Operative Treatment of Finger Carpometacarpal Joint Fracture-Dislocations
DEFINITION
Fractures and dislocations of the carpometacarpal (CMC) joints of the index through small fingers involve intraarticular fractures at the base of the metacarpals or pure dislocations between the metacarpals and carpus. The fracture can involve the base of the metacarpal or the trapezoid, capitate, or hamate articular surface.These fractures and dislocations can result in instability and articular incongruity (FIG 1).
ANATOMY


FIG 1 • A,B. Multiple dorsal CMC dislocations involving the index through small fingers. The ring and small fingers have a gliding articulation on the hamate, which allows for the closure of the handaround objects and is very important in power grip. This mobility makes them more susceptible to injury. The extensor carpi ulnaris tendon attaches to the dorsal base of the small finger metacarpal.4The deep motor branch of the ulnar nerve crosses around the base of the hamate hook from ulnar to radial and runs along the volar surface of the CMC joints (FIG 2B). It is vulnerable at the time of injury or during fixation.
PATHOGENESIS

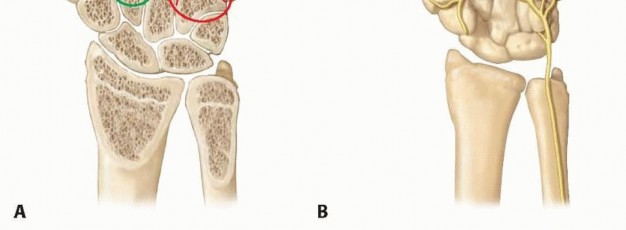
FIG 2 • A. Variable articular congruity of the various CMC joints. B. Deep motor branch of the ulnar nerve adjacent to the metacarpal bases.
NATURAL HISTORY
The natural result of an untreated fracture-dislocation is progressive arthritis of the involved joints. This occurs due to progressive subluxation of the joint(s) and articular incongruity (FIG 4A-D).
PATIENT HISTORY AND PHYSICAL FINDINGS


IMAGING AND OTHER DIAGNOSTIC STUDIES


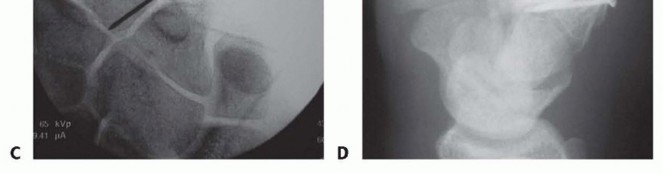
FIG 4 • A. PA radiograph demonstrating subluxation of index through small finger metacarpal bases and thumb metacarpal fracture. B. Lateral radiograph of subluxated metacarpals. C. PA radiograph of same patient demonstrating complete dislocation 2 weeks after injury. D. Lateral view demonstrating dislocation.

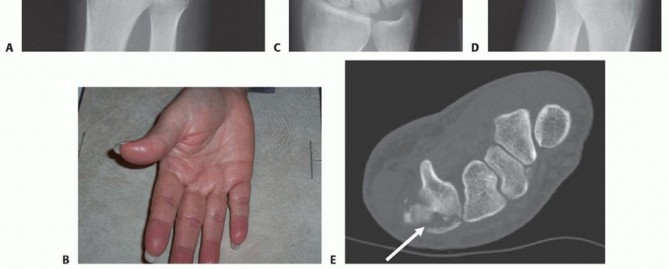
FIG 5 • A. A conventional PA view of the hand creates an oblique view of the ring and small finger bases. B. Hand properly positioned for AP view of the ring and small finger CMC joints. C. Postoperative PA film after open reduction with internal fixation of the ring and small finger CMC joints. D. AP projection clearly shows the joint reduction in the same patient shown in C. E. CT scan of the fracture of the dorsal lip of the hamate. Arrow indicates hamate comminution and displacement of dorsal lip fragment.P.450A true frontal radiograph is most easily obtained by positioning the hand in an anteroposterior (AP) projection with the dorsum of the hand placed flat on the cassette (or image intensifier, if using fluoroscopy). The base of the affected metacarpal should lie on the cassette (FIG 5B). This will result in a far more accurate portrayal of the joint, essential for assessing the fracture as well as checking hardware position after fixation.Visualization of the joint surfaces at the base of the ring and small fingers differs in a typical PA projection (FIG 5C) and a properly positioned film of the same patient (FIG 5D).The same principle holds for obtaining lateral radiographs. A semisupinated lateral view will best visualize the base of the index and middle CMC joints,5 and a semipronated lateral view will best show the bases of the ring and small finger CMC joints.2A computed tomography (CT) scan should be obtained in most cases to assess for articular injury. CT also is especially helpful for visualizing impacted articular surface fragments. The best visualization and determination of fracture patterns will be possible if the scan is obtained after preliminary reduction of any displaced fracturesor dislocations associated with a fracture (FIG 5E).10
DIFFERENTIAL DIAGNOSIS
Metacarpal fracture Carpal bone fracture CMC fracture-dislocationFracture associated with neurovascular injury
NONOPERATIVE MANAGEMENT


