Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic

Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 2 High Yield
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Detailed Explanation
An inability to participate in athletics generally is considered an indication for continued symptomatic treatment only. All of the other answers suggest the possibility of more significant pathology that may require more urgent treatment. Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
Question 3
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
Intramembranous ossification occurs through the direct formation of bone without the formation of a cartilaginous intermediate. Clinically, both intramembranous and endochondral ossification occur simultaneously during fracture healing; however, the latter is characterized by the differentiation and maturation of chondrocytes, vascular invasion of a hypertrophic cartilage matrix, and bone formation. Collagens type II and X are cartilage specific and would be characteristic of endochondral ossification, not intramembranous ossification. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 4
A 23-year-old man who is a competitive overhead athlete has shoulder pain. Based on the pathology shown in Figure 47, what treatment option would yield the highest satisfaction and return to overhead sports?

Explanation
The patient has a classic type II SLAP tear that will respond best to arthroscopic repair. Labral debridement has been shown to lead to predictably poor results, and biceps tenodesis and tenotomy may be appropriate for an older patient who is not a competitive overhead athlete. Snyder SJ, Karzel RP, Del Pizzo W, et al: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279.
Question 5 High Yield
Which of the following variables has been shown to have the greatest influence on the higher rate of anterior cruciate ligament (ACL) tears in women when compared to men for similar sports?

Detailed Explanation
All of the variables have been proposed as possible causes for the increased incidence of ACL tears in women versus men. The general differences in the level of neuromuscular training however, specifically conditioning and muscle strength, have been shown to play the greatest role. Harmon KJ, Ireland ML: Gender differences in noncontact anterior cruciate ligament injuries. Clin Sports Med 2000;19:287-302. Arendt EA: Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med 1995;23:694-701.
Question 6High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 7 High Yield
The lateral arm flap is based on what arterial supply?
Detailed Explanation
The lateral arm flap is based on the posterior radial collateral artery, a branch of the profunda brachial artery. Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
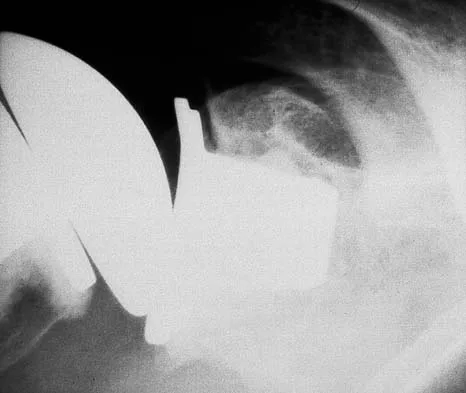
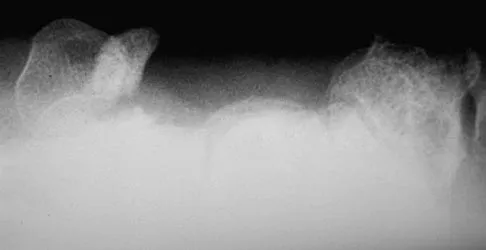
Question 8High Yield
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?

Explanation
The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 9High Yield
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of
Explanation
When external rotation at the side is limited, the most likely diagnosis is contracture of the rotator cuff interval, including the superior glenohumeral and coracohumeral ligaments. Therefore, the treatment of choice is arthroscopic release of the rotator cuff interval.
Question 10High Yield
An 18-year-old man recently underwent an uncomplicated arthroscopic partial medial meniscectomy that was complicated by reflex sympathetic dystrophy (RSD), also termed "sympathetically maintained pain" (SMP). What is the most common finding of this condition?

Explanation
The hallmark for RSD or SMP is the presence of pain that is out of proportion to that expected for the degree of the injury. SMP often extends well beyond the involved area and is present in a nonanatomic distribution. The pain is frequently described as a burning sensation, with extreme sensitivity to light touch. Joint stiffness can be present but is a nonspecific finding. There may be cold intolerance, but this is not a cardinal symptom. Sweating actually may be increased. Osteopenia, if present, is a late finding. Lindenfeld TN, Bach BR Jr, Wojtys EM: Reflex sympathetic dystrophy and pain dysfunction in the lower extremity. Instr Course Lect 1997;46:261-268.
Question 11
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of

Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 12 High Yield
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm3, with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?

