Operative Treatment of Thumb Carpometacarpal Joint Fractures
DEFINITION
The first carpometacarpal (CMC) joint comprises the thumb metacarpal base and the trapezium.The thumb CMC joint is vital to the function of the hand, and injuries can result in pain, weakness, and loss of grip or pinch strength.Two fracture-dislocation patterns commonly result from trauma to the thumb CMC joint:BennettandRolando fractures.Bennett fractures are intra-articular fractures in which the metacarpal shaft is radially displaced by the pull of the abductor pollicis longus (APL) tendon, leaving an intact ulnar fragment at the base of the thumb metacarpal that is held reduced by the strong volar beak ligament (FIG 1A).Rolando fractures are complex intra-articular fractures involving the base of the thumb metacarpal that often have a T- or Y-type pattern. These fractures are classically described as being three-part;however, the name also applies to more comminuted fracture variants (FIG 1B).10
ANATOMY
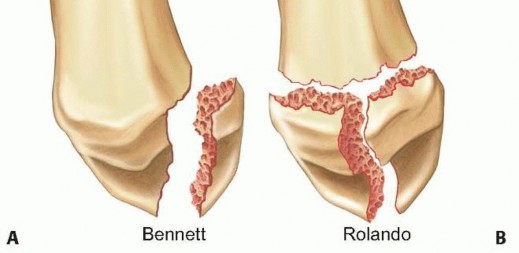
FIG 1 • A. A typical Bennett fracture is a unicondylar fracture of the base of the first metacarpal with the fracture fragment consisting of the volar ulnar corner of the proximal metacarpal. B. A Rolando fracture is multifragmentary, with the entire articular base of the metacarpal being involved. By definition, no portion of the metacarpal shaft is in continuity with the CMC joint. The thumb metacarpal serves as the site of attachment for several tendons, including the APL at the proximal base, the adductor pollicis distally, and the thenar muscles volarly.15The articular surfaces of the thumb metacarpal base and trapezium resemble reciprocally interlocking saddles and allow motion in many planes.11,15Joint stability is maintained by five primary ligaments: the anterior volar (beak), the posterior oblique, the dorsoradial, and the anterior and posterior intermetacarpal ligaments (FIG 2).7Buchler et al2 described three zones at the base of the thumb metacarpal (FIG 3):Zone 2 represents the central portion of the joint that is normally loaded. Zone 1 includes the volar aspect of the joint.Zone 3 involves the dorsal aspect of the joint.The trapezium has several important adjacent articulations. These include the first metacarpal base, the radial aspect of the second metacarpal base, the scaphoid, and the trapezoid (along with the trapezium, these last two make up the scaphotrapeziotrapezoid [STT] joint) (FIG 4).
PATHOGENESIS
Bennett fractures occur when the partially flexed thumb metacarpal is axially loaded, resulting in a Bennett articular fragment (the volar ulnar portion of the metacarpal base) and the remainder of the metacarpal that displaces dorsally, proximally, and radially.Rolando fractures result from a similar injury mechanism and may have a variable degree of comminution at the base of the thumb metacarpal.In Bennett-type fractures, the thumb metacarpal shaft is displaced dorsally and proximally by the pull of the APL at the metacarpal base, the extensor pollicis longus (EPL) which inserts more distally, and angulated ulnarly bythe APL (FIG 5A).15Rolando-type fractures are subject to the same deforming forces, except that the APL can sometimes displace both the shaft and the dorsoradial basilar articular fragment.Due to the deforming forces that act on the fracture fragments, both injury patterns are usually unstable and difficult to reduce and stabilize by closed means.
NATURAL HISTORY
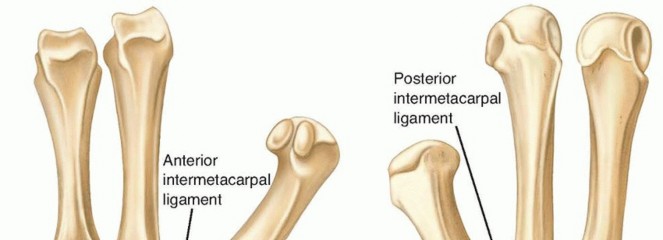


FIG 2 • A,B. Anterior and posterior views of the thumb basal joint stabilizing ligamentous structures. The crucial anterior volar oblique (beak) ligament is often attached to the displaced Bennett fragment.
PATIENT HISTORY AND PHYSICAL FINDINGS
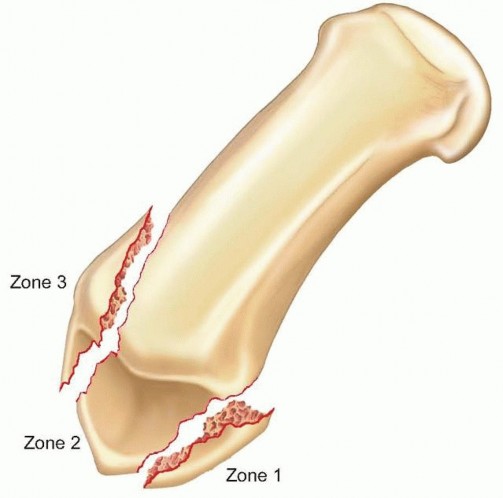
FIG 3 • The three zones found in fractures of the first metacarpal base. The central zone 2 is critical for joint stability and if involved usually requires open reduction and internal fixation.

