Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?

Explanation
The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg's syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers. Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Question 2
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
Intrafocal pinning allows the Kirschner wires to be placed through a site of comminution and then drilled through intact cortex. Generally Kapandji intrafocal pinning is done for dorsal comminuted extra-articular dorsal bending fractures, but it also may be used to elevate and buttress radial comminution. Simple intra-articular fractures can also be treated with pinning alone. Intrafocal pinning works best as a dorsal or radial buttress to prevent shortening. When there is volar comminution, the fracture is prone to shortening and supplemental external fixation or plating is recommended. Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394. Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Question 3
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 4High Yield
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
EIP transfer results in no functional deficit. If the tendon is cut proximal to the sagittal band, there will be no extensor deficit. Browne EX, Teague MA, Snyder CC: Prevention of extensor lag after indicis proprius transfer. J Hand Surg Am 1979;4:168-172.
Question 5
A 55-year-old woman undergoes an anterior cervical diskectomy and fusion at C5-C6 through a left-sided approach. One year later, she requires an anterior cervical diskectomy and fusion on another level. Which of the following is considered a contraindication to performing a right-sided approach for the revision procedure?
Explanation
When attempting a revision anterior cervical approach from the side opposite the original approach, it is important to evaluate the function of the vocal cords. If this evaluation reveals dysfunction of the vocal cord on the side of the original approach, then an approach on the contralateral side should not be attempted. Injury to the stellate ganglion, which causes a Horner's syndrome, should not preclude an approach on the contralateral side. While the side of the symptomatology can influence the surgeon's choice as to the side of an anterior approach, it does not preclude a certain approach. When approaching the lower cervical spine from the right side, the recurrent laryngeal nerve can cross the surgical field and should be preserved. Excessive intraoperative pressure on the esophagus can increase the incidence of dysphagia, but its incidence is no different with either approach. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 387-394.
Question 6
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of
Explanation
Following a CVA, the muscular imbalance often leads to a fixed contracture of the shoulder in adduction, internal rotation, and flexion. The responsible muscles include the pectoralis major, subscapularis, teres major, and latissimus dorsi. If stretching cannot produce enough improvement for axillary hygiene, then surgery is an option. If the shoulder resists external rotation during examination with the arm at the side, as in this patient, then the subscapularis is spastic and contributing to the deformity as well and needs to be released along with the pectoralis. Phenol nerve blocks are most effective and best given within 6 months of the initial CVA to be effective. Lidocaine blocks may be helpful in determining whether a deformity is caused by a fixed soft-tissue contracture or by spasticity but play no role once the contracture is present. The modified L'Episcopo procedure is indicated in patients with contracture secondary to brachial plexus birth palsies. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 7 High Yield
A 7-year-old boy sustained a 2-cm laceration to the anterior aspect of his left knee after falling on a rock. Examination reveals that the joint surface is not visible through the wound. Radiographs show no evidence of a foreign body or free air in the joint. Management should consist of

Detailed Explanation
The possibility of an open joint injury should be considered in any patient who has a small periarticular laceration. Failure to promptly diagnose and treat such injuries may lead to septic arthritis. The diagnosis of an open joint is easily made when there is visible communication of the joint through the traumatic wound, or when intra-articular air is present on a radiograph. In the absence of these findings, the diagnosis of an open joint may be established by the saline load test, in which a volume of saline is injected into the joint under sterile conditions. If fluid extravasates through the traumatic wound, the diagnosis of an open joint is established. Voit and associates used a saline load test in 50 patients with periarticular lacerations suggestive of joint penetration. When they compared the clinical prediction of whether or not the laceration had penetrated the joint and the test results, the authors reported a false-positive clinical result in 39% of patients and a false-negative clinical result in 43%. The authors concluded that the saline load test was valuable in evaluating periarticular lacerations. Voit GA, Irvine G, Beals RK: Saline load test for penetration of periarticular lacerations. J Bone Joint Surg Br 1996;78:732-733.
Question 8
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Question 9 High Yield
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include

Detailed Explanation
Bilateral flattening of the femoral heads suggests multiple epiphyseal dysplasia; therefore, a skeletal survey is indicated to look for involvement of other epiphyses. Unilateral flattening of the femoral head would suggest Legg-Perthes disease. Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Question 10 High Yield
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?