Detailed Explanation
The differential diagnosis includes septic hip and transient synovitis. Both disorders may present with a joint effusion. The increased teardrop distance and loss of range of motion implies that there is excess fluid in the joint. While the other tests can confirm this, only aspiration can characterize the fluid further, thereby indicating the etiology of the effusion. Provided there is enough fluid obtained at aspiration, the joint fluid should be sent for Gram stain, culture, cell count, glucose, and protein studies.
Question 13
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of

Explanation
Most patients with a significant recurrent neuroma will not obtain relief with conservative methods. Pain results from a stump neuroma at the weight-bearing area from too short of a resection of the nerve or from regrowth of the remaining nerve end. Although steroid injection may be helpful in localizing symptoms or providing temporary relief, it rarely cures a stump neuroma. Orthotics with a metatarsal pad will likely increase pressure and pain at the neuroma site. Physical therapy could temporize the symptoms but will not address the underlying problem. Similarly, bone decompression alone will not alter the location of the neuroma stump. Revision of the nerve to a more proximal level off of the weight-bearing area is the most likely method to succeed. A plantar approach facilitates identification and ability to revise the nerve to a more proximal level. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657. Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Question 14High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 15
A 10-month-old girl has the spinal deformity shown in Figures 55a and 55b with no apparent neurologic finding. The next step in evaluation should be to obtain


Explanation
Approximately 60% of patients with a congenital spine abnormality have associated malformations outside the spinal column. Genitourinary abnormalities are probably the most common, occurring in up to 37% of patients. These are usually anatomic anomalies, such as renal agenesis, duplication, fusion, and ectopia. A genitourinary ultrasound is the least invasive screening tool. Other associated anomalies include cervical vertebral abnormalities, VATER syndrome, and intraspinal abnormalities such as diastematomyelia. An MRI scan is not recommended as part of the screening examination; however, if the patient had neurologic signs or symptoms, an MRI scan would be indicated. Beals RK, Robbins JR, Rolfe B: Anomalies associated with vertebral malformations. Spine 1993;18:1329-1332.
Question 16
Figures 39a and 39b show the MRI scans of a 25-year-old man with right shoulder pain. Figure 39c shows the arthroscopic view from a posterior portal in the beach chair position. What is the most likely diagnosis?



Explanation
The MRI scans show coronal oblique and sagittal oblique views of a partial articular surface supraspinatus tear or tendon avulsion (PASTA lesion). The arthroscopic view is a posterior portal of the glenohumeral joint viewing the articular surface of the supraspinatus. These tears are a common source of shoulder pain and are often amenable to transtendon arthroscopic repair without detachment of the intact bursal surface. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105. McConville OR, Iannotti JP: Partial-thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Question 17High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 18
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?

Explanation
The patient has an obvious slipped capital femoral epiphysis of the left hip for which the recommended treatment is percutaneus pinning in situ. Development of a contralateral slip is less likely at this age; therefore, observation of the right hip is indicated because there is no general agreement regarding prophylactic fixation. Typically, there is no role for spica casting. Physical therapy is not indicated as a primary treatment, and reduction is contraindicated, as it has been associated with osteonecrosis. Loder RT, Aronsson DD, Greenfield ML: The epidemiology of bilateral slipped capital femoral epiphysis: A study of children in Michigan. J Bone Joint Surg Am 1993;75:1141-1147. Aronsson DD, Karol LA: Stable slipped capital femoral epiphysis: Evaluation and management. J Am Acad Orthop Surg 1996;4:173-181. Hurley JM, Betz RR, Loder RT, Davidson RS, Alburger PD, Steel HH: Slipped capital femoral epiphysis: The prevalence of late contralateral slip. J Bone Joint Surg Am 1996;78:226-230.
Question 19
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 20
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?

Explanation
Type I fractures are trochanteric fractures usually secondary to osteolysis. Type II fractures are located around the stem. Type III fractures are distal to the stem. If the fracture and prosthesis are stable, the fracture can be treated nonsurgically. If the fracture is unstable, the stability of the prosthesis should be assessed. If the prosthesis is unstable (type IIB), treatment should consist of revision to a long stem prosthesis that bypasses the fracture by two cortical diameters. If, as in this patient, the prosthesis is not loose (type IIA), open reduction and internal fixation is the appropriate option. Proximal femoral allograft is appropriate for type IIIC fractures in which the proximal bone is significantly compromised and the femoral component is loose. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 21 High Yield
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Detailed Explanation
The tendon most prone to rupture in a patient with rheumatoid arthritis of the wrist is the extensor digiti quinti. It can be a silent injury since the extensor digitorum communis can provide extension to the fifth finger. The extensor digiti quinti is at high risk since it is overlying the ulnar head where it is prone to attritional rupture (Vaughan-Jackson syndrome). Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Question 22High Yield
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
The patient's chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported. Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Question 23
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?

Explanation
The MRI scan shows disruption of the subscapularis muscle. Subscapularis rupture is associated with weakness in internal rotation as shown with a positive lift-off test as described by Gerber and Krushell. The belly press test also has been shown to be a useful clinical test for this problem. Weakness in external rotation and abduction is more consistent with supraspinatus and infraspinatus tears. Deltoid atrophy is associated with an axillary nerve injury. Loss of biceps contour is associated with rupture of the long head of the biceps. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 24High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 25
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?





