INTRODUCTION TO PEDAL MALUNIONS
The human foot is a highly complex, load-bearing structure designed to adapt to uneven terrain while providing a rigid lever for terminal stance and propulsion. Fractures of the pedal skeleton, when healed in suboptimal alignment, disrupt this delicate biomechanical equilibrium. Malunions within the foot rarely present merely as cosmetic concerns; they frequently manifest as debilitating pain, intractable plantar keratoses (IPK), transfer metatarsalgia, and progressive secondary osteoarthritis.
The objective of surgical intervention for any foot malunion is the restoration of a painless, plantigrade, and functional foot. Cosmetic improvement, while psychologically beneficial to the patient, is rarely a primary indication for operative reconstruction. This comprehensive guide details the pathoanatomy, preoperative evaluation, and surgical management of malunions affecting the phalanges, metatarsals, and the talus.
MALUNION OF THE PHALANGES OF THE TOES
Pathoanatomy and Clinical Presentation
Malunion of fractures involving the phalanges of the toes rarely causes sufficient functional disability to justify surgical intervention. The lesser toes primarily serve to increase the weight-bearing surface area during the terminal stance phase of gait, but they do not require highly skillful or independent movements.
However, a severe angular or rotational deformity can lead to adjacent digit impingement, overriding toes, or painful dorsal corns secondary to shoe wear friction. In the hallux, malunion can disrupt the windlass mechanism, leading to altered first ray mechanics and secondary metatarsophalangeal (MTP) joint arthrosis.
Surgical Indications and Techniques
When a phalangeal deformity causes intractable pain or recurrent skin breakdown that fails conservative management (e.g., wide toe-box shoes, silicone toe spacers), surgical correction is indicated.
Surgical Approach:
Correction is typically achieved through a dorsal or mid-lateral longitudinal incision.
1. Lateral Approach: Preferred for lesser toes to avoid the dorsal extensor apparatus and the plantar neurovascular bundles.
2. Dorsal Approach: Utilized when addressing the MTP joint or when a dorsal closing wedge osteotomy is planned. Meticulous care must be taken to retract and protect the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons.
Operative Options:
* Corrective Osteotomy: For extra-articular malunions with good joint mobility, a simple closing wedge or derotational osteotomy at the apex of the deformity, stabilized with a 0.045-inch Kirschner wire (K-wire), is often sufficient.
* Resection Arthroplasty: For complete correction of severe, rigid deformities—particularly those involving the interphalangeal joints—wide resection of the malunited segment or a partial phalangectomy (e.g., DuVries arthroplasty) may be required.
Clinical Pearl: Wide resection of the phalanges can be performed with relative impunity in the lesser toes, as fine motor control is not a functional prerequisite. However, maintaining the integrity of the plantar plate and flexor tendons is crucial to prevent a flail toe.
MALUNION OF THE METATARSALS
Biomechanics and Pathoanatomy
The metatarsals form the anterior structural arch of the foot. Malunion of the metatarsal neck or shaft is highly disabling if the distal fragment heals with plantar angulation. Because the metatarsal heads bear significant weight during the propulsive phase of gait, plantar angulation drives the metatarsal head into the sole, producing a prominent osseous mass.
This localized pressure leads to the formation of a painful intractable plantar keratosis (IPK). If the original fracture was severely comminuted, the resulting hypertrophic callus and malunion mass may be so prominent that it clinically simulates a soft tissue or osseous tumor. Conversely, dorsal angulation malunions elevate the metatarsal head, rendering it incompetent for weight-bearing and transferring the load to adjacent metatarsals (transfer metatarsalgia).
Pediatric Considerations
In the pediatric population, the approach to metatarsal malunion is markedly different due to the robust remodeling potential of the immature skeleton.
Surgical Warning: Surgery should not aim to restore perfect radiographic apposition in children younger than 9 years old.
Spontaneous correction of angulation occurs predictably with growth, governed by Wolff's Law. Remodeling is most robust when the deformity is:
1. Near a joint (e.g., juxta-epiphyseal).
2. In the plane of motion of that adjacent joint (sagittal plane).
An offset in an epiphysis usually corrects itself spontaneously provided the physis (growth plate) has not been irreversibly injured at the time of the initial trauma.
Preoperative Planning and Deformity Analysis
Operative treatment of malunion for most metatarsal fractures should be delayed until 6 to 12 months post-injury. This allows for maximal spontaneous remodeling, resolution of soft tissue edema, and stabilization of the fracture callus.
Exceptions to Delayed Surgery: Intra-articular malunions require earlier intervention to prevent rapid, irreversible post-traumatic arthrosis.