Detailed Explanation
The eccentric metaphyseal location, skeletal maturity, narrow zone of transition, and lack of symptoms suggest a benign process and are consistent with a healed nonossifying fibroma. These lesions typically fill in (ossify) with skeletal maturity, eventually remodeling and disappearing. Radiographic monitoring is indicated. Biopsy is not recommended unless the lesion changes radiographically. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393. Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Question 11
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 12
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?

Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 13
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show

Explanation
The radiograph shows the correct tibial tunnel and anterior femoral tunnel; therefore, range of motion will most likely show loss of flexion. Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin Sports Med 1999;18:109-171.
Question 14
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 15 High Yield
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to


Detailed Explanation
The radiograph shows a fracture distal to the prosthesis in a stable, apparently well-fixed prosthetic stem. The well-fixed prosthesis-bone composite is stiff, creating a modulus mismatch between the proximal and distal femur. Therefore, the risk of fracture, particularly in osteoporotic bone, is increased at this level. Revision of the stem to a longer construct is unnecessary, and standard plate and screw fixation has been shown to yield union rates of greater than 90%. Nonsurgical treatment of fractures distal to the tip of the prosthesis results in high nonunion rates, reported to be from 25% to 42%. Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 16
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 17
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?


Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 18
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 19High Yield
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?



Explanation
The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 20
Figure 47 shows a transverse MRI scan of a patient's left shoulder. The findings reveal which of the following abnormalities?

Explanation
The MRI scan shows a defect in the posterior aspect of the humeral head, commonly referred to as a Hill-Sachs lesion. This is an impaction fracture of the humeral head that occurs during anterior shoulder dislocation. The abnormality on this image is an irregularity of the posterior humeral head; the humeral head otherwise has a homogenous appearance. The coracoid, subscapularis, and posterior labrum are normal. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 21 High Yield
When treating thoracolumbar spine fractures, which of the following is considered the major advantage of using a thoracolumbosacral orthosis (TLSO) when compared to a three-point fixation brace (Jewett)?

Detailed Explanation
When treating thoracolumbar spine fractures, the major advantage of using the TLSO is greater rotational control. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 347-349. Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA: Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am 1986;17:161-170.
Question 22High Yield
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable. Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Question 23High Yield
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 24High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 25
Based on the diagram shown in Figure 16, what muscle derives its innervation from the nerve identified by the letter "A"?

Explanation
The nerve labeled A is the axillary nerve, a branch from the posterior cord. The posterior cord innervates the subscapularis, latissimus dorsi, teres major and minor, deltoid, triceps, anconeus, brachioradialis, and extensors of the forearm. The axillary nerve innervates the teres minor and deltoid. The pectoralis minor is innervated by the medial cord. The supraspinatus and the subclavius are innervated by the superior trunk. The brachialis is innervated by the lateral cord. Moore K: Anatomy, ed 3. Philadelphia, PA, Williams and Wilkins, 1992.
Question 26
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?

Explanation
Posttraumatic osteolysis of the distal portion of the clavicle is a condition that can be a complication of acute or repetitive trauma. The distal end of the clavicle is frayed and resorbed. Resorption may occur after weeks or months. The end of the clavicle may reconstitute over a period of months, or the acromioclavicular joint may remain widened. The differential diagnosis for distal clavicular erosion also includes rheumatoid arthritis, hyperparathyroidism, neoplastic destruction, cleidocranial dysplasia, and pyknodysostosis. Acutely, a type 2 acromioclavicular joint injury does not result in erosion or resorption of the clavicle. Periosteal sleeve injuries radiographically mimic acromioclavicular joint dislocation. Rickets occurs only in childhood.
Question 27
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
The first extensor compartment of the wrist typically contains a single extensor pollicis brevis tendon and the abductor pollicis longus tendon that nearly always has multiple tendon slips. The extensor pollicis brevis tendon is frequently found to be separated from the slips of the abductor pollicis longus tendon by an intracompartmental septum. During surgery, this septum must be divided to complete the release of the compartment. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Question 28
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site. Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 29
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 30
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 31
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 32High Yield
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation. Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 33High Yield
A patient who is an observant Jehovah's Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?

