INTRODUCTION AND HISTORICAL PERSPECTIVE
The "painful heel" represents one of the most ubiquitous, yet historically misunderstood, clinical entities in orthopaedic surgery. In 1922, Stiell astutely observed that "painful heel appears to be a condition which is seldom efficiently treated, for the simple reason that the causation is not exactly diagnosed." Over four decades later, Lapidus and Guidotti (1965) echoed this sentiment, noting that the term was used deliberately in lieu of a precise etiological diagnosis because the exact cause remained elusive. Today, despite advanced imaging and biomechanical modeling, the precise, inclusive cause of pain beneath the anteromedial prominence of the calcaneal tuberosity remains a complex interplay of mechanical, degenerative, and neurogenic factors.
While historical misattributions to gonorrhea and tuberculosis have been rightfully discarded, the modern economic and epidemiological burden of this condition is staggering. Tong and Furia reported that over 2 million patients are treated for plantar fasciitis annually in the United States alone, with estimated treatment costs ranging from $192 million to $376 million (2007 data). For the orthopaedic surgeon, mastering the differential diagnosis, biomechanics, and precise surgical indications is paramount to resolving this often frustrating condition.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of plantar anatomy is the foundation of both conservative and operative management. The plantar aponeurosis is a thickened fibrous band of connective tissue divided into three distinct components: medial, central, and lateral.
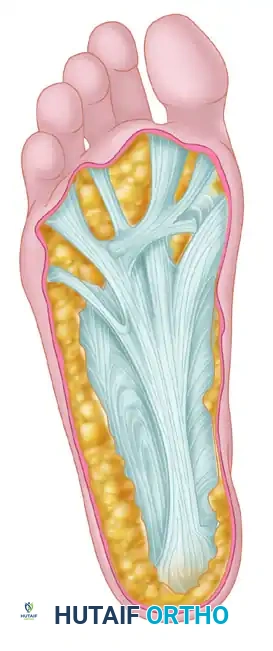
The central component is the most robust, originating from the medial process of the calcaneal tuberosity. It courses distally, dividing into five slips that insert into the plantar plates of the metatarsophalangeal (MTP) joints, the flexor tendon sheaths, and the bases of the proximal phalanges.
The Windlass Mechanism
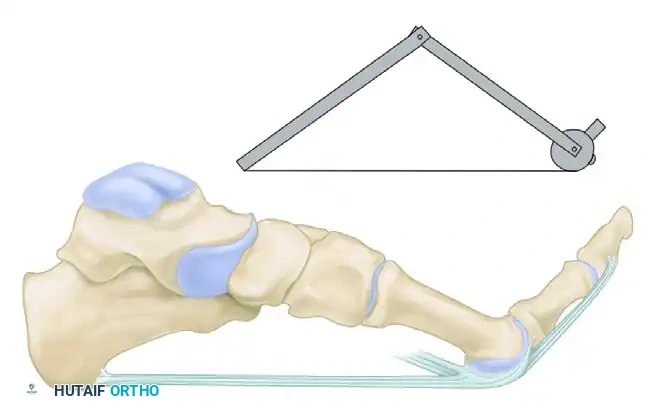
The biomechanical function of the plantar fascia is best conceptualized through the "windlass mechanism," first postulated by the English anatomist Hicks. The plantar fascia acts as a dynamic cable. As the toes are dorsiflexed during the terminal stance phase of gait, the plantar fascia is wound around the "drum" of the metatarsal heads.
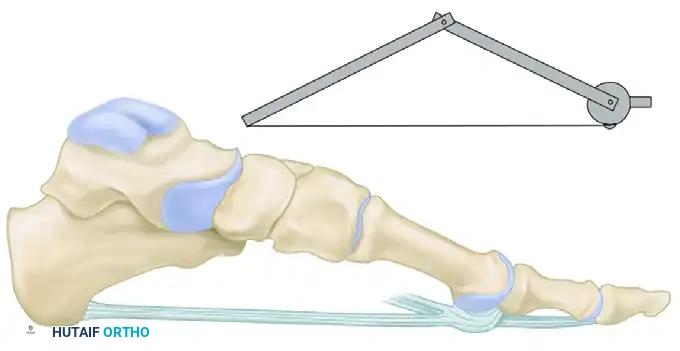
When the foot is in a neutral position, the fascia remains at resting length. However, upon dorsiflexion of the digits, this tightening of the fascial cable elevates the longitudinal arch, locking the midtarsal joints and converting the foot into a rigid lever for propulsion.
