
Score: 0%
Orthopedics Online MCQs
of 100
A 70-year-old otherwise healthy woman is undergoing correction of thoracic kyphosis with spinal cord compression via a posterior approach. She receives an inhaled anesthetic, her mean arterial pressure is 93 mm Hg, and her core temperature is 37.2°C. Her spinal cord is being monitored with somatosensory-evoked potentials and transcranial motor-evoked potentials. She has very low amplitude and increased latency as detected by neurophysiologic monitoring. Which action should be taken?


A 70-year-old otherwise healthy woman is undergoing correction of thoracic kyphosis with spinal cord compression via a posterior approach. She receives an inhaled anesthetic, her mean arterial pressure is 93 mm Hg, and her core temperature is 37.2°C. Her spinal cord is being monitored with somatosensory-evoked potentials and transcranial motor-evoked potentials. She has very low amplitude and increased latency as detected by neurophysiologic monitoring. Which action should be taken?
The anterior interosseous nerve (AIN) originates from the median nerve at what distance from the medial epicondyle:
of 100
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
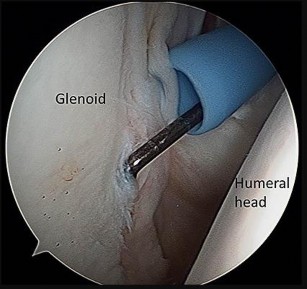
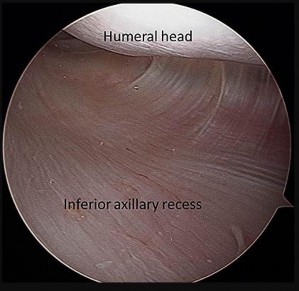
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
A 57-year-old man undergoes total hip arthroplasty, has an uncomplicated early postoperative course, and a normal neurovascular status is documented. However, on postoperative day two he develops a progressive foot drop that increases over the next 24 hours. Postoperative repeat radiographs of the hip arthroplasty are unrevealing. There is no suggestion of swelling of the thigh to suggest a subfascial wound hematoma. What is the next most appropriate step?
During the course of a revision total knee arthroplasty via a medial parapatellar exposure, the surgeon does a complete intra-articular release and synovectomy but exposure is still inadequate. A quadriceps snip is performed and, at the end of the procedure, the knee is stable throughout a range of motion and the postoperative radiographs show acceptable alignment of the components. The patient’s postoperative physical therapy regimen should include which of the following?
-
A 25-yo man sustains the injury shown in Figures 29a and 29b as a result of high-speed trauma. Examination reveals diffuse weakness in the lower extremities that is slightly worse on the right side, and decreased rectal tone and sensation. A CT scan is shown in figures 29c and 29d. Definitive treatment of the injury to the spine is delayed because of a severe pulmonary contusion. At 15 days after the injury, the patient’s neurological status remains unchanged. Management should now consist of

A 25-yo man sustains the injury shown in Figures 29a and 29b as a result of high-speed trauma. Examination reveals diffuse weakness in the lower extremities that is slightly worse on the right side, and decreased rectal tone and sensation. A CT scan is shown in figures 29c and 29d. Definitive treatment of the injury to the spine is delayed because of a severe pulmonary contusion. At 15 days after the injury, the patient’s neurological status remains unchanged. Management should now consist of
The normal values (±2 standard deviations) for kyphosis in the general population of children and adolescents are:
of 100
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?

Which medication has been identified as a risk factor for a nerve injury after shoulder arthroplasty:
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
The most effective method of reducing deep infection in total joint replacement is:
When considering arthroscopiCtreatment of a malunion, what is the procedure most frequently performed:
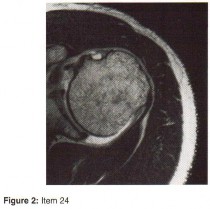
Which gene or protein is the most specific marker of mature osteoblasts but is not expressed by immature, proliferating osteoblasts?
Internal impingement is characterized by which of the following anatomic lesions?

