge specifies that a quadriceps snip, a technique used to improve exposure during revision total knee arthroplasty, does not require alteration of the patient’s postoperative physical therapy regimen. This critical understanding ensures consistent rehabilitation protocols and optimal recovery following complex knee reconstructive surgery.
Score: 0%
ORTHOPEDIC MCQS 010 Adult Reconstructive Surgery of the Hip and Knee Examination 7
QUESTION 1
During the course of a revision total knee arthroplasty via a medial parapatellar exposure, the surgeon does a complete intra-articular release and synovectomy but exposure is still inadequate. A quadriceps snip is performed and, at the end of the procedure, the knee is stable throughout a range of motion and the postoperative radiographs show acceptable alignment of the components. The patient’s postoperative physical therapy regimen should include which of the following?
1
No restriction in range of motion or weight bearing after surgery.
2
Limit flexion to 30 degrees postoperatively, progressing 10 degrees per week
3
Limit flexion to 90 degrees for the first 6 weeks postoperatively
4
Limit to active flexion only with no passive flexion or active extension for 6 weeks
5
Use of a hinged knee brace for 6 weeks postoperatively
A quadriceps snip is performed by extending a medial parapatellar approach superiorly and laterally across the quadriceps tendon. It is then repaired primarily at the end of the procedure. The primary advantage of this technique over other surgical maneuvers that improve exposure at the time of revision total knee arthroplasty is that the postoperative regimen for physical therapy does not need to be altered.
Scientific References
: Younger AS, Duncan CP, Masri BA: Surgical exposures in revision total knee arthroplasty. J Am Acad Orthop Surg 1998;6:55-64.
Della Valle CJ, Berger RA, Rosenberg AG: Surgical exposures in revision total knee arthroplasty. Clin Orthop Relat Res 2006;446:59-68.
Barrack RL, Smith P, Munn B, et al: The Ranawat Award. Comparison of surgical approaches in total knee
arthroplasty. Clin Orthop Relat Res 1998;356:16-21.
QUESTION 2
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
1
initiation of a first-generation cephalosporin while awaiting culture results.
2
initiation of broad-spectrum antibiotics while awaiting culture results.
3
ultrasound to evaluate for fluid collection around the knee.
4
surgical debridement of the knee before culture results are available.
5
inpatient observation and no antibiotics until culture results are available.
Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
Figure 3a Figure 3b
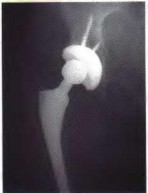
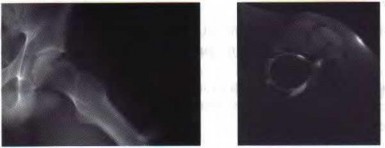
QUESTION 3
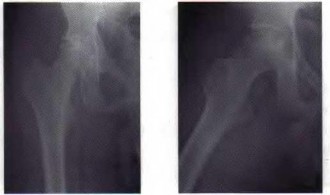
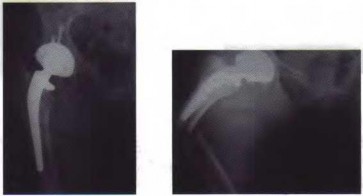
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
1
Use of an abduction orthosis for 6 weeks
2
Modular exchange of the femoral head to a 36-mm head and a longer neck
3
Modular exchange of the polyethylene liner to a constrained acetabular insert
4
Revision and repositioning of the acetabular component and use of a 36-mm femoral head
5
A physical therapy program stressing abductor strengthening
The radiograph shows well-fixed components without evidence of loosening. The CT scan shows severe retroversion of the acetabular component. Revision of the component into the correct amount of anteversion
will most reliably rectify the instability in the face of severe component malposition.
_AL-Madena Copy_
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
QUESTION 4
A patient with a history of rheumatoid arthritis reports a painful total hip arthroplasty 3 years after the index procedure. Radiographs reveal loosening of the femoral component. Preoperative blood work shows an erythrocyte sedimentation rate (ESR) of 38 mm/h (normal 0-29 mm/h) and a C-reactive protein (CRP) of 8.9 (0.2-8.0). What is the most appropriate action at this time?
1
Technetium bone scan
2
Hip aspiration for culture
3
FDG-PET scan
4
Surgery with no further investigations
5
Revision surgery and obtain an intraoperative frozen section
The question centers on the appropriate work-up for a failed total hip arthroplasty prior to revision surgery. The preoperative ESR is elevated and the CRP is at the upper end of normal. If either the ESR or CRP is elevated, further investigations are required to exclude infection as a cause of loosening, particularly in a patient only 3 years after the index procedure. A technetium scan alone is nonspecific and will show increased uptake because of the loose femoral component. An intraoperative frozen section is a helpful confirmatory investigation, but whenever possible the diagnosis should be made preoperatively to allow for appropriate surgical planning. Recently, investigators have shown the value of FDG-PET scanning as a useful investigation for diagnosing infection; however, it is no more accurate than the combined use of an ESR and CRP, and does not allow for identification of an infecting organism. At this point, a hip aspiration for culture is the most appropriate investigation.
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
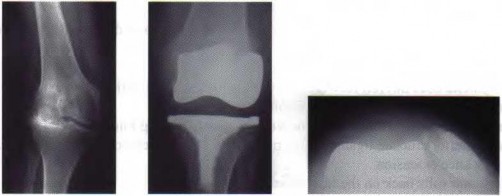
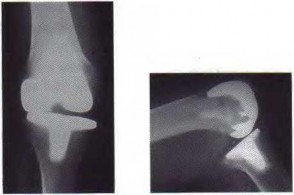
Figure 5a Figure 5b
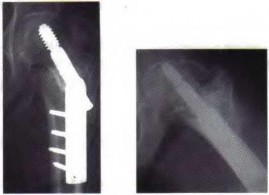
QUESTION 5
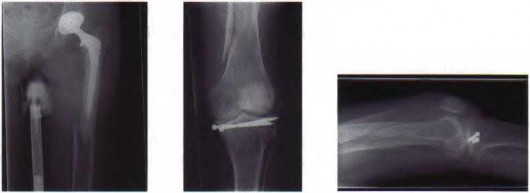
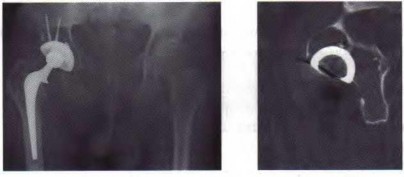
A 7 5-year-old man who sustained an intertrochanteric hip fracture underwent open reduction and internal fixation with a sliding hip screw. Six months after the procedure, the patient has shortening and external rotation of the extremity and progressively severe groin pain with ambulation. Radiographs are shown in Figures 5a and 5b. What is the most appropriate management?
1
Valgus/flexion osteotomy of the proximal femur with repeat open reduction and internal fixation
2
Conversion to bipolar hemiarthroplasty with a cementless femoral component
3
Conversion to total hip arthroplasty with a calcar replacement femoral component that bypasses the hardware
4
External bone stimulator
5
Removal of hardware, followed by physical therapy and use of a shoe lift
The patient has an intertrochanteric fracture malunion with protrusion of the hardware and penetration into the acetabulum. To restore leg length and relieve pain, total hip arthroplasty is necessary. Valgus osteotomy is appropriate for fracture nonunion with an intact femoral head with no signs of osteonecrosis. Bipolar hemiarthroplasty with acetabular erosion will most likely lead to pain as will removal of the hardware with or without physical therapy.
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Figure 6
QUESTION 6
Figure 6 shows the radiograph of a 72-year-old woman who underwent a primary total hip arthroplasty
17 years ago. She now reports groin pain. Optimal surgical management should consist of which of the following?
1
Synovectomy and polyethylene liner exchange
2
Synovectomy, polyethylene liner exchange, and femoral stem revision
3
Synovectomy and complete acetabular revision
4
Synovectomy, bone grafting of lytic lesions, and retention of the components and polyethylene liner
5
Revision of all components with synovectomy
Polyethylene wear is evident due to the superiorly eccentric position of the femoral head within the acetabulum. Despite proximal femoral osteolysis, the component appears well fixed, as does the acetabulum. The acetabular component appears to be well positioned. Therefore, an isolated synovectomy and polyethylene liner exchange is indicated. If the hip is stable, there is no need for more extensive revision work.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
QUESTION 7
Which of the following statements best describes how unicompartmental knee arthroplasty (UKA) differs from total knee arthroplasty (TKA)?
1
TKA has a higher reoperation rate than UKA during the first 10 postoperative years.
2
TKA provides for more normal rotational kinematics than UKA.
3
UKA more closely replicates normal knee kinematics than TKA.
4
Mobile bearings have been successful in UKA but not TKA.
5
Mobile bearings have been successful in TKA but not UKA.
Because UKA does not require cruciate sacrifice, patellofemoral resurfacing, or rotational changes to the femur or tibia, it reliably recreates normal knee kinematics. UKAs have generally demonstrated higher reoperation rates than TKAs at intermediate and long-term follow-up, due in part to progression of arthritis in the nonresurfaced compartments. Mobile bearings have been clinically successful in both UKA and TKA.
REFERENCES: Patil S, Colwell CW Jr, Ezzet KA, et al: Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 2005;87:332-338.
Gioe TJ, Killeen KK, Hoeffel DP, et al: Analysis of unicompartmental knee arthroplasty in a community- based implant registry. Clin Orthop Relat Res 2003;416:111-119.
QUESTION 8
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
1
Increased risk of total hip dislocation
2
Decreased range of motion
3
Fewer options for femoral head bearing material
4
Acceptable wear with modern bearing surfaces
5
Increased component impingement
Larger diameter femoral heads reduce the risk of hip dislocation by allowing greater range of motion before component impingement becomes a risk, and no reports have shown an increase in bearing wear. With modem bearings, volumetric wear should remain low, despite the increase in head diameter. Large femoral heads are available in all common bearing materials
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22-mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Figure 9
QUESTION 9
A 68-year-old man underwent a primary total hip arthroplasty 2 years ago for a femoral neck fracture. His early postoperative course was unremarkable, but he notes some aching in the thigh since surgery. His symptoms have gotten worse over the last year, such that he now has activity-related thigh pain that limits his walking ability. An AP hip radiograph is shown in Figure 9. What is the most appropriate surgical management?
1
No surgery is indicated
2
Revision of the acetabular component
3
Revision of the femoral component
4
Psoas tendon tenotomy
5
Strut grafting of the femur to stiffen the bone near the tip of the implant
The radiograph shows a loose femoral component with failure of osseous integration.
There is a reactive radiolucent line around the fiber mesh portion of the implant, hypertrophy of the bone under the collar, and a pedestal formation at the distal tip of the implant, all of which indicate failure of bone ingrowth. If
bone ingrowth had occurred, there would be stress shielding of bone under the collar.
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res 1990;257:107-128.
Lieberman JR, Huo MH, Schneider R, et al: Evaluation of painful hip arthroplasties: Are technetium bone scans necessary? J Bone Joint Surg Br 1993;75:475-478.
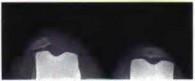
Figure 10 shows patellar radiographs of a 68-year-old woman who underwent bilateral total knee arthroplasty 2 months ago. Following a recent fall onto the left side, she now reports anterior pain in the left knee. A CT scan shows that the femoral and tibial components are appropriately externally rotated and radiographs show acceptable axial alignment and no evidence of loosening. What is the most appropriate treatment option?
1
Fracture fixation and bracing
2
Lateral retinacular release with proximal realignment
3
Tibial component revision
4
Distal realignment by medialization of the tibial tubercle
5
Revision of the patellar component
Treatment of patellofemoral instability after total knee arthroplasty (TKA) is directed by its etiology. In instances of component malpositioning, revision of one or both components is indicated.
If the components are determined to be in satisfactory position, soft-tissue procedures can be pursued. Lateral retinacular release is usually the first soft-tissue procedure used to improve patellofemoral mechanics. In this patient, the patellar fracture fragment is so small that it can be excised. Distal realignment is not usually used as the first line of treatment for patellar maltracking following TKA.
REFERENCES: Fehring TK, Christie MJ, Lavemia C, et al: Revision total knee arthroplasty: Planning, management, and controversies. Instr Course Lect 2008;57:341-363.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
QUESTION 11
Which of the following best describes the legal definition of standard of care?
1
Conforming to a majority norm
2
Providing the most minimally acceptable care
3
Providing average care
4
Providing the care you would expect for yourself or a loved one
5
Reasonable treatment that exhibits knowledge, skill, diligence, and care
The standard of care is a legal concept that is elusive and amorphous, although the term is used widely by physicians to mean different things. Different state courts across the United States have also applied different meanings to the term “standard of care.” Most commonly, the standard of care is that which a reasonable physician would have done under similar circumstances. Expert testimony from other physicians is often required to educate a jury in a medical malpractice trial about the applicable standard of care. As a general rule, treatment that exhibits knowledge, skill, diligence, and care on the part of the physician is likely to fall within the standard of care, regardless of variations in the definition of this term.
REFERENCES: Lewis MH, Gohagan JK, Merenstein DJ: The locality rule and the physician’s dilemma: Local medical practices vs the national standard of care. JAMA 2007;297:2633-2637.
AAOS Expert Witness Program, www3.aaos.org/member/expwit/expertwitaess.cfm
QUESTION 12
Which of the following statements most accurately describes the risk of ileus following total joint arthroplasty?
1
Older age decreases risk.
2
Male gender decreases risk.
3
The risk is roughly 1% in total joint arthroplasty patients.
4
The risk more commonly occurs in total knee arthroplasty (TKA) patients than in total hip arthroplasty (THA) patients.
5
A history of abdominal surgery has no effect on risk.
The risk of postoperative ileus is noted to be higher in patients undergoing THA than patients undergoing TKA. Older age, male gender, and a history of abdominal surgery have been identified as risk factors.