injuries. A recent case study described the first documented case of thenar compartment syndrome from a thumb metacarpal base fracture.20P.409 FIG 4 • A radiographic view of the trapezium and its articulations including the basal joint. The view is taken with the patient's arm abducted 45 degrees with the hand pronated 45 degrees with the x-ray beam vertically oriented. This evaluates both sides of the basal joint and associated trapezial joint fractures. (Copyright Joshua Mitgang, MD.)
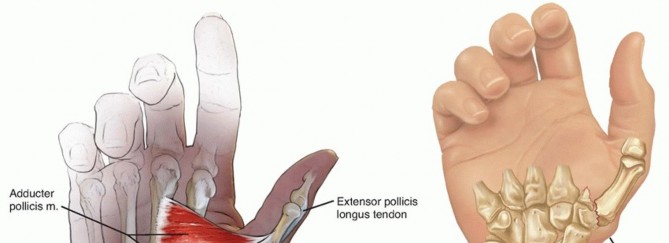
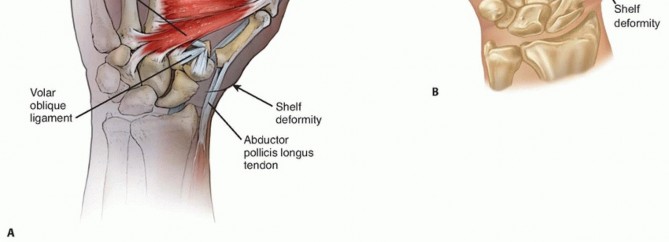
FIG 5 • A. The typical deforming forces about a Bennett fracture. The APL and EPL serve to sublux the main portion of the thumb metacarpal dorsally and radially, whereas the adductor pollicis rotates the fragment ulnarly. The volar oblique ligament holds the volar ulnar fragment of the thumb metacarpal in place. B. A typical shelf deformity is depicted in a Bennett fracture. When viewing the thumb from the lateral perspective, the thumb metacarpal shaft can be seen riding dorsally as it displaces from the unstable CMC joint. Function of the EPL, flexor pollicis longus (FPL), and extensor pollicis brevis (EPB) should be confirmed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP), lateral, and oblique images of the hand should be obtained, although the oblique plane of the thumb in relation to the hand may make these images difficult to interpret.A true AP view of the thumb CMC joint, known as theRoberts view, can be obtained with the forearm maximally pronated with the dorsum of the thumb placed on the cassette (FIG 6A).17A true lateral view, advocated by Billing and Gedda,1 is obtained with the hand pronated 20 degrees and the thumb positioned flat on the cassette. The x-ray beam is tilted 10 degrees from vertical in a distal to proximal direction (FIG 6B).Radiographs of the contralateral, uninjured basal joint are helpful in certain cases as a template for reconstruction.Computed tomography may be indicated if a significant amount of articular comminution is present or when plain films inadequately demonstrate the pathology.A traction view may be helpful in Rolando-type fractures (FIG 6C).Fluoroscopy alone should be used with caution in ensuring anatomic reduction, as this has recently been shown to be less accurate than plain x-rays or direct visualization.4
DIFFERENTIAL DIAGNOSIS
Bennett-type fracture Rolando-type fractureBasal joint degenerative joint disease STT joint arthrosisThumb CMC joint ligamentous injury Trapezial body fractureDe Quervain tenosynovitis
NONOPERATIVE MANAGEMENT
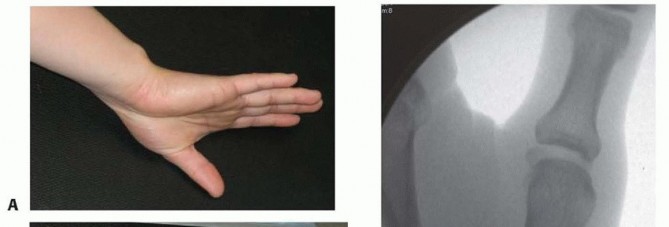
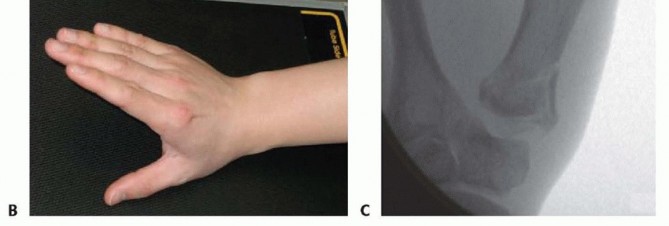
FIG 6 • A. An ideal AP view of the thumb and CMC joint is taken with the forearm hyperpronated and the dorsum of the thumb on the cassette. B. A true lateral view of the CMC joint is obtained with the radial aspect of the thumb on the cassette and the other fingers clear of the x-ray beam. C. A fluoroscopic view of a Rolando fracture with traction applied. Distraction at the CMC joint helps to delineate the fragments at the base of the metacarpal. (Copyright John Capo, MD.) Some studies looking at closed treatment have demonstrated decreased motion, grip strength, and radiographic evidence of degenerative joint disease at long-term follow-up.14Development of degenerative changes may occur if there is any residual subluxation of the thumb metacarpal shaft.3,9
SURGICAL MANAGEMENT
The majority of displaced Bennett fractures and almost all Rolando fractures require percutaneous Kirschner wire fixation or open reduction and internal fixation.The goals of surgery are to restore the articular congruity of the thumb CMC joint and to align the first metacarpal base articular surface with the trapezium.In thumb CMC joint fractures associated with trapezial body fractures, the trapezial articular surface should first be reduced anatomically before proceeding to the thumb metacarpal fracture.16
BENNETT FRACTURES
Closed reduction and percutaneous pinning is the preferred treatment for most Bennett fractures with displaced fracture fragments representing less than 25% to 30% of the articular surface.7,16The metacarpal base often needs to be pinned to the unfractured second metacarpal, trapezoid, or trapezium tolessen the deforming forces on the fracture.Open reduction is necessary when there is residual displacement of the joint surface greater than 2 mm after attempted closed reduction and percutaneous pinning or impaction in the force-bearing aspect of the joint surface (Buchler zone 2).15
ROLANDO FRACTURES
Closed reduction with longitudinal traction and percutaneous pinning is indicated if successful reduction can be achieved under fluoroscopic guidance; this is usually successful only when large T- or Y-type fragments are present.If the joint cannot be reduced by closed methods, open reduction and internal fixation with a combination of smooth wires; screws; and 1.5- to 2.7-mm L, T, or blade plates is indicated.Significant comminution may require either external fixation or a combination of external fixation, limited internal fixation with Kirschner wires and small (1.3 or 1.5 mm) screws, and cancellous bone grafting as advocated byBuchler et al.2
PREOPERATIVE PLANNING
A thorough history and physical examination are mandatory to choose the appropriate treatment and rule out associated injuries.True AP, lateral, and oblique radiographs of the thumb should be obtained in all cases. Traction radiographs help assess the effects of ligamentotaxis on fracture reduction.Surgery may be performed acutely, but if significant soft tissue swelling is present, elevation in a well-padded thumb spica splint for 2 to 5 days may be necessary before undergoing operative fixation.16
POSITIONING
The patient is placed supine on the operating room table.A radiolucent hand table is used to allow for intraoperative fluoroscopy.The patient is moved toward the operative side to center the hand on the table. A nonsterile tourniquet is placed on the upper arm.General, regional (axillary or infraclavicular), or local (wrist block with local infiltration) anesthesia can be used, although muscle relaxation is often necessary to obtain proper reduction.7,16
APPROACH
The Wagner approach can be used for both Bennett and Rolando fractures in which open reduction is necessary.P.411
TECHNIQUES
Closed Reduction and Percutaneous Pinning of Bennett and Rolando Fractures Longitudinal traction, abduction, and pronation of the thumb is performed while applying direct manual pressure over the metacarpal base.16


