Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 2
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
Polyethylene wear debris can result in significant synovitis and subsequent cloudy appearing synovial fluid. Typically, laboratory studies show a WBC of less than 30,000/mm3 no left shift. Cytologic examination can reveal intra-articular polyethylene particles. Infected total knee arthroplasty is extremely uncommon in a healthy, immune-competent patient who has a normal preoperative erythrocyte sedimentation rate and C-reactive protein level.
Question 3
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner's syndrome?

Explanation
The sympathetic chain approaches the lateral border of the longus coli muscle at C6 and is more vulnerable to injury at this level. Injury to the chain will cause Horner's syndrome, usually seen as unilateral ptosis.
Question 4
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient's diagnosis?



Explanation
The more severe the trauma, the higher the rate of subsequent clavicular nonunion. Neither duration nor type of immobilization has been clearly demonstrated to be a causative factor in the development of nonunion. Similarly, closed reduction has not been found to alter the healing course in midshaft clavicular fractures. Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
Question 5
High Yield
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
The CT scan is an important test to help determine the extent of involvement of the talocalcaneal facet in a talocalcaneal coalition. In a young patient with no arthritis and joint involvement of less than 50%, resection of the coalition and fat pad interposition has been shown to be successful. A calcaneal osteotomy does not address the coalition. Subtalar arthroereisis has been used for treatment of a flexible flatfoot; tarsal coalition patients have a rigid-type flatfoot deformity. Sullivan JA: The child's foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Question 6
A 52-year-old woman reports nagging shoulder pain that has been present for months and is slowly progressive in nature. The patient also reports nocturnal pain and notes that the pain is not activity related. Figures 27a and 27b show the radiograph and bone scan, and Figures 27c through 27e show T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. Based on these findings, what is the most likely diagnosis?





Explanation
The radiograph reveals a metaphyseal lesion with some stippled mineralization suggesting a chondroid tumor. The bone scan shows increased uptake, beyond what is expected for a simple enchondroma, and beyond the limits of the lesion. The MRI sequences shows a lobular lesion on the T1- and T2-weighted (bright on the T2 sequence) images with inhomogeneous uptake of gadolinium; both findings are typical for a chondroid lesion. The history of pain, the positive bone scan, the age of the patient, the size of the lesion, and the central location (enostotic) of the lesion all suggest a malignant cartilage tumor. The images are not consistent with the other diagnoses. In particular, plasmacytoma is more uniformly bright on T2-weighted images and often has a negative bone scan. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 187-194.
Question 7
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must

Explanation
While it is recommended that a patient gain full range of motion, pain-free function, and symmetric strength prior to returning to vigorous activities, it is absolutely essential that radiographs of the fracture site reveal a circumferential external bridging callus to prevent refracture. This is particularly important for comminuted femoral fractures with various sized fragments. It is also recommended that a return to rodeo riding be postponed for at least 1 year. Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112. Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am 1991;73:1561-1566.
Question 8
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?

Explanation
The sympathetic trunk runs longitudinally along the medial border of the psoas. The ilioinguinal nerve emerges along the upper lateral border of the psoas and travels to the quadratus lumborium, and the genitofemoral nerve lies more laterally on the psoas. The ureter is adherent to the posterior peritoneum and falls away from the psoas and the spine in the dissection, as does the aorta. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Question 9
High Yield
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?

Explanation
Malrotation of the foot is frequently overlooked in this clinical setting. This can be judged by evaluating and comparing the transmalleolar axes of the affected and unaffected legs. The rotation occurs through the physis and frequently is not recognized until the patient has been walking for a few months. The other conditions are not expected to occur in the clinical setting described. Phan VC, Wroten E, Yngve DA: Foot progression angle after distal tibial physeal fractures. J Pediatr Orthop 2002;22:31-35.
Question 10
High Yield
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of


Explanation
The patient has a displaced intra-articular tibial tuberosity fracture; therefore, the treatment of choice is open reduction and internal fixation. Periosteum is often interposed between the fracture fragments and prevents satisfactory closed reduction. Fortunately, most patients with this injury are close to skeletal maturity and therefore, growth arrest and recurvatum are unusual. Nondisplaced fractures can be treated with a cast, but displaced fractures are best treated with open reduction and internal fixation. Intra-articular fractures can disrupt the joint surface and are sometimes associated with a meniscal tear; therefore, arthroscopy may be needed at the time of open reduction and internal fixation. McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
Question 11
A 56-year-old man with a history of chronic lower back pain from lumbar spondylosis reports a 2-day history of acute incapacitating back pain. He denies any history of acute trauma, although he reports the pain starting after a coughing spell. He also reports difficulty urinating and some fecal incontinence. Examination reveals generalized lower extremity weakness, saddle paresthesia, hyporeflexia in the lower extremities, and loss of rectal tone. What is the most appropriate management at this time?