Explanation
Jehovah's Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah's Witnesses will accept the use of a cell saver in a "closed circuit." Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 34High Yield
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?

Explanation
The child has a near complete central physeal arrest of the distal femur and worsening limb-length discrepancy will develop. She is growing at the average rate for the population. The distal femoral physis grows at a rate of roughly 9 mm per year. Girls finish their growth at approximately age 14 years. Thus, at maturity the left leg will be 6.4 cm longer than the right. An angular deformity has not developed at this point and her arrest is central; therefore, angular deformity is unlikely to develop in any plane. Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Question 35
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of

Explanation
The patient has a chondroblastoma of the proximal humerus; therefore, the treatment of choice is curettage and bone grafting. Surgical resection of the proximal humerus is not indicated in the initial treatment of an intraosseous chondroblastoma. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
Question 36High Yield
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?

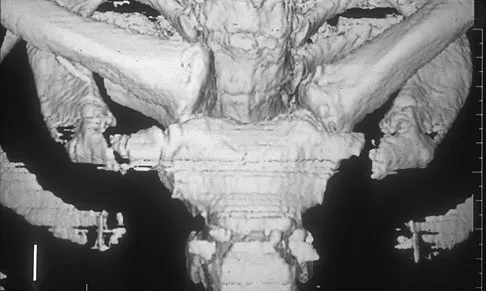
Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 37
What term best describes the process involved when a growth factor produced by an osteoblast stimulates the differentiation of an adjacent undifferentiated mesenchymal cell during fracture repair?
Explanation
Growth factors are proteins secreted by cells that can act on target cells to produce certain biologic actions. These actions can be described as autocrine, paracrine, and endocrine. Autocrine actions are those in which the growth factor influences an adjacent cell of its origin or identical phenotype. Paracrine actions are those in which the protein influences an adjacent cell that is different in its origin or phenotype. Endocrine actions are those in which the factor influences a cell located at a distant anatomic site. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Question 38High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?

Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44. Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Question 39High Yield
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
Developmental dislocation of the radial head most frequently presents as a painless mass over the posterior aspect of the elbow. Patients do not have feelings of elbow subluxation but may report pain or clicking. Limitation of motion is most frequently found in the pronation and supination arc rather than in flexion and extension. Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.
Question 40
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
A muscle that lengthens as it is activated is an eccentric contraction. Isometric contraction involves no change in length. Concentric contraction occurs while the muscle is shortening. In isotonic contraction, the force remains constant through the contraction range. Isokinetic muscle contraction occurs at a constant rate of angular change of the involved joint. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 12-13.
Question 41High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion. Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 42
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?


Explanation
The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future. Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Question 43 High Yield
When counseling a patient with hypophosphatemic rickets, which of the following scenarios will always result in a child with the same disorder?
Detailed Explanation
Hypophosphatemic rickets is an inherited disorder that is transmitted by a unique sex-linked dominant gene. Therefore, if a male patient has a female offspring, his affected X chromosome will be transmitted and all of his female children will have hypophosphatemic rickets. All male offspring of a male patient will be unaffected. All offspring of a female patient have a 50% chance of having the disorder. Understanding the inheritance of hypophosphatemic rickets facilitates early diagnosis and early treatment. Medical treatment with phosphorus and some types of vitamin D (most authors recommend calcitriol) improves, but does not fully correct, the mineralization defect in hypophosphatemic rickets. However, if medical treatment is begun before the child begins walking, the growth plate is then adequately protected and a bowleg deformity will most likely be prevented. Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Question 44
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?