TECH FIG 1 • A,B. Lateral and posteroanterior (PA) views of a Bennett fracture with intra-articular displacement. C. The metacarpal base is first reduced to the trapezium and then a pin (0.045) is placed across the CMC joint. Two additional pins are provisionally placed and readied to stabilize the Bennett fracture fragment. D. The two smaller pins (0.035) are then advanced across into the Bennett fragment. (Copyright John Capo, MD.) If the Bennett fracture fragment is of ample size, fixation to the fragment may be used in addition (TECH FIG 1D).Large fragments may be manipulated percutaneously with Kirschner wire “joysticks” and then stabilized.The wires are bent and cut outside of the skin, followed by application of a well-padded thumb spica splint with the thumb in abduction and wrist in extension.If less than 2 mm of step-off cannot be obtained by closed reduction, the surgeon should consider abandoning this technique for an open reduction and internal fixation.7,16In rare instances, a similar technique can be used for Rolando fractures, with large T- or Y-type fracture patterns with minimal comminution.1. Open Reduction and Internal Fixation of Bennett Fractures
INCISION AND DISSECTION
A Wagner approach is used for open reduction of a Bennett fracture (TECH FIG 2A).An incision is made on the dorsoradial aspect of the thumb CMC joint at the junction of the glabrous and nonglabrous skin and curved in a volar direction toward the distal wrist crease to the flexor carpi radialis (FCR) tendon sheath (TECH FIG 2B).The palmar cutaneous branch of the median nerve, the superficial radial nerve, and distal branches of the lateral antebrachial cutaneous nerve are at risk in this approach and should be carefully protected (TECH FIG 2C).The thenar muscles are elevated extraperiosteally from the CMC joint and a longitudinal capsulotomy is made to expose the joint and the fracture fragments.An effort should be made to preserve all soft tissue attachments to the fracture fragments (TECH FIG 2D). The fracture line is exposed and cleaned of all hematoma and early callus.This often requires abduction, supination, and dorsal displacement of the metacarpal shaft to expose the volar ulnar Bennett fragment.
REDUCTION AND FIXATION
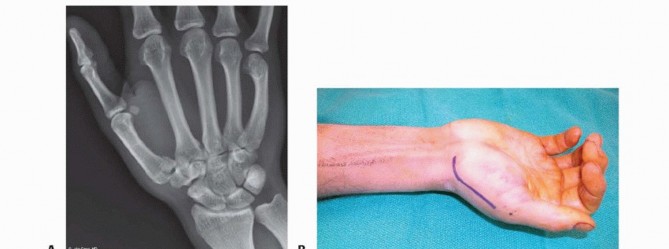


TECH FIG 2 • A. A preoperative radiograph demonstrating a large (˜40%) Bennett fracture with intra-articular displacement. B. The typical incision for open reduction and internal fixation of a Bennett or Rolando fracture. The proximal aspect starts at the FCR tendon sheath. In the case of a Rolando fracture, especially one treated by plate fixation, the distal portion of the incision should extend along the thumb metacarpal. C. Distal nerve branches are seen during the exposure of these fractures. The nerves can usually be retracted dorsally to allow exposure of the CMC joint. D. The thenar muscles are reflected volarly and the CMC joint is entered. The volar oblique fracture is now clearly visualized. Care is taken to maintain soft tissue attachments. (Copyright John Capo, MD.)


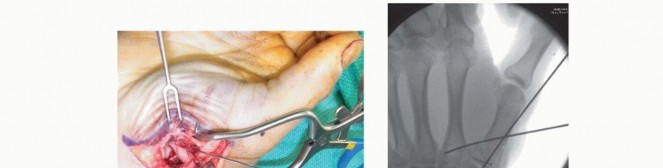
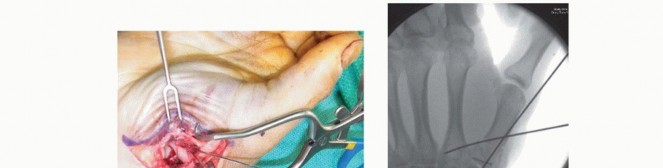
TECH FIG 3 • A. The fracture is cleared of hematoma and then reduced with a pointed reduction forceps. A provisional Kirschner wire is placed percutaneously from the dorsal metacarpal shaft into the fragment. B. Two screws of 1.3 mm diameter are placed in a lag fashion from the metacarpal shaft into the fracture fragment.(continued)


TECH FIG 3 •(continued)C,D. Lateral and AP postoperative views showing reduction of the fracture and articular surface with two screws inserted in different planes. (Copyright John Capo, MD.) Screws should be precisely evaluated radiographically to be certain they are not in the CMC joint or adjacent second metacarpal base (TECH FIG 3C,D).If fixation is tenuous, the metacarpal base can be pinned to the second metacarpal or to the carpus for added stability.Anatomic reduction of the articular surface is verified under direct visualization.The wound is closed in layers with absorbable sutures in the joint capsule, followed by nylon sutures in the skin. A thumb spica splint is applied.1. Open Reduction and Internal Fixation of Rolando Fractures
INCISION AND DISSECTION


TECH FIG 4 • A,B. Preoperative radiographs of a Rolando fracture demonstrating severe intra-articular comminution. C. The thumb thenar muscles have been elevated from the CMC joint and a capsulotomy has been performed. The fracture fragments are identified and cleared of hematoma. (Copyright John Capo, MD.)
REDUCTION AND FIXATION


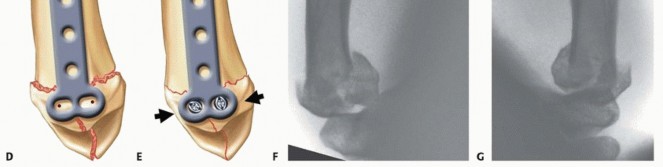
TECH FIG 5 • A. The articular surface is first reduced and provisionally stabilized with multiple small Kirschner wires. B,C. Intraoperative fluoroscopic lateral and AP views demonstrate excellent restoration of the joint surface. Kirschner wires have been placed from the thumb metacarpal into the trapezium and second metacarpal to stabilize the construct. D. The two proximal holes of the T plate are drilled offset for articular fragment reduction. E. The two proximal screws are tightened to compress the proximal fragments. F,G. AP and lateral views of a comminuted, displaced Rolando fracture.(continued)


TECH FIG 5 •(continued)H,I. Postoperative radiographs demonstrating excellent articular reduction using a 2-mm T plate. (A-C: Copyright John Capo, MD; D,E: Adapted from Howard F. Fractures of the basal joint of the thumb. Clin Orthop Relat Res 1987;[220]:46-51; F-I: Courtesy of Dominik Heim, MD.)

