Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Question 2
High Yield
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?

Explanation
The patient has hypertrophic arthritis, which is a strong risk factor for heterotopic bone formation. The remaining complications are possible but do not have the same significant risks. Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Question 3
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the

Explanation
The recurrent laryngeal nerve lies between the trachea and the esophagus and is subject to stretch injury if excessive retraction is applied. The vagus nerve lies in the carotid sheath. The sympathetic trunk lies anterior to the longus colli muscles. The hypoglossal nerve and superior laryngeal nerve are both at risk during the exposure but are not located between the trachea and esophagus. An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, chapter 2.
Question 4
Fully dense alumina and zirconia materials have been used as bearing materials in hip arthroplasty to provide greater wear resistance than polished metallic surfaces. Although both have shown reduced wear clinically, what concerns continue to exist about the use of zirconia?
Explanation
Zirconia as a bearing surface is "metastable," meaning that, in the microstructure of the material the zirconia molecules are ordered in a tetragonal fashion, but they can easily transform to a monoclinic microstructure that is less wear resistant. Transformation can occur with input of enough energy (eg, thermal energy imparted by steam sterilization or mechanical energy at the bearing surface). Zirconia was introduced as an alternative to alumina because it has a higher toughness, making it less susceptible to gross fracture (ceramics do not undergo fatigue fracture, but rather fail from a process of slow crack growth). Zirconia is highly biocompatible (as are many ceramics) and is essentially immune to corrosive processes that can plague metallic alloys such as stainless steel. Clarke IC, Manaka M, Green DD, et al: Current status of zirconia used in total hip implants. J Bone Joint Surg Am 2003;85:73-84. Haraguchi K, Sugano N, Nishii T, et al: Phase transformation of a zirconia ceramic head after total hip arthroplasty. J Bone Joint Surg Br 2001;83:996-1000.
Question 5
What is the most common result if the acetabulum is rotated too far anteriorly during a periacetabular osteotomy?
Explanation
In patients with hip dysplasia who undergo a periacetabular osteotomy, the authors note that the freed acetabular segment can be overcorrected for the deformity. If it is placed too anteriorly, then hip flexion is limited. Posterior dislocation is a rare complication. The other complications should not occur as a result of this procedure. Hussell JG, Rodriguez JA, Ganz R: Technical complications of the Bernese periacetabular osteotomy. Clin Orthop 1999;363:81-92.
Question 6
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?

Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Question 7
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?

Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 8
High Yield
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?

Detailed Explanation
The patient has a posterior dislocation. The radiograph reveals marked internal rotation, but fails to show whether the humeral head is posteriorly displaced. Therefore, an axillary radiograph should be obtained to help confirm the diagnosis. Transverse view CT or MRI scans also may be useful. The other studies will not help confirm the diagnosis. In addition to a direct posterior blow, a shoulder dislocation may be caused by a seizure disorder or electrocution. Bloom MH, Obata WG: Diagnosis of posterior dislocation of the shoulder with the use of Velpeau axillary and angle-up roentgenographic views. J Bone Joint Surg Am 1967;49:943-949.
Question 9
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea. Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Question 10
High Yield
What muscle is most often encountered during surgical approaches to C5-6?
Detailed Explanation
The omohyoid muscle crosses the surgical field from inferior lateral to anterior superior traveling from the scapula to the hyoid bone and may need to be transected. The posterior digastric crosses the field as well but higher near C3-4. The other muscles run longitudinally. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Question 11
High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?

Detailed Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 12
High Yield
What is the second most common primary bone malignancy in children?

