Operative Treatment of Radius and Ulna Diaphyseal Nonunions
DEFINITION
A diaphyseal forearm fracture should be treated as a nonunion if there is either no likelihood that the fracture will go on to union (ie, large segmental defect) or if the fracture has ceased to demonstrate any progression of healing.Secondary to the advent of compression plating, the incidence of forearm nonunions is low, with rates in the radius of 2% and the ulna of 4%. 7
ANATOMY
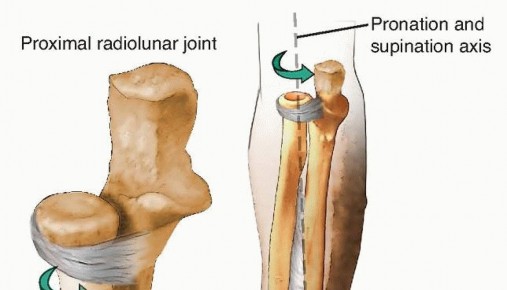
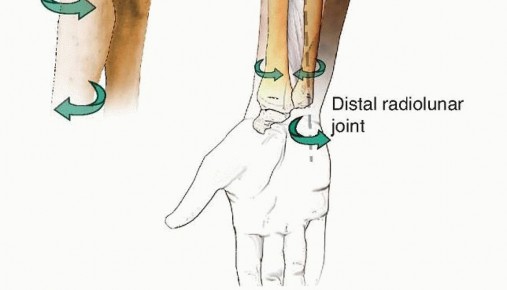
FIG 1 • The two bones of the forearm form a functional unit, with the axis of rotation extending from the radiocapitellar joint to the DRUJ. Extrinsic and intrinsic hand extensors and flexors originate in the forearm as well as do the wrist flexors. Additionally, the forearm provides passage to the neural and vascular elements that give the hand its intricate function. Forearm nonunions, depending on their etiology, can result in a considerable amount of scarring that obliterates normal tissue planes and complicates surgical dissection.
PATHOGENESIS
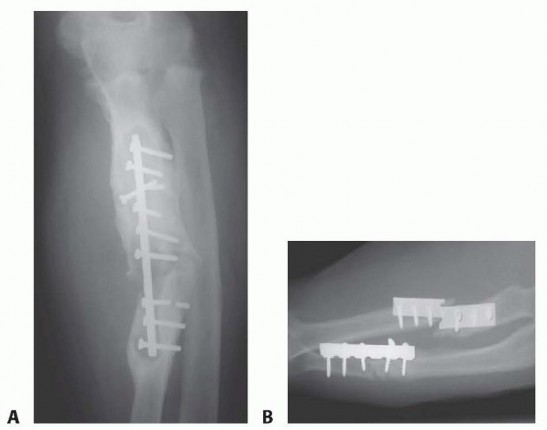
FIG 2 • A. Radiograph showing an infected, hypertrophic nonunion. The abundant callus formation indicates a biologically active nonunion. B. Radiograph showing an atrophic nonunion. There is complete absence of callus at the fracture site. The problem in an atrophic nonunion is lack of biologic activity. (Courtesy of Thomas R. Hunt III, MD.) P.225Many of the injuries that result in nonunion involve a defect; thus, most diaphyseal nonunions of the forearm are atrophic in nature ( FIG 2B).7Open both-bone forearm fractures and ballistic injuries are frequently associated with bone loss at the fracture site.Periosteal stripping, loss of the fracture hematoma, soft tissue and bone loss, and increased infection rate all increase the rate of nonunion.Comminuted open fractures with loss of bone have the highest rates of nonunion. 4
NATURAL HISTORY
Nonunions of the forearm do not heal without surgical intervention.The resultant loss of stability of one or both bones unhinges the entire mechanism of forearm motion with subsequent loss of pronation and supination.Because the movement of the PRUJ and DRUJ are intricately related to the normal length and rotational relationships between the radius and ulna, motion at these joints is affected by a forearm nonunion.Without treatment, the deformity that results from forearm nonunion can become permanent.