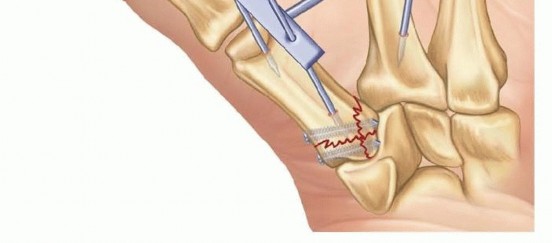
TECH FIG 6 • A schematic of an external fixator frame used for stabilization of a comminuted Rolando-type fracture. Care should be taken to place the thumb in a functional position with wide palmar and radial abduction.
PEARLS AND PITFALLS
|Indications ▪ Operative treatment should be considered if greater than 2 mm of step-off persists after closed reduction. Displaced Bennett fractures greater than 20%-25% of joint surface usually require open reduction and internal fixation for optimal reduction.Preoperative ▪ Proper radiographs, including a true lateral view and an AP hyperpronated view, evaluation must be obtained before operative treatment. CT scanning is usually indicated onlyif significant comminution is present or if plain radiographs are difficult to interpret.Thumb ▪ The thumb should be placed in a position of function with pinning andposition postoperative splinting. This position is palmar and radial abduction of 45 degrees and pronation of 120 degrees.Joint ▪ Joint reduction must be obtained because residual displacement leads to poor reduction outcomes. If adequate joint reduction cannot be verified by fluoroscopy, then opentreatment and direct visualization is mandatory. Percutaneous methods may be inadequate for fractures involving more than 25%-30% of the joint surface.15Postoperative ▪ Thumb spica casting for 4-6 weeks is necessary if percutaneous Kirschner wire management fixation is used. Premature early motion may break Kirschner wires that span theadjacent joints. Range-of-motion exercises can be begun 1-2 weeks postoperatively if stable plate fixation is used.|------
POSTOPERATIVE CARE
BENNETT FRACTURES
A thumb spica splint is applied in the operating room. Pin sites are inspected at 1 week and a thumb spica cast is applied for 4 to 6 weeks, until fracture union.Hand therapy is begun at 2 to 3 weeks for thumb interphalangeal (IP) and metacarpophalangeal (MP) joint motion and index through small finger range of motion.Pins are removed at 4 to 6 weeks and therapy is advanced to the CMC joint along with intermittent immobilization using a removable thumb spica splint.16In patients treated with interfragmentary compression screws and therefore more stable fixation, active range-of-motion exercises can be started at 1 to 2 weeks postoperatively with a removable splint for protection.20
ROLANDO FRACTURES
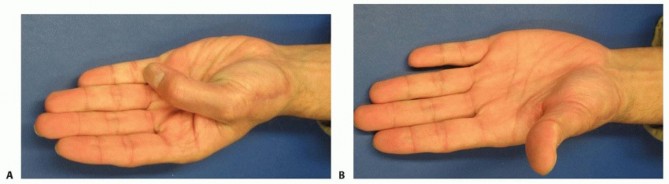
FIG 7 • Clinical photographs of a patient with a Rolando fracture who had undergone open reduction and internal fixation 8 months previously, demonstrating a functional range of flexion (A) and extension (B). (Copyright John Capo, MD.)
OUTCOMES
The majority of patients can expect a successful recovery after operative treatment of Bennett or Rolando fractures19 (FIG 7).Superior results are seen in operatively treated fractures in which there is no residual subluxation of the thumb metacarpal shaft and less than 2 mm of intra-articular displacement.3,15It is generally agreed that if pain and articular incongruity persist after 6 months following closed or open treatment, arthrodesis of the thumb metacarpal to the trapezium or basal joint arthroplasty may be indicated.CMC joint fusion is durable, but patients have difficulty with placing their hand on a flat surface and getting the hand into a pants pocket.Basal joint arthroplasty for acute fractures should be reserved for older, lower demand patients.
COMPLICATIONS
Malunion and subsequent arthrosis resulting from inadequate articular reduction Pin tract infectionInjury to the superficial cutaneous nerves during open dissection and percutaneous fixation Contracture of the first web space from immobilization or pinning of the thumb in an adducted position
REFERENCES
- Billing L, Gedda KO. Roentgen examination of Bennett's fracture. Acta Radiol 1952;38:471-476.
- Buchler U, McCollam SM, Oppikofer C. Comminuted fractures of the basilar joint of the thumb: combined treatment by external fixation, limited internal fixation, and bone grafting. J Hand Surg Am 1991;16(3):556-560.
- Cannon SR, Dowd GS, Williams DH, et al. A long-term study following Bennett's fracture. J Hand Surg Br 1986;11:426-431.
- Capo JT, Kinchelow T, Orillaza NS, et al. Accuracy of fluoroscopy in closed reduction and percutaneous fixation of simulated Bennett's fracture. J Hand Surg Am 2009;34(4):637-641.
- Charnley J. Finger fractures. The Closed Treatment of Common Fractures, ed 3. Edinburgh: Churchill Livingstone, 1981:150.
- Cullen JP, Parentis MA, Chinchilli VM, et al. Simulated Bennett fracture treated with closed reduction and percutaneous pinning. A biomechanical analysis of residual incongruity of the joint. J Bone Joint Surg Am 1997;79:413-420.
- Day S, Stern P. Fractures of the metacarpals and phalanges. In: Wolfe S, Hotchkiss R, Pederson W, et al, eds. Green's Operative Hand Surgery, ed 6. Philadelphia: Elsevier, 2011:283-287.
- Foster RJ, Hastings H II. Treatment of Bennett, Rolando, and vertical intra-articular trapezial fractures. Clin Orthop Relat Res 1987;(214): 121-129.