Explanation
Ewing's sarcoma is the second most common bone tumor in children with an incidence of three per one million Caucasian children younger than 21 years of age. Ewing's sarcoma is rare in African Americans. Osteosarcoma is the most common bone tumor in children. Rhabdomyosarcoma is the most common soft-tissue sarcoma in children. Fibrosarcoma is a rare primary bone tumor most commonly seen in adults. Adamantinoma is a rare primary bone malignancy also most commonly seen in adults in the tibia. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Question 13
High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 14
High Yield
What nerve is most likely to be injured during the anterior exposure of C2-3?
Detailed Explanation
The hypoglossal nerve exits from the ansa cervicalis at approximately the C2-3 level and can be injured during retraction up to the C2 level. The superior laryngeal nerve lies at about C4-5. The facial nerve is much higher. The vagus nerve runs with the internal jugular and carotid much more laterally. The phrenic nerve exits posteriorly. Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.
Question 15
High Yield
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
The most important consequence of a displaced talar neck fracture after closed or open treatment is malunion. Because displacement of the talar neck is associated with displacement of the subtalar joint, any malunion leads to intra-articular incongruity or malalignment of the subtalar joint. Varus malunion is common when there is comminution of the medial talar neck. This results in pain, osteoarthritis, and hindfoot deformity that requires further treatment. Because of these complications, it is imperative that all displaced talar neck fractures are reduced anatomically; fragmented fractures may require bone grafting to maintain the length and rotation of the neck. Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 16
An 83-year-old woman with diabetes mellitus has a history of recurrent infection over the medial aspect of her great toe and has had a painless bunion for the past 45 years. Shoe wear modifications have failed to provide relief. Pedal pulses are palpable. Figures 30a and 30b show the clinical photograph and radiograph. Management should now consist of


Explanation
The presence of recurrent breakdown over the medial eminence despite shoe wear modifications is an indication for surgery. A number of factors must be considered when deciding on an appropriate course of treatment. These include age, activity level, joint congruency, joint degeneration, and the patient's symptoms and expectations. The indications for a simple bunionectomy are rather limited. In this patient, the goal of surgery is to alleviate the recurrent infection by removal of a large medial eminence. Because the bunion is painless and long-standing, it does not warrant treatment. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 123-134.
Question 17
Which of the following is most commonly associated with an open clavicular fracture?

Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 18
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?


Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 19
High Yield
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 20
High Yield
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T1-weighted MRI scan are shown in Figures 28a and 28b. Management should consist of


Explanation
The radiograph and MRI scan reveal a lytic lesion in the left femoral neck region that extends to the lesser trochanter. Although external beam radiation and radioactive iodine infusion may be helpful in controlling the local disease, the patient is at high risk for femoral neck fracture given the location of the lesion. Prophylactic surgery is indicated; therefore, the treatment of choice is a cemented bipolar hemiarthroplasty. The use of a compression hip screw and side plate or an intramedullary nail has a high likelihood of failure with disease progression. Postoperative treatment with radiation therapy and bisphosphonates is also indicated. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264. Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Question 21
High Yield
A 61-year-old woman with a long-standing history of rheumatoid arthritis reports progressive elbow pain for the past 12 months. She denies any recent trauma to the elbow; however, she notes increasing pain and decreased joint motion that are now compromising her function. Radiographs are shown in Figures 57a and 57b. What is the most appropriate treatment at this time?


Detailed Explanation
The patient has end-stage arthritis of the elbow with advanced joint destruction. At this point, nonsurgical management is unlikely to provide much relief of symptoms. Arthroscopic procedures can provide relief, but it is likely to be incomplete and unpredictable. The most reliable surgical option is total elbow arthroplasty. Currently, semiconstrained components are generally preferred because constrained components have been associated with a high rate of early prosthetic loosening. Little CP, Graham AJ, Karatzas G, et al: Outcomes of total elbow arthroplasty for rheumatoid arthritis: Comparative study of three implants. J Bone Joint Surg Am 2005;87:2439-2448.
Question 22
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
All of the factors listed contribute to some extent to the pull-out strength of lumbar pedicle screws, but bone mineral density correlates most precisely. Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Question 23
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of


Explanation
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Question 24
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of

Explanation
Osteolysis of the distal clavicle is common in weightlifters; therefore, distal clavicle excision is the treatment of choice. A subacromial decompression alone would not alleviate the acromioclavicular joint symptoms. Interval closure, biceps degeneration, and superior labrum anterior and posterior repair would limit superior migration but would not explain the abnormal bone scan. Thermal capsular shrinkage does not have a role here. Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Question 25
High Yield
What is the recommended insertion torque for halo pins in adults?

Explanation
Garfin and associates have shown that halo pins inserted with 8 in-lb of insertion torque results in significantly less loosening with cyclical loading than pins inserted with 6 in-lb of torque. Moreover, Botte and associates reported that 8 in-lb of torque is clinically safe and effective in lowering the incidence of pin loosening and infection. Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752. Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Question 26
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be


Explanation
The patient has a unicameral bone cyst. Because the subtrochanteric part of the femur is a high-stress region, the treatment of choice is bone curettage and grafting. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Question 27
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided. Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 28
High Yield
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?