SURGICAL MANAGEMENT
PREOPERATIVE PLANNING
Careful review of all imaging studies will facilitate planning of fracture fragment exposure and identify sites for internal fixation.
POSITIONING
The patient is positioned supine on the operating table with a standard arm table.The surgeon often is more comfortable seated on the head side of the arm table. This avoids the neck strain that may result from looking “over the top” that happens when the arm externally rotates and the surgeon is seated on the axilla side of the table (FIG 6A).
APPROACH
A dorsal extensile approach provides satisfactory exposure of any of the CMC joints. Incisions placed between metacarpals allow access to two adjacent joints.Cross the wrist with oblique extensions if necessary.Marking out the anticipated locations of nearby nerve branches can be helpful (FIG 6B).P.451
TECHNIQUES
DORSAL EXPOSURE

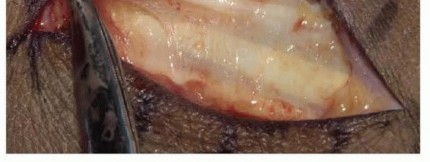
TECH FIG 1 • Dorsal cutaneous branch of the ulnar nerve crossing the incision.
FRACTURE EXPOSURE
FRACTURE REDUCTION



TECH FIG 2 • A. Provisional fracture reduction using the hamate surface as a mold for articular reduction of the metacarpal base. B. Initial reduction of the shaft and stabilization of the articular surface. (continued)

TECH FIG 2 • (continued) C. Fluoroscopic view of articular reduction. D. Dorsal hamate lip fixation with three screws.
DEFINITIVE FIXATION


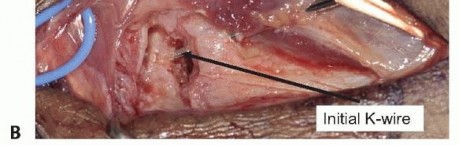
TECH FIG 3 • A. Fracture-dislocation of the ring and small finger metacarpal bases using pins and a screw. B. Percutaneous K-wire fixation of a metacarpal shaft fracture and CMC dislocation. Simple K-wire fixation is satisfactory for isolated dislocations with fracture (TECH FIG 3B).The insertion point for a percutaneous wire often is quite distant from the dislocation site in crushed and severely swollen hands.4. Adjunctive TechniquesThe construct can be protected by placing the affected metacarpal under slight distraction and pinning it to the adjacent metacarpal.Alternatively, the proximally directed deforming force of the extensor carpi ulnaris can be reduced by detaching it from the base of the small finger metacarpal at the beginning of the procedure and securing it to the hamate at the close, thereby avoiding proximal pull on the base of the small finger metacarpal.I have never found it necessary to use this alternative approach, but it may be helpful in a delayed presentation, where myostatic contractures due to shortening are present.P.453PEARLS AND PITFALLS
|||Imaging ▪ Ensure that adequate radiographs are available for intraoperative review.1. If necessary, obtain a CT scan.Positioning ▪ It is often easier for the surgeon to be seated on the outside of the hand table, instead of in the axilla between the table and patient, due to the limited internal rotation present in the shoulder, which can make visualization difficult from the usual seating position.Exposure ▪ The dorsal cutaneous branch of the ulnar nerve crosses the incision obliquely and lies immediately across the operative field for exposure of the fourth and fifth CMC joints. Cutting this nerve often is associated with very symptomatic neuromas, although the sensory deficit is well tolerated.Fracture ▪ Fragments can be small, and periosteal stripping can result in devitalization. Use management fracture lines for visualization of the articular surface as much as possible. A dentalpick, fine K-wire joysticks, and provisional fixation before final screw insertion can be helpful. Provisional fixation should be done with careful attention to the anticipated location of definitive fixation. Avoid malrotation of the shaft during reduction by grasping it together with one or two adjacent metacarpals when aligning it relative to the joint. Small degrees of malrotation at the base of the metacarpal can result in substantial distal overlap of the digits.Postoperative ▪ Consider placing a temporary distraction K-wire between adjacent metacarpals to protection limit the load placed on the articular surface before it has healed.|------
POSTOPERATIVE CARE
Aftercare following operative fixation falls into three general phases: acute swelling control and wound healing (10 to 14 days), fracture consolidation and maintenance of digit range of motion (4 to 6 weeks), and restoration of global hand function and strength (2 to 6 months).Immediate measures following surgery include strict elevation and range-of-motion exercises through a full arcof motion.4 This limits swelling, reduces pain, and prevents accumulation of protein-rich edema fluid that will slow rehabilitation.The relative speed at which the hand can be mobilized during the weeks after surgery depends on a number of factors, including the magnitude of the original injury, stability of fixation, reliability of the patient, and specific occupational or athletic needs.The radiograph in TECH FIG 2D shows the hand of a physician with stable fixation of a dorsal hamate injury who was mobilized and given a 1-pound lifting restriction shortly after surgery to allow continuation of his residency training.In contrast, unreliable patients require immobilization for 6 weeks in a cast (see TECH FIG 3B).Patients should be warned that full grip strength is the last thing that will recover and may take months.2 It is not uncommon for patients to report pain with a handshake for an extended period of time.
OUTCOMES