Explanation
Cauda equina syndrome is a medical emergency that must be quickly diagnosed and treated to avoid long-term complications. Cauda equina syndrome typically presents with low back pain, unilateral or usually bilateral sciatica, saddle sensory disturbances, bladder and bowel dysfunction, and variable lower extremity motor and sensory loss. Although a number of pathologies can cause cauda equina syndrome, in a patient with a history of chronic back pain, disk pathology is the most common cause of acute onset cauda equina syndrome. Whereas radiographs may be useful in a traumatic onset of symptoms, MRI is the most appropriate study. Cauda equina syndrome should be evaluated on an emergent basis and admission for work-up is appropriate. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Question 12
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?

Explanation
It is generally accepted that reconstructions of the proximal tibia are associated with the highest incidence of failure, probably because of poor soft-tissue coverage, the need for extensor mechanism reconstruction, and other anatomic issues. It also may be related to the fact that patients with tumors of the proximal tibia, in general, have a better prognosis and better survival rates than patients with tumors located elsewhere in the body. Reconstructions of the proximal humerus may be more durable because they are not involved in weight-bearing activities.
Question 13
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?


Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 14
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
The average location of the anterior portal is 6.3 cm distal to the anterior superior iliac spine. The lateral femoral cutaneous nerve typically has divided into three or more branches at the level of the anterior portal. The portal usually passes within several millimeters of the most medial branch. Injury to the nerve can lead to meralgia paresthetica. The femoral nerve lies an average minimum distance of 3.2 cm from the anterior portal. The ascending branch of the lateral circumflex artery lies approximately 3.7 cm inferior to the anterior portal. Neither the ascending branch of the medial circumflex artery nor the superior gluteal nerve are at risk. Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Question 15
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 16
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
Microvascular studies have shown that the majority of the blood supply to the cruciate ligaments comes from the middle geniculate artery, although there is collateral flow through the other geniculates and from bone. Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Question 17
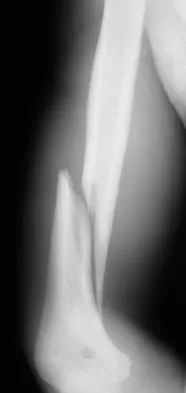
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of


Explanation
Compression plating remains the treatment of choice for most established humeral nonunions. Autograft is felt to be superior to allograft. Electrical stimulation has not been found to improve healing rates in patients with nonunion after intramedullary nailing. Retrograde nailing with flexible nails gives inadequate rotational control to promote healing in this patient. Adding cancellous graft alone will not stabilize the nonunion site. Dynamic locking has been successful only in the lower extremity because the bone can be loaded axially. McKee MD, Miranda MA, Riemer BL, et al: Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492-499.
Question 18
A Canale view best visualizes which of the following structures?

Explanation
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 19
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of

Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 20
Figure 19 shows the current radiograph of a 48-year-old man who reports hip pain and marked difficulty walking after undergoing revision of a failed total hip replacement 2 years ago. What is the mechanism of failure?

Explanation
Fatigue from repetitive loading of the stem with the distal aspect well-fixed resulted in stem failure. If the stem had loosened, it would not have broken. Crevice corrosion occurs at a taper interface; galvanic corrosion occurs at the junction of two metals of differing electrochemical potentials, not along a uniform portion of the implant. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Question 21
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Explanation
Transfer of the flexor digitorum longus tendon is a common technique combined with other procedures to treat patients with posterior tibial tendon insufficiency. However, it is contraindicated in patients with a fixed hindfoot deformity, hypermobility, or neuromuscular compromise. It is relatively contraindicated in patients who are obese, and those older than age 60 to 70 years. Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Question 22
High Yield
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?

Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 23
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?


Explanation
This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear. Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573. Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 24
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Very large corrections of tibial deformity can be achieved at or just below the tibial tubercle. This level of osteotomy maintains the relationship between the tubercle and the rest of the joint, does not alter patellofemoral mechanics, and avoids complicating possible future conversion to total knee arthroplasty. High tibial osteotomy is contraindicated for large corrections because of excessive elevation of the tibial tubercle and overhang of the lateral plateau. Correction in the tibial diaphysis creates a zig zag pattern in the tibia by correcting below the deformity and risks nonunion in cortical bone. There is no evidence that the femur is deformed; therefore, femoral osteotomy is not indicated.
Question 25
High Yield
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
High-level pitchers with symptomatic UCL tears require reconstruction, with autograft being the best studied graft selection. With concomitant ulnar nerve symptoms, a simultaneous ulnar nerve transposition provides good results. Ligament "repairs" and allograft reconstructions have not shown good long-term results. Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Question 26
Fully dense alumina and zirconia materials have been used as bearing materials in hip arthroplasty to provide greater wear resistance than polished metallic surfaces. Although both have shown reduced wear clinically, what concerns continue to exist about the use of zirconia?
Explanation
Zirconia as a bearing surface is "metastable," meaning that, in the microstructure of the material the zirconia molecules are ordered in a tetragonal fashion, but they can easily transform to a monoclinic microstructure that is less wear resistant. Transformation can occur with input of enough energy (eg, thermal energy imparted by steam sterilization or mechanical energy at the bearing surface). Zirconia was introduced as an alternative to alumina because it has a higher toughness, making it less susceptible to gross fracture (ceramics do not undergo fatigue fracture, but rather fail from a process of slow crack growth). Zirconia is highly biocompatible (as are many ceramics) and is essentially immune to corrosive processes that can plague metallic alloys such as stainless steel. Clarke IC, Manaka M, Green DD, et al: Current status of zirconia used in total hip implants. J Bone Joint Surg Am 2003;85:73-84. Haraguchi K, Sugano N, Nishii T, et al: Phase transformation of a zirconia ceramic head after total hip arthroplasty. J Bone Joint Surg Br 2001;83:996-1000.
Question 27
High Yield
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?

