DEFINITION
Hand metacarpals can fracture at their base, shaft, neck, or head. Such fractures can lead to shortening, rotation, or angulation.Metacarpals provide a base for each finger and injury to a metacarpal can severely compromise independent digital function.Treatment strategy for metacarpal injuries must consider the ability of the human hand to compensate for such injuries.
ANATOMY

PATHOGENESIS

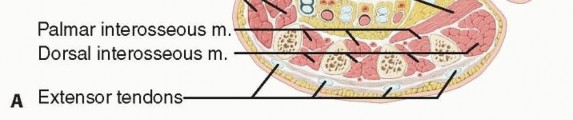


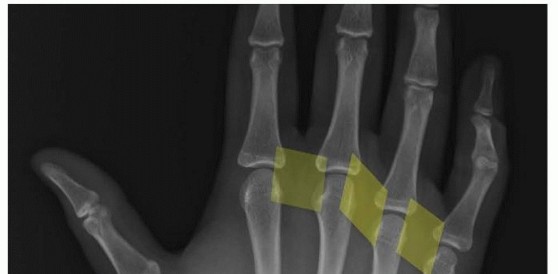
FIG 2 • A. The metacarpals have a triangular shape. The interosseous muscles cover the radial and ulnar surfaces of the metacarpals. The extensor tendons are in close proximity to the dorsal surface. B. The dorsal apparatus covers the MP joint. The extrinsic extensor tendons extend the MP joint and the intrinsic tendons flex it.


FIG 3 • A. Fracture of the neck of the fifth metacarpal with a flexed, apex dorsal angulation (boxer's fracture). B. Torsional injuries lead to long oblique fractures with a risk for malrotation. C. Short transverse fracture from a direct impact. D. Crush injuries can lead to a combination of injuries with an increased risk of compartment syndrome and significant stiffness. The shortened fourth metacarpal pulls the head of third metacarpal in a proximal and ulnar direction through deep transverse metacarpal ligament. E. Neglected fight bite injury ultimately leading to loss of the metacarpal head. Crush injuries can lead to comminuted fractures with significant soft tissue injuries and a heightened risk of compartment syndrome (FIG 3D).
NATURAL HISTORY
Metacarpal fractures are mainly affected by shortening and rotation. The effect of these two components is minimized in the central metacarpals due to the stabilizing effect ofP.457the deep transverse metacarpal ligaments and the bordering intact metacarpals. This stabilizing effect is lost incases of multiple metacarpal fractures and more severe injuries (see FIG 3D).Shaft fractures of the third and fourth metacarpals tend to do well with minimal intervention. Border metacarpals are more prone to shortening and rotation.Every 2 mm of shortening of the metacarpal can lead to a 7-degree lag at the MP joint.12Fractures of the metacarpal neck typically result in apex dorsal angulation, which may lead to significant shortening. The increased mobility afforded by the ulnar CMC joints allows more tolerance of angulation in the ulnar metacarpals (fourth and fifth). Whereas some have accepted up to 70 degrees, most authors haverecommended intervention if the angulation exceeds 30 to 40 degrees.4,6,9 The radial metacarpals (second to third) have stiffer CMC joints, and correspondingly, the tolerance for angulation is reduced to only 10 to 15degrees.7Thumb metacarpal extra-articular base and shaft fractures can easily tolerate 30 degrees of angulation due to its highly mobile CMC joint.1Fractures of the metacarpal head with a significant gap or step-off, or fractures that involve a significant portion of the articular surface, should be considered for open reduction and stabilization.2
PATIENT HISTORY AND PHYSICAL FINDINGS
History: Note the mechanism of injury, time since injury, and any treatment received so far. Also, note the age, vocation, and hobbies of the patient. Comorbidities should also be recorded.Inspection: The skin needs to be checked for any signs of an open fracture. A small laceration near the MP joint may be the only sign of a “fight bite” injury which requires urgent débridement to prevent joint and bone infection (FIG 3E). Also, note digit malrotation and extension lag at the MP and proximal interphalangeal (PIP) joints. A severely edematous hand may signal compartment syndrome or an internal degloving injury.Palpation: The neurovascular examination should include checking activation of the first dorsal interosseous muscle to confirm activity of the motor branch of the ulnar nerve. Tense compartments and pain with passive motion may signal a developing compartment syndrome.
IMAGING AND OTHER DIAGNOSTIC STUDIES
The posteroanterior (PA) view can show shortening, especially relative to the adjacent metacarpals. Fracture angulation can be seen on the lateral view but is often best seen on the oblique view. Fractures of the base of the fifth metacarpal are best seen on the pronated oblique view.Specialized views of the metacarpal head can show the volar aspect (Brewerton) or the dorsal aspect (skyline).Traction views in the anesthetized patient may help elucidate pattern and extent of injury.Computed tomography (CT) scan can help in extensively comminuted fractures or articular injuries.
DIFFERENTIAL DIAGNOSIS
Open fracturesFight bite with bacterial inoculation of the MP joint Pathologic fractures
NONOPERATIVE MANAGEMENT