PATIENT HISTORY AND PHYSICAL FINDINGS
Although some nonunion patients present with clear deformity, there are others whose only complaint is pain.Frequently, there is also a limitation in forearm rotation.Additionally, limitations in wrist and finger motion are frequently present when there is significant change in ulnar variance secondary to bone shortening.Pain may be exacerbated by use of the extremity for lifting and pushing and strength is severely impaired. Pain may be caused by torsional stressing of the forearm.Physical examinationEvaluate the skin and soft tissue envelope. Long-standing infected nonunions may develop draining sinuses. Thorough vascular examination to look for any vasculopathyPalpate the nonunion site for pain.Stress the forearm by resisting flexion, extension, pronation, and supination. Look for loss of motion at the elbow or wrist.Look for a loss of pronation or supination.Infection is always considered as a cause of nonunion, especially if the initial fracture was open or if the patient has had surgery on the affected arm.If the patient was previously treated at another facility, be sure to clarify if there was any postoperative drainage or if antibiotics were required. Obtain the previous records if possible.As is the case for any nonunion patient, look for host factors that affect bone healing such as tobacco use. A detailed metabolic workup should be performed that includes tests for vitamin D, albumin, pre-albumin, calcium, alkaline phosphatase (ALP), hemoglobin A1c (for diabetics), thyroidstimulating hormone (TSH), and testosterone.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs in neutral forearm rotation should be obtained of both the affected forearm as well as of the uninjured forearm. This provides a comparison view for a full evaluation of the deformity.In the event of a questionable nonunion, computed tomography (CT) can be used to evaluate bone healing at the site in question.CT also helps elucidate rotational deformities, the presence and extent of a synostosis, and the bony relationships of the DRUJ and PRUJ.An infection workup should be performed in all patients. This includes an erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and a complete blood count (CBC).If laboratory tests are normal, but infection is seriously suspected, consider a technetium 99m bone scan followed by an indium 111-labeled leukocyte scan.Magnetic resonance imaging (MRI) or a biopsy of the nonunion site can also be used to evaluate for infection.
DIFFERENTIAL DIAGNOSIS
InfectionForearm malunionUndiagnosed PRUJ or DRUJ injurySymptomatic implants IOM injury
NONOPERATIVE MANAGEMENT
Nonoperative management of a symptomatic nonunion should be reserved for patients who are poor operative candidates or noncompliant with treatment efforts. As with any nonunion, the treatment course is long and complicated and requires patience on the part of both the patient as well as the surgeon.Patient participation is essential, and smoking cessation is required prior to repair of the nonunion. Smoking cessation should be stopped 4 weeks prior to surgery to negate the anti-inflammatory effects.Typically, two nicotine tests 2 weeks apart prior to surgery confirms smoking cession.Rarely, a patient will develop a stable, fibrous union that allows for pain-free function. These patients do not require an operation.
SURGICAL MANAGEMENT
The primary goal of treatment is to obtain union. Significant improvements in range of motion are not always realized. In some cases where forearm motion is taking place through the nonunion site, obtaining union can even result in loss of motion. The patient should be aware of this preoperatively.Surgery focused on the PRUJ or DRUJ may be required to improve motion.Previously operated wound beds have severe scarring, and there is an increased risk of neurovascular injury during surgery.
PREOPERATIVE PLANNING
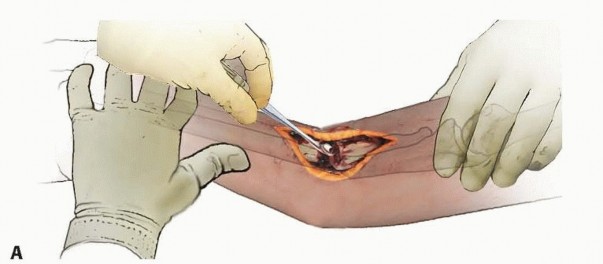
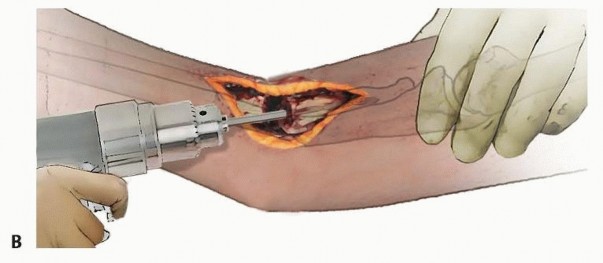
FIG 3 • A. Complete débridement of the nonunion site is the essential first step. Any fibrous or necrotic material must be removed and the bone ends delivered. B. Medullary canals are opened using increasing diameter drill bits to allow vascular ingrowth. Ensure that all potentially necessary surgical instruments are available. This could include such specialty items as full-length anatomic plates, curved curettes, osteotomes, and a high-speed burr.We do not use allograft bone chips as a cancellous graft expander unless our harvest provided anextraordinarily poor yield.When using cancellous grafting or the Masquelet technique, consider using bone morphogenic protein (BMP), as it has been shown to have a higher incidence of healing in those instances. 2
POSITIONING
Supine positioning on the radiolucent table with a radiolucent hand tableC-arm imaging should be tested prior to starting the case to ensure that full-length images of the forearm can be obtained without difficulty.Consider saving rotational profile images of the contralateral forearm for intraoperative referral.If anterior iliac crest grafting is planned, then the ipsilateral iliac crest should be prepped appropriately.If a large amount of graft is required, the authors recommend the RIA for harvesting from the contralateral femur, as harvesting posterior iliac crest bone graft (PICBG) requires a significant positioning change.