A 28-year-old man has decreased finger proximal interphalangeal (PIP) joint range of motion after open reduction and internal fixation of a proximal phalanx fracture with the use of a side plate. Examination shows greater passive PIP joint flexion with metacarpophalangeal (MP) joint extension, than when the MP joint is flexed. This finding demonstrates contracture/scarring of which of the following structures? ](http://www.orthobullets.com/anatomy/10120/medbullets-onboarding--draft-html)
A 14-year-old girl with a history of multiple food allergies and severe asthma was involved in a motor vehicle accident and sustained an isolated right femur fracture. Which of the following medications is the best choice to control her pain:
During knee arthroscopy, you discover an irreparable complete radial tear of the medial meniscus. After partial medial meniscectomy what should be the primary concern?
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?
A 57-year-old man under workers' compensation underwent a carpal tunnel
2. release 1 year ago and has not returned to work because of numbness and pain.
3. His job requires him to use a rivet gun. The previous carpal tunnel release was
4. performed through a standard incision. Electromyogram and nerve conduction
5. studies are normal; however, conservative treatment, including splinting,
6. stretching exercises, and a steroid injection has failed. Two-point discrimination
7. measures 5 mm in each digit. Management at this time should include
8. 1- observation and possible job retraining.
9. 2- internal neurolysis and coverage of the nerve with silicone sheeting.
10. 3- iontophoresis, fluids therapy, and transcutaneous nerve stimulation.
11. 4- surgical decompression through a standard approach.
12. 5- surgical decompression and coverage of the nerve with a hypothenar fat flap.
2. release 1 year ago and has not returned to work because of numbness and pain.
3. His job requires him to use a rivet gun. The previous carpal tunnel release was
4. performed through a standard incision. Electromyogram and nerve conduction
5. studies are normal; however, conservative treatment, including splinting,
6. stretching exercises, and a steroid injection has failed. Two-point discrimination
7. measures 5 mm in each digit. Management at this time should include
8. 1- observation and possible job retraining.
9. 2- internal neurolysis and coverage of the nerve with silicone sheeting.
10. 3- iontophoresis, fluids therapy, and transcutaneous nerve stimulation.
11. 4- surgical decompression through a standard approach.
12. 5- surgical decompression and coverage of the nerve with a hypothenar fat flap.
A 14-year-old boy is lifting weights and feels a sudden pain in his back, associated with sciatica bilaterally. The sciatica persists for several weeks. The radiograph shown in Figure 7a is negative, and the CT scan shown in Figure 7b is available for evaluation. An MRI scan is read as a disk bulge. Management should consist of

-
Almost 50% of all long-term complications following total knee arthroplasty are due to
Almost 50% of all long-term complications following total knee arthroplasty are due to
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following?
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of**
of 100
Risk for osteonecrosis associated with this injury is most related to
Risk for osteonecrosis associated with this injury is most related to
Which of the following is not a risk factor for fracture of the distal femur proximal to total knee replacement (TKR):
Figures 23a and 23b show the AP and lateral radiographs of the elbow of a 30-year-old professional pitcher. The pathology shown in these studies is most consistent with which of the following conditions?
A 78-year-old community ambulator without assistive devices suffers a displaced femoral neck fracture and is treated acutely with a hemiarthroplasty. He is discharged to a skilled nursing facility, and follows up in your clinic 4 weeks after his surgical date. He brings a report from the physical therapist that states the patient's "Timed up and Go Test" is 11 seconds. This score is predictive of which of the following:
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?


of 100
Figures 96a and 96b are the MRI sections of the symptomatic left knee of a 28-year-old man with left anterior knee pain 18 months after undergoing an allogenic bone marrow transplant for acute myelogenous leukemia. His intraoperative fluoroscopy images are shown in Figures 96c and 96d. What is most critical when obtaining a diagnosis for this patient?


Figures 96a and 96b are the MRI sections of the symptomatic left knee of a 28-year-old man with left anterior knee pain 18 months after undergoing an allogenic bone marrow transplant for acute myelogenous leukemia. His intraoperative fluoroscopy images are shown in Figures 96c and 96d. What is most critical when obtaining a diagnosis for this patient?
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
**Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?









SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
**Question 1 of 100**
Which ligamentous structure attaches to the fracture fragment?
Iontophoresis delivers medications such as analgesics or steroids through the skin using an electrical charge.
Which of the following mutations occurs in patients with spondyloepiphyseal dysplasia with progressive osteoarthropathy:
Which of the following musculoskeletal complications may occur in patients taking fluoroquinolones, such as ciprofloxacin:
A 54-year-old laborer has a 6-month history of lateral elbow pain. An elbow examination reveals full range of motion, tenderness over the lateral epicondyle, and pain with resisted wrist extension with the elbow in extension. Elbow radiograph findings are normal. You perform a steroid injection and the patient's symptoms are decreased 6 weeks later. One year after receiving the injection, this patient—when compared to a patient who did not have a steroid injection—is likely to
Which of the following wear mechanisms is the worst possible situation:
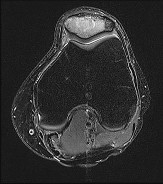
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. Knee range of motion is between 0° and 70°. What is the most appropriate treatment option?
---

---
Management of lateral scapular winging emphasizes strengthening of the
2. 1- deltoid.
3. 2- trapezius.
4. 3- subscapularis.
5. 4- latissimus dorsi.
6. 5- serratus anterior.
2. 1- deltoid.
3. 2- trapezius.
4. 3- subscapularis.
5. 4- latissimus dorsi.
6. 5- serratus anterior.
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed?
of 100
Figures 1 through 3 are the radiographs of a 7-year-old girl who sustained complex orthopaedic injuries falling from an all-terrain vehicle. She underwent successful treatment, which healed all of the injuries with no evidence of avascular necrosis or physeal arrest of the right proximal femur, but complete physeal arrest of the distal femur is noted 12 months post-injury. She returns at age 13 years complaining of leg-length discrepancy (LLD). Bone age is age 13. Based on her predicted leg length discrepancy at maturity, which procedure is most appropriate?

Figures 1 through 3 are the radiographs of a 7-year-old girl who sustained complex orthopaedic injuries falling from an all-terrain vehicle. She underwent successful treatment, which healed all of the injuries with no evidence of avascular necrosis or physeal arrest of the right proximal femur, but complete physeal arrest of the distal femur is noted 12 months post-injury. She returns at age 13 years complaining of leg-length discrepancy (LLD). Bone age is age 13. Based on her predicted leg length discrepancy at maturity, which procedure is most appropriate?
A 15-year-old boy presented with inability to elevate his right shoulder and flex his elbow. He sustained a fall from an all-terrain vehicle 8 weeks ago. He landed on the right shoulder and twisted his neck. Radiographs of the skull, chest, cervical and thoracic spine, and shoulder were normal. There was no loss of consciousness, chest pain, or breathing difficulties. The patient was observed in the hospital until stable and referred for follow-up in the hand clinic at 4 weeks. An electromyelogram (EMG) was scheduled. C linical examination revealed weakness of deltoid, supraspinatus, infraspinatus, teres minor, biceps, brachialis, brachioradialis, and extensor carpi radialis longus. The remainder of his forearm musculature was preserved and he could
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
Diagnosis of the condition is:
grasp, release, and pinch. Sensations were decreased along the distribution of the axillary nerve. There was 3 cm wasting of his arm and 2 cm of the forearm. Tinelâs sign is positive around the clavicle. Hornerâs signs are absent and his arm lies against the body. The EMG report showed fibrillation potentials in the weak muscles. The patient can now flex his elbow. When asked to demonstrate, he flexes his wrist and pronates his forearm to swing his elbow into flexion.
Diagnosis of the condition is:
of 100
The patient’s symptoms fail to improve after a 6-month course of nonsurgical treatment. His inability to return to his full job duties after surgery is most likely related to
The patient’s symptoms fail to improve after a 6-month course of nonsurgical treatment. His inability to return to his full job duties after surgery is most likely related to
A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
An athletic 35-year-old man participates in competitive sports for recreation. During a weight-lifting workout, he described striding forward with his left foot on his flexed right hip. He heard an audible pop and immediately experienced pain in his right hip. Since the injury, he has had difficulty with movement and pain in the right hip. After a week of continued symptoms, he consulted an orthopaedic surgeon who ordered an MRI scan which indicated a partial tear of the right tensor fascia lata and physical therapy was recommended. Specific instructions for the therapist in the initial phase of rehabilitation to prevent hip arthrofibrosis, yet not injure the muscle further, should include which of the following?
Slide 1
A 24-year-old man presents with a short forearm and a hand deformity. The patient is otherwise healthy with no other congenital defects. The clinical appearance of his forearm is shown (Slide). Your diagnosis is:
A 24-year-old man presents with a short forearm and a hand deformity. The patient is otherwise healthy with no other congenital defects. The clinical appearance of his forearm is shown (Slide). Your diagnosis is:
-Etanercept modifies the natural history of inflammatory arthropathies through what mechanism?
of 100
If aspiration findings are negative or equivocal, the diagnosis can be established with
If aspiration findings are negative or equivocal, the diagnosis can be established with
of 100
A 4-week-old girl is referred for an evaluation of her hips. She was the product of a full-term uncomplicated pregnancy. She was delivered by Cesarean section because of breech presentation. She has an older sister treated for developmental dysplasia of the hip (DDH). On examination her hips are stable on Barlow and Ortolani testing. Her primary care practitioner obtained a bilateral dynamic hip ultrasonography. On the ultrasound exam, both hips are stable with stress. The alpha angles are 53°, and there is 48% femoral head coverage. What is the best next step in management?
A 4-week-old girl is referred for an evaluation of her hips. She was the product of a full-term uncomplicated pregnancy. She was delivered by Cesarean section because of breech presentation. She has an older sister treated for developmental dysplasia of the hip (DDH). On examination her hips are stable on Barlow and Ortolani testing. Her primary care practitioner obtained a bilateral dynamic hip ultrasonography. On the ultrasound exam, both hips are stable with stress. The alpha angles are 53°, and there is 48% femoral head coverage. What is the best next step in management?
**FOR ALL MCQS CLICK THE LINK ORTHO****MCQ BANK**
Intermediate doses (650 mg to 4 g/day) inhibit COX-1 and COX-2, blocking prostaglandin (PG) production, and have analgesic and antipyretic effects. Illustration A shows the mechanism of action of aspirin.
InCORRECT Answers: 1,2,4,5: Aspirin does not have any of these mechanisms of action.
725. A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?


