Explanation
The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
Question 26High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
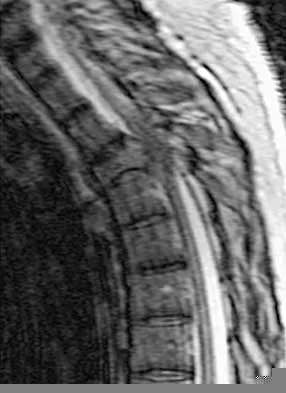
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 27
Figure 21 shows the radiograph of a 32-year-old patient with right hip pain that has failed to respond to nonsurgical management. What is the most appropriate surgical treatment at this time?

Explanation
The radiograph reveals developmental dysplasia of both hips. The patient has classic anterolateral undercoverage of the femoral head on the right side as demonstrated by a high acetabular index (measured at 27 degrees). Anterior undercoverage can be determined by drawing the marking for the anterior wall that fails to overlap the femoral head in this patient. Currently in North America, the most accepted surgical management for symptomatic dysplasia of the hip with good joint space is a Bernese (Ganz) periacetabular osteotomy. Surgical dislocation of the hip and femoroacetabular osteoplasty may be considered for patients with symptomatic femoroacetabular impingement of the hip. Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 28
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
The smallest pedicle isthmic width is at L1, whereas T12 has the largest pedicle width in the upper lumbar and lower thoracic spine. Although smaller in diameter than T12, both T10 and T11 have larger pedicle widths than L1.
Question 29 High Yield
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to

Detailed Explanation
The valgus stress at the elbow caused by throwing strains the medial collateral ligament. The medial epicondyle, on which the ligament inserts, is the last ossification center to fuse to the distal humerus, and acute avulsion of the medial epicondyle can occur in adolescents. If the elbow is allowed to heal in a displaced position, valgus instability and loss of elbow extension may result. Valgus instability is especially problematic for the throwing athlete. Surgical treatment with rigid internal fixation is the treatment of choice for displaced medial epicondyle avulsion fractures. Valgus instability is prevented, and the rigid fixation allows for early range of motion. Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Question 30
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
Absence of the rotator cuff results in superior migration of the humeral head because of unopposed deltoid function. This proximal migration results in eccentric loading of glenoid components with early loosening. Hemiarthroplasty yields good pain relief with limited goals of active elevation of 90 degrees. The coracoacromial arch should be preserved. Achieving satisfactory subscapularis tension is preferred to the use of an oversized humeral component. Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348. Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491. Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Question 31
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?


Explanation
The lesion is an aneurysmal bone cyst. These lesions are known to have a local recurrence rate of 5% to 50%. Young age, open physes, stage, and type of surgical removal and resulting margin have all been shown to affect the recurrence rate. Chemotherapy is not used in the treatment of aneurysmal bone cysts. Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Question 32
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk. Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 33 High Yield
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Detailed Explanation
Coleman block testing, performed by placing an elevation under the lateral border of the foot, is used to determine if the forefoot and/or plantar flexed first ray is causing a compensatory varus in the hindfoot. The block is placed under the lateral border of the foot, and therefore does not have any relation to the Achilles tendon and suppleness of the hindfoot. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 34High Yield
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries. Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Question 35
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The histologic features of multiple myeloma are distinctive for this lesion. The plasma cells are round or oval and have an eccentric nucleus and prominent nucleolus. These characteristics and a clear area next to the eccentric nucleus representing the prominent Golgi center are pathognomonic for plasma cells. Lymphoma is in the differential diagnosis; the most frequent types that occur in bone are large cell or mixed small and large cell types. The histologic appearance of the specimen is not consistent with the other choices.
Question 36High Yield
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?

Explanation
Anatomic positioning of the acetabular component has been shown to be the optimal position for reconstruction of the acetabulum in total hip arthroplasty for DDH. The use of medialized component positioning has been shown to be successful at maximizing the host bone coverage and minimizing the use of bone graft to structurally support the acetabular component. A small acetabular component can be used successfully as long as the femoral head is also reduced in size to maintain the thickness of the acetabular polyethylene. High and lateral positioning for the acetabular reconstruction will result in an increase in the joint reaction forces. In addition, a high and lateral placement will not provide adequate bone to stabilize the reconstruction. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360. Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Question 37
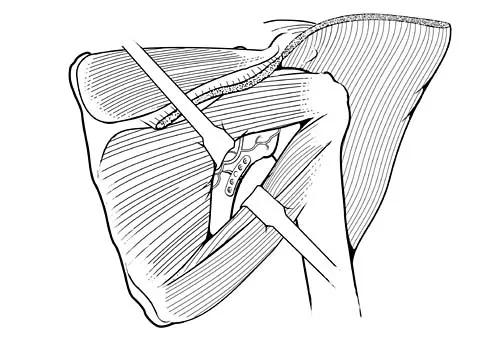
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?