Explanation
Turf toe occurs in collision and contact sports in which the athlete pushes off to accelerate or change direction and there is hyperextension of the great toe MTP joint. Typically, there is also axial loading of the posterior hindfoot, which increases the hyperextension of the MTP joint. The most common presentation is pain and swelling of the MTP joint and inability to hyperextend the joint without significant symptoms. With significant force, fractures of the sesmoids and plantar soft tissues can occur. The radiographs do not show a dislocation of the great toe MTP joint because it is concentrically located on both radiographs. However, the radiographs show a fracture of the lateral sesamoid or a diastasis of a bipartite lateral sesamoid. The medial sesamoid is also proximal indicating a rupture of the plantar (volar) plate. Therefore, the most likely diagnosis is a fracture of the lateral sesamoid with rupture of the plantar plate leading to proximal migration of the proximal fragment of the lateral sesamoid and the medial sesamoid. Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
Question 45
A 52-year-old woman who is right hand-dominant sustains an injury to her elbow in a fall. A radiograph is shown in Figure 60. The preferred treatment of this injury pattern should include

Explanation
The patient has a Bado type 2 variant Monteggia fracture with a radial head fracture. The type 2 variant is associated with a higher nonunion rate and poorer outcomes compared to other Bado-type Monteggia fractures. While it is potentially acceptable to repair the radial head, factors such as higher degrees of comminution and older age lead toward replacement as the treatment of choice. Plate and screw fixation is favored over Kirschner wire/tension band fixation because this is not a simple olecranon fracture. Plate placement in a type 2 fracture is dorsal to counteract very high tensile forces associated with fixation failure. Egol KA, Tejwani NC, Bazzi J, et al: Does a Monteggia variant lesion result in a poor functional outcome? A retrospective study. Clin Orthop Relat Res 2005;438:233-238. Jupiter JB, Leibovic SJ, Ribbans W, et al: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 46
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?

Explanation
Femoral acetabular impingement (FAI) is a pathologic entity leading to pain, reduced range of motion in flexion and internal rotation, and development of secondary arthritis of the hip. There are two types of FAI: cam impingement and pincher impingement. Cam impingement is seen when a nonspherical femoral head produces a cam effect when the prominent portion to the femoral head rotates into the joint. This mechanism produces shear forces that damage articular cartilage. Radiographs reveal early joint degeneration and flattening of the head neck junction (the so-called "pistol grip deformity") as seen in this image. The pincher type of impingement involves abnormal contact between the femoral head neck junction and the acetabulum, in the presence of a spherical femoral head. Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
Question 47
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?

Explanation
Studies have shown that when compared with fixation to the sacrum alone, the success rate of fusion across the lumbosacral junction increases when both the sacrum and ilium are included in the posterolateral construct. Curve correction, coronal balance, and pelvic balance are all attended to within the thoracolumbar spine and are not directly related to the pelvic fixation. Fretting and corrosion are a byproduct of metal-to-metal connections. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
Question 48High Yield
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T2-weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of



Explanation
The initial signs and symptoms of acute hematogenous osteomyelitis vary widely but usually include fever, bone pain, and impaired use of the involved extremity. In lower extremity infections, the child may limp or refuse to walk. Examination often reveals bone tenderness. In more advanced cases, erythema, warmth, and swelling may be present. The WBC and neutrophil counts are not always elevated, but the erythocyte sedimentation rate will be abnormal in more than 90% of patients. When the infection is diagnosed early, before a subperiosteal abscess has formed, antibiotics alone may be adequate to treat the infection. This patient has a more advanced infection, however, with the MRI scan revealing a subperiosteal abscess that was confirmed by aspiration. When an abscess is present, surgical drainage is generally indicated to remove devitalized tissue and to enhance the efficacy of the antibiotics. Further studies, such as bone or indium scans, are not necessary and will delay definitive treatment. Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Question 49High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?

Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Question 50
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 51High Yield
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?



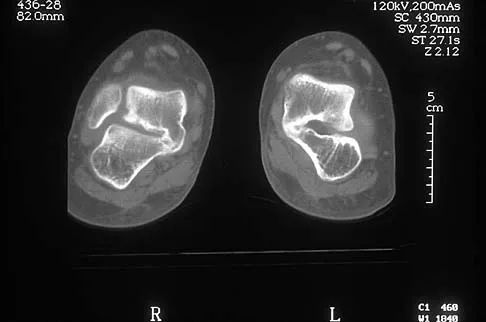
Explanation
The axial views show fusion of the talus and calcaneus at the medial facet (talocalcaneal coalition). Peroneal spastic flatfoot is a descriptive term applying to the symptoms of painful flatfoot associated with apparent peroneal spasm and is sometimes caused by tarsal coalition; however, this is not the most appropriate diagnosis for this patient. Flexible flatfoot with a short Achilles tendon often causes symptoms similar to the ones listed above, but subtalar motion should be normal. A diagnosis of calcaneonavicular coalition can be made based on plain oblique views of the foot but is not seen in these views. Posterior tibial tendon dysfunction in the absence of other pathology is uncommon in children. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 52 High Yield
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of