Detailed Explanation
The MRI scan shows increased signal intensity along the deep fibers of the supraspinatus near its insertion. This is typical of tendinosis and a probable partial-thickness rotator cuff tear. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 29
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
The great medullary artery originates as a direct or indirect branch of the left posterior intercostal artery, usually between T8 and T12. It becomes intradural and crosses over one to three disk spaces before turning to the midline where it anastomoses with the anterior spinal artery. Injury to this artery can result in devastating ischemia of the lower spinal cord. Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
Question 30
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?


Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 31
High Yield
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of

Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 32
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of


Explanation
In a patient with known metastatic disease, the surgeon must rule out additional lesions throughout the femur prior to surgical management. Lesions located in the diaphysis or in the peritrochanteric region may influence the surgical procedure. Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 33
High Yield
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm3. Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of

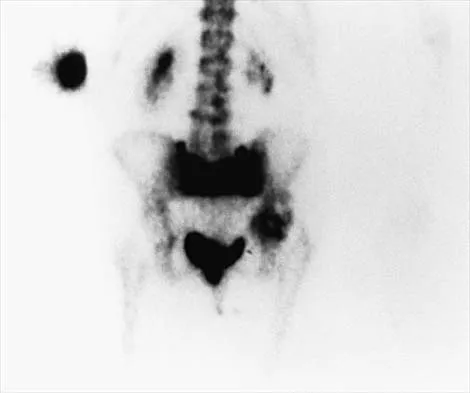
Explanation
The radiograph shows bilateral cemented total hip arthroplasties. The acetabular components are loose bilaterally, but there has been no acute change. Therefore, it is unlikely that the acetabular loosening is contributing to the patient's pain. The bone scan is consistent with a sacral insufficiency fracture. This is best treated with bed rest and pain medication. Activity can be increased as the pain allows. Revision will not address the pain. Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Question 34
High Yield
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of

Explanation
The patient has symptomatic grade IV Brooker heterotopic ossification. Once the bone has matured, it can be excised. Surgical excision should be combined with postoperative irradiation to avoid recurrence. Pharmacologic and irradiation intervention are not successful beyond the perioperative period unless they are combined with surgical excision of mature heterotopic ossification. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 35
High Yield
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
Explanation
The use of multiagent chemotherapy has been shown to be associated with a survival benefit in patients with osteosarcoma. The use of chemotherapy in adults with soft-tissue sarcoma remains somewhat controversial. It has not been associated with improved survival rates in patients with renal carcinoma, dedifferentiated chondrosarcoma, or melanoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Question 36
High Yield
What is the treatment of choice for the injury shown in Figures 20a through 20c?



Detailed Explanation
The radiographs show multiple carpometacarpal dislocations. Reduction is often obtainable but difficult to maintain. Internal fixation is required to maintain the reduction, preferably with Kirschner wires. Closed reduction and percutaneous pinning is preferred by some surgeons. Others recommend open reduction to remove irreconstructable osteochondral fragments from the individual joints and to ensure correct reduction of the carpometacarpal joints. Kirschner wires are removed at 6 to 8 weeks. Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
Question 37
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?


Explanation
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis. Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Question 38
High Yield
Figures 57a through 57c show the radiographs of a patient who has pain, discomfort, and a popping sensation localized to the posterior aspect of the knee after undergoing primary left total knee arthroplasty 6 months ago. Examination reveals that the patient is able to ambulate without a limp. There is no significant swelling, erythema, or effusion. Range of motion is 0 degrees to 115 degrees, and a palpable crepitation or snapping is detected at the posterior lateral joint line. What is the most likely diagnosis?