Explanation
The groin flap is based on the superficial circumflex iliac artery, an axial flap that has been a mainstay of providing soft-tissue coverage of the upper extremity. Flaps as large as 35 cm in length and 15 cm in width have been reported. An advantage of the flap is that when used as a pedicle flap, the donor site can be closed directly. A disadvantage of the flap is that it can be quite bulky and can have a thick layer of subcutaneous fat. The superficial circumflex iliac artery travels lateral and superficial to the fascia and below and parallel to the inguinal ligament. It is helpful to elevate the fascia at the medial border of the sartorius muscle to include the deep and superficial branches of the artery for improved flap survival. McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Question 38 High Yield
When treating thoracolumbar spine fractures, which of the following is considered the major advantage of using a thoracolumbosacral orthosis (TLSO) when compared to a three-point fixation brace (Jewett)?

Detailed Explanation
When treating thoracolumbar spine fractures, the major advantage of using the TLSO is greater rotational control. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 347-349. Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA: Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am 1986;17:161-170.
Question 39
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?

Explanation
In an article in the Journal of Shoulder and Elbow, 431 total shoulder arthroplasties were performed with a cemented all-polyethylene glenoid component between 1990 and 2000. Follow-up averaged 4.2 years. In total, 53 surgical complications occurred in 53 patients (12%). Of these, 32 were major complications (7.4%), with 17 of these requiring reoperation. Index complications in order of frequency included rotator cuff tearing, postoperative glenohumeral instability, and periprosthetic humeral fracture. Notably, glenoid and humeral component loosening requiring reoperation occurred in only one shoulder. Data from the contemporary patient group suggest that there are fewer complications of shoulder arthroplasty and less need for reoperation. Especially striking is the near absence of component revision because of loosening or other mechanical factors. Complications involving the brachial plexus have been reported following total shoulder arthroplasty but are not as common of a cause for failure. Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Question 40
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?


Explanation
The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 41
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
Chordomas are very radio- and chemotherapy resistant; therefore, en bloc resection with a negative margin is the preferred treatment. Lesions at or below S3 can be resected without compromising pelvis stability, and continence usually is maintained. The mean survival rate for patients with sacral chordomas is approximately 7 years. Patients with chordoma of the mobile (cervical, thoracic, or lumbar) spine have a mean survival rate of approximately 5 years. This difference is most likely the result of an earlier diagnosis. Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133. Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Question 42
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of


Explanation
The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition. Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Question 43High Yield
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
The diagnosis of bone and joint sepsis in a newborn is difficult because of the relative lack of obvious signs and symptoms. Fever is usually absent. A study of 34 newborns with osteomyelitis identified prematurity and delivery by cesarean section as predisposing factors. In that study, the most common clinical findings were pseudoparalysis, local swelling, and pain on passive movement. Because early diagnosis is so important, any infant who exhibits these findings should be suspected as having bone or joint sepsis. Once the area of involvement is identified, aspiration is mandatory. In newborns who have an infection about the hip, radiographs may reveal subluxation. In this patient, septic arthritis must be ruled out by aspiration of the hip. Developmental dysplasia of the hip is not painful and is not accompanied by localized swelling. If no purulent material is obtained at the time of hip aspiration, an arthrogram should be obtained to rule out epiphysiolysis of the proximal femur. Because the area of involvement has been identified by clinical examination, a gallium scan or MRI scan of the spine is not indicated. Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Question 44 High Yield
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Detailed Explanation
Sexual dysfunction is a common condition after extensive anterior lumbar surgical dissection. Erectile dysfunction usually is nonorganic but may be related to parasympathetic injury. The parasympathetic nerves are deep in the pelvis at the level of S2-3 and S3-4 and usually are not involved in the surgical field for anterior L4-5 and L5-S1 procedures. Retrograde ejaculation is the result of injury to the sympathetic chain on the anterior surface of the major vessels crossing the L4-5 level and at the L5-S1 interspace. Erectile function and orgasm are not affected by sympathetic injury. The pudendal nerve is primarily a somatic nerve and is not located in the surgical field. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Question 45 High Yield
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Detailed Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 46High Yield
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation. Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 47
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 48 High Yield
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Detailed Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 49High Yield
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
Numerous causes of tarsal tunnel syndrome have been reported. The most favorable outcomes from release of the tarsal tunnel are in patients who have a space-occupying lesion (eg, ganglion, lipoma, or neurilemoma). While electrodiagnostic studies may be abnormal preoperatively, there is a low correlation between clinical outcome and electromyographic findings. Intrinsic weakness is a late finding in long-standing nerve dysfunction. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 50
A patient with rheumatoid arthritis has an unstable pseudarthrosis after undergoing C1-2 posterior fusion. No neurologic deficits are noted, and repair with posterior transarticular fixation screws and a posterior wiring technique at C1-2 is planned. Which of the following preoperative studies offers the best visualization?
Explanation
Dickman and associates reported a greater than 10% incidence of vertebral artery anomalies at the C1-2 junction that would preclude the use of either unilateral or bilateral transarticular screw placement. They noted that 13 of 105 patients had a high-riding transverse foramen that precluded bilateral screw placement. In another series, 17 of 94 patients had unilateral high-riding transverse foramina and three had bilateral anomalies. Thin-cut CT with sagittal reconstructions offers the best visualization of the anomalous position of the vertebral artery. They noted that single screw placement in combination with posterior C1-2 fusion was an effective means to secure C1-2 stability. MRI gives excellent visualization of soft tissues and spinal cord compression but is not as clear as thin-cut CT for visualization of the vertebral artery foramina. Vertebral artery angiography is an invasive study with an inherent potential for complications. Electromyography does not correlate with vertebral artery anatomy. Paramore CG, Dickman CA, Sonntag VK: The anatomic suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg 1996;85:221-224. Dickman CA, Sonntag VK: Posterior C1-C2 transarticular screw fixation for atlantoaxial arthrodesis. Neurosurgery 1998;43:275-280.
Question 51 High Yield
Calcitonin acts as an antiresorptive agent by