REFERENCE: Parvizi J, Han SB, Tarity TD, et al: Postoperative ileus after total joint arthroplasty. J Arthroplasty 2008;23:360-365.
QUESTION 13
During surgical hip dislocation for the management of femoral acetabular impingement, preservation of what structure is paramount to maintaining vascularity to the femoral head?
1
Metaphyseal vessels
2
Medial epiphyseal artery
3
Superficial branch of the medial femoral circumflex artery
4
Deep branch of the lateral femoral circumflex artery
5
Deep branch of the medial femoral circumflex artery
When a trochanteric osteotomy is performed with the desire to maintain vascularity to the femoral head, as in the approach for a surgical hip dislocation, the deep branch of the medial femoral circumflex artery must be maintained. This branch courses along the posterior aspect of the greater trochanter, posterior to the tendon of obturator extemus, and anterior to the tendons of superior gemellus, obturator intemus, and inferior gemellus. It perforates the capsule above the superior gemellus and distal to the tendon or piriformis, before dividing into two to four terminal retinacular branches. Maintaining the attachment of the external rotators maintains the blood supply to the femoral head. Additionally, the superior-lateral retinacular vessels must also be maintained during femoral neck osteoplasty.
REFERENCES: Gautier E, Ganz K, Krugel N, et al: Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br 2000;82:679-683.
Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip: A technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001; 83:11191124.
Figure 14
QUESTION 14
A 68-year-old woman who underwent left total hip arthroplasty 14 years ago now reports pain in her thigh. A radiograph is shown in Figure 14. What is the most reliable method for reconstructing the femoral component?
1
Revision to a standard length cemented femoral component using third generation cementing techniques
2
Revision to a proximal femoral replacement device (“tumor prosthesis”)
3
Revision to a proximally porous-coated, metaphyseal loading cementless femoral component
4
Revision to a diaphyseal engaging, extensively coated cementless femoral component
5
Revision to an allograft-prosthetic composite
The patient has a loose, cemented femoral component. The proximal femur is deficient and may not have adequate strength to support a proximally porous-coated cementless implant. Cemented hip implants have shown higher rates of failure when used for revision surgery. An extensively coated, cementless stem that engages the diaphysis has been shown to have excellent long-term durability in patients such as this, where the diaphysis is preserved and more than 4 cm of intact diaphysis is available for fixation. Allograft-prosthetic composites and tumor replacement prostheses are used for patients with more severe bone loss of the proximal femur and would not be indicated for this patient.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and
Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Paprosky WG: The femur in revision total hip arthroplasty: Evaluation and classification. Clin Orthop Relat Res 2004;420:55-62.
Engh CA Jr, Ellis TJ, Koralewicz LM, et al: Extensively porous-coated femoral revision for severe femoral bone loss: Minimum 10-year follow-up. J Arthroplasty 2002;8:955-960.
Figure 15
QUESTION 15
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
1
Immediate admission to the hospital and emergent revision hip arthroplasty
2
Reassurance and follow-up if symptoms worsen
3
Repeat radiographs in 1 month
4
Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
5
A prescription for alendronate and reevaluation in 1 year
The radiograph shows significant osteolysis with loosening of the femoral component. The patient is symptomatic and surgery is indicated because of the extent of osteolysis and the loose femoral component.
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
QUESTION 16
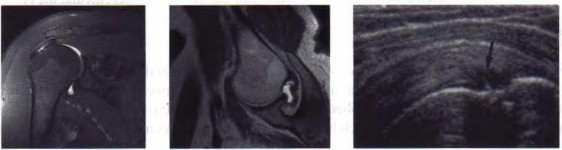
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?
1
Arthroscopic labral debridement
2
Reverse periacetabular osteotomy
3
Resurfacing hip arthroplasty
4
Femoral neck osteochondroplasty and resection of the detached labrum
5
Femoral neck osteochondroplasty and reattachment of the labrum
The patient has cam-type femoral acetabular impingement. He still has a well-maintained joint space without significant degenerative changes, and given his age a joint preserving procedure would be the procedure of choice. A reverse periacetabular osteotomy may be considered in a retroverted acetabulum; however, that is not the case here. A femoral neck osteochondroplasty is required to remove the cam of bone and reshape the femoral head-neck junction to improve the femoral head/neck ratio (femoral head offset). Typically, in isolated cam impingement, cartilage damage in the anterior-superior acetabulum precedes labral damage. Labral debridement alone does not address the pathology of impingement. In cases where labral detachment is present, reattachment has been shown to be superior to labral resection.
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Figure 17a Figure 17b Figure 17c
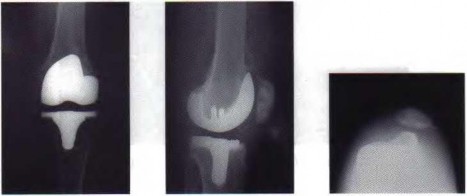
QUESTION 17
A 51-year-old woman who underwent a total knee arthroplasty 14 months ago for severe degenerative arthritis now reports progressive pain, swelling, and buckling of the knee. She must use crutches and is unable to negotiate stairs. Laboratory testing reveals a normal erythrocyte sedimentation rate and C-reactive protein. Radiographs of the patient are shown in Figures 17a through 17c. What is the most important test to further evaluate this problem?
1
Long standing anterior-posterior radiograph of the hip-knee-ankle
2
Axial CT views from the supracondylar distal femur to the proximal tibia below the tibial tubercle
3
Fluoroscopic stress views to demonstrate the position of subluxation
4
Bone scan
5
MRI scan
The cause of subluxation in this patient is multifactorial, and includes a laterally positioned patellar component, a tibial tray that is internally rotated and translated to the medial side of the proximal tibial surface, and a femoral component that is markedly internally rotated about 10 degrees. All of these findings will be apparent on a CT scan. The long standing radiograph may be helpful but does not show the particular rotational abnormalities of both implants that are causing this problem. Fluoroscopic review may show how unstable the patella is, but the initial Merchant’s view shows the basic problem. A bone scan does not provide information about component malposition. An MRI scan is inferior to a CT scan because of image artifact.
REFERENCES: Stiehl JB: Patellar instability in total knee arthroplasty. J Knee Surg 2003;16:229-235. Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
QUESTION 18
Changes to the properties of ultra-high molecular weight polyethylene with increasing irradiation dose include improved
1
resistance to oxidation.
2
ultimate tensile strength.
3
resistance to crack propagation.
4
fracture toughness.
5
volumetric wear.
Increased irradiation doses cause a decrease in the mechanical properties of the polyethylene, resulting in a decrease in ultimate tensile strength, fracture toughness, and resistance to crack propagation.
Irradiation leads to the production of free radicals, requiring a step in the manufacturing process (melting, annealing, vitamin E doping) to stabilize the free radicals and reduce the potential for oxidation. Wear resistance is improved with irradiation; however, there is minimal benefit with doses of greater than 10 Mrads.
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop Relat Res 2003;414:289-304.
Gordan AC, D’Lima DD, Colwell CW Jr: Highly cross-linked polyethylene in total hip arthroplasty. J Am Acad
Orthop Surg 2006;14:511-523.
Jacobs CA, Christian CP, Greenwald AS, et al: Clinical performance of highly cross-linked polyethylenes in total hip arthroplasty. J Bone Joint Surg Am 2007;89:2779-2786.
QUESTION 19
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
1
Ceramic-on-ceramic
2
Large diameter metal head on highly cross-linked polyethylene liner
3
Ceramic head on metal liner
4
Large diameter metal-on-metal total hip arthroplasty
5
Metal on conventional polyethylene liner (noncross-linked)
The most appropriate bearing of those listed would be a large diameter metal head on cross-linked polyethylene. Because of the renal insufficiency, metal-on-metal should be avoided because metal ions are renally excreted. Ceramic-on-ceramic implants are not necessary in this patient because of the patient’s limited activity and life expectancy, as well as the downside of increased cost, the small but definite risk of ceramic fracture, and the increased technical demands of inserting ceramic implants. A highly cross-linked liner is favored to allow for maximum head size as the patient may be at increased risk of dislocation because of his neurologic disorder.
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
QUESTION 20
A 52-year-old man who weighs 325 lb is wheelchair-bound from severe degenerative arthritis of the left hip. Twenty-four hours after cementless total hip arthroplasty, he develops shortness of breath and evaluation shows a saddle pulmonary embolus. The patient is started on enoxaparin sodium at 150 mg every 12 hours. Two days later, the patient’s hematocrit is 20% despite four units of transfused packed cells, and he now has developed a complete sciatic nerve palsy. What is the best course of action?
1
Emergent exploration of the sciatic nerve
2
Transfusion to raise the hematocrit to 30% and sequential neurovascular examinations
3
Placement of a vena cava filter, halt anticoagulation, blood transfusion, and exploration of the sciatic nerve
4
Transfusion to raise the hematocrit to 30%, continued administration of enoxaparin, and sequential neurovascular examinations
5
Placement of a temporary vena cava filter and exploration of the sciatic nerve
The purpose of this question is to draw attention to the early risks of therapeutic anticoagulation that will be instituted by an intensivist or pulmonologist to treat a life-threatening pulmonary embolus. The temporary vena cava filter is a recent innovation but will effectively reduce the risk of further pulmonary emboli. This requires reversal of anticoagulation for safe insertion of the filter and creates a safe situation for additional surgical solutions. Sciatic nerve compromise was caused by the expanding hematoma in this patient, which could be mitigated by exploration both to assess the nerve and to remove a large hematoma that presents its own longterm risks.
REFERENCES: Della Valle CJ, Steiger DJ, Di Cesare PE: Thromboembolism after hip and knee arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:327-336.
Weil Y, Mattan Y, Goldman V, et al: Sciatic nerve palsy due to hematoma after thrombolysis therapy for acute pulmonary embolism after total hip arthroplasty. J Arthroplasty 2006;21:456-459.
[American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty, ](http://www.aaos.org/research/guidelines/)[www.aaos.org/research/guidelines/](http://www.aaos.org/research/guidelines/) PEguide.asp
QUESTION 21
What is the most common cause of reoperation following contemporary hip resurfacing for degenerative coxarthrosis?
1
Limb-length discrepancy
2
Altered femoral offset
3
Snapping psoas tendon
4
Limitation of hip movement
5
Femoral neck fracture
Femoral neck fracture, necessitating revision surgery to a total hip arthroplasty, is the most likely common early complication after hip resurfacing. Cortical notching, varus positioning, and other technical variables appear to predispose to this complication. Limb lengths do not change appreciably after hip resurfacing; the same applies to femoral offset. Hip movement is not limited by hip resurfacing, and there is no evidence that psoas tendon impingement is increased by hip resurfacing.
REFERENCES: Steffen RT, Pandit HP, Palan J, et al: The five-year results of the Birmingham Hip Resurfacing arthroplasty: An independent series. J Bone Joint Surg Br 2008;90:436-441.
Amstutz HC: Present state of metal-on-metal hybrid hip resurfacing. J Surg Orthop Adv 2008;17:12-16.
QUESTION 22
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?
1
Postoperative indomethacin for 3 weeks
2
Postoperative indomethacin for 6 weeks
3
No treatment indicated; can treat later if heterotopic bone forms
4
800 centigrey of radiation given to the periprosthetic soft tissues preoperatively on the morning of surgery
5
400 centigrey of radiation given to the periprosthetic soft tissues day 2 postoperatively
This question centers on the prophylactic treatment to reduce the risk of heterotopic bone formation. Prophylaxis is indicated because he has already demonstrated bone formation with his prior hip arthroplasty, which places him at increased risk for developing heterotopic bone on the contralateral side. He is on warfarin and has renal insufficiency, which makes the use of NSAIDs contraindicated. The recommended dose is 600 to 800 centigrey of radiation given within 24 hours of surgery preoperatively or 72 hours postoperatively.
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
QUESTION 23
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
1
BMI >30
2
Presence of secondary changes of the acetabulum
3
Osteonecrosis of the femoral head
4
Age of younger than 55 years old
5
Male gender
This young patient has osteonecrosis of the femoral head with a large area of collapse.
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. distal femoral varus osteotomy.
2. osteoarticular transplant to the lateral femoral condyle.
3. unicondylar arthroplasty.
4. high tibial osteotomy.
5. Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
QUESTION 24
A healthy 78-year-old woman falls down a flight of stairs 2 years after undergoing left total hip arthroplasty. Radiographs are shown in Figures 25a through 25c. Optimal management should include which of the following?
1
Skeletal traction
2
Long stem femoral revision
3
Closed reduction and internal fixation with a retrograde femoral nail
4
Open reduction and internal fixation with a conventional plate and screws
5
Open reduction and internal fixation with a plate, proximal cables, and distal screws
The fracture occurs distal to the component, and does not jeopardize the cemented implant
fixation. The cement mantle is intact. The component appears well fixed and without osteolysis. In such cases, the femoral component can be left alone and the fracture fixed with internal fixation. There is no available intramedullary space proximal to the fracture to allow for a retrograde nail. A standard plate cannot obtain adequate fixation of the proximal fragment due to the presence of the femoral stem. Therefore, a plate that uses screws distal to the fracture and cables proximal to the fracture is the treatment of choice. Skeletal traction is usually reserved for patients unable to withstand surgery. This fracture is classified as a type C, according to the Vancouver classification of postoperative femoral fractures.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Brady OH, Garbuz DS, Masri BA, et al: The reliability and validity of the Vancouver classification of femoral fractures after hip replacement. J Arthroplasty 2000; 15:59-62.
QUESTION 25
Osteolysis after total hip arthroplasty with polyethylene acetabular bearings is most closely correlated with which of the following risk factors?