Detailed Explanation
Popliteal snapping syndrome represents the most likely diagnosis. Barnes and Scott noted that the popliteus tendon can be a potential source of internal derangement after total knee arthroplasty. They noted that it can be subluxated anteriorly and posteriorly over a retained lateral femoral condyle osteophyte. Allardyce and associates described the condition as a popliteus condition, snapping as it rolls over a retained lateral femoral condylar osteophyte. Patellar clunk syndrome is a distinct syndrome associated with the patella and has been reported in posterior stabilized knees. In addition to crepitation with range of motion, the patella literally snaps or jumps as the knee is taken from flexion to extension. Beight JL, Yao B, Hozack WJ, et al: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142. Barnes CL, Scott RD: Popliteus tendon dysfunction following total knee arthroplasty. J Arthroplasty 1995;10:543-545.
Question 39
High Yield
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
Rheumatoid arthritis (RA) is a complex multisystem disorder. It has been suggested that patients with RA have an impaired capacity to control infection with Epstein-Barr virus. Epstein-Barr virus has oncogenic potential and is implicated in the development of some lymphomas. Recent publications provide evidence for an altered Epstein-Barr virus-host balance in patients with RA who have a relatively high Epstein-Barr virus load. Large epidemiologic studies confirm that lymphoma is more likely to develop in patients with RA than in the general population. The overall risk of development of lymphoma has not risen with the increased use of methotrexate or biologic agents. Histologic analysis reveals that most lymphomas in patients with RA are diffuse large B cell lymphomas, a form of non-Hodgkin lymphoma. Epstein-Barr virus is detected in a proportion of these. Patients with RA do not have prevalence for infection with any of the other mentioned viruses. Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
Question 40
High Yield
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?

Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
Question 41
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
Breech positioning has been noted as the risk factor that most increases the relative risk of developmental dysplasia of the hip in multiple series and meta-analysis. All the other factors also increase the risk but to a lesser magnitude. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 42
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?

Explanation
Burks and Schaffer described an approach to the tibial insertion of the posterior cruciate ligament that uses the interval between the semimembranosus and the medial gastrocnemius. The medial gastrocnemius muscle is retracted laterally and protects the neurovascular bundle. This approach is used to repair an avulsion of the posterior cruciate ligament tibial attachment or for performing a posterior cruciate ligament tibial inlay reconstruction. Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Question 43
High Yield
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of

Explanation
Femoral shortening osteotomy for a Crowe type IV hip dislocation has been shown to provide superior results with minimal complications. Cementless fixation of the stem allows for modular implants that greatly simplify the reconstruction.
Question 44
High Yield
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of


Explanation
The radiograph is consistent with a unicameral (simple) bone cyst. The MRI scan reveals that the cyst is juxtaposed to the physis and therefore can be classified as active (latent cysts are more than 1 cm away from the physis). Active cysts are treated with aspiration and steroid injection, although repeated injections may be necessary. Curettage and bone grafting results in more reliable healing but may lead to growth arrest in active cysts. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Question 45
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 46
High Yield
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?



Explanation
Excessive hindfoot valgus can lead to abutment between the calcaneus and fibula. This valgus force can lead to a stress fracture of the distal fibula. Surgery may be required if an insufficiency fracture recurs despite orthotic management. Of the choices listed, a subtalar arthrodesis is most likely to achieve rebalancing of the foot at the level of the deformity. Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Question 47
The sartorius muscle is innervated by which of the following nerves?

Explanation
The femoral nerve enters the thigh behind the inguinal ligament, lying on the surface of the iliopsoas muscle lateral to the femoral artery and vein. The nerve divides into numerous muscular and cutaneous branches in the femoral triangle. The first motor branch (sometimes two branches) is to the sartorius. There is a variable branch to the pectineus. Subsequent branches go to the rectus femoris and then the vastus muscles in variable order. The last motor branch is to the articularis genu. The muscular branches can be injured in anterior approaches to the hip, especially the middle window of the ilioinguinal approach. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Question 48
High Yield
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
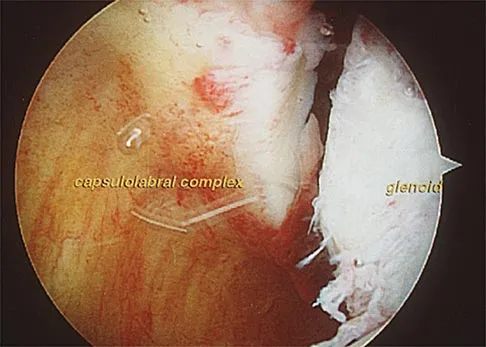
Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Question 49
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
A complete answer necessarily includes the means and standard deviations of bone mineral density in both groups. Given these, which are the basic results of the study, the P-value can be calculated if desired. All of the other options preclude assessment of the actual data, that is, the information collected by the study. P-values and confidence intervals should be perceived as additional information, which help to assess the certainty of relating the study's findings to the general population, but they should not be reported instead of the results (ie, the means and standard deviations).
Question 50
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of