Detailed Explanation
Calcitonin is a hormone that binds to osteoclasts and acts to decrease both osteoclast activity and number. Calcitonin is most effective in reducing vertebral compression fractures in high-turnover osteoporosis. It is also effective in treating regional osteoporosis. Because of its analgesic effect, it is helpful in treating painful acute compression fractures associated with osteoporosis.
Question 52High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 53
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?

Explanation
The classic MRI findings of osteomyelitis are a decrease in the normally high signal intensity of marrow on T1-weighted images and normal or increased signal intensity on T2-weighted images. This is the result of replacement of marrow fat by inflammatory cells and edema, which causes lower signal intensity than fat on T1-weighted images and higher signal intensity than fat on T2-weighted images. The addition of gadolinium to a T1-weighted sequence reveals increased signal intensity in the hyperemic marrow. Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 54
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
While some curly toe deformities spontaneously improve in younger children, the deformity is likely to persist in a 6-year-old child. Taping techniques result in no change or only a temporary decrease in deformity. Studies have shown that simple flexor tenotomy is as effective as flexor tendon transfer. Arthrodesis is rarely indicated. Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Question 55
A 13-year-old girl has had right groin pain for the past 3 weeks. She denies any history of trauma. Examination of the hip reveals no palpable soft-tissue mass or lymphadenopathy, and there is full range of motion. A plain radiograph and MRI scan are shown in Figures 15a and 15b. Biopsy specimens are shown in Figures 15c and 15d. What is the most likely diagnosis?




Explanation
Fibrous dysplasia frequently occurs in the proximal femur. Microfractures and remodeling can lead to the classic "Shepherd's crook deformity." The lesion has a ground-glass appearance on plain radiographs. The histologic appearance shows proliferating fibroblasts in a loose spindle cell background. Dysplastic metaplastic trabeculae are arranged in an irregular or "Chinese letter" appearance. Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415-1422.
Question 56 High Yield
What is the mechanism of action of bisphosphonates?
Detailed Explanation
Bisphosphonates are stable analogues of pyrophosphate that have a strong affinity for bone hydroxyapatite; these agents inhibit bone resorption by reducing the recruitment and activity of osteoclasts and increasing apoptosis. Bone formed while patients are receiving bisphosphonate treatment is histologically normal. Bisphosphonates have been shown to be effective in decreasing pathologic fractures, bone pain, and the need for radiation therapy in patients with multiple myeloma and metastatic carcinoma to bone. The most effective method of administration is via monthly intravenous infusion. Osteonecrosis of the mandible is sometimes a complication of this treatment. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 57
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?

Explanation
A rotator cuff tear is the most common cause of recurrent instability following a first-time dislocation in patients older than age 40 years. Dislocations occur through a posterior mechanism rather than by an isolated labral avulsion or a Bankart lesion as seen in younger patients. Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40. J Shoulder Elbow Surg 1995;4:416-418.
Question 58
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a

Explanation
The wound described indicates loss of soft tissue directly to the level of the tendon, precluding use of skin grafts if excursion of the tendon is desired. A cross-finger flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb. Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Question 59
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of


Explanation
The radiographs confirm a slipped capital femoral epiphysis of the left hip, as well as a widened growth plate on the contralateral hip. This is considered a stable slip because the patient is able to walk. Treatment options for stable slips include in situ pinning, bone graft epiphysiodesis, and in some centers severe slips are treated with primary osteotomy and epiphyseal fixation. Percutaneous in situ fixation is the most popular and widely used method of treatment. This juvenile patient has an endocrine condition and a widened growth plate on the right side; therefore, strong consideration should be given to pinning the contralateral hip "pre-slip." Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140. Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 60 High Yield
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of

Detailed Explanation
Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability. Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Question 61High Yield
Figures 22a and 22b show the radiograph and sagittal MRI scan of the upper cervical spine of a 62-year-old woman who has had a long history of rheumatoid arthritis. Following hospitalization and skeletal traction, her symptoms improve significantly, her neurologic examination returns to normal, and repeat radiographs show a normal occiput and C1-C2 relationship. Treatment should now include