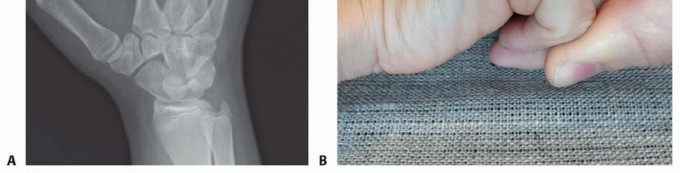
FIG 4 • A. Angled metacarpal shaft fractures deserve an attempt at closed reduction. B. Jahss maneuver. A dorsally directed force is applied to the flexed PIP joint while the metacarpal is stabilized proximally. (continued)

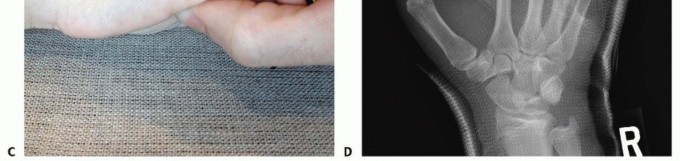

FIG 4 • (continued) C. Metacarpal neck reduction applying force at the metacarpal head itself while stabilizing the metacarpal shaft proximally. D. Fourth metacarpal shaft fracture reduction being stabilized with pressure directly on the metacarpal head. Note the MP joint is maintained in extension. E. MP flexion on the day of cast removal after being casted for 4 weeks. Be aware that prolonged immobilization of MP joints in extension may lead to collateral ligament contracture and result in difficulty regaining MP flexion.
SURGICAL MANAGEMENT
Indications for surgery include open fractures, open joint injuries (such as fight bites), malrotated fractures, unstable fractures, and those associated with other injuries that need surgery such as tendon or nerve lacerations.Relative indications for surgery include extensor tendon lag, metacarpal shortening, prominence of the metacarpal head in the palm, multiple metacarpal fractures, and intraarticular fractures.Contraindications for internal fixation include grossly contaminated fractures and infirmed patients.Contaminated fractures should be débrided and temporarily stabilized until definitive fixation can be performed.Percutaneous pins have the advantage of minimizing soft tissue injury. However, the fracture must be reducible through closed means.Percutaneous pins can be placed in a retrograde direction from distal to proximal entering the metacarpal through the collateral recesses. This technique allows stabilization of proximal neck or shaft fractures. Flexion of the MP joint facilitates access to the collateral ligament recesses.Antegrade pin fixation (bouquet pinning) from proximal to distal can provide stability to shaft and neck fractures. This technique has the advantage of avoiding the MP joints altogether, which, if enough stability is present, may even permit early motion. In the treatment of neck fractures, it may lead to less MP stiffnesscompared to retrograde (collateral recess) pinning.10 However, placement of the antegrade wires can be more challenging technically.There are many occasions when the fracture cannot be easily reduced through closed techniques and open approach is required. Such an approach allows for an anatomic reduction and placement of stable fixation. However, it also introduces a degree of soft tissue insult.P.459Screws provide rigid fixation while at the same time minimizing implant bulk. However, they are appropriate only for long oblique or spiral fractures whose lengths are at least twice the diameter of the bone at the level of the fracture.Plates provide rigid fixation in short oblique and transverse fractures but require significant soft tissue dissection. Rarely, the hardware will have to be removed once the fracture is healed.External fixators allow treatment of more complex fractures while minimizing soft tissue injury but do not allow precise control of the fracture fragments. External fixation may be desirable in the treatment of injuries with massive soft tissue disruption.
PREOPERATIVE PLANNING