Explanation
The patient has retorn his rotator cuff repair. This traumatic retear is different from a chronic tear and should be treated similar to an acute rotator cuff tear. Because the patient is younger than age 65 and has a small, single tendon tear, a revision rotation cuff repair is indicated with an expected tendon healing rate of greater than 95%. A physical therapy program is not indicated, and further delay in repair compromises his functional recovery. A cortisone injection is not indicated for this repairable tendon tear. Immobilization will not allow the tendon to heal once it has retorn. A debridement procedure is not indicated on this repairable tendon tear; this procedure is indicated in painful, chronic, irreparable tendon tears. Boileau P, Brassart N, Watkinson DJ, et al: Arthroscopic repair of full-thickness tears of the supraspinatus: Does the tendon really heal? J Bone Joint Surg Am 2005;87:1229-1240. Jost B, Zumstein M, Pfirrmann CWA, et al: Long-term outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2006;88:472-479.
Question 51
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a "severe" ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?

Explanation
The radiograph shows posttraumatic tibiofibular synostosis. This condition typically follows an eversion (high) ankle sprain that results in disruption of the interosseous membrane. Ossification usually develops within 6 to 12 months after the injury. Return to sports is possible despite the lack of normal ankle dorsiflexion and mobility between the tibia and fibula. Surgical excision is reserved for persistent pain that fails to respond to nonsurgical management once the ossification is "cold" on bone scintigraphy. Whiteside LA, Reynolds FC, Ellsasser JC: Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 1978;6:204-208. Henry JH, Andersen AJ, Cothren CC: Tibiofibular synostosis in professional basketball players. Am J Sports Med 1993;21:619-622.
Question 52
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 53
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?



Explanation
The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.
Question 54
High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 55
A 72-year-old woman with rheumatoid arthritis who underwent primary total knee arthroplasty 2 years ago has had diffuse knee pain that developed shortly after the surgery. The patient has difficulty with stair descent and arising from chairs. Evaluation for infection is negative. AP and lateral radiographs are shown in Figure 26. Management should now consist of

Explanation
The radiographs show posterior flexion instability that is the result of flexion-extension gap imbalance and/or posterior cruciate ligament incompetence after a posterior cruciate-retaining total knee arthroplasty. The radiographs also show anterior femoral displacement on the tibia. Pagnano and associates reported on a series of patients with painful total knee arthroplasties who had been previously diagnosed as having pain of unknown etiology, showing that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Question 56
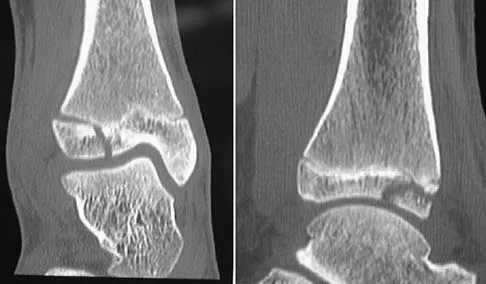
Figures 45a through 45c show the radiograph, CT scan, and MRI scan of a 15-year-old boy who has lateral ankle pain. What is the most likely diagnosis?



Explanation
The elongated anterior process of the calcaneus reaching distally toward the navicular is an abnormal finding. Instead of viewing the rounded, blunt distal anterior process of the calcaneus, a bridge extends to the navicular, albeit incomplete. These findings are consistent with a fibrous coalition. CT can reveal a stress fracture of the calcaneus, arthritis of the subtalar joint with subchondral cysts, or an os peroneal bone disruption in the peroneus longus, but those entities are not shown here. The plantar fascia is intact. Richardson EG: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 702-732.
Question 57
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
A 32-mm head design results in less linear wear but more volumetric wear particles. Modular components that allow motion between the polyethylene insert and the shell can result in backside wear. The oxidative degradation of gamma-irradiated polyethylene stored in air leads to increased wear. All of these factors lead to a greater particulate load and more osteolysis. Circumferential porous coating blocks ingrowth of particle-laden fluid and decreases osteolysis. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Fisher J, Hailey JL, Chan KL, et al: The effect of aging following irradiation on the wear of UHMWPE. Trans Orthop Res Soc 1995;20:12.
Question 58
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?

Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 59
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
A common side effect of interscalene nerve block for shoulder surgery is the blockade of the ipsilateral phrenic nerve. This, in turn, results in paresis of the diaphragm and up to a 30% reduction in pulmonary function volumes. Therefore, interscalene nerve block generally is not recommended for patients whose respiratory function is compromised. Other relative and absolute contraindications for interscalene nerve blocks include allergy to local anesthetics, infection at the injection site, uncontrolled seizure disorder, coagulation abnormality, and preexisting neurologic injury. Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.
Question 60
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty?

Explanation
The Grammont reverse total shoulder arthroplasty is designed to medialize the center of rotation, thereby increasing the deltoid moment arm and lengthening the deltoid. Werner CM, Steinmann PA, Gilbert M: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 61
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?


Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 62
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?

Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 63
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Question 64
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
The patient has internal impingement. Internal impingement is commonly seen in overhead throwing athletes. When positioned in the extreme cocking phase of the throwing cycle, the posterior glenoid impacts the articular surface of the infraspinatus and posterior fibers of the supraspinatus tendon. This impact can cause partial-thickness rotator cuff tearing and posterosuperior labral lesions. She has no evidence of anterior shoulder instability, and her range of motion is excellent which rules out adhesive capsulitis. Subacromial impingement is identified with anterolateral shoulder pain with internal rotation in the abducted position. A full-thickness rotator cuff tear in a 22-year-old individual would require significant trauma and would likely result in pain at rest and with lifting. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 65
High Yield
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
The stretching of the graft occurs over time as the graft is loaded. Time-dependent deformation under load is called creep and is common in viscoelastic materials such as ligament tissue. Creep can occur under both static and cyclic load conditions; time-dependent deformation will occur as long as load is applied to the tissue. Similarly, when a graft is initially tensioned to a given deformation at surgery, the load generated in the graft will decrease over time; this behavior is called stress relaxation and also is indicative of a viscoelastic material. Water content may affect the viscoelastic properties by changing the friction between collagen fibers, but studies have shown little difference in water content between grafts and normal ligaments. Fatigue failures may manifest themselves through damage to the ligament tissue, but this would require higher loads than are routinely experienced by grafts. Elastic stretch is recoverable and, therefore, does not contribute to a permanent stretch. Similarly, gross failure at the attachment would not cause a stretch, but rather a catastrophic instantaneous instability. Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Question 66
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?

Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 67
High Yield
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?

Detailed Explanation
There is no evidence that early weight bearing enhances ultimate rehabilitation. At the other extreme, weight bearing should not be delayed for a prolonged period of time. In a young, healthy individual, the rigid plaster dressing appears to be the safest method of protecting the wound during the early postoperative period. If the wound appears to be secure, early partial weight bearing can be safely initiated. Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Question 68
High Yield
The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has

Detailed Explanation
The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube. Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Question 69
High Yield
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?

Explanation
Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3. Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Question 70
High Yield
A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of



Explanation
The oblique nature of the fracture and extension of the fracture to the condyles implies an unstable fracture. Lag screw fixation provides an excellent chance of union, and the ability to start early range of motion. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 71
High Yield
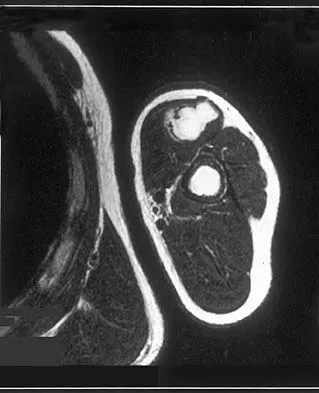
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of

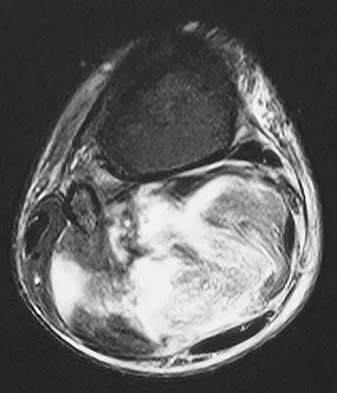
Explanation
Soft-tissue sarcomas generally are treated with radiation therapy and wide surgical resection. In this patient, involvement of most of the posterior calf compartment and circumferential involvement of the posterior tibial and peroneal neurovascular bundle makes limb salvage impractical. Any attempt at wide surgical resection would leave a poorly functioning limb with questionable surgical margins. A high below-knee amputation would be the best option. Radiation therapy alone is contraindicated. Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397. Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 72
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?

Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 73
High Yield
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
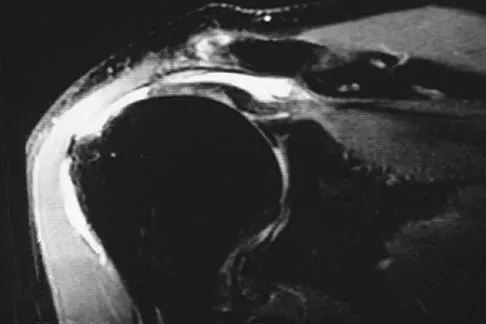
Explanation
The MRI scan reveals a full-thickness rotator cuff tear with retraction and increased signal in the subacromial space indicating joint fluid. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 74
High Yield
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?


Explanation
The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five "P's" of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease. Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998, pp 1826-1844.
Question 75
High Yield
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

Detailed Explanation
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures. Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Question 76
High Yield
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Detailed Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted. Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Question 77
Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?
Explanation
Surgical technique in patellar resurfacing has been found to be one of the critical factors in the success or failure of total knee arthroplasty. Theoretically, metal-backed patellar components are an excellent way of evenly distributing joint forces from the polyethylene button to bone (similar to the tibial component). However, despite this theoretical advantage, metal-backed patellae have been associated with a higher failure rate. Some of the observed problems include poor bone ingrowth, peg failure, dissociation of the metal plate and polyethylene button, and component fracture. Because of these factors, all-polyethylene patellae have proved to be the standard if patellar resurfacing is attempted. Medialization of the patellar component, a symmetrically thick patella, and external rotation of the femoral and tibial components improve patellar tracking. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Question 78
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 79
High Yield
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Detailed Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 80
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 81
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?




Explanation
Synovial sarcoma should always be considered in the differential diagnosis of a foot mass; however, the histopathology shows a typical example of PVNS, with hemosiderin, giant cells, and synovium. Synovial chondromatosis would have metaplastic cartilage in the synovium. The radiograph shows subtle erosion of the lateral cortex of the cuboid, and the MRI scan shows a soft-tissue mass. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830. Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Question 82
High Yield
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?



Explanation
Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients. Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 83
High Yield
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must

Detailed Explanation
While it is recommended that a patient gain full range of motion, pain-free function, and symmetric strength prior to returning to vigorous activities, it is absolutely essential that radiographs of the fracture site reveal a circumferential external bridging callus to prevent refracture. This is particularly important for comminuted femoral fractures with various sized fragments. It is also recommended that a return to rodeo riding be postponed for at least 1 year. Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112. Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am 1991;73:1561-1566.
Question 84
The inheritance of the deformity shown in Figure 1 is most commonly

Explanation
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
Question 85
A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?

Explanation
CMT is characterized by a cavovarus foot position that increases weight-bearing stresses along the lateral border. Removal of the fifth metatarsal head carries the risk of creating a transfer lesion at the fourth metatarsal head, particularly with a cavovarus foot. Claw toes are common in CMT, but the fifth toe would be flail in this situation. Ulceration is unlikely given the lack of underlying bone. Peroneal atrophy is associated with CMT but would not be a complication of this procedure. Charcot arthropathy is a neuropathic process frequently seen in individuals with diabetes mellitus. Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.
Question 86
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?

Explanation
The recurrence rate of anterior dislocation of the shoulder after the first episode in athletes younger than age 20 years is thought to be as high as 90%, making surgery after the initial episode a consideration. The rate drops from 50% to 75% in the 20- to 25-year age group and down to 15% in patients older than age 40 years. An excellent prospective study of 257 patients in Sweden showed that there was no difference in those who did or did not complete 3 weeks of immobilization. The study also showed variability among different age groups in the importance of athletic participation; athletes in the 12- to 22-year age group had a higher recurrence rate, whereas the more sedentary patients in the 23- to 29-year age group had a higher rate. Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Question 87
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30 degrees of flexion, which decreases as the knee is flexed to 90 degrees. What is the most likely diagnosis?