Detailed Explanation
The complications of femoral neck fractures in children include osteonecrosis, malunion, nonunion, and premature physeal closure. It is presumed that the risk of osteonecrosis is directly related to the amount of displacement at the time of injury and is not affected by the type of treatment. The risk of the other complications can be decreased depending on the type of treatment. Anatomic reduction by either closed or open methods can reduce the risk of malunion. The addition of internal fixation allows for maintenance of the reduction. In young children who cannot comply with a partial or non-weight-bearing status, the addition of a spica cast gives added protection. Canale ST: Fractures of the hip in children and adolescents. Orthop Clin North Am 1990;21:341-352.
Question 53 High Yield
A 75-year-old woman began a walking program 2 months after undergoing right total knee arthroplasty. She had to stop the program after 4 weeks because of hindfoot pain and ankle swelling. Radiographs are shown in Figures 42a and 42b. What is the most likely diagnosis?


Detailed Explanation
It is often tempting to assign a diagnosis of plantar fasciitis in patients with hindfoot pain. In this patient, the radiographs confirm a diagnosis of a calcaneal insufficiency fracture. The dense condensation of bone on the lateral view confirms the diagnosis. There is no radiographic evidence of a heel spur, osteochondral lesions, or chondrocalinosis. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 2591. Kearon C: Natural history of venous thromboembolism. Semin Vasc Med 2001;1:27-37.
Question 54
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?

Explanation
The MRI scan shows increased signal intensity along the deep fibers of the supraspinatus near its insertion. This is typical of tendinosis and a probable partial-thickness rotator cuff tear. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 55High Yield
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by

Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Question 56High Yield
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 57 High Yield
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Detailed Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 58 High Yield
Which of the following antibiotics is contraindicated in children?
Detailed Explanation
The tetracycline family of medications can stain teeth and bone in skeletally immature patients and as a result should be avoided in those patients. The remaining antibiotics have no known specific contraindication to use in children.
Question 59 High Yield
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?


Detailed Explanation
The radiographs show narrowing of the medial joint space, which indicates polyethylene wear and progressive varus alignment. Wear particles incite osteolytic lesions like the one seen on the lateral radiograph. O'Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Question 60
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 61 High Yield
What is the most common behavioral effect of anabolic steroid use in athletes?
Detailed Explanation
Users of anabolic steroids often display increased feelings of hostility and aggression. Although reports of psychotic, depressive, and manic behavior have been reported with the use of steroids, they are rare. Drug dependence, such as seen with narcotics, is not a feature of steroid use. Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Question 62
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of


Explanation
Lacerated radial nerves are associated with open humeral fractures. All open humeral fractures with radial nerve palsy should be managed with radial nerve exploration and skeletal stabilization. Closed humeral fractures with associated radial nerve palsy usually have an intact nerve with neurapraxia. Most of these patients recover without surgical treatment. If the patient has multiple injuries, skeletal stabilization may be indicated to improve mobilization. For an isolated closed humeral fracture with a radial nerve palsy, the treatment of choice is splinting for 1 to 2 weeks, followed by a humeral fracture brace. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Question 63
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 64High Yield
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the

Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 65
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?


Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 66
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?






Explanation
The radiograph demonstrates thickened trabeculae and thickened cortices in the left proximal femur compared to the right, and the bone scan shows increased uptake in this area. The MRI scans show thickened trabeculae with normal marrow signal. These findings are diagnostic of Paget's disease. Medical treatment, including bisphosphonates and calcitonin, is indicated for painful bone lesions. Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget's disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Question 67High Yield
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Question 68
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?