Detailed Explanation
The risk of synostosis is imminent with any technique for repairing a distal biceps tendon rupture. However, the risk is quite low for all approaches that avoid exposure of the ulna, including the muscle-splitting two-incision technique.
Question 28
High Yield
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?

Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Question 29
High Yield
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?

Detailed Explanation
The history and physical examination are consistent with a monoarticular joint condition but not typical of joint sepsis. The arthroscopic appearance of brownish proliferative synovium is typical of PVNS. PVNS is a monoarticular synovial disease of unknown etiology and is treated with total synovectomy. The proliferative synovitis is not consistent with chondromalacia. Synovial cell sarcoma is an extracapsular disease. Rheumatoid arthritis typically is polyarticular, and the synovial appearance is not associated with hemosiderin deposition. Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
Question 30
High Yield
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
Explanation
Incomplete cord syndromes have variable neurologic findings with partial loss of sensory and/or motor function below the level of injury. Incomplete cord syndromes include the anterior cord syndrome, the Brown-Séquard syndrome, central cord syndrome, and posterior cord syndrome. Central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness. Anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception. The Brown-Séquard syndrome involves a relatively greater ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. Posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain, and light touch, with loss of proprioception and temperature sensation below the level of the lesion. Spinal shock is the period of time, usually 24 hours, after a spinal injury that is characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury. Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Question 31
High Yield
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?

Explanation
Studies have shown that when compared with fixation to the sacrum alone, the success rate of fusion across the lumbosacral junction increases when both the sacrum and ilium are included in the posterolateral construct. Curve correction, coronal balance, and pelvic balance are all attended to within the thoracolumbar spine and are not directly related to the pelvic fixation. Fretting and corrosion are a byproduct of metal-to-metal connections. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
Question 32
High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of


Explanation
The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Question 33
High Yield
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?



Explanation
Although the degeneration of an isolated benign cartilaginous lesion into a chondrosarcoma is rare, it occurs in roughly 10% of patients with Ollier's disease. Pain is the most common symptom of chondrosarcoma. The treatment of low-grade chondrosarcoma ranges from intralesional excision to wide amputation. The intent of the surgery is to remove all the disease to decrease the chance of local recurrence. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 34
Examination of a 7-year-old girl with myelomeningocele reveals calcaneal deformities of both feet. She ambulates on both extremities wearing ankle-foot orthoses and has no upper extremity aids. She has grade 5/5 motor strength to the tibialis anterior muscles and absent motor strength to the triceps surae. There is no varus or valgus deformity of the hindfoot, and the skin over the heels is intact; however, mild callosities are present. Management should consist of
Explanation
A calcaneal deformity of the foot may occur in children who have low lumbar myelomeningocele. Strong dorsiflexors overcome a weak or absent gastrocnemius-soleus complex, leading to downward growth of the calcaneal apophysis. The deformity is usually progressive and does not respond to nonsurgical management. Most authorities recommend transfer of the tibialis anterior muscle through the interosseous membrane to the posterior aspect of the calcaneus. This procedure has been reported to be effective in limiting progression of the deformity. An extra-articular subtalar arthodesis, a treatment option for valgus deformity of the hindfoot, is not indicated. Similarly, Achilles tendon tenodesis to the fibula, an option for managing valgus of the ankle, is not indicated. Calcaneal osteotomy may be used in older children with severe calcaneal deformity. Stott NS, Zionts LE, Gronley JK, Perry J: Tibialis anterior transfer for calcaneal deformity: A postoperative gait analysis. J Pediatr Orthop 1996;16:792-798.
Question 35
A patient undergoes excision of a 3- x 3-cm soft-tissue sarcoma. The final histology results show tumor at the surgical margin. The surgical procedure performed is classified as
Explanation
Surgical margins are classified according to the plane of dissection in relation to the tumor. An intralesional procedure is where the plane of dissection passes through the tumor. A marginal resection involves a resection where the plane of dissection is through the reactive zone of the tumor. A wide resection is through completely normal tissue outside of the reactive zone. A radical resection removes all of the muscles and/or bone of the compartment that are involved by the tumor.
Question 36
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 37
High Yield
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 38
High Yield
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?