Explanation
Although opinions differ on whether a decompression is indicated in a patient with symptomatic basilar invagination, it is generally agreed that occipitocervical stabilization is indicated. This has been done with and without concomitant arthrodesis. Crockard HA, Grob D: Rheumatoid arthritis upper cervical involvement, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 701.
Question 62High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 63
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
The patient has a nondisplaced stress fracture of the tarsal navicular. Weight bearing is associated with a high rate of nonunion; therefore, management should consist of immobilization and no weight bearing for 8 weeks. Delayed union or nonunion is treated by excision of sclerotic fracture margins and bone grafting, with or without internal fixation. Generally, CT should be repeated to document healing before permitting a return to sports. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 64
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Vascular invasion, histologically similar to granulation tissue, has been noted between the columns in the zone of hypertrophy, leading to the theory of microtrauma as an etiology. SCFE is also associated with conditions that increase the height of the zone of hypertrophy, including the adolescent growth spurt and endocrinopathies. The perichondral ring has been shown to decrease in thickness with age. Normal undulations in the growth plate also decrease during this time, possibly further destabilizing the physis. Abnormal accumulations of proteoglycan have been reported. Chung SM, Batterman SC, Brighton CT: Shear strength of the human femoral capital epiphyseal plate. J Bone Joint Surg Am 1976;58:94-103.
Question 65
A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of

Explanation
The clinical presentation soon after injury may be surprisingly innocuous, but all high-pressure injection injuries of various materials are best treated by emergent surgical debridement of all foreign material from the flexor tendon sheath as well as the subcutaneous tissues. Subsequent hospital admission, IV antibiotics, and possible repeat debridements usually are necessary. The use of antibiotics alone is inadequate treatment of this severe injury. Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130. Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30. Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72. Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Question 66
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?




Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 67
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?

Explanation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Question 68 High Yield
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Detailed Explanation
When considering the diagnosis of scapholunate ligament injury, standard radiographic views of the hand will not always reveal widening of the scapholunate gap. Although MRI may reveal injury to the ligaments, the PA clenched fist view can be obtained in the office during the initial patient visit. Arthroscopy is not a first-line diagnostic tool. Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
Question 69
A 32-year-old professional football player has disabling left arm pain in the C7 dermatome that has been increasing in severity for the past 2 months. Examination shows a positive Spurling test on the left side, but no changes in motor, sensory, or deep tendon reflexes. Because nonsurgical management has failed to provide relief, he has chosen surgery to allow him to complete his season. The MRI scan and myelogram shown in Figures 19a and 19b show minimal disk bulge, but a root cutoff is noted at the left C7 foramen. Electromyography demonstrates C7 nerve root irritation. Which of the following procedures will best optimize his chances for completing the season?


Explanation
Because the patient has chronic pain, a possible lateral recess stenosis of the C7 root, and no neurologic deficits, keyhole foraminotomy is the treatment of choice for decompressing the exiting nerve root and offering an early return to play, especially when using a muscle-splitting posterior approach. Henderson and associates reported excellent results with posterolateral foraminotomy in patients with radicular symptoms. Although anterior cervical diskectomy and fusion is equally effective in the long term, a period of 6 to 12 weeks is required to allow the anterior fusion to heal prior to a return to play. Chen and associates reported that keyhole foraminotomy maintains cervical motion segment dynamics better than compared to anterior limited diskectomy and foraminotomy or anterior diskectomy with fusion. Henderson, CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512. Dillin W, Booth R, Cuckler J, Balderston R, Simeone F, Rothman R: Cervical radiculopathy: A review. Spine 1986;11:988-991.
Question 70High Yield
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?


Explanation
Synovial herniation pits or Pitt's pits are tumor simulators and are incidentally identified on radiographs obtained for either pain or trauma. The main diagnostic pitfall with this lesion is mistakenly identifying it as an osteoid osteoma. Accurate diagnosis is achieved by knowledge of the location and the characteristic imaging appearance. These are common lesions in individuals with femoroacetabular impingement. Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Question 71High Yield
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Question 72
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?


Explanation
The radiograph reveals bilateral severe acetabular protrusio. The bone scan and history confirm involvement of multiple joints, including the knees and the hindfoot. Although the first four choices can all cause the acetabular protrusio, the associated multiple joint involvement suggests the diagnosis of rheumatoid arthritis. Arthrokatadysis, or primary protrusio acetabuli, is often associated with osteomalacia but not other joint disease. Developmental dysplasia is a common cause of bilateral hip pathology but does not have acetabular protrusio. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, pp 956-957. Wheeless' Textbook of Orthopaedics: Acetabular Protrusio. www.wheelessonline.com/ortho/acetabular_protrusio
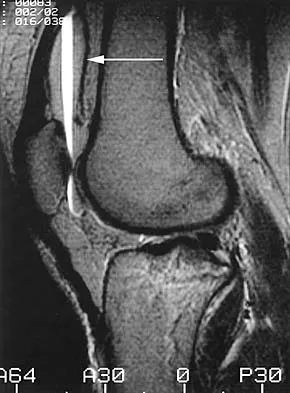
Question 73
The arrow in Figure 11 points toward a finding consistent with which of the following?