Explanation
Findings in patients with McCune-Albright syndrome include polyostotic fibrous dysplasia, multiple cafe-au-lait spots, and precocious puberty. The bone changes in NF-1 resemble nonossifying fibromas, not fibrous dysplasia. NF-2 has little bony change with typical ocular abnormalities. Paget's disease occurs in older individuals and does not present with cafe-au-lait spots. Ollier's disease (multiple enchondromatosis) may show bone changes but not the other findings. Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746. Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Question 69High Yield
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of

Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Question 70
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?

Explanation
The ulnar nerve is more prone to neuropathy than the radial or median nerves for many reasons. It has the greatest longitudinal excursion required to accommodate elbow range of motion, subjecting it to potential traction forces. The dimensions of the entrance of the cubital tunnel change with elbow motion, potentially causing compression in flexion. For these two reasons, the ulnar nerve is subjected to both compression and traction during elbow motion. Although it passes between two muscle heads as it enters the forearm, so do the median and radial nerves. Finally, the vascular supply is adequate because of the anastamoses between the superior ulnar collateral artery, the posterior ulnar recurrent artery, and the inferior ulnar collateral artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 369-378. Prevel CD, Matloub HS, Ye Z, Sanger JR, Yousif NJ: The extrinsic blood supply of the ulnar nerve at the elbow: An anatomic study. J Hand Surg Am 1993;18:433-438.
Question 71
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?




Explanation
Multiple hereditary exostosis and enchondroma commonly present as multiple lesions in the hand. Multiple hereditary exostosis consists of cartilage capped bony exostoses arising from the metaphyseal end of rapidly growing bones. Osteosarcoma and chondrosarcoma rarely appear as multiple lesions. Fracture callus can exhibit enchondral ossification that is usually circumferential, but the radiographic findings are not consistent with fracture. Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Question 72
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?


Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 73High Yield
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 74
A 10-year-old boy has a painful thigh mass. A radiograph, MRI scan, and biopsy specimen are shown in Figures 42a through 42c. What is the most likely diagnosis?



Explanation
A destructive mixed lytic and blastic metaphyseal lesion with a large soft-tissue mass in an adolescent is most likely an osteosarcoma until proven otherwise. The epicenter of the tumor is on the surface of the bone, most likely involves the periosteum, and is more likely to be chondroblastic in nature. Parosteal osteosarcoma is a low-grade tumor, much more radiodense, usually smaller, and found in the posterior distal femur of middle-aged patients. Chondrosarcomas are distinctly rare in childhood.
Question 75
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
A superior labrum, when intact, stabilizes the shoulder by increasing its ability to withstand excessive external rotational forces by an additional 32%. The presence of a SLAP lesion decreases this restraint and increases the strain in the superior band of the inferior glenohumeral ligament by over 100%. Rodosky MW, Harner CD, Fu FH: The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med 1994;22:121-130.
Question 76
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of

Explanation
The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Question 77High Yield
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?

Explanation
The prognosis of Legg-Perthes disease in children younger than age 6 years is good. There is no indication that surgical treatment will improve the outcome. Range-of-motion exercises to prevent contracture may be helpful. Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Question 78
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?

Explanation
The patient has a fixed deformity of the hindfoot and an Achilles tendon contracture; therefore, the treatment of choice is triple arthrodesis with Achilles tendon lengthening. Further bracing will not be helpful. Amputation is not indicated, and ankle arthrodesis will not address the hindfoot deformity. Palliative management would be more appropriate if the knee was unstable or the quadriceps were weak, because the equinus balances the ground reaction force across the knee. Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
Question 79 High Yield
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of

Detailed Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 80High Yield
Which of the following anatomic structures is labeled 6 in Figure 27?
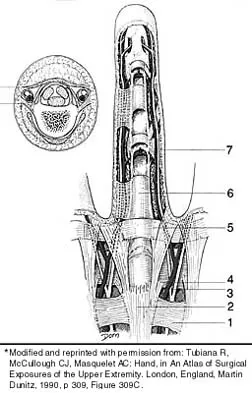
Explanation
The line labeled 6 points to the A2 pulley. This structure is the condensation of the digital flexor tendon sheath corresponding to the proximal aspect of the proximal phalanx. Grayson's ligament is volar to the digital nerve and artery. Cleland's ligament is dorsal to the digital nerve and artery. The sagittal band anchors the extensor tendons over the metacarpophalangeal joints. The triangular ligament connects the lateral bands just proximal to the terminal tendon inserting onto the base of the distal phalanx. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Question 81
Figures 21a and 21b show the radiograph and CT scan of a 14-year-old patient with thigh pain. The next most appropriate step in management should consist of