- Gedda KO. Studies on Bennett fractures: anatomy, roentgenology, and therapy. Acta Chir Scand Suppl 1954;193:1-114.
- Griffiths JC. Fractures of the base of the first metacarpal bone. J Bone Joint Surg Br 1964;46:712-719.
- Haines R. The mechanism of rotation at the first carpometacarpal joint. J Anat 1944;78:44-46.
- Jobe M, Calandruccio J. The hand: fractures, dislocations, and ligamentous injuries. In: Canale T, ed. Campbell's Operative Orthopedics, ed 10. Philadelphia: Elsevier, 2003:3489.
- Jupiter J, Axelrod T, Belsky M. Fractures and dislocations of the hand. In: Browner B, Jupiter J, Levine A, et al, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction, ed 4. Philadelphia: Elsevier, 2009:1221-1341.
- Livesley J. The conservative management of Bennett's fracture-dislocation: a 26-year follow-up. J Bone Joint Surg Br 1990;15(3):291-294.
- Pellegrini VD Jr. Fractures at the base of the thumb. Hand Clin 1988;4: 87-102.
- Raskin K, Shin S. Surgical treatment of fractures of the thumb metacarpal base: Bennett's and Rolando's fractures. In: Strickland J, Graham T, eds. The Hand (Master's Techniques in Orthopaedic Surgery). Philadelphia: Lippincott Williams & Wilkins, 2005:125-135.
- Roberts P. Bulletins et memoires de la Societe de Radiologie Medicale de France, 1936;24:687.
- Thurston AJ, Dempsey SM. Bennett's fracture: a medium to long-term review. Aust N Z J Surg 1993;63:120-123.
- Uludag S, Ataker Y, Seyahi A, et al. Early rehabilitation after stable osteosynthesis of intra-articular fractures of the metacarpal base of the thumb [published online ahead of print June 21, 2013]. J Hand Surg Eur Vol.Chapter 43Operative Treatment of Thumb Carpometacarpal Joint FracturesJohn T. Capo Joshua T. Mitgang Colin Harris
DEFINITION
The first carpometacarpal (CMC) joint comprises the thumb metacarpal base and the trapezium.The thumb CMC joint is vital to the function of the hand, and injuries can result in pain, weakness, and loss of grip or pinch strength.Two fracture-dislocation patterns commonly result from trauma to the thumb CMC joint: Bennett andRolando fractures.Bennett fractures are intra-articular fractures in which the metacarpal shaft is radially displaced by the pull of the abductor pollicis longus (APL) tendon, leaving an intact ulnar fragment at the base of the thumb metacarpal that is held reduced by the strong volar beak ligament (FIG 1A).Rolando fractures are complex intra-articular fractures involving the base of the thumb metacarpal that often have a T- or Y-type pattern. These fractures are classically described as being three-part;however, the name also applies to more comminuted fracture variants (FIG 1B).10
ANATOMY
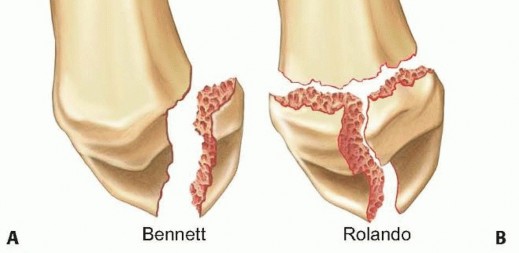
FIG 1 • A. A typical Bennett fracture is a unicondylar fracture of the base of the first metacarpal with the fracture fragment consisting of the volar ulnar corner of the proximal metacarpal. B. A Rolando fracture is multifragmentary, with the entire articular base of the metacarpal being involved. By definition, no portion of the metacarpal shaft is in continuity with the CMC joint. The thumb metacarpal serves as the site of attachment for several tendons, including the APL at the proximal base, the adductor pollicis distally, and the thenar muscles volarly.15The articular surfaces of the thumb metacarpal base and trapezium resemble reciprocally interlocking saddles and allow motion in many planes.11,15Joint stability is maintained by five primary ligaments: the anterior volar (beak), the posterior oblique, the dorsoradial, and the anterior and posterior intermetacarpal ligaments (FIG 2).7Buchler et al2 described three zones at the base of the thumb metacarpal (FIG 3):Zone 2 represents the central portion of the joint that is normally loaded. Zone 1 includes the volar aspect of the joint.Zone 3 involves the dorsal aspect of the joint.The trapezium has several important adjacent articulations. These include the first metacarpal base, the radial aspect of the second metacarpal base, the scaphoid, and the trapezoid (along with the trapezium, these last two make up the scaphotrapeziotrapezoid [STT] joint) (FIG 4).
PATHOGENESIS
Bennett fractures occur when the partially flexed thumb metacarpal is axially loaded, resulting in a Bennett articular fragment (the volar ulnar portion of the metacarpal base) and the remainder of the metacarpal that displaces dorsally, proximally, and radially.Rolando fractures result from a similar injury mechanism and may have a variable degree of comminution at the base of the thumb metacarpal.In Bennett-type fractures, the thumb metacarpal shaft is displaced dorsally and proximally by the pull of the APL at the metacarpal base, the extensor pollicis longus (EPL) which inserts more distally, and angulated ulnarly bythe APL (FIG 5A).15Rolando-type fractures are subject to the same deforming forces, except that the APL can sometimes displace both the shaft and the dorsoradial basilar articular fragment.Due to the deforming forces that act on the fracture fragments, both injury patterns are usually unstable and difficult to reduce and stabilize by closed means.
NATURAL HISTORY
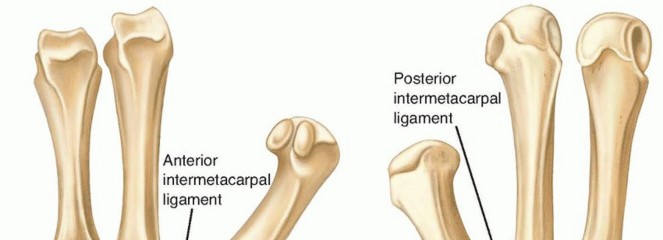