1
Patient weight
2
Femoral head bearing material
3
Linear wear rate
4
Decreased femoral offset
5
Increased femoral offset
The development of osteolysis appears to be multifactorial. Patient activity, component positioning, polyethylene oxidation level, and bearing surface all appear to contribute. They contribute, however, by increasing the rate of wear. Therefore, the one variable that correlates closest with the likelihood of osteolysis (and the magnitude of osteolysis) is the wear rate of the bearing couple. Wear can be measured linearly or volumetrically. Both correlate with the development of osteolysis.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 521-528.
QUESTION 26
Which of the following patients requires preoperative noninvasive cardiac testing?
1
52-year-old man scheduled to undergo elective lumbar decompression and fusion, with a history of hypercholesteremia, hypertension, and deep venous thrombosis following treatment of an ankle fracture
2
67-year-old woman scheduled to undergo total knee arthroplasty, with a history of myocardial infarction, cerebrovascular accident, and diabetes mellitus
3
68-year-old woman scheduled to undergo total hip arthroplasty for osteonecrosis, no known medical comorbidities, but has not seen a physician in more than 20 years and drinks 7 to 10 alcoholic beverages per week
4
72-year-old man with an intertrochanteric hip fracture, with a history of chronic renal failure, colon
cancer, and obesity
5
81-year-old man with a fracture of the proximal femur, history of myocardial infarction, prostate adenocarcinoma, and hypothyroidism, and prior to the fracture he was able to climb a flight of stairs
Noninvasive cardiac testing is recommended in the presence of the three or more of the following risk factors in a sedentary patient: history of coronary artery disease or myocardial infarction, history of heart failure, prior cerebrovascular accident, and diabetes mellitus or chronic renal disease. Preoperative stress testing is not recommended if patients can perform moderate activities such as climbing a flight of stairs.
REFERENCES: Bushnell BD, Horton JK, McDonald MF, et al: Perioperative medical comorbidities in the orthopaedic patient. J Am Acad Orthop Surg 2008;16:216-227.
Auerback A, Goldman L: Assessing and reducing the cardiac risk of noncardiac surgery. Circulation 2006;113:1361-1376.
Fischgrund JS (ed): Orthopaedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, pp 105-113.
Figure 28
QUESTION 27
A 62-year-old woman undergoes an uncomplicated primary metal-on-metal cementless hip arthroplasty. Her early postoperative course is unremarkable. She returns at 1 year reporting groin pain. Her symptoms are made worse with stair climbing and getting in and out of her vehicle. Examination reveals minimal discomfort with passive range of motion, but straight leg raising reproduces her symptoms. A radiograph is shown in Figure 28. What is the most appropriate surgical management?
1
Revision of the femoral component
2
Psoas tendon tenotomy
3
Exchange of the bearing to metal-on-polyethylene
4
Exchange of the bearing to ceramic-on-ceramic
5
Exchange of the bearing to a smaller femoral head and metal liner
The radiograph shows a cementless cup that is placed low within the native acetabulum and appears large relative to the patient’s native acetabulum. The size and inferior position of the cup place it at risk for causing psoas tendon irritation or impingement. Symptoms are typical for irritation of the psoas tendon and not consistent with either a loose implant (more mechanical activity-related pain) or metal hypersensitivity (more constant pain and not just associated with hip flexion activities). Controversy exists regarding tenotomy versus acetabular revision.
REFERENCES: Dora C, Houweling M, Koch P, et al: Iliopsoas impingement after total hip replacement: The results of non-operative management, tenotomy or acetabular revision. J Bone Joint Surg Br 2007;89:1031-1035.
Heaton K, Dorr LD: Surgical release of iliopsoas tendon for groin pain after total hip arthroplasty. J Arthroplasty 2002; 17:779-781.
Malik A, Maheshwari A, Dorr LD: Impingement with total hip replacement. J Bone Joint Surg Am 2007;89:1832-1842.
Trousdale RT, Cabanela ME, Berry DJ: Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty
1995;10:546-549.
QUESTION 28
Increasing tibial polyethylene conformity can have what effect on fixed bearing total knee arthroplasty?
1
Increased contact stress within the polyethylene
2
Increased risk of polyethylene delamination
3
Decreased mechanical forces transferred to the fixation surfaces
4
Decreased femoral rollback during flexion
5
Increased femoral rotation during flexion
Increasing conformity between the tibial polyethylene bearing and the femoral component has desirable and undesirable consequences. Increased conformity increases the contact area and thereby reduces contact stress within the polyethylene. This can lead to less risk of polyethylene wear, fracture, and delamination. However, increasing conformity also limits the ability of the femur to roll back during flexion, and may transfer increased shear stress to the fixation surfaces of the implants.
REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop Relat Res 2001;392:232-238.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
QUESTION 29
The anterior approach to total hip arthroplasty requires dissection between which of the following muscle planes?
1
Sartorius and gluteus maximus
2
Gluteus minimus and rectus femoris
3
Rectus femoris and sartorius
4
Tensor fascia lata and sartorius
5
Tensor fascia lata and rectus femoris
The anterior approach to the hip joint involves identifying the plane between the tensor fascia lata and the sartorius muscles.
REFERENCES: Berger RA, Duwelius PJ: The two-incision minimally invasive total hip arthroplasty: Technique and results. Orthop Clin North Am 2004;35:163-172.
Matta JM, Shahrdar C, Ferguson T: Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 2005;441:115-124.
28 • American Academy of Orthopaedic Surgeons
Figure 3Id Figure 31e
QUESTION 30
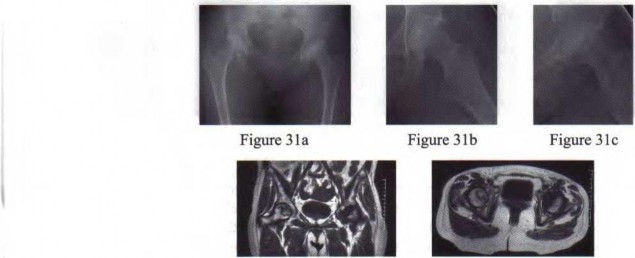
A 41-year-old female postal worker reports a 9-month history of left groin and lateral hip pain. She denies pain in the right hip. Her social history reveals that she smokes and drinks on average five alcoholic beverages per week. Her body mass index (BMI) is 26. Radiographs are shown in Figures 31a through 31c and coronal and axial MRI scans are shown in Figures 3 Id and 31e, respectively. What is the most important factor that will determine if her right hip will become symptomatic?
1
Patient age
2
Gender of the patient
3
Patient’s BMI and activity level
4
Size of the lesion
5
Association with alcohol use
Several factors have been examined as potentially predictive of progression in the patient with an asymptomatic osteonecrotic lesion of the femoral head. While the presence of ongoing risk factors, lesion location, lesion stage, age, gender, and BMI have all been suspected as important, the size of the lesion, particularly when over one third of the size of the femoral head, is a significant risk factor for progression.
REFERENCES: Nam KW, Kim YL, Yoo JJ, et al: Fate of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am 2008;90:477-484.
Hungerford DS, Jones LC: Asymptomatic osteonecrosis: Should it be treated? Clin Orthop Relat Res 2004;429:124-130.
Figure 32a Figure 32b Figure 32c Figure 32d
QUESTION 31
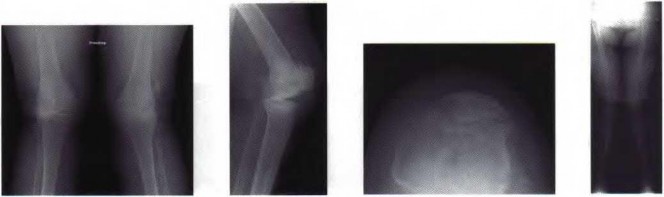
A 66-year-old woman reports pain in both of her knees that has been recalcitrant to nonsurgical management. Radiographs, including an AP of both knees, lateral and patellar views of the more symptomatic left knee and a mechanical axis, are shown in Figures 32a through 32d. The lateral radiograph shows maximal knee extension. When counseling the patient preoperatively regarding the risks of total knee arthroplasty, she should be educated that she is at higher risk than the typical patient for which of the following complications?
1
Deep venous thrombosis
2
Peroneal nerve injury
3
Wound healing problems
4
Femoral component loosening
5
Quadriceps tendon rupture
The patient has a large valgus deformity and flexion contracture that places her at increased risk for peroneal nerve injury. The peroneal nerve is tethered at the fibular head and correction of her valgus deformity and flexion contracture at the time of total knee arthroplasty can stretch the nerve, leading to peroneal nerve palsy.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 147155.
Asp JP, Rand JA: Peroneal nerve palsy after total knee arthroplasty. Clin Orthop Relat Res 1990;261:233- 237. Schinsky MF, Macaulay W, Parks ML, et al: Nerve injury after primary total knee arthroplasty. J Arthroplasty 2001; 16:1048-1054.
_AL-Madena Copy_
Figure 33a Figure 33b
QUESTION 32
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The _A_ A _L-M_ P _a_ r _d_ a _e_ d _n_ i _a_ o _C_ g _o_ r _p_ a _y_ ph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage?
1
Hip arthroscopy and labral debridement
2
Femoroacetabular osteoplasty and labral repair
3
Femoral osteotomy
4
Hemiarthroplasty
5
Total hip arthroplasty
The patient has femoroacetabular impingement. The prominence on the femoral neck has
resulted in a labral tear and detachment. An MR-arthrogram is the most appropriate modality for diagnosis of a labral tear. The diagnosis of a labral tear per se is not an indication for surgical intervention because the natural incidence of this condition is not known. Labral debridement without addressing the underlying anatomic abnormality is likely to result in a suboptimal outcome. The most appropriate treatment, when indicated, is shaving down of the femoral neck to remove the bony prominence and attachment of the labrum. Femoral osteotomy has no role in the treatment of this condition. The patient has minimal arthritis; therefore, arthroplasty is not indicated.
REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Relat Res 2003;417:112-120.
Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
QUESTION 33
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
1
Observation of the limb for 4 hours to see if the arterial spasm resolves
2
Measurement of lower leg compartment pressures
3
Magnetic resonance angiogram
4
Emergent return to the operating room for wound exploration while the patient anesthesia
5
Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
QUESTION 34
With respect to the safety of allogeneic transfusions, which of the following infectious diseases is not tested for during routine laboratory blood screening?
1
Human immunodeficiency virus (HIV)
2
Hepatitis C
3
Lyme disease
4
Syphilis
5
West Nile virus encephalitis
Routine screening of donated blood usually includes screening for Hepatitis B, Hepatitis C, syphilis, HIV-1 (responsible for AIDS), HIV-2, and West Nile virus. Several bloodbome diseases that are not routinely screened for during blood donation include Lyme disease, malaria, babesiosis, and Chagas disease. Because routine blood bank practices do not include screening for all potential bloodbome diseases, surgeons should be aware of the possibility of disease transmission.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 217-224.
QUESTION 35
A 57-year-old man undergoes total hip arthroplasty, has an uncomplicated early postoperative course, and a normal neurovascular status is documented. However, on postoperative day two he develops a progressive foot drop that increases over the next 24 hours. Postoperative repeat radiographs of the hip arthroplasty are unrevealing. There is no suggestion of swelling of the thigh to suggest a subfascial wound hematoma. What is the next most appropriate step?
1
MRI of the lumber spine
2
MRI of the knee joint
3
Electromyography and nerve conduction velocity studies of the sciatic nerve
4
Lumbar spine anterior/posterior and lateral radiographs
5
Venous Doppler of the lower extremity
Spinal stenosis is commonly found in patients with degenerative arthritis of the hip joint and would be a strong possibility for causing a foot drop if the radiographs do not reveal a dislocation or other direct mechanical cause for the sciatic nerve compromise.
REFERENCES: Dehart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Pritchett JW: Lumbar decompression to treat foot drop after hip arthroplasty. Clin Orthop Rel Res 1994;303:173-177.
QUESTION 36
A 68-year-old woman undergoes an uncomplicated primary total knee arthroplasty with cement. Twelve days later, the proximal wound appears healed and pain is decreased, but the distal wound continues to drain with slight surrounding redness. What is the most appropriate management?
1
Prescribe an antibiotic specific for hospital-acquired bacteria.
2
Recommend antibiotic ointment and peroxide treatment.
3
Place the knee in an immobilizer and observe.
4
Place sutures to close up the wound in the clinic.
5
Irrigate and debride the knee in the operating room.
Persistent wound drainage after a total knee arthroplasty can lead to infection and other complications. In this situation, antibiotics alone are not indicated, nor are topical wound treatment measures. Prompt, aggressive treatment includes returning the patient to the operating room for irrigation and debridement, with possible polyethylene exchange. Resection of components is not necessarily indicated at this early stage because the arthroplasty can still be salvaged.
REFERENCES: Vince K, Chivas D, Droll KP: Wound complications after total knee arthroplasty. J Arthroplasty 2007;22:39-44.
Dennis DA: Wound complications in total knee arthroplasty. Orthopedics 1997;20:837-840.
QUESTION 37
A nondisplaced fracture of the proximal medial femoral neck proximal to the lesser trochanter is noted at the time of insertion of a cementless tapered wedge-type femoral component in a total hip arthroplasty. Appropriate perioperative management should include which of the following?
1
Cerclage cable placed proximal to the lesser trochanter with partial weight bearing for 6 weeks postoperatively
2
No intraoperative or postoperative modifications are necessary
3
Non-weight-bearing for 6 weeks, retention of the femoral component, and no cerclage wire
4
Fracture exploration and repair with multiple cerclage cables, strut allograft and revision of the femoral component with a long-stemmed implant
5
Revision with a cemented implant
The fracture should be explored in its entirety. If it remains in the intertrochanteric region, a single cerclage cable passed above the lesser trochanter and tightened around the femoral component is appropriate. A more distal or displaced fracture should be repaired with cerclage cables and consideration for revision of the femoral component with a long-stemmed or cemented implant should be given.