Intermediate doses (650 mg to 4 g/day) inhibit COX-1 and COX-2, blocking prostaglandin (PG) production, and have analgesic and antipyretic effects. Illustration A shows the mechanism of action of aspirin.
InCORRECT Answers: 1,2,4,5: Aspirin does not have any of these mechanisms of action.
725. A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
of 100
Figure 77 shows the CT scan of a 65-year-old Asian man who has been experiencing increasing difficulty using his hands. His handwriting has changed and he feels off balance. What is the most likely cause of his symptoms?

Figure 77 shows the CT scan of a 65-year-old Asian man who has been experiencing increasing difficulty using his hands. His handwriting has changed and he feels off balance. What is the most likely cause of his symptoms?
Which of the following techniques is most commonly used to classify tissue type in soft-tissue tumors?
-
Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Assuming that the fracture shown in this radiograph (Figure


In a diagnostic test, the proportion of individuals who are truly free of a designated disorder identified by the test is known as
Which of the following medications may have a negative effect on bone healing following fracture?
Gene transfer to a cell using viral vectors is called:
A 58-year-old man underwent distal radius ORIF with a volar locking plate yesterday. Preoperatively, he reported some mild sensory disturbances in the volar thumb and index finger, but had 2-point discrimination of 6mm in each finger. Now, he complains of worsening hand pain and sensory disturbances in his volar thumb and index finger. Two-point discrimination is now >10mm in these fingers. Radiographs show a well-fixed fracture in good alignment. What is the most appropriate treatment at this time?
Which of the following is associated with tarsal tunnel syndrome?
of 100
Which 2 things generally need to be present for this injury to occur?
Which 2 things generally need to be present for this injury to occur?
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
The risk of progression with congenital kyphosis is greatest with which of the following?
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
A 13-year-old right-hand dominant pitcher was treated for Little League shoulder. What finding increases his risk of recurrence?
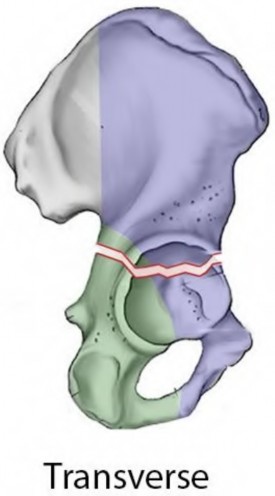
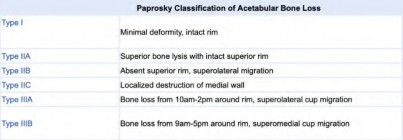
An 80-year-old female presents following a fall from standing. She was an active, independent, community ambulator prior to this event. Past surgical history is significant for a left total hip arthroplasty 10 years prior. A left hip XR is obtained and shown in Figure A. A CT is obtained and demonstrates a displaced transverse acetabulum fracture with medial cup migration. There is no evidence of femoral component loosening or fracture. There is no concern for infection and all inflammatory markers are within appropriate limits. Which treatment is most appropriate?