Detailed Explanation
The clinical result in this patient has been good, with no dislocations, suggesting that the components are in reasonably good position. The radiograph and examination at the time of surgery suggest that the acetabular component is well fixed. The surrounding bone of the acetabulum is osteopenic and there would most likely be considerable bone loss if the acetabular component is removed. Access to the osteolytic lesions is possible. Cementing an acetabular component into the retained socket will cause the least amount of bone loss, shorten the procedure, and most likely result in a functional hip. Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Question 39
High Yield
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis?

Detailed Explanation
The photograph shows the characteristic attitude of the hand when an anterior interosseous nerve palsy is present. The patient is unable to flex the interphalangeal joint to the joint of the thumb. Anterior interosseous nerve palsies are often misdiagnosed as tendon ruptures. Schantz K, Reigels-Nielsen P: The anterior interosseous nerve syndrome. J Hand Surg Br 1992;17:510-512.
Question 40
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
Patients with diabetes mellitus should be screened for the presence of protective foot sensation. In the absence of protective foot sensation, patients are at increased risk for the development of neuropathic ulcerations and neuropathic arthropathy. The most reliable screening tool for the presence of protective sensation is the ability to feel the 5.07 Semmes-Weinstein monofilament. Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Question 41
High Yield
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?

Explanation
Synovectomy of the knee prior to loss of articular cartilage has been shown to consistently relieve pain in patients with rheumatoid arthritis. Partial knee replacement will not arrest the process of joint destruction. Osteotomy of the hip has not been found to be a successful procedure in patients with rheumatoid arthritis. Hip arthrodesis should not be considered because of the multiarticular involvement in patients with rheumatoid arthritis. Core decompression of the hip has not been shown to save the femoral head because the necrosis appears to occur simultaneously with the inflammatory joint process. Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Question 42
High Yield
What is the most common reason for reoperation in total knee arthroplasty?

Detailed Explanation
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 43
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 44
High Yield
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
The MRI scan reveals a full-thickness rotator cuff tear with retraction and increased signal in the subacromial space indicating joint fluid. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 45
High Yield
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?

Explanation
The motorized shaver is adjacent to the acetabular labrum, which is torn. The femoral head and acetabulum are normal in appearance. Neither the fat pad nor a loose body is identified.
Question 46
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
The rate of wound complications is significantly increased after total knee arthroplasty in obese patients. Knee scores and the rate of aseptic loosening or patellar subluxation do not appear to be significantly altered. Winiarsky R, Barth P, Lotke P: Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770-1774. Stern SH, Insall JN: Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400-1404.
Question 47
High Yield
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of



Detailed Explanation
The patient has a chronic unrecognized volar lunate dislocation. Median nerve compression is the result of the lunate displaced into the carpal tunnel. The diagnosis can be made by radiographs; MRI is not necessary. A volar approach allows median nerve decompression with excision of the lunate, whereas a dorsal approach facilitates excision of the scaphoid and triquetrum. Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Question 48
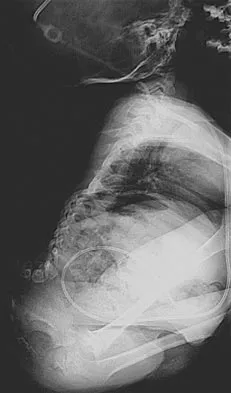
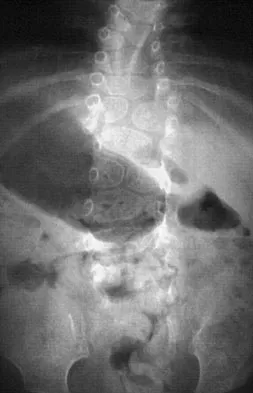
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches


Explanation
Mortality following trauma that requires surgical intervention for head, chest, and abdominal injury exceeds 90%. The type of pelvic fracture is a predictor of associated injury, blood requirements, and overall mortality. AP III pelvic fractures require the most blood, and are associated with significant abdominal trauma and shock. Lateral compression pelvic fractures are more associated with head, chest, and occasionally abdominal trauma, and mortality often occurs from associated injuries. Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000. Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Question 49
High Yield
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 50
High Yield
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
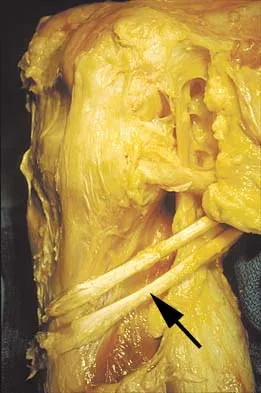
Explanation
The semitendinosus and gracilis tendons lie beneath the superficial fascia and superficial to the medial collateral ligament. The semitendinosus is located more inferior to the gracilis tendon. The sartorius is more posterior and distal as is the medial collateral ligament. The semimembranosus is posterior. Pagnani MJ, Warner JJ, O'Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Question 51
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management?