REFERENCES: Sharkey PF, Hozack WJ, Booth RE, et al: Intraoperative femoral fractures in cementless total hip arthroplasty. Orthop Rev 1992;21:337-342.
Sharkey PF, Wolf LR, Hume EL, et al: Insertional femoral fracture: A biomechanical study of femoral component stability. Semin Arthroplasty 1990;1:91-94.
Figure 39a Figure 39b Figure 39c
QUESTION 38
A 68-year-old woman reports pain and sensations of instability following a primary total knee arthroplasty 18 months ago. A preoperative radiograph is shown in Figure 39a and postoperative AP and patellar view
radiographs are shown in Figures 39b and 39c. A CT scan shows that the femoral component is internally rotated 8 degrees and the tibial component is internally rotated 4 degrees. Management should include which of the following?
1
A structured physical therapy program
2
A custom patellar stabilizing brace
3
Modular polyethylene liner exchange to a thicker liner
4
Revision of the femoral and tibial components
5
An open lateral retinacular release
The patient had a valgus knee preoperatively and in these patients, care must be taken to avoid internal rotation of the femoral component that can lead to patellar instability. At the present time she has a completely dislocated patella, evidence of coronal instability on her AP radiograph, and internally rotated femoral and tibial components; therefore, management should consist of revision of both of her components to place them in appropriate external rotation.
REFERENCES: Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention, and management. J Am Acad Orthop Surg 2003; 11:364-371.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 40
The term “paradoxical motion,” used to describe knee kinematics, is best described by which of the following definitions?
1. The patella does not roll forward into the trochlear groove during knee extension.
2. The tibia rolls back on the femur during knee extension.
3. The tibiofemoral contact point moves anteriorly during knee flexion.
4. The posterior cruciate ligament rolls posteriorly with respect to the anterior cruciate ligament during knee extension.
5. The femur rolls back on the tibia during knee flexion.
PREFERRED RESPONSE: 3
DISCUSSION: The term “rollback” describes the posterior movement of the tibiofemoral contact point with knee motion from extension to flexion. Therefore, with “paradoxical rollback” this contact point moves anteriorly. “Paradoxical rollback” is a term used to connote the inability of the anterior cruciate- deficient, posterior cruciate-retaining total knee prosthesis to create normal posterior femoral rollback with knee flexion.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR: In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res 2003;410:114-130.
Incavo SJ, Mullins ER, Coughlin KM, et al: Tibiofemoral kinematic analysis after total knee arthroplasty.
J Arthroplasty 2004;19:906-910.
QUESTION 39
Patients with hip dysplasia have a series of anatomic abnormalities that most commonly include which of the following?
1
Shallow, medialized acetabulum that is deficient anteriorly and superiorly
2
Large contact area between the femoral head and acetabulum
3
Large femoral head with long femoral neck
4
Excessive femoral neck anteversion and a posterior greater trochanter
5
Decreased neck-shaft angle
Patients with developmental dysplasia of the hip share a common pattern of anatomic abnormalities including an acetabulum that is shallow, lateralized, anteverted, and deficient anteriorly and superiorly. On the femoral side, the head is usually small, the neck is short and anteverted with a posteriorly placed trochanter, and the femoral canal is small. The neck-shaft angle is typically increased. The contact area of the femoral head and acetabulum is typically decreased.
REFERENCE: Sanchez-Sotelo J, Trousdale RT, Berry DJ, et al: Surgical treatment of developmental dysplasia of the hip in adults: I. Nonarthroplasty options. J Am Acad Orthop Surg 2002; 10;321-333.
Figure 42
QUESTION 40
An 82-year-old man who underwent a primary total knee arthroplasty 11 weeks ago is now seen following a fall from a standing height. A radiograph is shown in Figure 42. Examination reveals a small abrasion of the skin overlying the anterior aspect of the knee. He is able to actively extend the the knee but has a 10-degree extensor lag. Initial management should include which of the following?
1
A 4-week period of immobilization followed by protected range of motion in a hinged knee brace
2
Use of a cylinder cast for 12 weeks
3
Open reduction and internal fixation of the fracture using a tension band technique 4 Revision of the patellar component
5/. Resection of the proximal bony fragment and soft-tissue repair
The patient has a periprosthetic fracture of the patella but is able to actively extend his knee. Despite the wide displacement of the fracture fragments, nonsurgical management is recommended given the high risk of complications and problems when open treatment of these fractures is undertaken.
REFERENCES: Ortiguera CJ, Berry DJ: Patellar fracture after total knee arthroplasty. J Bone Joint Surg Am 2002;84:532-540.
Parvizi J, Kim KI, Oliashirazi A, et al: Periprosthetic patella fractures. Clin Orthop Relat Res
2006;446:161-166.
Figure 43a Figure 43b
QUESTION 41
An active 72-year-old man underwent a right hybrid total hip arthroplasty for osteoarthritis 4 years ago. His hip has functioned well until approximately 8 months ago. He now reports activity-related proximal thigh pain and groin pain. A current radiograph is shown in Figure 43a. A radiograph obtained prior to the onset of symptoms is shown in Figure 43b. What is the most likely cause of his symptoms?
1
Polyethylene wear with polyethylene-induced synovitis
2
Psoas tendon irritation secondary to psoas impingement over the anterior inferior edge of the acetabular component
3
Loose femoral component
4
Osteolysis secondary to polyethylene wear particles
5
Modulus mismatch of the stem and femur
The radiograph shows a loose femoral component. The implant has debonded showing a radiolucent line at the lateral shoulder (zone 1), and also increased radiolucency at the bone cement interface medially. The patient’s symptoms are mechanical in nature with activity-related pain. Symptoms are not characteristic of psoas tendon irritation. Although osteolysis is present, in the absence of fracture it is generally asymptomatic. Additionally, in this patient the osteolysis involving the proximal femur is much more likely to be secondary to cement particulate debris and less likely related to polyethylene wear particles.
REFERENCES: Jasty M, Maloney WJ, Bragdon CR, et al: The initiation of failure in cemented femoral components of hip arthroplasties. J Bone Joint Surg Br 1991;73:551-558.
Kwong LM, Jasty M, Mulroy RD, et al: The histology of the radiolucent line. J Bone Joint Surg Br 1992;74:67-73.
Verdonschot N, Tanck E, Huiskes R: Effects of prosthesis surface roughness on the failure process of cemented hip implants after stem-cement debonding. J Biomed Mater Res 1998;42:554-559.
Figure 44
QUESTION 42
A 64-year-old woman who underwent a successful total hip arthroplasty (THA) 2 years ago now reports a painful hip. A radiograph is shown in Figure 44. Laboratory evaluation includes an erythrocyte sedimentation rate (ESR) of 65 mm/h (0-30 mm/h) and a C-reactive protein of 5.4 mg/L (< 0.8 mg/L). What is the next step in management?
1
Ultrasound examination
2
Technetium bone scan
3
Indium-labeled WBC scan
4
Hip joint aspiration
5
Two-stage revision surgery
Hip joint aspiration, with analysis of the cell count, differential, and culture greatly aids in the diagnosis of infection in THA. Aspiration is indicated in this patient because both the ESR and C-reactive protein are elevated, and the radiograph shows well-fixed components without evidence of loosening. Technetium and Indium-labeled WBC scans have less specificity and sensitivity respectively, and may not be necessary if the diagnosis is confirmed by joint aspiration. Two-stage revision surgery may be the treatment of choice if infection is confirmed, but it is not the next step in this patient.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
QUESTION 43
The American Academy of Orthopaedic Surgeons thrombophlebitis prophylaxis guidelines for patients undergoing total joint arthroplasty include which of the following?
1
General as opposed to regional anesthesia
2
Preoperative assessment for risk of thromboembolic disease as well as bleeding
3
Routine use of inferior vena cava filters
4
Warfarin with a goal International Normalized Ratio (INR) of 2-3 for patients with standard risk of bleeding and thrombophlebitis
5
Thromboembolic compression stockings (TEDs)
The 2007 AAOS guidelines for thrombophlebitis prophylaxis for patients undergoing total hip and knee arthroplasty includes preoperative risk assesment for deep venous thrombosis, pulmonary embolism, and
bleeding. Regional anesthesia when appropriate is suggested. Inferior vena cava filters may be appropriate in selected patients. When warfarin is used as a chemoprophylactic agent, the goal INR is less than or equal to 2 to minimize the risk of bleeding. This is in contrast to the 2004 ACCP guidelines for warfarin with a goal INR of 2-3.
-
[REFERENCE: American Academy of Orthopaedic Surgeons Guideline on the Prevention of Symptomatic Pulmonary Embolism in Patients Undergoing Total Hip or Knee Arthroplasty. ](http://www.aaos.org/Research/)[www.aaos.org/Research/](http://www.aaos.org/Research/) guidelines/PEguide.asp
Figure 46
QUESTION 44
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management?
L Intensive physiotherapy
1
Alendronate
2
Indomethacin
3
Radiotherapy
4
Excision
The presence of Brooker grade 1 or 2 heterotopic ossification (HO) does not influence the outcome of total hip arthroplasty, whereas restricted range of motion and pain may occur in patients with more severe grade 3 or 4 HO. Treatment may be nonsurgical or surgical. Nonsurgical management includes intensive physiotherapy during the maturation phase of the disease in an attempt to limit the final stiffness. There appears to be no data regarding the effectiveness of this treatment. There is no role for NSAIDs or radiotherapy as a treatment for preexisting HO. Surgical treatment involves excision of the heterotopic bone and can be expected to improve the functional outcome. Bisphosphonates have been used in the past, but their use has been discontinued as they only postpone ossification until treatment is stopped.
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
QUESTION 45
What is the most common cause of early failure for patellofemoral arthroplasty?
1
Progression of tibiofemoral arthritis
2
Loosening of the femoral trochlear component
3
Loosening of the patellar component
4
Patellar instability/maltracking
5
Rupture of the quadriceps tendon from trochlear component impingement secondary to excessive anterior placement and flexion of the implant
In properly selected patients who have no or minimal tibiofemoral arthritis, the most common cause of early failure is patellofemoral instability secondary to uncorrected patellar malalignment, soft-tissue imbalance, or component malposition. Progression of tibiofemoral arthritis is also a leading cause of failure, but occurs late in about 25% of patients. Loosening of components has occurred in less than 1% of knees with cemented implants. A higher rate of loosening has been reported in cementless implants.
REFERENCES: Lonner JH: Patellofemoral arthroplasty. J Am Acad Orthop Surg 2007;15:495-506. Argenson JN, Flecher X, Parratte S, et al: Patellofemoral arthroplasty: An update. Clin Orthop Relat Res 2005;440:50-53.
Figure 48
QUESTION 46
An 88-year-old nursing home resident is seen in the emergency department after a fall. At the time of admission, physical examination of the affected extremity reveals absent pulses and inadequate capillary refill. A radiograph is seen in Figure 48. Appropriate management includes which of the following?
1
Emergent open reduction and internal fixation of the fracture
2
Emergent consultation with vascular surgery and a possible arteriogram
3
Revision of the femoral component followed by vascular surgical consultation
4
Open reduction and internal fixation of the fracture with intraoperative vascular consultation
5
Release traction until surgical management is performed
The patient has a Vancouver type B3 periprosthetic femur fracture (fracture around a total hip prosthesis with a loose stem and poor proximal bone stock). This type of periprosthetic fracture necessitates revision of the femoral component as well as fracture fixation. This patient has diminished blood flow in the extremity that necessitates emergent vascular surgical evaluation.
REFERENCES: Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215-220,
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for the treatment of periprosthetic fractures. J
Bone Joint Surg Am 2005;87:1777-1781. Question 49
An otherwise healthy 58-year-old woman reports hip pain after undergoing total hip arthroplasty 8 months ago. She gives a history of prolonged wound drainage after surgery treated with antibiotics.
Hip aspiration is positive for methicillin-resistant coagulase-negative staphylococcus. Appropriate management at this point includes which of the following?
1. Arthroscopic irrigation followed by appropriate antibiotic treatment
2. Treatment with 6 weeks of IV vancomycin and oral rifampin
3. Treatment with 6 weeks of IV vancomycin and oral rifampin, followed by indefinite oral antibiotic suppression
4. Open debridement with exchange of the polyethylene insert, followed by appropriate antibiotic
treatment
5. Open debridement with removal of the implants and insertion of an antibiotic spacer
PREFERRED RESPONSE: 5
DISCUSSION: The patient has a late chronic periprosthetic infection. The history points to a missed postoperative infection where the patient was treated with antibiotics for prolonged wound drainage. A low virulent organism, such as coagulase-negative staphylococcus, is often the pathogen. In an otherwise healthy patient with a reasonable life expectancy, the goal of treatment should be cure of the infection. Treatment for late chronic infection requires removal of the implants. Treatment with antibiotics alone, or debridement without removal of the implants is generally unsuccessful. Controversy exists regarding one- stage treatment with immediate reimplantation versus two-stage treatment with delayed reimplantation. Generally, a higher cure rate is achieved with a two-stage reimplantation (approximately 90% to 93%) than with one-stage reimplantation (75% to 80%).
REFERENCES: Hanssen AD, Spangehl MJ: Treatment of the infected hip replacement. Clin Orthop Relat Res 2004;420:63-71.
Isiklar ZU, Demirors H, Akpinar S, et al: Two-stage treatment of chronic staphylococcal orthopaedic
implant-related infections using vancomycin impregnated PMMA spacer and rifampin containing antibiotic protocol. Bull Hosp Jt Dis 1999;58:79-85.
QUESTION 47
Patients with ankylosing spondylitis undergoing total knee arthroplasty are likely to experience which of the following complications?