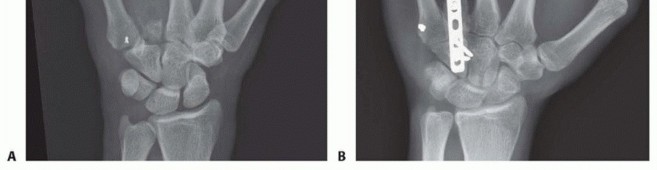


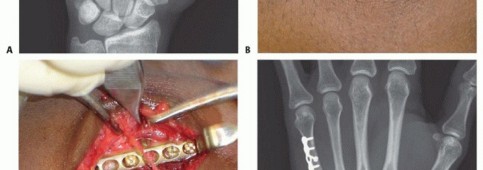
FIG 5 • A. Missing fourth metacarpal shaft and base after gunshot wound. Patient had tenuous dorsal skin. Metacarpal head temporarily stabilized with buried pins from fifth metacarpal. B. Once the soft tissues stabilized, the metacarpal was grafted from the iliac crest and stabilized with plate and screws to the hamate. C. Dorsal sensory branch of the ulnar nerve travelling through the center of the wound on a different patient. Grossly contaminated wounds, or those with tenuous soft tissues, may be best managed initially with limited fixation until more definitive fixation can be performed (FIG 5A).Bone grafting may also need to wait until the soft tissues have stabilized (FIG 5B).The need to address nerve, vessel, or tendon injuries may also affect the approach (FIG 5C).
POSITIONING
Most hand fractures are addressed with the patient supine and the hand on a hand table. Concomitant injuries or conditions may affect access to the hand.Regional or general anesthesia is most commonly used for metacarpal fractures. Local anesthesia may beappropriate in some circumstances.
APPROACH


FIG 6 • Dorsal approach to the MP joint of an index finger. Extensor tendon beneath top retractor. Capsule grabbed by pickup forceps. Articular cartilage seen deep to capsule.
TECHNIQUES
Closed Reduction and Pin Fixation of Metacarpal Fractures
Closed Reduction and Pin Fixation of Metacarpal Fractures
RETROGRADE COLLATERAL RECESS PINNING

TECH FIG 1 • A. Retrograde (collateral recess) pinning. B,C. Angled distal metacarpal fracture. (continued)



TECH FIG 1 • (continued) D,E. Fracture stabilized with two pins that have been advanced to the base of the metacarpal. (Copyright Thomas R. Hunt III, MD, DSc.)
ANTEGRADE BOUQUET PINNING
This technique requires a rotationally stable fracture that can be reduced through closed means (TECH FIG 2A).An incision is made at the base of the metacarpal. Careful dissection is carried through the soft tissues protecting the cutaneous nerve branches. The extensor tendons are retracted and the metaphysis of the base of the metacarpal is exposed.In the case of a fifth metacarpal, it is easier to make this approach straight ulnar as opposed to dorsal (TECH FIG 2B).A unicortical 2.7- or 3.5-mm tunnel is made with a drill. This tunnel is created angled in a proximal to distal direction (TECH FIG 2C).Commercially available sets include an awl that helps in establishing the tunnel through which the definitive fixation is placed.Two or three prebent wires (TECH FIG 2D) are then advanced through the tunnel, across the fracture, and lodged into the metacarpal head subchondral bone (TECH FIG 2E).Great care must be exercised advancing the wires to prevent them from penetrating through the opposite cortex.The wires can be advanced with a needle holder or a pin holder using some gentle oscillation.The hand is initially immobilized in a forearm-based splint with the MP joint in 70 to 90 degrees of flexion while allowing some motion of the IP joints.If stable fixation is accomplished early, MP joint motion is initiated. The affected finger can be buddy taped to the adjacent finger to avoid rotational forces across the fracture.The wires may be removed after 4 weeks or, if cut at the level of the bone, they may be left in place indefinitely.
TRANSVERSE PINNING