Explanation
The finding of a unilateral absent pedicle is often referred to as a winking owl sign and is a manifestation of pedicle destruction from metastatic disease. As the vertebral body is destroyed from the neoplastic process, it extends into the pedicle and destroys the cortical rim that normally creates the oval ring of the pedicle on an AP image. McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Question 74
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
Although the Holstein-Lewis fracture, described as an oblique distal one third fracture, is best known for its association with neurologic injury, radial nerve palsy is most commonly associated with middle one third humeral fractures. Most nerve injuries are neurapraxias or axonotmeses, with up to 90% resolving in 3 to 4 months. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 75 High Yield
What ligament is the primary stabilizer of the wrist following a proximal row carpectomy?

Detailed Explanation
The radioscaphocapitate ligament is the prime stabilizer between the radius and capitate, preventing ulnar translocation of the carpus. Its oblique orientation prevents the carpus from drifting ulnarly. This stout ligament must be protected when excising the scaphoid. Stern PJ, Agabegi SS, Kiefhaber TR, et al: Proximal row carpectomy. J Bone Joint Surg Am 2005;87:166-174.
Question 76
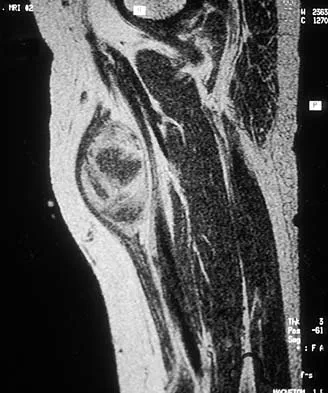
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?





Explanation
The radiographs reveal phleboliths on the volar side of the forearm consistent with hemangioma. The MRI scan reveals a rather well-circumscribed in size, irregular in shape, intramuscular soft-tissue mass in the volar aspect of the distal right forearm within the flexor group musculature. The mass demonstrates heterogeneous mixed signal intensity in both T1- and T2-weighted sequences with increased signal intensity on the T1, suggesting fat within the tumor, typical of hemangioma. The postgadolinium-enhanced sequences demonstrate heterogeneous enhancement. The MRI findings are consistent with a soft-tissue hemangioma. Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Question 77
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
There was no difference observed in the healing of tendon to bone when comparing healing to cortical bone and to a cancellous trough.
Question 78High Yield
What process is often found associated with other neoplasms?
Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 79
What are the most likely symptoms and examination findings related to the mass in zone 2 of Guyon's canal seen in Figure 17?

Explanation
The lesion lies in zone II of the ulnar tunnel. In that zone the deep motor branch of the ulnar nerve is susceptible to compression. Distal to the hook of the hamate, the motor branch of the ulnar nerve dives deep to innervate the interossei as it begins to move from an ulnar to radial direction. Because of its course, it has little or no give in response to a mass effect from the floor of Guyon's canal. Ganglions are the most common cause of ulnar nerve entrapment in the wrist. Lesions in zone I can affect both sensory and motor aspects of the ulnar nerve as well as the motor innervation of the hypothenar muscles. Lesions at the elbow or mid-to-proximal forearm are associated with dorsal hand numbness and tingling. Kuschner SH, Gelberman RH, Jennings C: Ulnar nerve compression at the wrist. J Hand Surg Am 1988;13:577-580.
Question 80
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of

Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 81
What type of metastatic tumor most often has a lytic radiographic appearance?

Explanation
Lung carcinoma most often has a lytic radiographic appearance. Bladder and prostate carcinoma are usually blastic. Breast carcinoma can be both blastic and lytic. Thyroid carcinoma may be difficult to visualize radiographically and may be seen only on MRI scans. Metastatic osteosarcomas typically produce bone. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 82High Yield
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?

Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 83 High Yield
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