1
Infection
2
Instability
3
Heterotopic ossification
4
Periprosthetic fracture
5
Patellar loosening
Patients with ankylosing spondylitis (AS) are likely to have achieved significant pain relief and improvement in function following total knee arthroplasty (TKA). These patients, however, are also likely to experience a higher incidence of complications, particularly stiffness and heterotopic ossification (HO). In one series, the incidence of HO following TKA in patients with AS was 20%.
REFERENCES: Parvizi J, Duffy GP, Trousdale RT: Total knee arthroplasty in patients with ankylosing spondylitis. J Bone Joint Surg Am 2001;83:1312-1316.
Fintersbush A, Amir D, Vatashki E, et al: Joint surgery in severe ankylosing spondylitis. Acta Orthop Scand 1988;59:491-496.
QUESTION 48
Posterior cruciate-retaining total knee arthroplasty has been studied by numerous methods including kinematic video fluoroscopy. Which of the following is the best description of typical kinematic behavior?
1
Unpredictable anterior femoral condylar translation from full extension to 90 degrees of flexion
2
Predictable femoral rollback from full extension to 90 degrees of flexion
3
Medial femoral condyle pivot with minimal medial femoral condyle translation and lateral femoral condyle posterior translation in flexion
4
Lateral femoral condyle pivot with minimal medial femoral condyle translation
5
Anterior tibial contact of both the medial and lateral femoral condyles in full extension
In vivo fluoroscopic studies have enlightened orthopaedic surgeons as to the actual kinematic performance of the total knee implants. Importantly, many technical factors combine to result in abnormal kinematics after total knee arthroplasty. The typical kinematics of the normal knee are negated by osteoarthritis and the various changes created by the surgeon’s technique. Dennis and associates observed that anterior femoral condylar translation during deep knee flexion was most commonly observed in posterior cruciate-retaining knees.
REFERENCES: Dennis DA, Komistek RD, Mahfouz MR, et al: Multicenter determination of in vivo kinematics after total knee arthroplasty. Clin Orthop Relat Res 2003;416:37-57.
Freeman MA, Pinskerova V: The movement of the normal tibio-femoral joint. J Biomech 2005-38'197- 208.
42 • American Academy of Orthopaedic Surgeons
Figure 52
QUESTION 49
A 52-year-old woman has a 60-degree extensor lag following a right total knee arthroplasty performed 16 months ago. Since the time of her primary total knee arthroplasty she has undergone primary repair of a patellar tendon rupture that occurred after a fall 8 months ago. A lateral radiograph of the knee is shown in Figure 52. A CT scan obtained to determine component rotation showed that the femoral component is internally rotated 9 degrees and the tibial component is internally rotated 12 degrees. Appropriate management at this time should include
1
a structured physical therapy program to increase quadriceps muscle strength.
2
a hinged knee brace locked in extension while ambulating.
3
exchange of the modular polyethylene spacer to a thicker insert and reconstruction of the patellar tendon using hamstring augmentation.
4
exchange of the modular polyethylene spacer to a thicker insert and reconstruction of the patellar tendon using an extensor mechanism allograft tensioned tightly in full extension.
5
revision of the tibial and femoral components and reconstruction of the patellar tendon using an extensor mechanism allograft tensioned tightly in full extension.
A chronic patellar tendon rupture is a difficult complication to manage. Patients typically present with both inability to extend their leg and instability of the extremity, oftentimes associated with multiple falls.
Attempts at secondary repair have been associated with high failure rates whereas the use of an extensor mechanism allograft has been shown to more effectively restore active extension in a substantial percentage of patients. Important aspects of the technique include fully tensioning the graft in full extension and immobilization of the extremity for 6 to 8 weeks postoperatively to allow for graft healing. Nonsurgical management will not result in an acceptable outcome for a young patient, and attempted secondary repair is associated with a high rate of failure, even when augmented with local tissues. This patient has gross rotational
malalignment of the components and the surgeon faced with this problem should consider obtaining a CT scan to determine component rotation preoperatively.
REFERENCES: Burnett RS, Berger RA, Paprosky WG, et al: Extensor mechanism allograft reconstruction after total knee arthroplasty: A comparison of two techniques. J Bone Joint Surg Am 2004;86:2694-2699.
Nazarian DG, Booth RE: Extensor mechanism allografts in total knee arthroplasty. Clin Orthop Relat Res
1999;367-123-129. , „. H
_AL-Madena Copy ^Lj-^M) Figure 53
QUESTION 50
Figure 53 shows the radiograph of a 48-year-old man who has a left side periprosthetic femoral fracture around the femoral stem of a previous revision hip arthroplasty. What is the most appropriate treatment?
1
Open reduction and internal fixation with a plate
2
Open reduction and internal fixation with a cable
3
Revision with a short stem and plate fixation
4
Revision with allograft prosthesis composite
5
Removal of the proximal femoral bone and replacement with a cemented segmental prosthesis
In type B3 fractures, the proximal femur is so deficient that it cannot be treated with open reduction and internal fixation or support a new femoral component. In younger patients, the femur can be reconstructed with allograft prosthesis composite to restore bone stock. Removal of the distal stem with trephines would compromise fixation with cement. Elderly and low-demand patients can be treated more simply with a cemented segmental replacement prosthesis, such as that used for tumor reconstruction.
REFERENCES: Parvizi J, Tarity TD, Slenker N, et al: Proximal femoral replacement in patients with non-neoplastic conditions. J Bone Joint Surg Am 2007;89:1036-1043.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.
Figure 54
QUESTION 51
A 66-year-old woman who underwent a right total knee arthroplasty 13 years ago now has pain, knee effusion, squeaking, and grinding in the operated knee. The patellar view radiograph is shown in Figure 54. What is most likely to be encountered during revision arthroplasty?
1
Loose femoral and/or tibial component
2
Fractured patella
3
Extensive metallosis
4
Patellar clunk
5
Ruptured extensor mechanism
Wear of the polyethylene insert of a metal-backed patellar or tibial component is a well-recognized complication following total knee arthroplasty. If the polyethylene insert completely wears out, the underlying metal-backed base plate will be in direct contact with the femoral component, resulting in scratching of the components and release of metal debris. The released metal debris results in black “tattooing” of the tissues or so-called metallosis. In addition, reactive synovitis and osteolysis occur secondary to a host response to both polyethylene debris and metal particles. Patients may report knee pain, swelling, squeaking, and an unstable feeling during walking and standing. Patellar clunk syndrome is characterized by the development of a fibrous nodule on the deep aspect of the quadriceps tendon that falls into the intercondylar notch of the femoral component during knee flexion.
REFERENCES: Chang FY, Tseng KF, Chen WM, et al: Metal-backed patellar component failure in total knee arthroplasty presenting as a giant calf mass. J Arthroplasty 2003;18:227-230.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed, metal-backed patellar
component. J Arthroplasty 2000;15:938-943.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Figure 55a Figure 55b
QUESTION 52
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
1
Nonsurgical management with the use of a cast-brace
2
Nonsurgical management with skeletal traction
3
Open treatment with a locked plate with or without strut allograft
4
Revision of the femoral component to a cemented femoral component that bypasses the fracture site by two cortical diameters
5
Revision of the femoral component to a cementless femoral component that bypasses the fracture site by at least two cortical diameters
The patient has a Vancouver type B2 periprosthetic femoral fracture with a loose, cementless femoral component. Radiographs show subsidence of the femoral component and the patient reports pain in the thigh for several years prior to the fall. When the femoral component is loose, revision is mandated to treat both the loose component and the fracture. Nonsurgical management is associated with a high risk of medical complications related to extended recumbency as well as a high rate of malunion and nonunion. Cementless femoral component revision has been shown to fare better than cemented femoral components, particularly for treating periprosthetic fractures of the femur.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
1. Discontinuation of the epidural and serial neurologic exams
2. Loosening of the surgical bandages and elevation of the extremity
3. MRI of the spine to evaluate for an epidural hematoma
4. Return to the operating room for angiography and vascular bypass
5. Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
QUESTION 53
What mechanical properties are observed in polyethylene used for total knee arthroplasty after the material undergoes oxidation?
1
Increased elastic modulus and decreased strength
2
Increased elastic modulus and increased ductility
3
Decreased elastic modulus and decreased strength
4
Decreased strength and increased ductility
5
Decreased elastic modulus and decreased ductility
When polyethylene undergoes oxidation, the material undergoes a decrease in strength and
ductility, and an increase in the elastic modulus. This makes the material more brittle, and leaves it vulnerable to delamination, fracture, and pitting.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee
Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 163-176.
QUESTION 54
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
i. Infection
1
Polyethylene wear
2
Instability
3
Patellar complications
4
Malalignment
There are multiple causes for failure of total knee arthroplasty, and more than one may exist at the same time. Sharkey and associates reviewed a series of revision total knee arthroplasties, and found that polyethylene failure was the most common cause of failure followed closely by component loosening. The most common cause of early failure (< 2 years post op) was infection. Instability and malalignment are both complications of surgical technique, and if these categories are combined, they would be the most common cause of all total knee failures.
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Figure 59a Figure 59b
QUESTION 55
Figures 59a and 59b show the radiographs of a 63-year-old woman who is seen in the emergency department after a minor twisting episode. History reveals that she underwent a successful mobile-bearing total knee arthroplasty for severe lateral compartment arthritis and valgus deformity 4 months ago. What is the most likely cause of this problem?
1
Flexion instability
2
Posterior cruciate ligament rupture
3
Lateral collateral ligament rupture
4
Chronic patellar instability
5
Prosthetic rotational malalignment
All of the instabilities listed may cause the above-noted radiographic appearance of a dislocated mobile-bearing total knee arthroplasty; however, the most likely scenario with reasonable placement of the implants and a lack of traumatic history, such as a fall, is flexion instability. Surgeons who consider the use of mobile-bearing implants must recognize that flexion and extension gap balancing is important to avoid insert subluxation.
REFERENCES: Thompson NW, Wilson DS, Cran GW, et al: Dislocation of the rotating platform after low contact stress total knee arthroplasty. Clin Orthop Relat Res 2004;425:207-211.
Stiehl JB: Clinical results and complications in mobile-bearing total knee arthroplasty. Instr Course Lect
2005;54:233-240.
QUESTION 56
Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?
1
Renal cell carcinoma
2
Leukocyte chromosomal aberrations
3
Carcinomas of the gastrointestinal tract
4
Soft-tissue sarcomas
5
Thyroid carcinoma
Metal-on-metal hip bearings have been associated with very low rates of wear and are commonly used in North America and Europe. Patients with these bearings have higher levels of metal ions (particularly cobalt and chromium) in the bloodstream than patients with bearings made of other materials. Although many researchers have been concerned that these ions may predispose to cancer, there has been no evidence that patients with metal-on-metal bearings are developing sarcomas or carcinomas with higher frequency than the general population. However, there has been mixed data as to whether hematopoietic malignancies are slightly more prevalent in patients with metal-on-metal bearings. Two recent reports have found chromosomal abnormalities, such as translocations and aneuploidy, to be increased in patients with metal-on-metal hip bearings. The clinical consequences of these changes, if any, remain unknown.
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
1. Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
2. Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
3. Hip spica pressure dressing and a 2-week course of oral antibiotics
4. Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
5. Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
PREFERRED RESPONSE: 2
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Figure 62
QUESTION 57
A 63-year-old woman reports pain in her groin, particularly when rising from a chair and when taking her first steps out of bed in the morning. History reveals that she underwent a left primary total hip arthroplasty 19 years ago. An AP radiograph is shown in Figure 62 and revision surgery is planned. What is the most reliable method for reconstruction of the acetabulum?
1
Use of a cemented, all polyethylene acetabular component
2
Use of a cementless, porous-coated acetabular component with adjunctive screw fixation
3
Use of an antiprotrusio cage
4
Use of a bilobed, cementless acetabular component
5
Use of a bipolar head placed directly into the acetabulum
The patient has severe wear and loosening of her cemented, all polyethylene acetabular component with a Paprosky type 2 acetabular defect. Optimal long-term results have been achieved with the use of a cementless, porous-coated acetabular component with adjunctive screw fixation. Cemented, all polyethylene components have been shown to have a high rate of failure when used in the revision setting. Bilobed components and antiprotrusio cages are unnecessary for this straightforward defect and have had mixed results reported in the literature. The use of a bipolar head placed directly into the acetabulum is associated with high rates of persistent pain and progressive acetabular erosion.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Schuaipaj T, Berger RA, et al: Revision of the acetabular component without cement after total hip
arthroplasty: A concise follow-up, at fifteen to nineteen years, of a previous report. J Bone Joint Surg Am 2005;87:1795-1800.
Templeton JE, Callaghan JJ, Goetz DD, et al: Revision of a cemented acetabular component to a cementless acetabular component: A ten to fourteen-year follow-up study. J Bone Joint Surg Am
2001;83:1706-1711.
QUESTION 58
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?
1
Observation, repeat radiographs, and reexamination in 6 weeks
2
A 14-day course of indomethacin
3
A 4-week course of indomethacin
4
Plan for a return to the operating room at 10 weeks for excision of the heterotopic bone
5
Arrange urgently for 800 centigrey of radiation to the soft tissues and areas of heterotopic bone around the hip, with shielding of the implants
The development of heterotopic bone occurs early after hip arthroplasty. The process begins within days after surgery; therefore, prophylactic treatment must be in the early postoperative period (preoperative radiation given within 24 hours of surgery, or postoperative radiation given within 72 hours of surgery, or nonsteroidal antiinflammatory drugs (NSAIDs) given postoperatively for 7 to 21 days - longer duration has not been shown to be of any additional benefit). At 6 weeks, prophylactic treatment with NS _AID_ s or radiation is no longer effective. Surgery at 10 weeks would be premature because the patient is currently asymptomatic with regards to the heterotopic bone, and surgery prior to full maturation of the bone may increase the risk for more abundant recurrence of bone.