Before proceeding, the surgeon must evaluate the degree of disuse osteoporosis and soft tissue atrophy. In cases of severe osteopenia, a period of active rehabilitation and weight-bearing may be preferable prior to attempting osteotomy and internal fixation.
Trigonometric Analysis of Deformity
Analysis of the deformity must recognize that most complex angulations can be resolved into a single true plane of deformity, which is a combination of the anteroposterior (AP) and varus/valgus (lateral) projections.
Ries and O’Neill developed a highly effective trigonometric analysis of long bone deformity. They designed a graphical method to determine the true maximal deformity based on standard orthogonal (AP and lateral) radiographs.
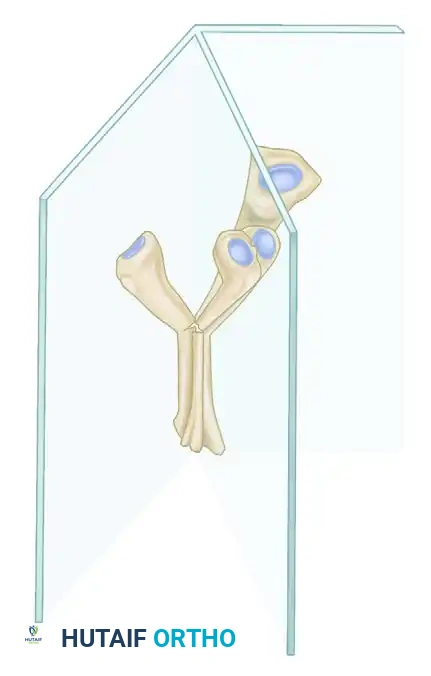
Above: A representation of a fracture angulated in a complex oblique plane, situated between the standard anteroposterior (AP) and lateral (LAT) radiographic planes.
To accurately plan a corrective osteotomy, the surgeon must calculate the true angle of deformity. The apparent angles seen on 2D radiographs are merely projections of this true 3D angle.
Above: The Ries and O’Neill method for determining bony deformity. CAD represents the angle measured on the AP radiograph; CAB represents the angle measured on the lateral radiograph. CAE represents the true magnitude of the deformity in its actual oblique plane (T).
By utilizing these trigonometric principles, the surgeon can plan a single-cut osteotomy (such as a closing wedge) that simultaneously corrects both the sagittal and coronal plane deformities.
Surgical Techniques for Metatarsal Malunion
1. Dorsal Closing Wedge Osteotomy:
For the classic plantar-angulated metatarsal malunion causing an IPK, a dorsal closing wedge osteotomy at the apex of the deformity (CORA - Center of Rotation of Angulation) is the workhorse procedure.
* Approach: A dorsal longitudinal incision over the affected metatarsal.
* Technique: The extensor tendons are retracted. A wedge of bone, based dorsally, is excised using an oscillating saw. The plantar cortex is ideally left intact to act as a hinge, though it often breaks during closure.
* Fixation: The osteotomy is closed, elevating the metatarsal head out of the plantar weight-bearing plane. Fixation is achieved with a dorsal plate and screws or crossed K-wires.
2. Ilizarov and Circular External Fixation:
For complex malunions involving significant shortening (brachymetatarsia secondary to overlap malunion) or multi-planar deformities, acute correction may stretch the neurovascular bundles excessively.
Ilizarov pioneered work on intercalary limb regeneration using circular external fixation techniques and various hinged constructs.
* Application: Miniature circular or monolateral rail frames allow for the simultaneous, gradual restoration of alignment, rotation, and length via distraction osteogenesis.
* Requirement: These techniques demand a profound understanding of cross-sectional anatomy to avoid pin-tract infections and tendon tethering.
3. Compensatory Procedures and Salvage:
Corrective surgery at the exact site of the malunion is not always feasible due to poor bone stock, previous infection, or severe comminution. In such instances, compensatory procedures (e.g., a Weil osteotomy distal to the malunion to elevate the head) may be necessary. If pain is the predominant symptom and the adjacent MTP or tarsometatarsal (TMT) joint is arthritic, arthrodesis (fusion) of the involved joint is the definitive salvage procedure.
MALUNION OF THE TALUS
Pathoanatomy and Biomechanics
The talus is the critical biomechanical link between the leg and the foot, distributing forces from the tibia to the calcaneus and the midfoot. It is unique in that approximately 60% of its surface is covered by articular cartilage, and it has no muscular attachments.
Malunion of a fracture of the talus is almost always seriously disabling. Whether the neck, the body, or both are involved, malunion produces profound incongruity and irregularity of the ankle (tibiotalar), subtalar (talocalcaneal), or talonavicular joints.
Malunion of the Talar Neck
Malunited fractures of the talar neck are biomechanically and biologically analogous to intracapsular fractures of the femoral neck.