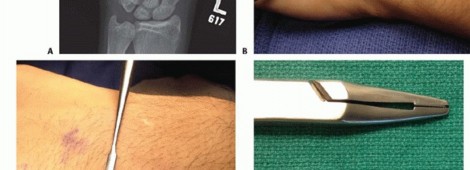
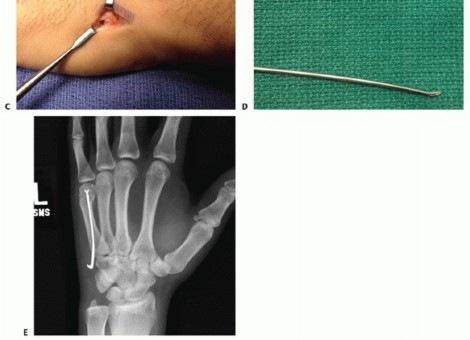
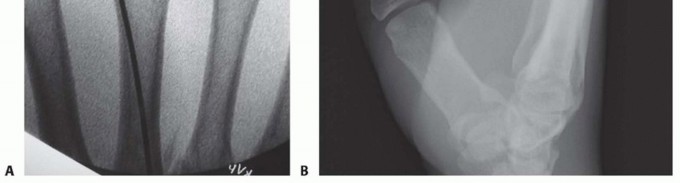
TECH FIG 2 • A. Angled metacarpal neck fracture. B. Incision at the ulnar base of the fifth metacarpal, exposing the insertion of the extensor carpi ulnaris (ECU) on the base of the metacarpal. Incision located on ulnar aspect of metacarpal to minimize irritation of the extensor tendons. C. Unicortical tunnel at the base of the metacarpal. D. Sample of prebent pin. Tip is angled to facilitate passage through the shaft. E. In metacarpal neck fractures or those at risk of shortening, it is important to bring the pins to the subchondral bone of the metacarpal head but not violate the head.




TECH FIG 3 • A. Second metacarpal fracture with an intact adjacent metacarpal and a narrow medullary canal. B. Fixation using one proximal pin to secure the shaft and two distal pins to secure the distal fragment. C,D. Fracture where the narrow medullary space made it difficult to pass a second wire through the canal. Supplemental fixation achieved through a transverse pin on the distal fragment. The fracture is anatomically reduced through closed means.The proximal fragment is first stabilized by pinning it to the adjacent intact metacarpal.Use the nick and spread technique while placing the wires to minimize the risk of iatrogenic cutaneous nerve injury.Keep pressure between the adjacent metacarpals to prevent convergence between the metacarpals as the wire is advanced.Be mindful of the arch-like arrangement of the metacarpals.The distal fragment is stabilized by placing two wires through the distal fragment into the adjacent intact metacarpal (TECH FIG 3B).The hand is immobilized in a forearm-based splint with the MP joints flexed 70 to 90 degrees while the pins are in place. The pins are kept for 3 to 4 weeks. The IP joints are left free to move.The pins are removed at 3 to 4 weeks, and the hand is placed in a removable splint for an additional 2 weeks.Alternatively, transverse pins can be used to augment other forms of fixation or control rotation (TECH FIG 3C,D).1. Open Reduction and Plate/Screw Stabilization of Metacarpal Fractures
DORSAL APPROACH FOR FIXATION

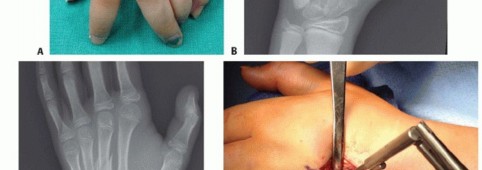

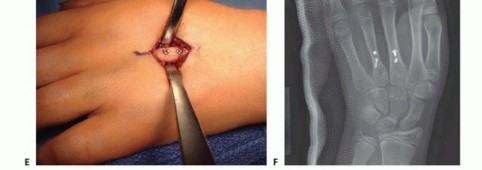
TECH FIG 4 • A-C. Patient with torsional injury to long and ring fingers leading to spiral fractures of the third and fourth metacarpals. The combined injury made it possible for malrotation to develop. D.
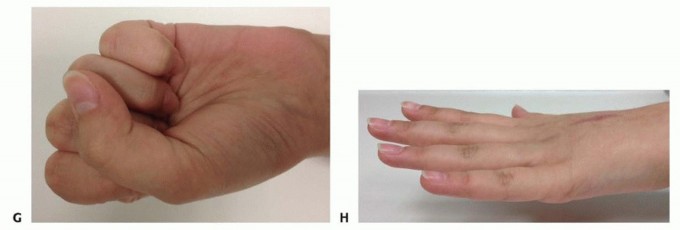
TECH FIG 4 • (continued) G,H. Motion at 6 weeks after surgery. The periosteum is elevated at the fracture site to assist with assessment of fracture reduction. As much of the interosseous muscle is left attached to the metacarpal as feasible to preserve blood supply to the bone.The fracture is reduced and provisionally stabilized with reduction clamps (TECH FIG 4D).
LAG SCREW FIXATION
Long oblique and spiral fractures whose lengths are at least twice the diameter of the bone at the level of the fracture are amenable to limited fixation with screws only (see TECH FIG 4A-C).Appropriately sized lag screws (1.4 to 2.7 mm) are placed. Typically, two or three screws are used (TECH FIG 4E,F).The first screw is placed perpendicular to the fracture in order to compress it and the second screw is placed perpendicular to the bone to resist longitudinal forces.In order to get proper compression with a lag screw construct, it is important to overdrill the near cortex.When using a 2.0-mm screw system, a 1.5-mm drill bit is used to drill both cortices. The near cortex is then overdrilled with a 2-mm drill bit.A countersink is used to maximize contact between the head of the screw and the bone. The size of the screw is measured and an appropriately sized screw is placed.The periosteum and interosseous muscle fascia are reapproximated to cover the screws. The juncturae tendinum are repaired and the skin is closed in standard fashion.The hand is then immobilized with the MP joints flexed 70 to 90 degrees with a forearm-based splint. Early motion can be started as early as 4 to 7 days, depending on fracture stability (TECH FIG 4G,H).
PLATE AND SCREW FIXATION