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory
drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Figure 64
QUESTION 59
Figure 64 shows the radiograph of a 61-year-old man with ankylosing spondylitis. He is scheduled to undergo left total hip arthroplasty. Which of the following perioperative interventions should be considered?
1
Intraoperative sciatic nerve monitoring
2
Preoperative radiation therapy with 700 centigray
3
Postoperative radiation therapy with 1,500 centigray
4
Postoperative continuous passive motion
5
Soft cervical collar during postoperative physical therapy
Patients with ankylosing spondylitis are at high risk for heterotopic ossification after total hip arthroplasty, and perioperative prophylaxis with nonsteroidal anti-inflammatory drugs or radiation therapy has been effective at reducing the risk. Radiation prophylaxis given within 24 hours preoperatively has been shown to be as effective as radiation given postoperatively. Doses of 700 to 800 centigray have been shown to be as effective as higher doses with less potential risk. Continuous passive motion has not been shown to improve the postoperative flexibility of these patients. Although these patients may have stiff spines and may be at risk for neurologic injury in the event of spinal fracture, a soft cervical collar is not expected to alter the risk should a catastrophic spinal injury occur. Since there has been no shortening of the limb, the sciatic nerve should not be at significantly higher risk for neurapraxia than with a more routine hip arthroplasty.
REFERENCES: Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;8:870-881.
Pellegrini VD Jr, Konski AA, Gastel JA, et al: Prevention of heterotopic ossification with irradiation after total
hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
QUESTION 60
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
1
In the second stage there is decreased catabolic activity with less matrix breakdown.
2
In the second stage there is less chondrocyte proliferation and decreased matrix production.
3
Matrix degradation includes increased proteoglycan production, more proteoglycan
production, and longer glycosaminoglycan chains.
4
Cartilage degeneration may be initiated by inflammation, overload, or decreased matrix production.
5
Chondrocyte repair responses improve with aging.
Inflammation, overload, or decreased matrix production may lead to cartilage degeneration. During the second stage of articular cartilage degeneration with osteoarthritis, there is increased chondrocyte activity with proliferation and increased production of extracellular matrix. At the same time, there is an increase in catabolic activity with removal of damaged matrix to facilitate matrix remodeling. Chondrocyte repair response decreases with aging. Matrix degradation includes decreased proteoglycan production, less aggregation, and shorter glycosaminoglycan chains.
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
QUESTION 61
An active 38-year-old male carpenter reports activity-related medial knee pain. Arthroscopy performed 3 years ago revealed a torn medial meniscus that was debrided and mild condylar changes of the medial femoral condyle and medial tibial plateau. Current standing radiographs reveal Ahlback stage II changes with mild medial femoral joint space narrowing and a 5-degree varus deformity. What is the best treatment option?
1
High tibial osteotomy
2
Arthroscopic debridement and condylar “microfracture”
3
Osteoarticular transplant to the medial femoral condyle
4
Unicondylar arthroplasty
5
Total knee arthroplasty
The choice of high tibial osteotomy is appropriate to correct a deformity that has a very high risk of leading to progressive arthritis. It should be more important than either the arthroscopic method or the osteoarticular transplantation, though one may also consider these options. Prosthetic choices are limited for a young active male in favor of less “end stage” options.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and
function decline in knee osteoarthritis. JAMA 2001;286:188-195.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005-13 279289.
QUESTION 62
A patient with a severe nickel allergy and degenerative joint disease of the hip would be best served by which of the following prosthetic options?
1
Cemented titanium stem, ceramic (alumina) head, and press-fit titanium cup
2
Cemented cobalt-chrome stem, ceramic (alumina) head, and press-fit cobalt-chrome cup
3
Press-fit titanium stem, cobalt-chrome head, and press-fit titanium cup
4
Press-fit titanium stem, titanium head, and press-fit titanium cup
5
Press-fit titanium stem, ceramic (alumina) head, and cementless titanium cup
Nickel is present in cobalt-chrome and stainless steel alloys used in orthopaedic surgery; therefore, these materials are not well suited for nickel-sensitive patients. Nickel is not present in titanium alloys or in ceramic components. Titanium is therefore the material of choice for the femoral and acetabular component.
Titanium is a poor option for the femoral head due to its susceptibility to abrasive wear. Titanium is also poorly suited to cemented applications in hip arthroplasty because it is less stiff than cobalt-chrome (and stainless steel), and therefore transmits greater stresses to the cement column. Titanium’s poor abrasion resistance can also leave the component susceptible to increased abrasive wear in the event of loosening and micromotion. Therefore, of the options available, a cementless titanium stem and socket with a ceramic head is the best choice. In nickel-sensitive total knee arthroplasty patients, cemented oxidized zirconium femoral components can be used in place of cobalt-chrome, and titanium tibial components (press-fit or cemented) have been used with success.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 63
Implant position at the time of primary total knee arthroplasty to optimize patellar tracking includes which of the following?
1
External rotation of the femoral and tibial components
2
Internal rotation of the femoral component and external rotation of the tibial component
3
Internal rotation of the femoral and tibial components
4
Medialization of the femoral component
5
Lateralization of the patellar component
Component rotation is a critical factor to optimizing patellar tracking at the time of primary and
revision total knee arthroplasty. Both the femoral and tibial components should be externally rotated whereas the patellar components should be medialized.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123145.
Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee
arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
Malo M, Vince KG: The unstable patella after total knee arthroplasty: Etiology, prevention and management. J Am Acad Orthop Surg 2003; 11:364-371.
QUESTION 64
The placement of supplemental screw fixation with acetabular component fixation is a typical adjunct measure but carries the greatest risk of vascular injury if placed in which of the following positions?
1
Superior
2
Posterior superior
3
Posterior inferior
4
Superior lateral
5
Anterior superior
Anatomic studies indicate that the safe areas for screws are superior and posterior. The external illiac artery is at risk with anteromedial placement, and the sciatic nerve may be compromised by posterior inferior screw placement.
REFERENCES: Lavemia CJ, Cook CC, Hernandez RA, et al: Neurovascular injury in acetabular reconstruction cage surgery: An anatomical study. J Arthroplasty 2007;22:124-132.
Wasielewski RC, Galat DD, Sheridan KC, et al: Acetabular anatomy and transacetabular screw fixation at the
high hip center. Clin Orthop Relat Res 2005 ;43 8:171 -176.
_AL-Madena Copy_
QUESTION 65
A 71-year-old woman has a failed revision hip arthroplasty and is undergoing a re-revision hip arthroplasty. Her last hip surgery was 4 years ago with revision of the acetabular component. Radiographs show a well-fixed extensively porous-coated femoral component and a failed acetabular component with proximal and medial migration through the floor of the acetabulum. Preoperative laboratory studies reveal an erythrocyte sedimentation rate (ESR) of 70 mm/h (normal 0-29 mm/h), a C-reactive protein (CRP) of 23.3 (normal 0.2-8.0), and a negative hip aspiration. At the time of surgery, tissues look inflamed and a frozen section shows 20 WBC per high power field; however, a Gram stain is negative. What is the most appropriate action at this point?
1
Proceed with the revision as planned
2
Obtain cultures and proceed with revision of the acetabulum only
3
Obtain cultures and proceed with revision of the femur only
4
Obtain cultures, remove the implants, and insert an antibiotic spacer
5
Obtain cultures and close
Despite the negative aspiration preoperatively, intraoperative findings are suspicious for infection. Additionally, the preoperative blood work is also concerning for infection with an elevated CRP and ESR. The frozen section is also positive. Most important is the unreliability of the Gram stain. Numerous investigators have show high false negative rates for Gram stain in chronic periprosthetic infection. The Gram stain should not be relied on for decision-making in revision surgery, particularly when other investigations point to infection. With the information available, the diagnosis is deep infection. The best course of action is to obtain cultures, remove the implants, and insert an antibiotic spacer. Only obtaining cultures and closing would require a second operation to remove the implants if the cultures are positive.
REFERENCES: Sanzen L, Sundberg M: Periprosthetic low-grade hip infections: Erythrocyte sedimentation rate and C-reactive protein in 23 cases. Acta Orthop Scand 1997;68:461-465.
Spangehl MJ, Hanssen AD, Osman DR: Diagnosis and treatment of the infected hip arthroplasty, in Morrey BF(ed _A_)_L_ :_-M_ Jo _a_ i _d_ n _e_ t _na_ R _C_ e _o_ p _p_ l _y_ acement Arthroplasty, ed 3. Philadelphia, PA, Churchill Livingstone, 2003, pp 856-874. Question 71
A 79-year-old patient has a history of peripheral vascular disease and reports chronic knee pain. She has had coronary artery disease treated with angiography and stents on two occasions. Peripheral pulses are absent in both lower extremities, but the patient is disabled by advanced chronic degenerative arthritis in her right knee and would like to proceed with a total knee arthroplasty. The next most appropriate evaluation should include which of the following?
1. Ankle-brachial index of the affected lower extremity
2. Femoral popliteal angiography
3. Venous Dopplers of both lower extremities
4. MRI of the popliteal fossa
5. Radiographs to identify calcified plaques in the femoral artery
PREFERRED RESPONSE: 1
DISCUSSION: This question is designed to draw attention to the fact that peripheral vascular disease carries an increased risk of complications for the patient and should be carefully evaluated. The vascular surgeon will make the choice of revascularization or surgical clearance for knee reconstruction based on the initial results of the ankle-brachial index.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9:253-257.
Figure 72
QUESTION 66
A 56-year-old woman with rheumatoid arthritis who underwent total hip arthroplasty 17 years ago now reports pain and progressive shortening of the extremity over the past year. An AP radiograph of the hip is shown in Figure 72. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 34 mm/h (normal 0 to 28 mm/h) and a C-reactive protein of 10.2 (normal 0.2-8.0). She is presently taking oral antibiotics for a urinary tract infection. What is the next most appropriate step in management?
1
Aspiration of the hip joint and if negative, revision of the acetabular component
2
Aspiration of the hip joint and culture once she has discontinued the antibiotics for 3 weeks
3
Triple phase bone scan
4
Indium-111 leukocyte scan
5
Serial plain radiographs and protected weight bearing
The patient has a loose acetabular component, which explains her pain and progressive shortening. She has a history of inflammatory arthritis, elevated ESR and C-reactive protein, and has recently been treated for an infection. Thus, the suspicion for infection is high and must be ruled out. A triple phase bone scan can assist in the identification of component loosening but cannot differentiate infection from noninfectious causes. Indium-111 scans have been shown to have limited utility, although a negative scan can be helpful in ruling out infection. The selective preoperative use of aspiration of the hip joint has been shown to be effective and is most likely to identify infection; however, the patient must be off of antibiotics for a minimum of 2 weeks prior to her aspiration to avoid a false negative culture.
REFERENCES: Della Valle CJ, Zuckerman JD, Di Cesare PE: Periprosthetic sepsis. Clin Orthop Relat Res 2004;420:26-31.
Lachiewicz PF, Rogers GD, Thomason HC: Aspiration of the hip joint before revision total hip arthroplasty:
Clinical and laboratory factors influencing attainment of a positive culture. J Bone Joint Surg Am 1996;78:749-754. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Figure 73
QUESTION 67
An active 18-year-old patient reports severe left hip pain that prevents her from playing lacrosse. An AP radiograph of the pelvis is shown in Figure 73. What is the most appropriate option for this patient?
1
Activity modification
2
Hip fusion
3
Periacetabular osteotomy
4
Femoral osteotomy
5
Total hip arthroplasty
The patient has developmental dysplasia of the hip (DDH). There is anterolateral deficiency of the acetabulum as is evidenced by the increased acetabular index and the reduced center- edge angle. The patient has some arthritis of the hip with narrowing of the joint space and cyst formation visible on the radiograph. Although all of the mentioned choices may be acceptable treatments for dysplasia of the hip, periacetabular osteotomy is the best and most appropriate option for this young patient. Periacetabular osteotomy allows correction of the problem and can even improve the joint space as the new region of the acetabulum is rotated into the weight-bearing region. Hip fusion is very poorly tolerated by young patients, especially women. Femoral osteotomy alone is unlikely to address the problem because the major problem is on the acetabular side. Although the patient has arthritis, because of the young age of the patient, prosthetic replacement is not an attractive option. The outcome of periacetabular osteotomy even for patients with moderate arthritis has been favorable, deferring the need for total hip arthroplasty by a mean of 6.5 years.
REFERENCES: Weinstein SL, Mubarak SJ, Wenger DR: Developmental hip dysplasia and dislocation: Part 1. Instr Course Lect 2004;53:523-530.
Parvizi J, Burmeister H, Ganz R: Previous Bernese periacetabular osteotomy does not compromise the results of total hip arthroplasty. Clin Orthop Relat Res 2004;423:118-122.
Figure 74
QUESTION 68
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of
1
primary repair of the MCL and use of a posterior stabilized total knee arthroplasty (TKA) prosthesis.
2
augmentation of the MCL with a collagenous tissue scaffold and use of a posterior stabilized TKA
prosthesis.
3
complete release of the lateral collateral ligament (LCL) and use of a posterior stabilized TKA prosthesis.
4
lateral unicompartmental arthroplasty.
5
use of a varus-valgus constrained TKA prosthesis.
Patients with severe valgus deformity may have near complete attenuation of the MCL. Attempts at ligament repair or reconstruction at the time of TKA can have unpredictable outcomes, leading to an unstable TKA. Although there may be a role for trying to reconstruct the ligament in conjunction with a nonconstrained implant in young patients with long life expectancies, in elderly patients a constrained prosthesis can provide varus-valgus stability with a predictable outcome. In younger patients, there is concern that the extra prosthetic constraint may shorten the longevity of the prosthetic fixation. In older patients, the constrained implant is likely to last a lifetime, with several studies documenting excellent survivorship (96%) at 10 years. Complete release of the LCL will leave the knee grossly unstable medially and laterally, and could necessitate a hinged prosthesis.