APPROACH
If there has previously been surgery on the forearm, these incisions should be used if possible.In general, one should adhere to careful dissection techniques with minimal periosteal stripping and minimal muscle elevation. The available blood supply to the nonunion site should be compromised as little as possible.The medullary canals should be recannulated using a drill until bleeding emanates from the canal ( FIG 3).To increase blood flow, the cortex of the bone on either side of the nonunion may be feathered with anP.227osteotome or fenestrated with a small-diameter drill or K-wire.For access to the mid and distal radius, the volar approach of Henry provides excellent exposure. (Refer to the chapter in this book entitled, “Diaphyseal Forearm Fractures,” for a complete description.)Proximal radius nonunions may be best accessed using the dorsal approach of Thompson.The ulna is accessed along its entire length using the subcutaneous approach. The dorsal ulnar cutaneous branch of the ulnar nerve should be identified distally.
TECHNIQUES
DIRECT COMPRESSION


TECH FIG 1 • A. An extreme example of a distal-third radius shaft fracture with a significant bone defect and DRUJ injury. B. The ulna was shortened, and the radius nonunion was compression-plated in addition to the wrist being fused.

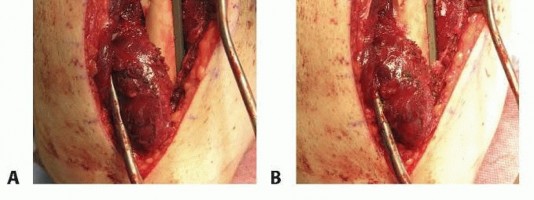
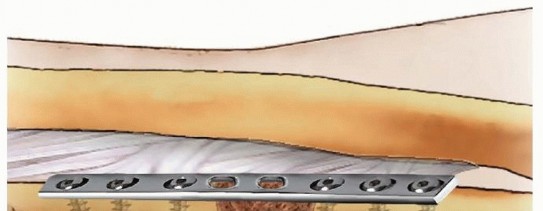
TECH FIG 2 • A. A partial defect after débridement and plating. B. Cancellous autograft packed into the defect.
TRICORTICAL ILIAC CREST AUTOGRAFT
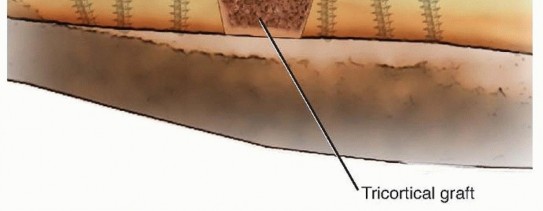
TECH FIG 3 • Modified Nicoll technique with tricortical iliac crest graft. The graft is chamfered, allowing the graft to be compressed as the plate is applied.
Masquelet Technique
In cases of partial or segmental defect, antibiotic-containing methylmethacrylate cement is used to fill the defect, and a bridge plate can applied to span the zone of injury. Length and rotation must be verified against the opposite side and with assessment of pronation and supination range of motion.
All of the necrotic bone and fibrous tissue in the nonunion site is débrided.
Similar to the technique for cancellous grafting, a bridge plate must be carefully applied.
The cement should be packed in the defect in a manner that will make the extraction process easier.
Prescoring the cement makes extracting the cement in pieces easier.
The cement should overlap the cut bone ends by a millimeter or two to prevent fibrous tissue forming over the freshly cut bone.
After a 6-week interval, through the original incision, the pseudomembrane is incised longitudinally, and the cement spacer is removed. Cancellous autograft with or without BMP is used to fill the void. Again, the volume of graft required should be estimated preoperatively and a graft source chosen that best facilitates that volume.
P.229Vascularized Bone Grafting
A donor graft is chosen based on the grafting requirements.
The distal ulna can be grafted using a distal radius bone graft based on the fourth extensor compartment
artery (ECA). Although this form of grafting may only be used to graft defects less than 2 cm in length, it has a wide arc of mobilization and can be used for much of the distal third of the ulna. 6
MASQUELET TECHNIQUE
VASCULARIZED BONE GRAFTING
TECH FIG 4 • A. A 6-cm defect in the radius. B. An appropriately sized free fibula graft was compression-plated in the defect. The associated skin island is seen. C. At case end, with the skin island incorporated into the initial incision. D. At 6 weeks follow-up. The patient eventually went on to union.