of 100
A 42-year-old man with an L1 burst fracture, no neurologic deficit, and evidence of disruption of the posterior ligamentous complex as observed on MRI is treated with percutaneous stabilization without fusion.
A 42-year-old man with an L1 burst fracture, no neurologic deficit, and evidence of disruption of the posterior ligamentous complex as observed on MRI is treated with percutaneous stabilization without fusion.
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
A 20-year-old healthy female endurance athlete has lower leg pain and dorsal foot paresthesias after
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
**Baseline**
**1 Minute**
**5 Minutes**
---|---|---|---
**Anterior**
7
32
25
**Lateral**
8
29
23
**Superficial Posterior**
12
25
17
**Deep Posterior**
14
22
16
The patient decides to pursue surgical intervention. Which compartments should be released?
running for 30 minutes. She has seen another physician and has been ruled out for a bone stress injury. She has tried extensive nonsurgical measures such as shoe modification and an extended period without running. You suspect chronic exertional compartment syndrome and perform intramuscular compartment pressure measurements at three separate time points with the following results:
**Baseline**
**1 Minute**
**5 Minutes**
---|---|---|---
**Anterior**
7
32
25
**Lateral**
8
29
23
**Superficial Posterior**
12
25
17
**Deep Posterior**
14
22
16
The patient decides to pursue surgical intervention. Which compartments should be released?
of 100
A 73-year-old man goes to the emergency department after tripping and falling down roughly thirteen steps at home. Prior to the injury, the patient had well-controlled medical comorbidities and was independent with all activities of daily living. Figures 1 through 3 show the injury sustained by the patient. What is the most appropriate definitive treatment for this patient?

A 73-year-old man goes to the emergency department after tripping and falling down roughly thirteen steps at home. Prior to the injury, the patient had well-controlled medical comorbidities and was independent with all activities of daily living. Figures 1 through 3 show the injury sustained by the patient. What is the most appropriate definitive treatment for this patient?
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Hand and wrist: MCQ AND EMQ Questions
MCQs
MCQs
Optimal treatment for a symptomatic ganglion is:
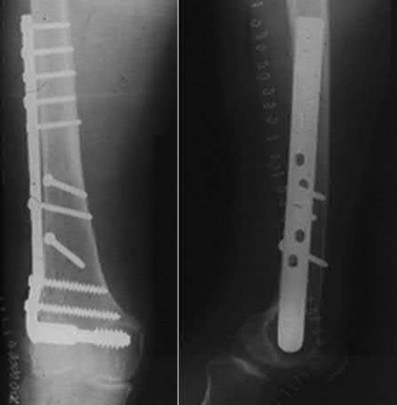
Fixed-angle implants are often used for fixation of distal femur fractures. Three commonly used implants (Implants A, B and C) are shown in Figures A, B and C respectively. Which of the following statements is true reagarding these implants?