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.
Figure 75
QUESTION 69
Figure 75 shows the radiograph of a healthy 52-year-old woman who has severe right hip pain that has been unresponsive to nonsurgical management. What is the most appropriate surgical procedure at this time?
1
Total hip arthroplasty
2
Hemiarthroplasty of the hip
3
Valgus femoral osteotomy
4
Periacetabular osteotomy
5
Varus femoral osteotomy
The patient has developmental dysplasia of the right hip, as can be noted by the shallow acetabulum and lack of femoral head coverage. She has secondary osteoarthritis, manifested radiographically by joint space narrowing, periarticular sclerosis, and subchondral acetabular cyst formation. Femoral and/or acetabular redirectional osteotomies are most effective when performed before the onset of arthritis. After osteoarthritis has set in, total hip arthroplasty is the most reliable procedure for reducing pain. Hemiarthroplasties are not indicated in the presence of arthritic changes of the acetabulum.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 403-414.
QUESTION 70
Which of the following surgical maneuvers is most likely to enhance proper patellar tracking during total knee arthroplasty and minimize the need for a lateral retinacular release?
1
Use of a mobile-bearing prosthesis
2
Anterior placement of the tibial tray
3
Internal rotation of the femoral component
4
Internal rotation of the tibial component
5
External rotation of the tibial component
Slight external rotation of the tibial component medializes the tibial tubercle and helps reduce the tendency for lateral patellar maltracking. Mobile bearings have not been shown to improve patellar tracking.
Internal rotation of the tibial or femoral component will accentuate patellar maltracking. AP positioning of the tibial tray will affect the force across the patella, but it is not likely to affect patellar tracking.
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337. Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective randomized study of 240 primary total knee arthroplasties. Clin Orthop Relat Res 2004:428:221-227.
Figure 77a Figure 77b
QUESTION 71
An obese 62-year-old man (BMI 38) who underwent a cementless total hip arthroplasty 14 months ago fell from a ladder and is now unable to bear weight on the extremity. A radiograph from his 3-month visit is shown in Figure 77a and a radiograph from the time of the injury is shown in Figure 77b. Appropriate management includes which
of the following?
1
Nonsurgical management with the use of a cast-brace
2
Nonsurgical management with skeletal traction
3
Open treatment with a plate with or without strut allograft
4
Revision of the femoral component to a cemented femoral component that bypasses the fracture site by two cortical diameters
5
Revision of the femoral component to a cementless femoral component that bypasses the
fracture site by at least two cortical diameters
The patient has a Vancouver type B1 fracture of the femur with a well-fixed femoral component. When comparing the two radiographs, the proximal femoral component position has not changed and remodeling is seen around the component. Nonsurgical management is associated with the complications of extended recumbency. As the femoral component is well-fixed, revision of the femoral component is not necessary.
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Ricci WM, Bolhofner BR, Lofitus T, et al: Indirect reduction and plate fixation, without grafting, for
periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-2245.
QUESTION 72
An 83-year-old man with a history of diabetes mellitus reports abdominal pain on postoperative day number three following a total hip arthroplasty. The patient reports having a bowel movement the prior evening. Examination reveals that the abdomen is distended but nontender. What is the next step in management?
1
Rectal examination for occult blood
2
Insertion of a nasogastric tube with lavage to identify blood in the gastric contents
3
Radiograph of the abdomen
4
Ultrasound of the abdomen
5
CT of the abdomen
The patient has risk factors, symptoms, and signs of Ogilvie syndrome of acute colonic pseudo-obstruction. This unusual but potentially catastrophic complication is characterized by functional colonic obstruction without an associated mechanical blockage. This disorder has been associated with advanced age, male gender, the use of narcotic pain medications, and patients who have undergone hip arthroplasty. The first step in management of any complication is diagnosis, and the diagnosis is most rapidly made using radiographs that show dilation of the large intestine.
REFERENCES: Nelson JD, Urban JA, Salsbury TL, et al: Acute colonic pseudo-obstruction (Ogilvie syndrome) after arthroplasty in the lower extremity. J Bone Joint Surg Am 2006;88:604-610.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip
arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
QUESTION 73
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
1
Revise the cup bearing to polyethylene
2
Revise the cup bearing to polyethylene and replace the femoral head with a metal design
3
Increase the cup abduction angle
4
Decrease the cup abduction angle
5
Continue routine follow-up and observation
In the absence of component malpositioning, hip pain, or other compelling reasons to reoperate, a squeaking ceramic bearing is not an indication for revision surgery. The patient can be reassured and observed.
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.
Figure 80a Figure 80b
QUESTION 74
A healthy 74-year-old man reports right knee pain and swelling 6 years after undergoing primary total knee arthroplasty. Radiographs are shown in Figures 80a and 80b. He states he had severe bilateral bowlegged deformity for the last 20 years, but the right side got “a little better after the knee arthroplasty.” The infection work-up is negative, and a review of a bone scan and serial radiographs reveals no signs of component loosening. Lateral ligaments appear lax on examination. Optimal surgical management should consist of which of the following?
1
Tibial polyethylene exchange
2
Tibial polyethylene exchange and lateral collateral ligament reconstruction and medial collateral ligament release
3
Revision of all components and soft-tissue balancing
4
Isolated tibial revision
5
Femoral revision and tibial polyethylene exchange
The prosthesis has failed 6 years after implantation. In this patient, the tibial component is in 5 degrees of varus, so the varus mechanical axis was never restored to neutral. The polyethylene bearing is significantly narrowed medially, a sign of incomplete release of the tight medial structures and residual varus angulation of the limb. A polyethylene exchange alone will not correct the varus malalignment of the tibia, nor will a femoral revision with polyethylene exchange. An isolated tibial revision will correct the varus but will probably render the posterior cruciate ligament incompetent, necessitating a femoral revision to a posterior cruciate-substituting design. The procedure most likely to result in a successful outcome is a full revision. Soft-tissue releases to balance the medial and lateral sides also are required.
REFERENCES: Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott- Raven, 1999, pp 137-250.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
1. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
QUESTION 75
Which of the following organisms is most often found in a late (> 3 months) infection of a total hip arthroplasty?
1
Staphylococcus aureus
2
Staphylococcus epidermidis
3
Group B streptococcus
4
Eschericia coli
5
Streptococcus viridans
Staphylococcus epidermidis is the most common organism found in an infected total hip arthroplasty greater than 3 months from the origional surgery. Staphylococcus aureus is more common in acute postoperative infections, and E. coli is associated with infections of the urinary tract. Streptococcus species are less common.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL American Academy of Orthopedic Surgeons, 2006, pp 475-503.
Figure 82
QUESTION 76
A patient sustained a periprosthetic femoral fracture. The proximal femur is comminuted and the femoral component is loose. The patient has absent pulses and poor capillary refill. An emergent arteriogram is shown in Figure 82. What is the most appropriate management?
1
Open reduction and internal fixation of the fracture
2
Traction, followed by revision total hip arthroplasty and vascular repair
3
Revision total hip arthroplasty, four compartment fasciotomy, and sequential neurovascular examination
4
Revision total hip arthroplasty, followed by vascular repair
5
Traction, followed by vascular shunting, revision total hip arthroplasty, and definitive vascular repair
The patient requires emergent revascularization with signs of ischemia of unknown duration. The leg has shortened substantially and initial management requires traction to return the leg to length. This should be followed by revascularization of the leg. A temporary shunt may be helpful until the fracture has been stabilized (revision total hip arthroplasty) with the leg at full length. Definitive vascular bypass should then be performed.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215- 220. Question 83
During normal human knee flexion (beginning with the knee fully extended), which of the following statements best describes tibial rotation with respect to the femur?
1. Rotation is constantly occurring in both directions during the flexion cycle.
2. The tibia initially externally rotates, then progressively internally rotates.
3. The tibia initially internally rotates, then progressively externally rotates.
4. The tibia initially internally rotates, then remains in that rotational position until deep flexion when further internal rotation occurs.
5. The tibia initially externally rotates, then remains in that rotational position until deep flexion when further external rotation occurs.
PREFERRED RESPONSE: 4
DISCUSSION: During knee flexion, the tibia initially rotates internally in approximately the first 20 degrees and generally maintains this rotational position until flexion past 90 degrees when significantly more internal rotation occurs.
REFERENCE: Coughlin KM, Incavo SJ, Churchill DL, et al: Tibial axis and patellar position relative to the femoral epicondylar axis during squatting. J Arthroplasty 2003;18:1048-1055.
QUESTION 77
The anterior approach to the hip (iliofemoral or Smith-Peterson) puts which of the following anatomic structures at greatest risk?
1
Femoral artery
2
Femoral nerve
3
Lateral femoral cutaneous nerve
4
Medial femoral circumflex artery
5
Obturator artery
The anterior approach to the hip involves a dissection between the sartorius and the tensor fascia lata (TFL) superficially, followed by a deep dissection between the rectus femoris and gluteus medius. The lateral femoral cutaneous nerve generally enters the top of the thigh overlying the sartorius, and then usually crosses the interval between the sartorius muscle and the tensor fascia lata more distally. As the fascia between the sartorius and the TFL is incised, the nerve is at risk. The ascending branch of the lateral femoral circumflex artery is also at risk during this approach. The femoral nerve should not be in the plane of dissection as it lies medial to the sartorius.
REFERENCE: Hoppenfeld S, DeBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippinocott, 1984, pp 301-315.
QUESTION 78
Which of the following polyethylene manufacturing processes is expected to generate the greatest degree of polyethylene oxidation?
1
Sterilization with ethylene oxide
2
Sterilization with gamma radiation in a vacuum condition
3
Sterilization with gamma radiation in air
4
Sterilization with gamma radiation in oxygen-free gasses
5
Cross-linking the polyethylene followed by melting
Oxidation of polyethylene has been associated with increased rates of polyethylene wear. Oxidation occurs after polyethylene has been irradiated in the presence of oxygen. Gamma irradiation has been commonly employed to sterilize the polyethylene prior to sterile packaging. Over the last decade, several methods of reducing oxidation of polyethylene have been used. These include irradiation in an inert gas (such as argon or nitrogen), irradiation in vacuum packaging, and avoiding irradiation altogether and sterilizing the polyethylene with ethylene oxide, gas plasma, or vaporized hydrogen peroxide. Crosslinking polyethylene has been done with gamma irradiation and electron beam irradiation. Heating/ melting the material after irradiation allows the free radical chains within the polyethylene to cross-link together rather than oxidize.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 333-344.
QUESTION 79
When compared to total hip arthroplasty, hip resurfacing offers which of the following advantages?
1
Better patient compliance with precautions
2
Increased patient activity in sports
3
Increased mobility of the hip
4
Improved pain relief
5
Preservation of proximal femoral bone
When compared to the outcomes of conventional hip arthroplasty with large diameter femoral heads, hip resurfacing does not result in better outcomes in terms of compliance with hip precautions, increased hip mobility, pain relief, or improved patient activity. The advantage of hip resurfacing is in preserving proximal femoral bone stock that may be advantageous in revision surgery, should that become necessary.
REFERENCES: Schmalzried TP: Why total hip resurfacing. J Arthroplasty 2007;22:57-60. Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Figure 87a Figure 87b
QUESTION 80
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?
1
Surgical traction for 6 weeks followed by application of a cast brace
2
Application of a femoral cable plate
3
Femoral revision with a cemented long stem prosthesis
4
Application of cerclage wired double allograft femoral struts
5
Femoral revision with a cementless long taper fluted modular stem and proximal allograft strut supplementation
Severe periprosthetic fractures after total hip arthroplasty with a loose implant and progressive bone loss are difficult problems for orthopaedic surgeons, with a high complication rate. Recent literature favors the use of long fluted tapered stems that have a long distal taper that may optimally engage the remaining femoral shaft isthmus. Plating options are problematic because the ability to use screws with the plate is limited by the intramedullary stem. Although not the only solution to this problem (such as allograft-prosthetic composites, impaction grafting, tumor prostheses), long distally fixed stems circumvent this problem by enhancing fracture healing and create a long-term prosthetic solution in these most difficult cases.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Figure 88a Figure 88b
QUESTION 81
A 45-year-old man underwent a femoral varus intertrochanteric osteotomy at age 19 years for Perthes disease. He now reports intractable left hip pain, is unable to ambulate more than _Vi_ block, and has pain on stairs. Adjunct nonsurgical management, such as nonsteroidal anti-inflammatory drugs and physical therapy, has failed to provide relief. Radiographs shown in Figures 88a and 88b reveal end-stage degenerative joint disease. What is the most appropriate management of the proximal femoral deformity?
1
Femoral osteotomy with realignment of the femoral canal to accommodate a cementless prosthesis
2
Custom prosthesis that will accommodate the prior osteotomy deformity
3
Hip arthrodesis
4
Cemented femoral component without femoral osteotomy
5
Valgus femoral osteotomy
Whereas the choice of a particular option may seem controversial in this scenario because all
answers seem possible, the literature favors a femoral osteotomy of the femoral canal with a cementless prosthesis that offers some form of distal fixation. Such implants are widely available and allow for healing of the reconstructive osteotomy. Custom implants are problematic because bone assessing algorithms may not be accurate with the dysplastic hip. Hip arthrodesis is not a good option in this age group because ipsilateral spine and knee arthritis can be aggravated. Finally, cemented femoral stem placement has given way to cementless prosthetics in younger patients because the results of cement in osteotomy cases are inferior.
REFERENCES: Parsch D, Jung AW, Thomsen M, et al: Good survival of uncemented tapered stems for failed intertrochanteric osteotomy: A mean 16 years followup study in 45 patients. Arch Orthop Trauma Surg 2007;128:1081-1085.