FIG 2 • A,B. Anterior and posterior views of the thumb basal joint stabilizing ligamentous structures. The crucial anterior volar oblique (beak) ligament is often attached to the displaced Bennett fragment.
PATIENT HISTORY AND PHYSICAL FINDINGS
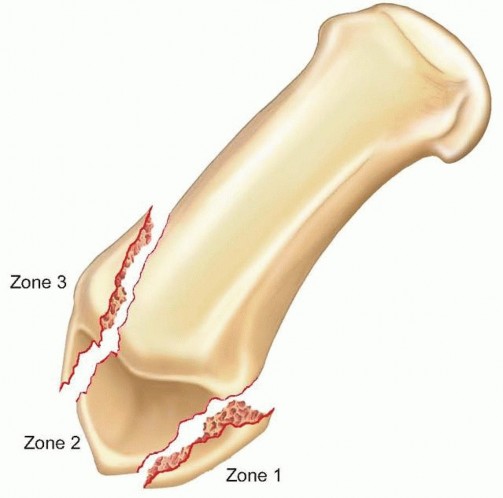
FIG 3 • The three zones found in fractures of the first metacarpal base. The central zone 2 is critical for joint stability and if involved usually requires open reduction and internal fixation.

injuries. A recent case study described the first documented case of thenar compartment syndrome from a thumb metacarpal base fracture.20P.409 FIG 4 • A radiographic view of the trapezium and its articulations including the basal joint. The view is taken with the patient's arm abducted 45 degrees with the hand pronated 45 degrees with the x-ray beam vertically oriented. This evaluates both sides of the basal joint and associated trapezial joint fractures. (Copyright Joshua Mitgang, MD.)
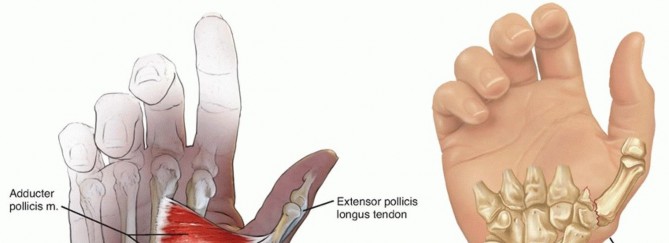
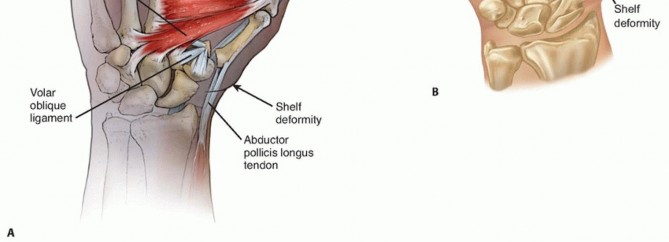
FIG 5 • A. The typical deforming forces about a Bennett fracture. The APL and EPL serve to sublux the main portion of the thumb metacarpal dorsally and radially, whereas the adductor pollicis rotates the fragment ulnarly. The volar oblique ligament holds the volar ulnar fragment of the thumb metacarpal in place. B. A typical shelf deformity is depicted in a Bennett fracture. When viewing the thumb from the lateral perspective, the thumb metacarpal shaft can be seen riding dorsally as it displaces from the unstable CMC joint. Function of the EPL, flexor pollicis longus (FPL), and extensor pollicis brevis (EPB) should be confirmed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP), lateral, and oblique images of the hand should be obtained, although the oblique plane of the thumb in relation to the hand may make these images difficult to interpret.A true AP view of the thumb CMC joint, known as the Roberts view, can be obtained with the forearm maximally pronated with the dorsum of the thumb placed on the cassette (FIG 6A).17A true lateral view, advocated by Billing and Gedda,1 is obtained with the hand pronated 20 degrees and the thumb positioned flat on the cassette. The x-ray beam is tilted 10 degrees from vertical in a distal to proximal direction (FIG 6B).Radiographs of the contralateral, uninjured basal joint are helpful in certain cases as a template for reconstruction.Computed tomography may be indicated if a significant amount of articular comminution is present or when plain films inadequately demonstrate the pathology.A traction view may be helpful in Rolando-type fractures (FIG 6C).Fluoroscopy alone should be used with caution in ensuring anatomic reduction, as this has recently been shown to be less accurate than plain x-rays or direct visualization.4
DIFFERENTIAL DIAGNOSIS
Bennett-type fracture Rolando-type fractureBasal joint degenerative joint disease STT joint arthrosisThumb CMC joint ligamentous injury Trapezial body fractureDe Quervain tenosynovitis
NONOPERATIVE MANAGEMENT
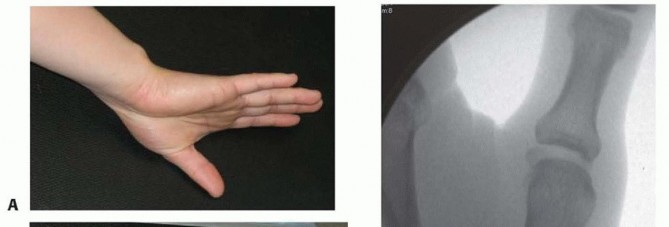
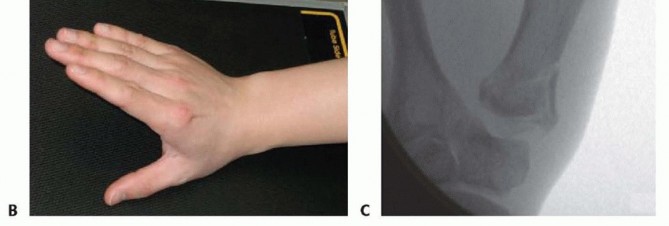
FIG 6 • A. An ideal AP view of the thumb and CMC joint is taken with the forearm hyperpronated and the dorsum of the thumb on the cassette. B. A true lateral view of the CMC joint is obtained with the radial aspect of the thumb on the cassette and the other fingers clear of the x-ray beam. C. A fluoroscopic view of a Rolando fracture with traction applied. Distraction at the CMC joint helps to delineate the fragments at the base of the metacarpal. (Copyright John Capo, MD.) Some studies looking at closed treatment have demonstrated decreased motion, grip strength, and radiographic evidence of degenerative joint disease at long-term follow-up.14Development of degenerative changes may occur if there is any residual subluxation of the thumb metacarpal shaft.3,9
SURGICAL MANAGEMENT
The majority of displaced Bennett fractures and almost all Rolando fractures require percutaneous Kirschner wire fixation or open reduction and internal fixation.The goals of surgery are to restore the articular congruity of the thumb CMC joint and to align the first metacarpal base articular surface with the trapezium.In thumb CMC joint fractures associated with trapezial body fractures, the trapezial articular surface should first be reduced anatomically before proceeding to the thumb metacarpal fracture.16
BENNETT FRACTURES
Closed reduction and percutaneous pinning is the preferred treatment for most Bennett fractures with displaced fracture fragments representing less than 25% to 30% of the articular surface.7,16The metacarpal base often needs to be pinned to the unfractured second metacarpal, trapezoid, or trapezium tolessen the deforming forces on the fracture.Open reduction is necessary when there is residual displacement of the joint surface greater than 2 mm after attempted closed reduction and percutaneous pinning or impaction in the force-bearing aspect of the joint surface (Buchler zone 2).15
ROLANDO FRACTURES
Closed reduction with longitudinal traction and percutaneous pinning is indicated if successful reduction can be achieved under fluoroscopic guidance; this is usually successful only when large T- or Y-type fragments are present.If the joint cannot be reduced by closed methods, open reduction and internal fixation with a combination of smooth wires; screws; and 1.5- to 2.7-mm L, T, or blade plates is indicated.Significant comminution may require either external fixation or a combination of external fixation, limited internal fixation with Kirschner wires and small (1.3 or 1.5 mm) screws, and cancellous bone grafting as advocated byBuchler et al.2
PREOPERATIVE PLANNING
A thorough history and physical examination are mandatory to choose the appropriate treatment and rule out associated injuries.True AP, lateral, and oblique radiographs of the thumb should be obtained in all cases. Traction radiographs help assess the effects of ligamentotaxis on fracture reduction.Surgery may be performed acutely, but if significant soft tissue swelling is present, elevation in a well-padded thumb spica splint for 2 to 5 days may be necessary before undergoing operative fixation.16
POSITIONING
The patient is placed supine on the operating room table.A radiolucent hand table is used to allow for intraoperative fluoroscopy.The patient is moved toward the operative side to center the hand on the table. A nonsterile tourniquet is placed on the upper arm.General, regional (axillary or infraclavicular), or local (wrist block with local infiltration) anesthesia can be used, although muscle relaxation is often necessary to obtain proper reduction.7,16
APPROACH
The Wagner approach can be used for both Bennett and Rolando fractures in which open reduction is necessary.P.411
TECHNIQUES
Closed Reduction and Percutaneous Pinning of Bennett and Rolando Fractures Longitudinal traction, abduction, and pronation of the thumb is performed while applying direct manual pressure over the metacarpal base.16