Explanation
In patients older than age 40 years, a high suspicion of a rotator cuff tear should be kept in those patients with weakness after shoulder dislocation. Both posterior rotator cuff and subscapularis injuries have been documented. The next most appropriate step in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography. Stayner LR, Cumming J, Andersen J, et al: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239.
Question 52
High Yield
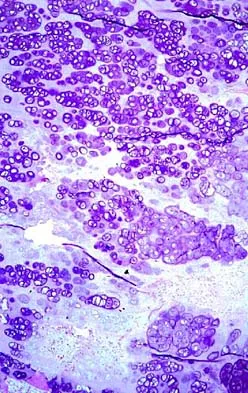
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?





Detailed Explanation
The pathology demonstrates a very cellular chondroid matrix with multinucleated forms, atypia, and myxomatous regions. This is most consistent with a myxoid chondrosarcoma. The radiograph shows a well-circumscribed lesion in the superior and medial aspect of the right acetabulum. The CT and MRI scans confirm these same findings with no evidence of matrix mineralization or significant surrounding edema. Unfortunately, in this location with this appearance, the radiographic differential diagnosis includes all the diagnoses listed. Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14. Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Question 53
High Yield
A 24-year-old man who works at a local oyster and clam farm sustained a laceration on his hand at work. Examination reveals a cellulitic index finger without evidence of tenosynovitis. After appropriate irrigation and debridement, what antibiotic is most appropriate?
Explanation
Injuries involving brackish water and shellfish can have devastating consequences caused by Vibrio vulnificus infections. Patients may have a severe invasive infection, with three main clinical features: primary septicemia, wound infection, and gastroenteritis. Antibiotic administration is crucial because mortality rates of up to 50% have been observed with Vibrio septicemia. The current recommendation is to give a third-generation cephalosporin such as ceftazadime. Chiang SR, Chuang YC: Vibrio vulnificus infection: Clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 2003;36:81-88.
Question 54
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of

Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 55
High Yield
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
During osteolysis, IL-6 is secreted by fibroblasts in the membrane surrounding the prosthesis. IL-6 also can be secreted by osteoblasts in other settings, but they are not the predominant source of IL-6 in particle-induced osteolysis. The remaining cells are not major sources of IL-6.
Question 56
High Yield
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?


Explanation
The deformity is long-standing, the hindfoot is immobile, and the radiographs reveal severe degenerative arthritis involving the entire hindfoot, severe deformity, and talonavicular dislocation. The "exostosis" responsible for the callus is the talar head; resection would severely destabilize the foot. Degenerative arthritis and fixed deformity preclude lateral column lengthening, medial slide calcaneal osteotomy, and talonavicular arthrodesis. Triple arthrodesis is the only viable option. Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Question 57
High Yield
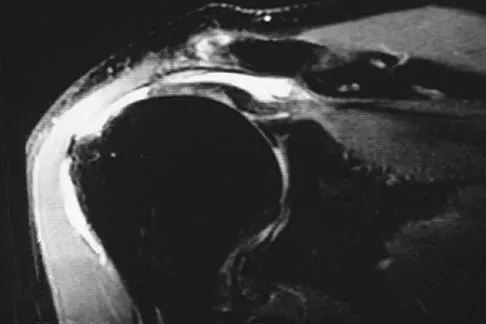
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of

Detailed Explanation
The MRI scan shows a massive tear of the supraspinatus tendon with medial retraction to the level of the glenoid. This is most likely an attritional tear with a high risk of failure of the repair. The preferred treatment is nonsurgical management for pain and stiffness. Acromioplasty and coracoacromial ligament release in this setting are controversial, as they can result in the devastating complication of anterosuperior subluxation of the humerus. Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Question 58
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?

Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 59
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
Cotler and associates reported on the use of awake skeletal traction to reduce facet fracture-dislocations in 24 patients. Seventeen patients required more than 50 pounds of traction (the "traditional" limit) to achieve reduction. More than 100 pounds of traction was safely used in one-third of the patients in this study. A cadaver study has supported the safe use of traction with weights in excess of 100 pounds. Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 60
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 61
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
The patient has sustained a low-velocity, low-caliber gunshot wound to the foot. Because the injury occurred within a period of 8 hours, this is classified as a type I wound. Several studies support the use of surface debridement, cleansing, and sterile dressings as the treatment of choice. More aggressive measures are reserved for high-velocity injuries and shotgun injuries. Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31. Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Question 62
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of


Explanation
Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 63
High Yield
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 64
High Yield
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of


Detailed Explanation
The patient has a stress fracture of the olecranon; therefore, the most appropriate management is modification of activities below the threshold of symptoms to allow for healing. Ultrasound provides no benefit, and immobilization is not necessary. MRI is not necessary because there is no associated ligamentous injury. Arthroscopy is not indicated. Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Question 65
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?



Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 66
High Yield
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene's molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first 5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of 3 to 5 years has a direct effect on wear of polyethylene. Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122. Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
Question 67
High Yield
Mutations of what gene are associated with the subsequent development of osteosarcoma?
Explanation
Patients with a mutation of the retinoblastoma gene (RB) have an increased likelihood for the development of osteosarcoma. The EWS-FLI1 gene is the fusion product of a chromosomal translocation of 11:22. EGF-R and IGF-R are growth factor receptors, but mutations in these genes have not been correlated with osteosarcoma. VEGF is a proangiogenic molecule that is involved in tumor formation in multiple sites but not the development of osteosarcoma. Scholz RB, Kabisch H, Delling G, et al: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;7:265-273.
Question 68
High Yield
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Urbaniak and Harvey reported donor site morbidity following free vascularized fibular graft in 198 consecutive patients. At a 5-year follow-up, they reported overall complications in 24% of the patients. The most common complication was a sensory deficit (11.8%), followed by motor weakness (2.7%), flexor hallucis longus contracture (2%), and deep venous thrombosis (less than 1%).
Question 69
High Yield
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?

Explanation
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal. Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Question 70
High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of


Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 71
High Yield
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
There is a spectrum of heat-related conditions. Heat cramps are the mildest form of heat illness. In heat exhaustion, cramps are associated with headache and weakness, and the skin is pale and moist. Treatment of heat cramps or heat exhaustion consists of removing and loosening excess clothing, applying ice to the axilla and groin, ingestion of cool water, and cool water sprays. This patient demonstrates symptoms of heat stroke which is a medical emergency. The core body temperature may be as high as 106 to 110 degrees F (41.1 to 43.3 degrees C). In heat stroke, the patient may no longer be sweating, and the skin may be hot and red. The athlete is usually confused, weak, nauseated, and may have seizure activity. Central nervous system depression has been called the most important marker of heat stroke, and progresses from confusion and bizarre behavior to collapse, delirium, and coma. Bizarre behavior is often the first sign of heat stroke. The patient needs to be treated and moved to a medical facility rapidly. During transfer, IV fluids and cooling of the athlete should be initiated. The best treatment of heat-related illness appears to be prevention with adequate hydration and monitoring of conditions (temperature and humidity), with cancellation of competition when conditions do not comply with guidelines. Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902. Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Question 72
High Yield
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?

Explanation
Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 73
High Yield
An otherwise healthy 65-year-old man reports thigh pain of insidious onset. He states that the pain is increased with weight bearing and also occurs at night. He denies any history of cancer. Radiographs are shown in Figures 22a and 22b. A bone scan shows an isolated lesion. CT scans of the chest and abdominal are negative for any other lesions. Initial management should consist of


Explanation
The patient has a solitary lesion that is at high risk for fracture. While metastatic lesions are most common in this age group, a stabilization procedure is contraindicated until results of a biopsy confirm the presence of a metastasis. Because of the lytic lesion and the associated calcification shown on the radiograph, the most likely diagnosis is a chondrosarcoma. Therefore, any type of stabilization procedure with a rod or plate would compromise a wide surgical excision to remove the entire proximal femur. Radiation therapy and chemotherapy are also contraindicated until biopsy results are obtained. Because of these factors, obtaining a frozen section biopsy specimen is considered the next most appropriate step in management. If a metastatic lesion is confirmed on the frozen section, a stabilization procedure could then be performed under the same anesthetic. Therefore, it is important to have a pathologist available at the time of a biopsy. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 74
High Yield
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of

Detailed Explanation
Dislocation of the long head of the biceps tendon is the result of a defect in the region of the rotator cuff interval, coracohumeral ligament-superior glenohumeral ligament pulley, or an associated tear of the medial insertion of the subscapularis tendon. In the case of an intra-articular dislocation of the long head of the biceps tendon associated with a tear of the subscapularis tendon, stabilization of the biceps tendon is difficult in this situation; therefore, biceps release or tenodesis and repair of the subscapularis tendon is the treatment of choice. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Question 75
Which of the following findings best describes the effects of increasing conformity of a fixed tibial bearing component and femoral component in total knee arthroplasty?
Explanation
In the design of tibial and femoral components, a compromise must be made between contact stresses and constraint. Increased conformity increases constraint, limits motion, and potentially increases stress on the knee-cement interface. By increasing conformity, the surface area over which force is applied is increased, resulting in decreased peak contact stresses and decreased component wear rates. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 76
High Yield
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of

Explanation
Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 77
High Yield
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?

Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Question 78
Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?

Explanation
The first step in the treatment of an amputation residual limb (stump) ulcer is local wound care and adjustment of the residual limb-prosthetic interface, as well as adjusting prosthetic alignment. Surgical revision should be undertaken only when prosthetic modification is unsuccessful. Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.
Question 79
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 80
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 81
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?


Explanation
The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Question 82
High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 83
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Explanation
Lonner and associates conducted a prospective study to determine the reliability of analysis of intraoperative frozen sections for the identification of infection during 175 consecutive revision total joint arthroplasties (142 hips and 33 knees). The mean interval between the primary arthroplasty and the revision arthroplasty was 7.3 years (range, 3 months to 23 years). Of the 175 patients, 23 had at least 5 polymorphonuclear leukocytes per high-powered field on analysis of the frozen sections and were considered to have an infection. Of these 23 patients, five had 5 to 9 polymorphonuclear leukocytes per high-powered field and 18 had at least 10 polymorphonuclear leukocytes per high-powered field. The frozen sections for the remaining 152 patients were considered negative. On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field. The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection. Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813. Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558. Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Question 84
High Yield
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of

Explanation
The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites. Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Question 85
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?

Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 86
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?

Explanation
Serum lactate levels can be used to evaluate the effectiveness of the resuscitation of patients who have multiple injuries. Even after resuscitation, patients may have occult hypoperfusion as defined by a serum lactate level of greater than 2.5 mmol/L. The studies referenced indicate that these patients are at increased risk of perioperative complications such as organ failure or adult respiratory distress syndrome if definitive surgical fixation of the orthopaedic injuries is pursued prior to correction of the occult hypoperfusion. The other markers may be an indication of current physiology but have not been correlated with perioperative risks. Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977. Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Question 87
High Yield
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
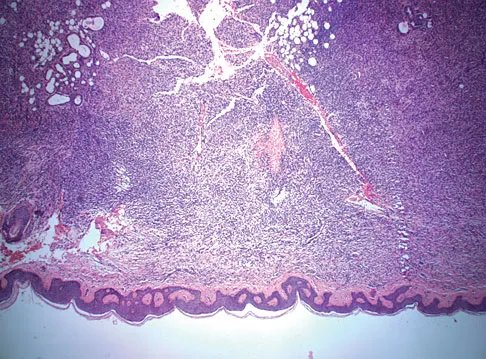
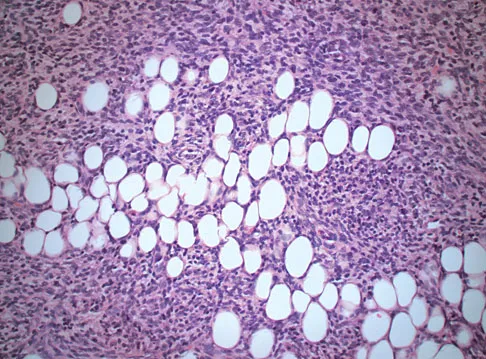
Explanation
Dermatofibrosarcoma protuberans (DFSP) is a rare superficial sarcoma that is frequently misdiagnosed at presentation. It is frequently excised prior to suspecting that the lesion is a sarcoma and if not appropriately treated with tumor bed resection to obtain wide margins, these lesions have a high incidence of local recurrence. It is recommended that the wide excision include the deep fascia and a 2.5- to 3-cm cuff of normal-appearing skin. Distant disease spread is rare and usually occurs in the face of a multiply recurrent lesion. Despite the apparent gross circumscription of these lesions, the tumor diffusely infiltrates the dermis and subcutaneous tissues. A characteristic histologic finding can be seen in the deep margins of the tumor where it intricately interdigitates with normal fat. Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol 1999;25:392-397.
Question 88
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?

Explanation
Achilles tendon tension is not affected by knee position when the ankle is in 20 degrees to 25 degrees of plantar flexion. Skin perfusion overlying the Achilles tendon is maximal in 20 degrees of plantar flexion and is reduced beyond 20 degrees of plantar flexion. Neutral flexion or any amount of dorsiflexion compromises the repair.
Question 89
The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has

Explanation
The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube. Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Question 90
High Yield
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?
Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 91
High Yield
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
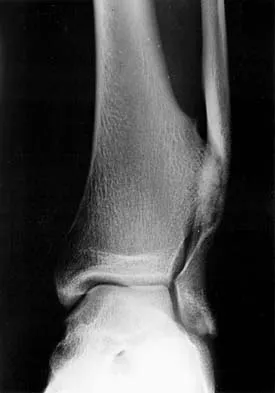
Explanation
For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Question 92
High Yield
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
Glassman and associates reported a significantly higher pseudarthrosis rate when ketorolac was used postoperatively compared to a similar group of patients who were not given ketorolac. Animal studies from the same institution support these clinical findings. To reduce narcotic dosage, nonsteroidal anti-inflammatory drugs (NSAIDs) have been promoted as an adjunct for postoperative analgesia in patients undergoing spinal fusion. However, a high failure rate of arthrodesis has been associated with postoperative use of NSAIDs. The analgesics oxycodone hydrochloride, hydrocodone/acetaminophen, and tramadol, as well as the tricyclic antidepressant imipramine, have not been shown to inhibit fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 93
High Yield
An 18-year-old high school football player sustains a thigh injury that results in the findings shown in Figure 1. Initial management should consist of