Explanation
The radiographs show increased density and reactive bone formation. A faint nidus can be seen on the radiograph but is obvious on the CT scan. The initial therapy for an osteoid osteoma should be oral anti-inflammatory drugs. A biopsy or SPECT bone scan is not indicated because the osteoid osteoma is clearly seen on the CT scan. If the patient fails to respond to nonsurgical therapy, CT-guided radiofrequency ablation or surgical excision is indicated depending on the anatomic location. Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 82
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?

Explanation
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%. McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 83
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of

Explanation
Answering this question requires understanding of two important biomechanics concepts. First, because neither the object being held in the hand nor the body is moving and, hence, their accelerations are zero, the problem is one of static equilibrium in which the sum of the moments acting on the body is zero. Second, a moment is the action of a force that causes an object to rotate about any point away from its line of action. The magnitude of the moment is the magnitude of the force multiplied by the perpendicular distance between the line of action and the point (often called the moment arm or lever arm). In this problem, two forces are causing moments about the elbow. The magnitude of the moment caused by the object in the hand is 5 N times 30 cm or 150 N-cm. To maintain equilibrium, the moment caused by the biceps force must also have a magnitude of 150 N-cm. Its moment arm is 2 cm, so the magnitude of the biceps force is 150 N-cm divided by 2 cm, which equals 75 N. In general, functional loads such as the object are always at a mechanical advantage (ie, have a longer moment arm) over the muscle. Therefore, muscles must generate large forces to overcome the moments caused by even small functional loads. An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
Question 84
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of

Explanation
The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper's injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach. Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Question 85 High Yield
What is the most common bone tumor in the hand?

Detailed Explanation
The most common bone tumor in the hand is an enchondroma. Forty-two percent of these lesions occur in the small tubular bones. They frequently present with a fracture in these locations. Fractures are usually treated nonsurgically. Indications for surgery include patients with symptomatic lesions or those who are considered high risk for recurrent fracture. The histologic appearance of an enchondroma in the hand is more cellular than enchondromas found in the long bones. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 103.
Question 86 High Yield
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?


Detailed Explanation
In an atrophic nonunion with a good soft-tissue envelope, adequate plating with cancellous bone graft can be used to span defects of up to 6 cm. Cortical graft from the fibula or iliac crest is not necessary. BMP-7 is a bone graft substitute and should not be used alone in this patient because the hardware is loose.
Question 87
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Knee pain and swelling in the first week after ACL reconstruction is usually related to a postoperative hemarthrosis. A large hemarthrosis creates capsular distension, which inhibits active quadriceps contraction by a neurologic reflex, the H. reflex. Kennedy and associates reported that an experimentally induced knee effusion at 60 mL was found to result in profound inhibition of reflexly evoked quadriceps contraction. Removal of the hemarthrosis by aspiration will improve strength and often instantaneously restore the ability to contract the quadriceps muscle. A large effusion will also limit knee flexion. EMG and NCVS are not necessary unless there is a high index of suspicion of a femoral neuropathy. Diagnostic ultrasonography is not necessary in this patient but can be useful in the assessment of patellar tendon integrity. MRI is not indicated and would most likely be limited by artifact and postoperative changes. Continuous passive motion is not indicated and would most likely worsen the patient's symptoms. Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Question 88
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?