PEARLS AND PITFALLS
Patient preparation1.Demand smoking cessation prior to operative intervention. Perform a metabolic workup on all patients.Patient decision making1.Ensure that the patient understands the risk and morbidity associated with nonunion surgery and autologous bone grafting. Explain that functional outcomes are frequently not as good as surgical outcomes.Abnormal operative anatomy2.Start tissue dissection outside the zone of previous surgery to establish and define normal tissue planes.3.Take time and care during dissection, as scarring and muscle contractions can significantly alter the relevant neurovascular anatomy.Establish blood flow at the nonunion site1.Cannulate the intramedullary canals with a 3.5- or 4.0-mm drill bit. Feather or fenestrate the surrounding cortical bone.Reestablish normal1.Take contralateral forearm images in the operating room prior to starting surgery. Have a forearm bone model available if possible.|anatomy ▪ Consider using anatomic plates.Regain length ▪ Use a temporary external fixator or the articulating tensioner to lengthen the bone in question.Disuse ▪ Use long, locking plates to distribute the load more evenly. osteopenia atnonunion siteDefect ▪ Cut cortical grafts longer than the measured defect.management ▪ Use stainless steel plates with locking secures for longer lasting bridge constructs.1.Consider spacer placement and using the Masquelet technique.|------
POSTOPERATIVE CARE
Postoperative splints are typically used to facilitate wound healing; however, these are removed at the first postoperative visit and active range-of-motion exercises are begun.Lifting is restricted to less than 2 to 5 pounds—patients should be able to do many of their normal activities of daily living, and this is encouraged.Advancement of lifting restrictions is usually delayed for 3 to 4 months or until there is radiographic evidence of bony union.If there is a delay in motion recovery postoperatively, static-progressive night splinting is instituted to regain motion. Manipulations of the forearm should be avoided.P.230
OUTCOMES
As in forearm fractures, forearm nonunions have high rates of nonunion after operative treatment. The aforementioned methods cite healing rates between 95% and 100%. 3,5,7In the cases of forearm nonunions that are related to either poor initial operative technique or to bone loss, solving the causal problem during the nonunion surgery usually leads to success in treating the nonunion.In those patients whose nonunion was caused by infection, recurrence of the infection is a poor prognostic indicator. Almost all the patients who fail their nonunion repair have a recurrence of a deep infection.Overall, patient satisfaction does not mirror the success of achieving bony union. Roughly only two-thirdsof patients report good or excellent results. 3,5,7 This likely represents the high demands that patients require of their upper extremities as well as the limitations of motion that frequently occur in revision forearm surgery.
COMPLICATIONS
New onset infection or resurgence of the organism(s) of a previously infected nonunion can both occur.Frequently, the nonunion has already altered the normal range of motion of the forearm through scar tissue and contracture formation. Repair of the nonunion unfortunately can add to scar tissue and contracture formation and result in even more loss of motion. (Fortunately, pain and subjective feeling of stability of the limb improve.)Secondary to extensive scar tissue formation associated with nonunions and the extensile exposure needed for repair, the propensity of neurovascular injury is greater secondary to the loss of “normal” tissue planes.Recurrent nonunion and hardware failureIn the event of extensive dissection in the area of the IOM, synostosis may occur. Donor site pain or dysesthesias
REFERENCES
- Cai XZ, Yan SG, Giddins G. A systematic review of the non-operative treatment of nightstick fractures of the ulna. Bone Joint J 2013; 95(7): 952-959.
- Calori GM, Colombo M, Mazza E, et al. Monotherapy vs. polytherapy in the treatment of forearm non-unions and bone defects. Injury 2013;44(suppl 1):S63-S69. doi:10.1016/S0020-1383(13)70015-9.
- Kamrani RS, Mehrpour SR, Sorbi R, et al. Treatment of nonunion of the forearm bones with posterior interosseous bone flap. J Orthop Sci 2013;18(4):563-568. doi:10.1007/s00776-013-0395-0.
- Moed BR, Kellam JF, Foster RJ, et al. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68(7):1008-1017.
- Moroni A, Rollo G, Guzzardella M, et al. Surgical treatment of isolated forearm non-union with segmental bone loss. Injury 1997;28(8): 497-504.
- Pagnotta A, Taglieri E, Molayem I, et al. Posterior interosseous artery distal radius graft for ulnar nonunion treatment. J Hand Surg Am 2012;37(12):2605-2610. doi:10.1016/j.jhsa.2012.09.004.
- Ring D, Allende C, Jafarnia K, et al. Ununited diaphyseal forearm fractures with segmental defects: plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86-A(11): 2440-2445.
- Ring D, Rhim R, Carpenter C, et al. Comminuted diaphyseal fractures of the radius and ulna: does bone grafting affect union rate? J Trauma 2005;59(2):438-441. doi:10.1097/01.ta.0000174839.23348.43.