TECH FIG 5 • A,B. Short oblique fracture of the metacarpal. C,D. Fracture stabilized with a lag screw and a neutralization plate. E,F. Short transverse fracture of the second metacarpal stabilized with a compression plate. (C,D: Copyright Thomas R. Hunt III, MD, DSc.)



TECH FIG 6 • A,B. Intra-articular head fracture of the fourth metacarpal. C. Dorsal approach to an MP joint. Extensor tendon beneath top retractor. Capsule grabbed by pickup forceps. Articular cartilage seen deep to capsule. D,E. Intra-articular fracture stabilized with headless screws. (continued)


TECH FIG 6 • (continued) F,G. Intra-articular head fracture stabilized with extra-articular screws.



TECH FIG 7 • A,B. Coronal intra-articular fracture that extends to the metacarpal neck. C,D. If there is no comminution, the fracture can be addressed through a volar approach and stabilized with lag screws.
PEARLS AND PITFALLS
|Natural ▪ Many metacarpal fractures can do exceedingly well with minimal intervention. historyFight bites ▪ Be vigilant of small lacerations near the MP joint, which may be the only sign of a fight bite that needs urgent débridement to prevent a devastating infection.Severe ▪ Polytrauma patients with severe hand injuries are at risk of missed injuries, open trauma fractures, compartment syndrome, and intrinsic contracture.|Mobilization ▪ Allow tendon-gliding exercises as early as possible to minimize scar formation.1. Critical structures can be protected during drilling by using the oscillation mode.Drilling1. Pins can be used to manipulate the fracture to a reduced position.2. Sometimes, it is easier to apply the plate to one side of the fracture and then perform the reduction and fixation to the opposite side of the fracture.3. Always check finger rotation prior to completing fixation.Fracture reduction
POSTOPERATIVE CARE
P.470Immobilization in the postoperative period will depend on the stability of the reconstruction and the status of the soft tissues.Fractures stabilized with retrograde (collateral recess) or transverse pins should be immobilized with the MP joints flexed 70 to 90 degrees for 3 to 4 weeks while the pins are in place. The IP joints should be allowed to move to minimize stiffness.Fractures stabilized with antegrade (bouquet) pins should be immobilized with the MP joints flexed 70 to 90 degrees for 3 to 4 weeks. Some authors allow early motion of the MP joint with bouquet pinning,understanding that there may be some loss of reduction.3Fractures that have been stabilized with rigid fixation such as plates or screws should be immobilized in a splint with the MP joints flexed 70 to 90 degrees for 4 to 7 days. An early motion program can then be instituted. A removable splint in the functional position should be used for protection until fracture stability.A hand therapist can be consulted if significant stiffness or lack of progress is noted during the early recovery period. However, in patients with severe injuries, it is often best to start therapy early.Protected activities should continue until fracture stability, which is often at least 4 to 6 weeks. In cases of delayed union, bone grafting can be considered.If plates are bothersome, they can be removed as early as 4 to 6 months after fracture consolidation.
OUTCOMES
Metacarpal shaft fractures with limited shortening (2 to 5 mm) do well without surgery due to the stabilizing effect of the adjacent metacarpal and supporting ligaments.8Fractures of the fifth metacarpal neck that have healed with significant angulation of up to 70 degrees can have satisfactory outcomes.6,15Percutaneous pins can stabilize the reduction of many distal and proximal metacarpal shaft fractures. In the treatment of metacarpal neck fractures, antegrade (bouquet) pinning may lead to less stiffness of the MP joint compared to retrograde (collateral recess) and transverse pinning.10,16Plate fixation of short oblique, transverse, or multiple metacarpal fractures can provide the necessary stability to start an early motion program but on occasion will require hardware removal.11Screw fixation of articular head fractures can stabilize the fracture, but a degree of stiffness of the MP joint is expected.13