COMPLICATIONS
Complications include those common to any periarticular surgery: Failure of wound healingHematoma formationNeurovascular injury Neuroma formation Tendon adhesions Posttraumatic arthritis Nonunion or malunion Joint stiffness WeaknessOccasionally, small fragments may resorb, leading to collapse and articular incongruity (FIG 7). Long-term arthritis can be treated with fusion of the affected joint.4 FIG 7 • Radiograph taken several months following K-wire fixation of a fracture-dislocation of the fifth CMC joint. Fragments were too small for screw fixation and were resorbed. P.454Alternatively, an interposition “anchovy” using the palmaris longus as a biologic spacer can be inserted after resection of the arthritic joint surfaces, analogous to that performed for thumb basal joint arthritis.3A recent report described using a proximal interphalangeal (PIP) joint silicone implant as an interposition spacer in the fifth metacarpal-hamate interspace for three patients with chronic arthritis of the fifth CMC-hamate joint.13 The follow-up was extremely short (mean 20 months), and the known propensity for silicone implant fracture over time will determine whether this is a satisfactory long-term solution for patients with this form of arthritis.
REFERENCES
- Bergfield TG, DuPuy TE, Aulicino PL. Fracture-dislocations of all five carpometacarpal joints: a case report. J Hand Surg Am 1985;10: 76-78.
- Bora FW Jr, Didizian NH. The treatment of injuries to the carpometacarpal joint of the little finger. J Bone Joint Surg Am 1974;56: 1459-1463.
- Gainor BJ, Stark HH, Ashworth CR, et al. Tendon arthroplasty of the fifth carpometacarpal joint for treatment of posttraumatic arthritis. J Hand Surg Am 1991;16:520-524.
- Glickel SZ, Barron OA, Catalano LW. Dislocations and ligament injuries in the digits. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Churchill Livingstone, 2005:364-366.
- Hsu JD, Curtis RM. Carpometacarpal dislocations on the ulnar side of the hand. J Bone Joint Surg Am 1970;52:927-930.
- Kjaer-Petersen K, Jurik AG, Petersen LK. Intra-articular fractures at the base of the fifth metacarpal: a clinical and radiographical study of 64 cases. J Hand Surg Br 1992;17:144-147.
- Lawliss JF III, Gunther SF. Carpometacarpal dislocations. J Bone Joint Surg Am 1991;73:52-59.
- Lilling M, Weinberg H. The mechanism of dorsal fracture dislocation of the fifth carpometacarpal joint. J Hand Surg Am 1979;4:340-342.
- Lundeen JM, Shin AY. Clinical results of intraarticular fractures of the base of the fifth metacarpal treated by closed reduction and cast immobilization. J Hand Surg Br 2000;25:258-261.
- Marck KW, Klasen HJ. Fracture-dislocation of the hamatometacarpal joint: a case report. J Hand Surg Am 1986;11:128-130.
- Papaloizos MY, Le Moine PH, Prues-Latour V, et al. Proximal fractures of the fifth metacarpal: aretrospective analysis of 25 operated cases. J Hand Surg Br 2000;25:253-257.
- Petrie PW, Lamb DW. Fracture-subluxation of the base of the fifth metacarpal. Hand 1974;6:82-86.
- Proubasta IR, Lamas CG, Ibañez NA, et al. Treatment of little finger carpometacarpal posttraumatic arthritis with a silicone implant. J Hand Surg Am 2013;38(10):1960-1964.