Detailed Explanation
The radiograph shows myositis ossificans within the quadriceps muscle. This condition occurs as a complication of muscle injury. Initial treatment should include rest, ice, compression, and elevation. While gentle active range of motion is encouraged in the functional recovery from this injury, passive stretching is contraindicated as it can enhance hemorrhage and accentuate the development of myositis ossificans. Ultrasound is similarly contraindicated because it can enhance the development of myositis ossificans and has no proven efficacy in this patient; electrical stimulation also has no proven benefits. Massage is contraindicated in the initial management of this injury because of its influence on increasing local blood flow. Anderson JE (ed): Grant's Atlas of Anatomy. Baltimore, MD, Williams & Wilkins, 1978, pp 4.39-4.49. Brumet ME, Hontas RB: The thigh, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112. Antao NA: Myositis of the hip in a professional soccer player: A case report. Am J Sports Med 1988;16:82-83.
Question 94
High Yield
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10 degrees of hip abduction on the left and 30 degrees on the right with the hips and knees extended. The Thomas test shows 20 degrees of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0 degrees on the left and -10 degrees on the right. The neck shaft angles are 170 degrees bilaterally. Which of the following procedures would offer the best results?
Detailed Explanation
The patient has bilateral subluxated hips, with nearly vertical neck shaft angles; therefore, the treatment of choice is varus derotation osteotomy. Shortening of the bone on one or both sides may be necessary to allow adequate range of motion postoperatively. In patients this age and with this degree of bony deformity, soft-tissue releases are not likely to lead to hip stability. Botulinum toxin has been shown to be effective in the treatment of ankle equinus, but its efficacy in other areas has not been demonstrated as yet. The indications for obturator neurectomy are unclear at present. Proximal femoral resection is a salvage procedure for long-standing hip dislocations that are symptomatic and not reconstructable. Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Question 95
High Yield
A 19-year-old man sustained the isolated injury seen in Figure 28a. He is adequately resuscitated. A closed reduction was performed in the emergency department, and postreduction radiographs are shown in Figures 28b and 28c. What is the next most appropriate step in management?



Explanation
Incarcerated fragments and nonconcentric reductions are best treated with urgent open reduction, retrieval of the fragments, and internal fixation. Delayed treatment increases the damage to the articular surface, even if traction is applied. There is no role for nonsurgical management with entrapped fragments and nonconcentric reduction of the hip. Epstein HC, Wiss DA, Cozen L: Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9-17.
Question 96
High Yield
At the L4-5 level, what is the location of the S2-5 nerve roots in relationship to the L5 and S1 nerve roots?
Explanation
The nerve roots of S2-5 are positioned dorsally and in the midline relative to the L5 and S1 nerve roots. The L5 nerve root is located lateral to S1 as it prepares to exit under the L5 pedicle. The S1 nerve root is located lateral and ventral to the S2-5 nerve roots. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 3-17.
Question 97
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of



Explanation
The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal. Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Question 98
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?

Explanation
The bright signal on the T2-weighted MRI scan suggests fluid. The multiloculated appearance in proximity to the proximal tibiofibular joint suggests that the most likely diagnosis is a ganglion. They typically increase and decrease in size and can be diagnosed by the classic gelatinous fluid obtained through needle aspiration. Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Question 99
Figures 1a through 1c show the radiograph and MRI scans of a 16-year-old patient who has a painful hip. Examination reveals a significant limp, limited abduction and internal rotation, and severe pain with internal rotation and adduction. A biopsy specimen is shown in Figure 1d. What is the deposited pigment observed in this condition?




Explanation
Pigmented villonodular synovitis (PVNS) is a synovial proliferative disorder that remains a diagnostic difficulty. The most common clinical features are mechanical pain and limited joint motion. On radiographs, the classic finding is often a large lesion, associated with multiple lucencies. Other findings may include a normal radiographic appearance, loss of joint space, osteonecrosis of the femoral head, or acetabular protrusion. MRI is the imaging modality of choice and will show the characteristic findings of a joint effusion, synovial proliferation, and bulging of the hip. The synovial lining has a low signal on T1- and T2-weighted images, secondary to hemosiderin deposition. Copper deposition occurs in patients with Wilson's disease, which mainly affects the liver. Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 100
High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?

Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