Detailed Explanation
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Question 84High Yield
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
When you are employed as a team physician, you are obligated to inform the players and the team organization of all athletically relevant medical issues. This differs significantly from the normal rule of patient confidentiality. If the player came to see you and you were not the team physician, you may not inform the team unless the player so desires. As the team physician, you are not obligated to inform the media. Tucker AM: Ethics and the professional team physician. Clin Sports Med 2004;23:227-241.
Question 85High Yield
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
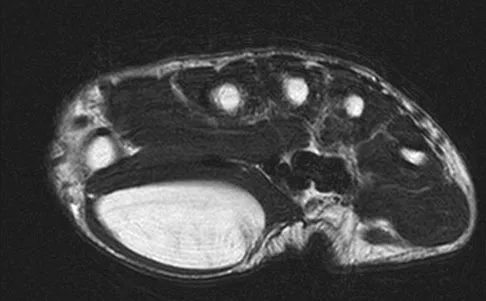
Explanation
The MRI scan shows a large mass (lipoma) in the thenar muscles of the palm. The recurrent motor branch of the median nerve innervates the thenar muscles. The anterior interosseous nerve (AIN) in the proximal forearm innervates the flexor pollicis longus, pronator quadratus, and flexor digitorum pollicis to the index and frequently the middle finger. The terminal branch of the AIN innervates only the wrist capsule. The palmar cutaneous branch of the ulnar nerve is a sensory structure to the hypothenar area. There is no commonly described recurrent branch of the ulnar nerve.
Question 86High Yield
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
After major limb replantation, the occurrence of ischemic rhabdomyonecrosis can result in lactic acidosis and myoglobulinemia. These complications can be limited by rapid repair of the arterial supply, potentially using a shunt before skeletal stability. Repair of the venous system should be performed after repair of the artery. High volume fluid replacement will maintain a diuresis, thus limiting the complications from myoglobulinemia. Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Question 87High Yield
Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
Explanation
There is no difference between the rates of union, malunion, range of motion of the hip or knee, muscle weakness, or infection for the two types of femoral nail insertion. The only difference is the location of the morbidity, which is around the insertion point of the rod. The antegrade technique has more morbidity about the hip, and the retrograde insertion technique has more morbidity about the knee. Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169. Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Question 88High Yield
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
In a study of 52 patients with infected total knee arthroplasties, Windsor and associates showed that the average leukocyte count was 8,300/mm3 and that aspirated knee fluid was positive in all patients except one. Knee radiographs can be unclear in showing infection, which may be present without radiographic signs of loosening. Technetium Tc 99m and gallium bone scans may not conclusively show the presence of infection, particularly in the first 3 years after knee arthroplasty. Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Question 89
In what decade does the peak incidence of conventional osteosarcoma occur?
Explanation
Conventional osteosarcoma most frequently occurs in the second decade, followed by the third decade. Approximately 70% to 75% of patients with osteosarcoma are between the ages of 10 and 25 years. Secondary osteosarcoma (arising in Paget's disease or radiation-induced) is seen in older adults. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Question 90
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 91
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?


Explanation
Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 92High Yield
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?

Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Question 93
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?

Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 94High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature. Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233. Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526. Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Question 95High Yield
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 96 High Yield
Bacitracin is a topical antibiotic agent that may be added to solutions and used for intraoperative lavage. What is this agent effective against?
Detailed Explanation
Bacitracin is a polypeptide obtained from a strain (Tracy strain) of Bacillus subtilis. It is stable and poorly absorbed from the intestinal tract; its only use is for topical application to skin, wounds, or mucous membranes. Concentrations of 500 to 2,000 units per milliliter of solution or gram of ointment are used for topical application. Bacitracin is mainly bactericidal for gram-positive bacteria, including penicillin-resistant staphylococci. In combination with polymixin B or neomycin, bacitracin is useful for suppression of mixed bacterial flora in surface lesions. Bacitracin is toxic for the kidney, causing proteinuria, hematuria, and nitrogen retention; therefore, it has no place in systemic therapy. Bacitracin is said not to induce hypersensivity readily, but reactions to this agent have been described. Rosenstein BD, Wilson FC, Funderburk CH: The use of bacitracin irrigation to prevent infection in postoperative skeletal wounds: An experimental study. J Bone Joint Surg Am 1989;71:427-430.
Question 97High Yield
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
Parvizi and associates studied the 30-day mortality rate after more than 22,000 total knee arthroplasties and found that the rate after bilateral total knee arthroplasty was significantly higher than after unilateral total knee arthroplasty. Aseptic loosening, bleeding, and range of motion have not been shown to be statistically different between patients who had unilateral and simultaneous bilateral total knee arthroplasty.
Question 98
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Internal impingement in the thrower's shoulder occurs in the abducted, externally rotated position as described by Walch and associates. The injury is thought to occur from repetitive contact between the posterosuperior portion of the labrum and glenoid against the articular side of the rotator cuff and greater tuberosity. Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40. Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Question 99High Yield
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of

Explanation
Proximal humeral fractures in children are classified as metaphyseal or Salter-Harris type I or II fractures, and most of these fractures are treated with closed methods. Eighty percent of the growth of the humerus comes from the proximal physis; therefore, tremendous remodeling potential is present. Indications for open reduction include open fractures or severely displaced fractures in adolescents with minimal growth remaining. Acceptable limits of reduction in adolescent proximal humeral fractures include bayonet apposition and angulation of less than 35 degrees. Common blocks to reduction in adolescents include the biceps tendon and periosteum. For this fracture, use of a shoulder sling without reduction will lead to healing and an excellent result as the proximal humerus remodels. Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332. Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372. Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Question 100High Yield
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