TECH FIG 1 • A,B. Lateral and posteroanterior (PA) views of a Bennett fracture with intra-articular displacement. C. The metacarpal base is first reduced to the trapezium and then a pin (0.045) is placed across the CMC joint. Two additional pins are provisionally placed and readied to stabilize the Bennett fracture fragment. D. The two smaller pins (0.035) are then advanced across into the Bennett fragment. (Copyright John Capo, MD.) If the Bennett fracture fragment is of ample size, fixation to the fragment may be used in addition (TECH FIG 1D).Large fragments may be manipulated percutaneously with Kirschner wire “joysticks” and then stabilized.The wires are bent and cut outside of the skin, followed by application of a well-padded thumb spica splint with the thumb in abduction and wrist in extension.If less than 2 mm of step-off cannot be obtained by closed reduction, the surgeon should consider abandoning this technique for an open reduction and internal fixation.7,16In rare instances, a similar technique can be used for Rolando fractures, with large T- or Y-type fracture patterns with minimal comminution.22. Open Reduction and Internal Fixation of Bennett Fractures23. Incision and DissectionA Wagner approach is used for open reduction of a Bennett fracture (TECH FIG 2A).An incision is made on the dorsoradial aspect of the thumb CMC joint at the junction of the glabrous and nonglabrous skin and curved in a volar direction toward the distal wrist crease to the flexor carpi radialis (FCR) tendon sheath (TECH FIG 2B).The palmar cutaneous branch of the median nerve, the superficial radial nerve, and distal branches of the lateral antebrachial cutaneous nerve are at risk in this approach and should be carefully protected (TECH FIG 2C).The thenar muscles are elevated extraperiosteally from the CMC joint and a longitudinal capsulotomy is made to expose the joint and the fracture fragments.An effort should be made to preserve all soft tissue attachments to the fracture fragments (TECH FIG 2D). The fracture line is exposed and cleaned of all hematoma and early callus.This often requires abduction, supination, and dorsal displacement of the metacarpal shaft to expose the volar ulnar Bennett fragment.
REDUCTION AND FIXATION
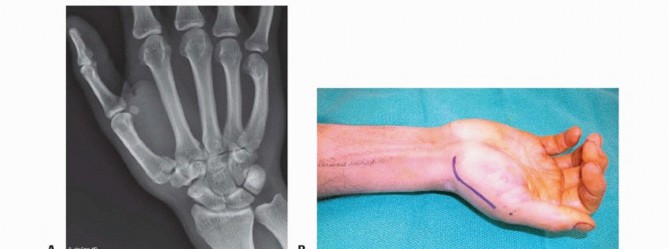


TECH FIG 2 • A. A preoperative radiograph demonstrating a large (˜40%) Bennett fracture with intra-articular displacement. B. The typical incision for open reduction and internal fixation of a Bennett or Rolando fracture. The proximal aspect starts at the FCR tendon sheath. In the case of a Rolando fracture, especially one treated by plate fixation, the distal portion of the incision should extend along the thumb metacarpal. C. Distal nerve branches are seen during the exposure of these fractures. The nerves can usually be retracted dorsally to allow exposure of the CMC joint. D. The thenar muscles are reflected volarly and the CMC joint is entered. The volar oblique fracture is now clearly visualized. Care is taken to maintain soft tissue attachments. (Copyright John Capo, MD.)


TECH FIG 3 • A. The fracture is cleared of hematoma and then reduced with a pointed reduction forceps. A provisional Kirschner wire is placed percutaneously from the dorsal metacarpal shaft into the fragment. B. Two screws of 1.3 mm diameter are placed in a lag fashion from the metacarpal shaft into the fracture fragment. (continued)


TECH FIG 3 • (continued) C,D. Lateral and AP postoperative views showing reduction of the fracture and articular surface with two screws inserted in different planes. (Copyright John Capo, MD.)


TECH FIG 4 • A,B. Preoperative radiographs of a Rolando fracture demonstrating severe intra-articular comminution. C. The thumb thenar muscles have been elevated from the CMC joint and a capsulotomy has been performed. The fracture fragments are identified and cleared of hematoma. (Copyright John Capo, MD.)
REDUCTION AND FIXATION


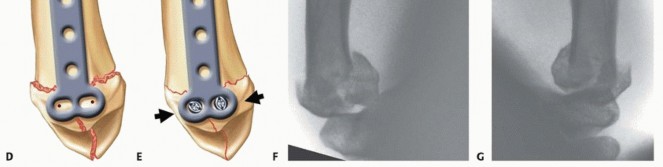
TECH FIG 5 • A. The articular surface is first reduced and provisionally stabilized with multiple small Kirschner wires. B,C. Intraoperative fluoroscopic lateral and AP views demonstrate excellent restoration of the joint surface. Kirschner wires have been placed from the thumb metacarpal into the trapezium and second metacarpal to stabilize the construct. D. The two proximal holes of the T plate are drilled offset for articular fragment reduction. E. The two proximal screws are tightened to compress the proximal fragments. F,G. AP and lateral views of a comminuted, displaced Rolando fracture. (continued)


TECH FIG 5 • (continued) H,I. Postoperative radiographs demonstrating excellent articular reduction using a 2-mm T plate. (A-C: Copyright John Capo, MD; D,E: Adapted from Howard F. Fractures of the basal joint of the thumb. Clin Orthop Relat Res 1987;[220]:46-51; F-I: Courtesy of Dominik Heim, MD.)