Suzuki K, Kawachi S, Matsubara M, et al: Cementless total hip replacement after previous intertrochanteric valgus osteotomy for advanced osteoarthritis. J Bone Joint Surg Br 2007;89:1155-1157. Zadeh HG, Hua J, Walker PS, et al: Uncemented total hip arthroplasty with subtrochanteric derotational osteotomy for severe femoral anteversion. J Arthroplasty 1999;14:682-688.
QUESTION 82
Which of the following has been associated with an increased likelihood of stress shielding after cementless total hip arthroplasty?
1
Use of titanium alloy femoral components
2
Use of proximally fixed femoral components
3
Use of distally fixed femoral components
4
Use of press-fit stems in patients with narrow intramedullary canals
5
Use of plasma sprayed components
Although stress shielding has not been associated with adverse clinical outcomes to date, it is a commonly observed process after cementless total hip arthroplasty. Factors that increase the magnitude of stress shielding include the use of distally fixed cobalt-chrome stems, particularly in patients with osteoporosis. Large diameter femoral components (larger than 18 mm in diameter) have also been associated with an increased prevalence of stress shielding.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 83
During total hip arthroplasty, neurologic injury most commonly occurs in which of the following structures?
1
Inferior gluteal nerve
2
Obturator nerve
3
Peroneal branch of the sciatic nerve
4
Tibial branch of the sciatic nerve
5
Femoral nerve
The incidence of nerve injury with total hip arthroplasty is approximately 1%. The sciatic nerve is involved roughly 80% of the time, with the peroneal branch being almost always involved. Isolated tibial branch involvement is reported to occur in only 1% of neurologic injuries related to hip arthroplasty. The superior gluteal nerve may be injured in direct lateral approaches.
REFERENCES: Barrack RL: Neurovascular injury: Avoiding catastrophe. J Arthroplasty 2004; 19:104107. Lewallen DG: Neurovascular injury associated with hip arthroplasty. Instr Course Lect 1998;47:275-283. Schmalzried TP, Noordin S, Amstutz HC: Update on nerve palsy associated with total hip replacement. Clin Orthop Relat Res 1997;344:188-206.
Figure 91a Figure 91b
QUESTION 84
A 71-year-old man underwent an uncomplicated hybrid ceramic-on-conventional polyethylene hip arthroplasty 8 years ago. He now has minimal hip symptoms, but radiographs show massive acetabular osteolysis. An AP pelvis radiograph is shown in Figure 91a and a sagittal CT scan is shown in Figure 91b. What is the most appropriate treatment?
1
Symptomatic treatment with analgesics and a follow-up radiograph in 2 years
2
Revision of the acetabular component and exchange of the ceramic head
3
Revision of both the acetabular and femoral components
4
Revision of the acetabular liner, bone grafting, and exchange of the femoral head to metal
5
Revision of the acetabulum and exchange of the femoral head to metal
The patient has massive osteolysis for which surgery is indicated. Follow-up in 2 years risks further progression of osteolysis and the potential for catastrophic failure. The acetabular component appears well-fixed (CT scan shows a pillar of bone extending down to the dome of the acetabulum) and well positioned and removal should be avoided because the resulting defect may be extremely large and difficult to reconstruct. A liner exchange is favored, provided that the cup is well positioned and of sufficient size to accept a new liner with adequate thickness. In this case, bone grafting behind the socket (without destabilizing it) would be indicated, although routine bone grafting of osteolytic defects is controversial. Revising a ceramic head to a new ceramic head should also be avoided because ceramic head fractures have occurred with placement on a used taper. Metal adapter sleeves are available for some implants if a ceramic head is desired.
REFERENCES: Barrack RL, Burak C, Skinner HB: Concerns about ceramic in THA. Clin Orthop Relat Res 2004;429:73-79.
Lombardi AV Jr, Berend ICR: Isolated acetabular liner exchange. J Am Acad Orthop Surg 2008; 16:243248. Naudie DD, Engh CA Sr: Surgical management of polyethylene wear and pelvic osteolysis with modular
uncemented acetabular components. J Arthroplasty 2004; 19; 124-129.
QUESTION 85
Advantages of a resurfacing metal-on-metal hip arthroplasty over a large diameter metal-on-metal total hip arthroplasty include which of the following?
1
Lower risk of femoral component loosening
2
Acetabular bone preservation
3
Lower reoperation rate
4
Femoral bone preservation
5
Lower wear rate
A resurfacing hip arthroplasty preserves bone stock in the proximal femur, at the expense of a higher reoperation rate because of component loosening and femoral neck fracture. Wear rate is the same as both types of hip arthroplasty use a large head metal-on-metal bearing surface.
REFERENCES: Shimmin A, Beaule PE, Campbell P: Metal-on-metal hip resurfacing arthroplasty. J Bone Joint Surg Am 2008;90:637-654.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65.
QUESTION 86
Patients with fulminant disseminated intravascular coagulation (DIC) have which of the following findings?
1
Patients frequently have elevated fibrinogen levels.
2
Patients frequently have decreased D-Dimer levels.
3
Rapid infusion of IV heparin is generally curative.
4
Prothrombin time (PT) is usually normal.
5
Activated partial thromboplastin time (aPTT) is frequently elevated.
Disseminated intravascular coagulation is a syndrome that spans a spectrum from relatively asymptomatic to life-threatening. In its fulminant form, patients undergo widespread microvascular thrombosis leading to overconsumption of coagulation factors and platelets, and then subsequent hemorrhage. End-organ failure frequently results. The condition is therefore a “thrombohemorrhagic” disorder. The exact pathophysiology remains poorly understood, but can be seen in conjunction with a variety of medical conditions, including massive transfusions, sepsis, bums, crush injuries, liver disease, autoimmune disorders, hemolysis, obstetrical emergencies, and malignancy. Laboratory abnormalities frequently include depressed levels of fibrinogen and platelets, increased levels of fibrinogen degradation products and D-Dimer, and an elevation in the PT and aPTT. In fulminant DIC, treatment is controversial and frequently unsuccessful, leading to death in affected patients. Heparin, although commonly used, has not been shown to have beneficial effects in controlled trials. Low-grade DIC will frequently improve with correction of the underlying medical disorder.
_AL-Madena Copy_
REFERENCE: Townsend CM, Beauchamp RD, Evers BM, et al (eds): Sabiston Textbook of Surgery: The Biologic Basis of Modern Surgical Practice, ed 18. Philadelphia, PA, Saunders Elsevier, 2008, pp 122123.
Figure 94
QUESTION 87
Figure 94 shows the lateral radiograph of an 80-year-old woman who is an independent ambulator and has a supracondylar periprosthetic fracture around the knee. What is the most appropriate management for this patient?
1
Closed reduction and nonsurgical management
2
Open reduction and internal fixation using a distal femoral locking plate
3
Open reduction and internal fixation using an intramedullary rod
4
Revision total arthroplasty using distal femoral allograft
5
Revision total knee arthroplasty using distal femoral replacement
A supracondylar femoral periprosthetic fracture that is a reducible or an irreducible fracture with poor distal bone stock and in the vicinity of loose or malpositioned components (type III) is very difficult to treat. One of the treatment options for patients with a loose femoral component and poor bone stock is the use of distal femoral replacement. The distal femoral replacement can be performed with relative ease, expediency, and is best suited for elderly or sedentary patients.
REFERENCES: Kassab M, Zalzal P, Azores GM, et al: Management of periprosthetic femoral fractures after total knee arthroplasty using a distal femoral allograft. J Arthroplasty 2004;19:361-368.
Kim KI, Egol KA, Hozack WJ, et al: Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res
2006;446:167-175.
QUESTION 88
Effective management of heterotopic ossification (HO) following total hip arthroplasty should include which of the following?
1
Indomethacin treatment for 10 days postoperatively
2
Immediate excision of established heterotopic ossification followed by radiation therapy or indomethacin
3
Postoperative administration of ethylhydroxydiphosphonate
4
Preoperative administration of radiation therapy 1 week before surgery
5
Postoperative administration of radiation therapy
Postoperative administration of ethylhydroxydiphosphonate results in delay of mineralization of osteoid, but ultimately HO formation is not decreased. In addition, the delay in mineralization does not improve range of motion of involved hips. Indomethacin has proven to be an effective long-term therapy. To be most effective, radiation therapy must be done in the immediate postoperative period.
REFERENCES: Iorio R, Healy WL: Heterotopic ossification after hip and knee arthroplasty: Risk factors, prevention, and treatment. J Am Acad Orthop Surg 2002;10:409-416.
Pellegrini VD Jr, Gregoritch SJ: Preoperative irradiation for prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Pellegrini VD Jr, Konski AA, Gastel JA, et al: Prevention of heterotopic ossification with irradiation after total hip
arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
QUESTION 89
Computer navigation in total knee arthroplasty (TKA) has demonstrated which of the following?
1
Decreased cost
2
Improved clinical outcomes
3
Fewer outliers in terms of component position
4
Improved longevity
5
Decreased surgical time
Computer navigation has been shown to improve the accuracy of placement of TKA components with fewer outliers. However, the surgical time and cost are increased. No studies to date have demonstrated improved clinical outcomes or implant survivorship.
REFERENCE: Haaker RG, Stockheim M, Kamp M, et al: Computer-assisted navigation increases precision of component placement in total knee arthroplasty. Clin Orthop Relat Res 2005;433:152-159.
_AL-Madena Copy_
QUESTION 90
Which of the following statements best describes the kinematic behavior of the knee during motion from full extension to flexion?
1
Both the medial and lateral knee tibiofemoral contact points rotate and translate equally with increasing knee flexion.
2
The medial femoral condyle translates much less than the lateral femoral condyle with knee flexion.
3
The lateral femoral condyle translates much less than the medial femoral condyle with knee flexion.
4
The medial compartment rotates internally whereas the lateral compartment rotates externally.
5
The lateral compartment rotates internally whereas the medial compartment rotates externally.
During normal knee flexion, knee kinematic analysis reveals that the medial tibiofemoral contact point moves very little (translates) in the anterior-posterior direction, whereas the lateral contact point moves much
greater in the anterior-posterior direction (translates), resulting in more lateral translation, rollback, and medial pivoting.
REFERENCE: Churchill DL, Incavo SJ, Johnson CC, et al: The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res 1998;356:111-118.
Figure 98a Figure 98b Figure 98c Question 98
A 71-year-old businessman reports medial knee pain recalcitrant to nonsurgical management.
Examination reveals that his body mass index (BMI) is 28 and he has a mild varus deformity with a range of
motion from 5 degrees to 130 degrees of flexion. Anterior drawer and Lachman’s test are negative. Radiographs are shown in Figures 98a through 98c. For cultural and religious reasons, he is concerned about maintaining his range of motion and kneeling ability. Which of the following options is best?
1. High tibial osteotomy
2. Unicompartmental knee arthroplasty
3. Cruciate-retaining total knee arthroplasty with a fixed bearing design
4. Posterior stabilized total knee arthroplasty with a fixed bearing design
5. Cruciate-sacrificing total knee arthroplasty with a rotating platform design PREFERRED RESPONSE: 2
DISCUSSION: Unicompartmental arthroplasty of the knee is associated with better range of motion than either total knee arthroplasty or high tibial osteotomy. In a prospective randomized trial of unicompartmental and total knee arthroplasty for patients with medial compartment osteoarthritis, patients with the unicompartmental prosthesis had better range of motion. The literature that compares range of motion in cruciate-retaining as opposed to posterior stabilized and fixed bearing as opposed to mobile- bearing total knees suggests relatively equivalent range of motion between these designs.
REFERENCES: Newman JH, Ackroyd CE, Shah NE: Unicompartmental or total knee replacement? Five- year results of a prospective randomized trial of 102 osteoarthritic knees with unicompartmental arthritis.
J Bone Joint Surg Br 1998;80:862-865.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 59-69.
QUESTION 91
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
1
Proceed with implantation of the final components.
2
Perform a Z-lengthening of the patellar tendon.
3
Increase the size of the femoral component and use posterior femoral augments to decrease the size of the flexion gap.
4
Increase the size of the femoral component and use augments both distally and posteriorly to lower the joint line and decrease the size of the flexion gap.
5
Place distal femoral augments on the femoral component to lower the joint line.
The surgeon in this case is faced with a common scenario at the time of revision total knee arthroplasty and the tendency is to elevate the joint line. Elevation of the joint line is associated with deleterious effects including anterior knee pain, restricted knee flexion, and instability. The error that has been made is resting the femoral component on the bone that is left behind after removal of the prior component; this typically leads to a femoral component that is too small (leading to an enlarged flexion gap) and proximal to where it should be (enlarging the extension gap). Although the flexion and extension gaps are equivalent, joint line elevation has occurred. To correct this problem, the femoral component size should be increased or offset posteriorly (to decrease the size of the flexion gap) and distal femoral augments should be used to decrease the size of the extension gap and restore the joint line to the appropriate level.
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
1. Placement of a cerclage cable around the femoral neck above the lesser trochanter
_AL-Madena Copy_
2. Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
3. Removal of the press-fit implant and cementing of the same femoral stem
4. Final seating of the cementless femoral component without additional measures
5. Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
PREFERRED RESPONSE: 2
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
_Your Source for Lifelong Orthopaedic Learning_
QUESTION 92
What is the most common maxillofacial/dental injury in ice hockey?
1
Temporomandibular
2
Lip laceration
3
Tooth avulsion
4
Crown fracture
5
Mandible fracture
Lahti and associates reported that the most common dental injury in a study of 479 injured ice hockey players was a noncomplicated crown fracture, which accounted for 43.5% of all maxillofacial/ dental injuries. The most common cause of injury was a blow from an ice hockey stick. As a cause of injury, the stick was approximately three times as common in games as in training, and only 10% of injured players wore some sort of protective guard. A tooth avulsion is a partial or complete
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
REFERENCES: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.