COMPLICATIONS
Some degree of stiffness affects the surgical treatment of most metacarpal fractures.Stiffness of the MP joint can originate from contracture of the collateral ligaments and capsule after a period of immobilization. It may also occur from adhesions of the extensor tendons, especially after an open approach. Early mobilization as tolerated by the fixation can minimize it.Extension lag may develop from fracture shortening or tendon adhesions. Loss of articular congruity of the metacarpal head may block motion.Malrotation is poorly tolerated by most patients and should be addressed surgically.The dorsal sensory branches of the ulnar and radial nerve are very sensitive to manipulation.The deep motor branch of the ulnar nerve can be caught in the cutting tips of an inadvertent drill passage.Even though nonunions of metacarpal are rare, delayed unions can be seen, especially in short transverse fractures treated with a plate. If a nonunion does develop and the plate breaks, consideration should be given to bone grafting and revision fixation.Pin site infections can often be treated with oral antibiotics until the pins can be safely removed.
REFERENCES
- Day CS, Stern PJ. Fractures of the metacarpals and phalanges. In: Wolfe SW, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 6. Philadelphia: Elsevier, 2011:239-258.
- Diaz-Garcia R, Waljee JF. Current management of metacarpal fractures. Hand Clin 2013;29(4):507-518.
- Downing ND, Davis TR. Intramedullary fixation of unstable metacarpal fractures. Hand Clin 2006;22:269-277.
- Eichenholtz SN, Rizzo PC III. Fracture of the neck of the fifth metacarpal bone—is overtreatment justified? JAMA 1961;178:425-426.
- Hofmeister EP, Kim J, Shin AY. Comparison of 2 methods of immobilization of fifth metacarpal neck fractures: a prospective randomized study. J Hand Surg Am 2008;33(8):1362-1368.
- Hunter JM, Cowen NJ. Fifth metacarpal fractures in a compensation clinic population. A report on one hundred and thirty-three cases. J Bone Joint Surg Am 1970;52:1159-1165.
- Jupiter JB, Belsky MR. Fracture and dislocations of the hand. In: Browner BD, Jupiter JB, Levine AM, et al, eds. Skeletal Trauma. Philadelphia: WB Saunders, 1992:925-1024.
- Khan A, Giddins G. The outcome of conservative treatment of spiral metacarpal fractures and the role of the deep transverse metacarpal ligaments in stabilizing these injuries. J Hand Surg Eur Vol 2015;40(1):59-62.
- Manueddu CA, Della Santa D. Fasciculated intramedullary pinning of metacarpal fractures. J Hand Surg Br 1996;21(2):230-236.
- Schädel-Höpfner M, Wild M, Windolf J, et al. Antegrade intramedullary splinting or percutaneous retrograde crossed pinning for displaced neck fractures of the fifth metacarpal? Arch Orthop Trauma Surg 2007;127:435-440.
- Souer JS, Mudgal CS. Plate fixation in closed ipsilateral multiple metacarpal fractures. J Hand Surg Eur Vol 2008;33(6): 740-744.
- Strauch RJ, Rosenwasser MP, Lunt JG. Metacarpal shaft fractures: the effect of shortening on the extensor tendon mechanism. J Hand Surg Am 1998;23(3):519-523.
- Tan JS, Foo AT, Chew WC, et al. Articularly placed interfragmentary screw fixation of difficult condylar fractures of the hand. J Hand Surg Am 2011;36:604-609.
- Tavassoli J, Ruland RT, Hogan CJ, et al. Three cast techniques for the treatment of extra-articular metacarpal fractures: comparison of short-term outcomes and final fracture alignments. J Bone Joint Surg Am 2005;87:2196-2201.
- van Aaken J, Kämpfen S, Berli M, et al. Outcome of boxer's fractures treated by a soft wrap and buddy taping: a prospective study. Hand 2007;2(4):212-217.
- Winter M, Balaguer T, Bessière C, et al. Surgical treatment of the boxer's fracture: transverse pinning versus intramedullary pinning. J Hand Surg Eur Vol 2007;32:709-713.