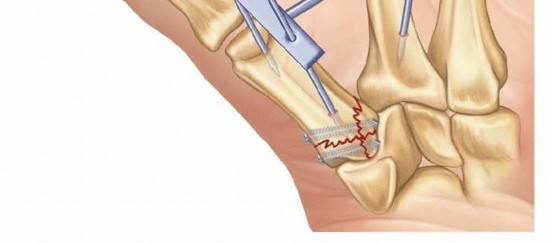
TECH FIG 6 • A schematic of an external fixator frame used for stabilization of a comminuted Rolando-type fracture. Care should be taken to place the thumb in a functional position with wide palmar and radial abduction.
PEARLS AND PITFALLS
|Indications ▪ Operative treatment should be considered if greater than 2 mm of step-off persists after closed reduction. Displaced Bennett fractures greater than 20%-25% of joint surface usually require open reduction and internal fixation for optimal reduction.Preoperative ▪ Proper radiographs, including a true lateral view and an AP hyperpronated view, evaluation must be obtained before operative treatment. CT scanning is usually indicated onlyif significant comminution is present or if plain radiographs are difficult to interpret.Thumb ▪ The thumb should be placed in a position of function with pinning andposition postoperative splinting. This position is palmar and radial abduction of 45 degrees and pronation of 120 degrees.Joint ▪ Joint reduction must be obtained because residual displacement leads to poor reduction outcomes. If adequate joint reduction cannot be verified by fluoroscopy, then opentreatment and direct visualization is mandatory. Percutaneous methods may be inadequate for fractures involving more than 25%-30% of the joint surface.15Postoperative ▪ Thumb spica casting for 4-6 weeks is necessary if percutaneous Kirschner wire management fixation is used. Premature early motion may break Kirschner wires that span theadjacent joints. Range-of-motion exercises can be begun 1-2 weeks postoperatively if stable plate fixation is used.|------
POSTOPERATIVE CARE
BENNETT FRACTURES
A thumb spica splint is applied in the operating room. Pin sites are inspected at 1 week and a thumb spica cast is applied for 4 to 6 weeks, until fracture union.Hand therapy is begun at 2 to 3 weeks for thumb interphalangeal (IP) and metacarpophalangeal (MP) joint motion and index through small finger range of motion.Pins are removed at 4 to 6 weeks and therapy is advanced to the CMC joint along with intermittent immobilization using a removable thumb spica splint.16In patients treated with interfragmentary compression screws and therefore more stable fixation, active range-of-motion exercises can be started at 1 to 2 weeks postoperatively with a removable splint for protection.20
ROLANDO FRACTURES
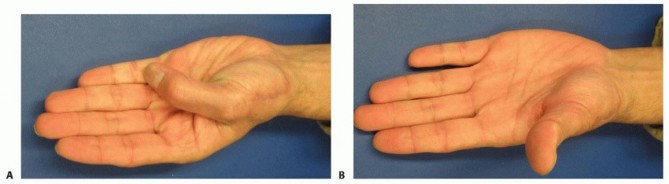
FIG 7 • Clinical photographs of a patient with a Rolando fracture who had undergone open reduction and internal fixation 8 months previously, demonstrating a functional range of flexion (A) and extension (B). (Copyright John Capo, MD.)
OUTCOMES
The majority of patients can expect a successful recovery after operative treatment of Bennett or Rolando fractures19 (FIG 7).Superior results are seen in operatively treated fractures in which there is no residual subluxation of the thumb metacarpal shaft and less than 2 mm of intra-articular displacement.3,15It is generally agreed that if pain and articular incongruity persist after 6 months following closed or open treatment, arthrodesis of the thumb metacarpal to the trapezium or basal joint arthroplasty may be indicated.CMC joint fusion is durable, but patients have difficulty with placing their hand on a flat surface and getting the hand into a pants pocket.Basal joint arthroplasty for acute fractures should be reserved for older, lower demand patients.
COMPLICATIONS
Malunion and subsequent arthrosis resulting from inadequate articular reduction Pin tract infectionInjury to the superficial cutaneous nerves during open dissection and percutaneous fixation Contracture of the first web space from immobilization or pinning of the thumb in an adducted position
REFERENCES
- Billing L, Gedda KO. Roentgen examination of Bennett's fracture. Acta Radiol 1952;38:471-476.
- Buchler U, McCollam SM, Oppikofer C. Comminuted fractures of the basilar joint of the thumb: combined treatment by external fixation, limited internal fixation, and bone grafting. J Hand Surg Am 1991;16(3):556-560.
- Cannon SR, Dowd GS, Williams DH, et al. A long-term study following Bennett's fracture. J Hand Surg Br 1986;11:426-431.
- Charnley J. Finger fractures. The Closed Treatment of Common Fractures, ed 3. Edinburgh: Churchill Livingstone, 1981:150.
- Cullen JP, Parentis MA, Chinchilli VM, et al. Simulated Bennett fracture treated with closed reduction and percutaneous pinning. A biomechanical analysis of residual incongruity of the joint. J Bone Joint Surg Am 1997;79:413-420.
- Day S, Stern P. Fractures of the metacarpals and phalanges. In: Wolfe S, Hotchkiss R, Pederson W, et al, eds. Green's Operative Hand Surgery, ed 6. Philadelphia: Elsevier, 2011:283-287.
- Foster RJ, Hastings H II. Treatment of Bennett, Rolando, and vertical intra-articular trapezial fractures. Clin Orthop Relat Res 1987;(214): 121-129.
- Gedda KO. Studies on Bennett fractures: anatomy, roentgenology, and therapy. Acta Chir Scand Suppl 1954;193:1-114.
- Griffiths JC. Fractures of the base of the first metacarpal bone. J Bone Joint Surg Br 1964;46:712-719.
- Haines R. The mechanism of rotation at the first carpometacarpal joint. J Anat 1944;78:44-46.
- Jobe M, Calandruccio J. The hand: fractures, dislocations, and ligamentous injuries. In: Canale T, ed. Campbell's Operative Orthopedics, ed 10. Philadelphia: Elsevier, 2003:3489.
- Jupiter J, Axelrod T, Belsky M. Fractures and dislocations of the hand. In: Browner B, Jupiter J, Levine A, et al, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction, ed 4. Philadelphia: Elsevier, 2009:1221-1341.
- Livesley J. The conservative management of Bennett's fracture-dislocation: a 26-year follow-up. J Bone Joint Surg Br 1990;15(3):291-294.
- Pellegrini VD Jr. Fractures at the base of the thumb. Hand Clin 1988;4: 87-102.
- Raskin K, Shin S. Surgical treatment of fractures of the thumb metacarpal base: Bennett's and Rolando's fractures. In: Strickland J, Graham T, eds. The Hand (Master's Techniques in Orthopaedic Surgery). Philadelphia: Lippincott Williams & Wilkins, 2005:125-135.
- Roberts P. Bulletins et memoires de la Societe de Radiologie Medicale de France, 1936;24:687.
- Thurston AJ, Dempsey SM. Bennett's fracture: a medium to long-term review. Aust N Z J Surg 1993;63:120-123.
- Uludag S, Ataker Y, Seyahi A, et al. Early rehabilitation after stable osteosynthesis of intra-articular fractures of the metacarpal base of the thumb [published online ahead of print June 21, 2013]. J Hand Surg Eur Vol.
- Werman H, Rancour S, Nelson R. Two cases of thenar compartment syndrome from blunt trauma. J Emerg Med 2013;44(1):85-88.
- Werman H, Rancour S, Nelson R. Two cases of thenar compartment syndrome from blunt trauma. J Emerg Med 2013;44(1):85-88.