Explanation
It is generally accepted that reconstructions of the proximal tibia are associated with the highest incidence of failure, probably because of poor soft-tissue coverage, the need for extensor mechanism reconstruction, and other anatomic issues. It also may be related to the fact that patients with tumors of the proximal tibia, in general, have a better prognosis and better survival rates than patients with tumors located elsewhere in the body. Reconstructions of the proximal humerus may be more durable because they are not involved in weight-bearing activities.
Question 89High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of


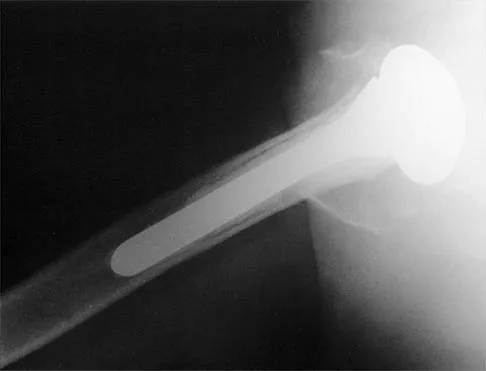
Explanation
Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Question 90
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
Nonsurgical management is considered for proximal tears as well as partial tears in some individuals. Surgical management is often not appropriate in older or sedentary patients. However, patients treated nonsurgically will have a significant cosmetic defect, as well as weakness in adduction and internal rotation. Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Question 91
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?

Explanation
Recurrent dislocations may follow an earlier dislocation. One study found that in patients who had a patellar dislocation between the ages of 11 to 14 years, 60% had a recurrent dislocation. The incidence of recurrent dislocation dropped to 33% in patients who had a patellar dislocation between the ages of 15 to 18 years. The authors also found that the incidence of recurrence was greater in patients who demonstrated a predisposition to dislocation as determined by evaluation of the unaffected knee. Predisposing signs included passive lateral hypermobility of the patella, a dysplastic distal third of the vastus medialis obliquis muscle, and a high and/or lateral position of the patella. A second study found that the risk of redislocation was considerably higher in patients who were in their teens at the first episode of dislocation compared to older patients. There are no studies linking either a patella baja or a bipartite patella to an increased risk of redislocation. Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Question 92High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of


Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 93
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
The long-term effect of transient quadriplegia is unknown. Based on a history of one brief episode of transient quadriplegia and normal examination and MRI findings, the risk of permanent spinal cord injury with a return to play is low. There is a risk of recurrent episodes of transient quadriplegia after the initial episode. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136. Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509. Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Question 94
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of


Explanation
Open reduction and internal fixation is the treatment of choice for accurate reduction of the disrupted intercarpal ligaments. In addition, the displaced scaphoid fracture will require open reduction and internal fixation and possible bone grafting. Closed reduction and long arm casting will not allow accurate reduction of the dislocated intracarpal intervals, and it is unlikely to allow accurate reduction of the scaphoid. The maneuver required to effect closed reduction of a displaced scaphoid fracture will most likely cause the scaphoid lunate interval to displace. Closed reduction with percutaneous pin fixation or with an external fixator is unable to effect anatomic reduction of the injury. Proximal row carpectomy is used as a salvage procedure for a variety of degenerative and posttraumatic problems of the wrist. Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120. Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Question 95 High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Detailed Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 96 High Yield
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Detailed Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 97
A 13-year-old girl has had a firm mass and pain in her right shoulder for the past several weeks. She denies any history of trauma. A radiograph and MRI scan are shown in Figures 31a and 31b. Biopsy specimens are shown in Figures 31c and 31d. What is the most likely diagnosis?




Explanation
The patient has osteosarcoma. The radiograph suggests an aggressive primary tumor of bone, and the histology shows malignant cells surrounded by osteoid, classic for osteosarcoma. Ewing's sarcoma histologically consists of small round blue cells. Osteochondroma and periosteal chondroma occur in the shoulder but have a different histologic pattern and a less aggressive radiographic appearance. Chondrosarcomas rarely occur in children. Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Question 98
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?

Explanation
It is critical for graft isometry and knee stability that the femoral tunnel be placed as far posterior as possible on the lateral femoral condyle. Superiorly, the graft should be at the one o'clock position on the left knee. Resident's ridge is a false posterior shelf that often seems like the extreme posterior cortex. Abnormal tunnel placement results in a variety of complications, including an unstable knee, early graft failure, and joint stiffness. Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Question 99High Yield
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
At present, radiologists perform multiple MRI images to rule out all possible diagnoses. The ability to specify the anticipated changes on MRI should become more important as a means of reducing costs. MRI is sensitive to changes in free water (or hemorrhage) and thus this will appear dark on T1 and bright on T2. Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Question 100High Yield
What is the function of the rotator cuff during throwing?

Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