of 100
Reconstruction of the structure injured in Figures 65a and 65b is important to limit which pattern of instability?
Reconstruction of the structure injured in Figures 65a and 65b is important to limit which pattern of instability?
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?
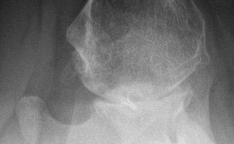
Figure 1 shows a current AP radiograph of the elbow of a 12-year-old high
2. school pitcher who has pain and restricted motion, especially in extension.
3. Physical therapy has failed to relieve the symptoms. Treatment should now
4. include
5. 1- continued physiotherapy.
6. 2- manipulation under anesthesia.
7. 3- debridement with osteochondral allograft replacement of the defect.
8. 4- arthroscopy and possible open debridement.
9. 5- arthroscopy, bone graft, and arthroscopic fixation of the fragment.
2. school pitcher who has pain and restricted motion, especially in extension.
3. Physical therapy has failed to relieve the symptoms. Treatment should now
4. include
5. 1- continued physiotherapy.
6. 2- manipulation under anesthesia.
7. 3- debridement with osteochondral allograft replacement of the defect.
8. 4- arthroscopy and possible open debridement.
9. 5- arthroscopy, bone graft, and arthroscopic fixation of the fragment.
of 100
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis. The surgery is uncomplicated. What is the most common indication for future revision?
A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis. The surgery is uncomplicated. What is the most common indication for future revision?
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
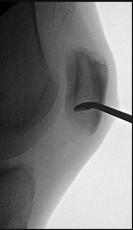
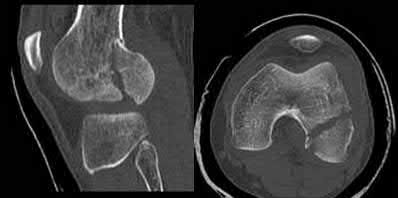
A 10-year-old boy tripped as he was running down a hill, felt a painful pop in his right knee, and was unable to bear weight on the involved lower extremity. Examination reveals a tense effusion and an extensor lag of the right knee. Figures 36a and 36b show AP and lateral radiographs. Management should consist of
Glomus tumors are characterized by all of the following except:
"C ollar button" abscess refers to:
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after
primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to
3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1%
neutrophils. No growth of organisms is seen on routine culture. What is the best next step?
A 33-year-old woman with a history of a traumatic fall onto her wrist and tenderness over the scapholunate (SL) interval presents to the clinic. Radiographs are normal, and magnetic resonance imaging reveals a partial tear of the SL ligament. The remaining wrist ligaments are normal. If conservative therapy is attempted, then it should consist of:
of 100
The patient is treated by another physician and undergoes the procedure shown in Figures 40a and 40b. She currently cannot stand upright. Spinopelvic measurements reveal her pelvic incidence to be 85 degrees and pelvic tilt to be 40 degrees. Her lordosis from T12-S1 is 35 degrees. Which additional surgical procedure should be considered?
40A
B

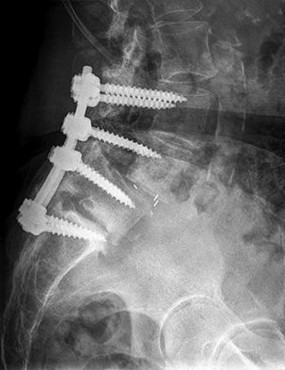
The patient is treated by another physician and undergoes the procedure shown in Figures 40a and 40b. She currently cannot stand upright. Spinopelvic measurements reveal her pelvic incidence to be 85 degrees and pelvic tilt to be 40 degrees. Her lordosis from T12-S1 is 35 degrees. Which additional surgical procedure should be considered?
40A
B
The single most important criterion to identify the type of hip implant for future analysis in a hip arthroplasty register is:
of 100
During a medial approach to the hip, which anatomic structure identified in the figures can help surgeons locate the true acetabulum?
During a medial approach to the hip, which anatomic structure identified in the figures can help surgeons locate the true acetabulum?
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. This patient elects nonsurgical treatment and later experiences persistent instability. Examination reveals an asymmetric Dial test finding and a varus thrust during ambulation. Which osteotomy and correction appropriately addresses this chronic instability pattern?
---

---
The most common forearm deformity in patients with hereditary multiple osteochondromatosis is:
You are asked to consult on a 4-day-old neonate admitted because of failure to thrive. She has swelling of her left shoulder. Examination reveals limited motion of her hips and left shoulder. Radiographs of the shoulder and pelvis are negative. Laboratory studies show a WBC count of 24,000/mm3, an erythrocyte sedimentation rate of 50/h, and C-reactive protein is 16.4. What is the next most appropriate step in management?
Patients treated with zoledronic acid within 90 days of a hip fracture, followed up with annual treatment, will most likely show:
Which of the following is not a common finding in cloacal exstrophy:
Which of the following surgical options after resection of a sarcoma about the knee would require a patient to expend the greatest amount of energy while walking?
of 100 A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?

Keywords