Vascular Implications:
The tenuous blood supply to the talar body (primarily from the artery of the tarsal canal, a branch of the posterior tibial artery) is frequently disrupted during the initial trauma. Malunion, especially with significant displacement, further impairs local microcirculation. This can precipitate progressive degeneration, subchondral collapse, or frank osteonecrosis (avascular necrosis - AVN) of the talar head or body, leading to devastating articular irregularity.
Deformity Patterns:
Union of the talar neck may occur with the distal fragment (talar head) in rotation, lateral deviation, or medial deviation.
* Valgus Malunion: This is the most common deformity pattern. The talar head deviates medially and dorsally. This results in a flattened longitudinal arch, a pronated midfoot, and impingement of the lateral column.
* Varus Malunion: Less common but highly symptomatic. The talar head deviates laterally and plantarly. This forces the foot into a rigid, supinated position. The patient walks on the lateral border of the foot, leading to rapid overload of the fifth metatarsal, recurrent ankle sprains, and peroneal tendon pathology. Furthermore, varus malunion blocks the normal eversion of the subtalar joint, severely limiting the foot's ability to accommodate uneven ground.
Surgical Management of Talar Malunions
The surgical approach to talar malunions is dictated by the presence of adjacent joint arthrosis, the viability of the talar body (presence of AVN), and the exact plane of the deformity.
1. Corrective Osteotomy (Joint-Sparing):
In rare cases where the malunion is identified early, the articular cartilage of the subtalar and talonavicular joints remains pristine, and there is no evidence of osteonecrosis, a corrective opening or closing wedge osteotomy of the talar neck can be attempted.
* Approach: A dual anteromedial and anterolateral approach is often required to fully visualize the talar neck and protect the neurovascular structures.
* Technique: For a varus malunion, a medially based opening wedge osteotomy (using structural autograft from the iliac crest) is performed to restore the anatomic neck-body angle. Rigid fixation with headless compression screws or mini-fragment plates is mandatory.
2. Triple Arthrodesis (The Gold Standard Salvage):
Historically and currently, the definitive treatment for symptomatic varus or valgus malunion of the talar neck—especially when accompanied by subtalar or talonavicular arthrosis—is a triple arthrodesis.
* Indications: Rigid deformity, established post-traumatic arthritis, or early-stage osteonecrosis where the structural integrity of the talus can still support fusion.
* Technique: The procedure involves the surgical fusion of the subtalar, talonavicular, and calcaneocuboid joints.
* The articular cartilage is meticulously denuded down to bleeding subchondral bone.
* The deformity is corrected acutely by selective wedge resections of the joint surfaces (e.g., taking a laterally based wedge from the subtalar joint to correct a varus deformity).
* The foot is positioned in 5 degrees of valgus, neutral dorsiflexion, and slight external rotation to match the contralateral limb.
* Rigid internal fixation is achieved using large-fragment cannulated screws.
Clinical Pearl: When performing a triple arthrodesis for a talar malunion, the talonavicular joint must be reduced and fixed first to establish the medial column length and rotation, followed by the subtalar joint, and finally the calcaneocuboid joint.
3. Pantalar Arthrodesis or Talectomy:
In catastrophic cases involving severe malunion of the talar body with complete osteonecrosis, collapse, and pan-tarsal arthritis, a triple arthrodesis is insufficient.
* Pantalar Arthrodesis: Involves fusion of the tibiotalar joint in addition to the triple arthrodesis joints. This provides a stable, painless, but highly rigid plantigrade foot.
* Talectomy (Astragalectomy) with Tibiocalcaneal Fusion: If the talar body is completely necrotic and fragmented, it must be excised. The tibia is then fused directly to the calcaneus (often utilizing an intramedullary retrograde nail). This results in limb shortening but provides a durable, vascularized, weight-bearing construct.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Regardless of the specific bone addressed, the postoperative management of foot malunion surgery requires strict adherence to biological healing principles.
- Phase I (0-6 Weeks): Strict non-weight-bearing in a well-padded short leg cast or rigid fracture boot. Elevation is critical to manage edema and prevent wound dehiscence, particularly following complex midfoot or hindfoot reconstructions.
- Phase II (6-12 Weeks): Clinical and radiographic evaluation of osteotomy/fusion site healing. If bridging trabeculae are visible, the patient may begin progressive partial weight-bearing in a CAM (Controlled Ankle Motion) boot. Active range of motion exercises for non-fused joints are initiated.
- Phase III (3-6 Months): Transition to regular footwear, often requiring custom orthotics to accommodate minor residual deformities or to support the newly reconstructed arch. Physical therapy focuses on proprioception, peroneal strengthening, and gait retraining.