Explanation
The flexed knee and ankle mechanism of injury can result in a PCL and/or posterolateral corner injury. The examination reveals an isolated injury to the posterolateral corner (arcuate, popliteus, posterolateral capsule). This results in increased posterior translation and external rotation, as well as varus that is most notable at 30 degrees of flexion and decreases as the knee is further flexed to 90 degrees. Combined PCL and posterolateral corner injuries are characterized by increasing instability as the knee is flexed to 90 degrees from 30 degrees, while isolated PCL tears show the greatest degree of instability at 90 degrees of flexion. A rupture of the quadriceps tendon would not affect anterior or posterior stability, whereas an isolated rupture of the lateral collateral ligament, which is a rare injury, is characterized by varus instability at 30 degrees of knee flexion without posterior translation. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 88
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 89
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of

Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Question 90
High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 91
High Yield
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?

Explanation
The child has a near complete central physeal arrest of the distal femur and worsening limb-length discrepancy will develop. She is growing at the average rate for the population. The distal femoral physis grows at a rate of roughly 9 mm per year. Girls finish their growth at approximately age 14 years. Thus, at maturity the left leg will be 6.4 cm longer than the right. An angular deformity has not developed at this point and her arrest is central; therefore, angular deformity is unlikely to develop in any plane. Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Question 92
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?

Explanation
In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311. DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 93
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty. Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 94
High Yield
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?

Detailed Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 95
High Yield
What are the four most common soft-tissue sarcomas to spread via the lymph node system?

Explanation
Soft-tissue sarcomas most frequently metastasize to the lung, but certain histologic types have a predilection for the lymph node system as well. Rhabdomyosarcoma, clear cell sarcoma, epithelioid sarcoma, and synovial sarcoma are four of the most common types to spread in this fashion. Careful evaluation and/or sentinel lymph node biopsy plays a role in disease staging and prognosis. Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Question 96
Figure 42 shows the sagittal T2-weighted MRI scan of a patient's right knee. These findings are most commonly seen with a complete tear of the

Explanation
The MRI scan reveals disruption of the lateral capsule and ligaments with fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions. LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Question 97
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 98
High Yield
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. What type of injury pattern is shown?


Detailed Explanation
The patient has a transscaphoid dorsal perilunate dislocation. The radiographs clearly define a dorsal dislocation of the capitolunate joint, and the scaphoid fracture component is easily visible on the AP view. A scaphoid fracture alone is an unlikely diagnosis because of the midcarpal dislocation component. The radiocarpal joint is not dislocated because the lunate is sitting in the lunate fossa of the radius. Isolated radiocarpal dislocations are not associated with a midcarpal disruption. While a midcarpal dislocation is a component of a dorsal perilunate dislocation, this diagnosis does not address the scaphoid fracture. A volar lunate dislocation is not seen because the lunate is reduced in the lunate fossa of the distal radius. Volar lunate dislocations are in the spectrum of injury of perilunate dislocations and fracture-dislocations; however, the radiographs show a transscaphoid dorsal perilunate dislocation. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 99
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
These finding indicate central cord syndrome, and injury that is more common in the older population who have some degree of spondylosis. The physiologic insult can be a central spinal hematoma with resultant hematomyelia. Bowel and bladder functional return has a good prognosis, unlike the upper extremity motor loss. Cauda equina syndrome generally involves injury at the lumbar levels, with some degree of lower extremity motor loss. Posterior cord syndrome is characterized by preservation of motor function below the level of injury and position/vibratory sensory loss. Brown-Sequard syndrome, which is often produced by a penetrating injury, results in contralateral hypalgesia and ipsilateral weakness. Anterior cord syndrome has a poor prognosis for functional return; lower extremity findings include loss of light touch, sharp/dull, and temperature sensations below the level of injury, as well as motor function. Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Question 100
High Yield
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?
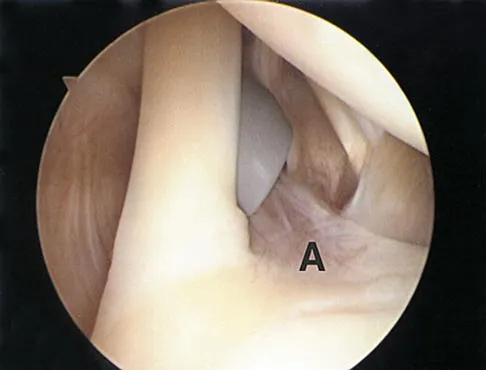
Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