This dynamic elevation places immense traction on the origin of the plantar fascia at the medial calcaneal tubercle. The most dense, unyielding section of the plantar aponeurosis originates precisely where the most common point of local tenderness is elicited during clinical examination.
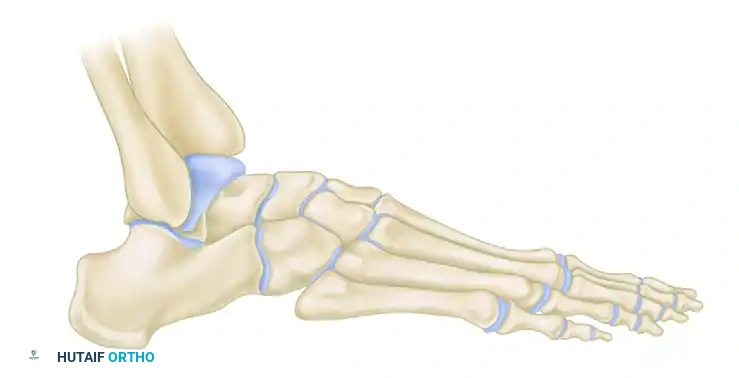
Bony Anatomy and the "Heel Spur"
Radiographic evaluation often reveals a traction spur on the anteromedial, plantar aspect of the calcaneal tuberosity.
Clinical Pearl: It is a common misconception that the calcaneal heel spur is located within the origin of the plantar fascia. Anatomical studies demonstrate that this traction spur actually coincides with the origin of the flexor digitorum brevis (FDB) muscle, which lies immediately deep to the plantar fascia. The spur itself is rarely the primary source of nociception; rather, it is a radiographic marker of chronic biomechanical overload.
ETIOLOGY AND PATHOGENESIS
The etiology of painful heel syndrome is multifactorial, encompassing degenerative, mechanical, and neurogenic components.
Degenerative Fasciosis
Similar to the angiofibroblastic tendinosis seen in the extensor carpi radialis brevis in "tennis elbow," plantar fasciitis is more accurately described as "plantar fasciosis." Repetitive traction and aging produce microscopic tears, collagen degeneration, and cystic changes at the fascial origin. Furthermore, aging brings about a gradual reduction in collagen, water content, and elastic fibrous tissue within the elastic adipose tissue of the heel pad. This heel pad atrophy significantly diminishes shock absorption, exacerbating soreness under the calcaneal tuberosity.
Neurogenic Entrapment (Baxter's Nerve)
A critical, yet frequently overlooked, cause of painful heel syndrome is the entrapment of the first branch of the lateral plantar nerve (Baxter's nerve). Schon and Baxter proposed that 1% to 2% of patients with chronic heel pain suffer from this neurogenic pathology.
The nerve passes between the deep surface of the abductor hallucis and the medial margin of the quadratus plantae, coursing laterally toward the abductor digiti minimi. Entrapment typically occurs at the deep fascial edge of the abductor hallucis muscle or adjacent to the calcaneal spur.
Diagnostic Pitfall: Patients with isolated plantar fasciitis exhibit tenderness strictly at the medial calcaneal tubercle. In contrast, patients with Baxter's nerve entrapment will demonstrate maximal tenderness radiating along the course of the lateral plantar nerve, inferior to the flexor retinaculum, and often present with a positive Tinel's sign over the nerve.
DIFFERENTIAL DIAGNOSIS
A rigorous diagnostic workup is mandatory to exclude systemic or infectious etiologies before diagnosing idiopathic painful heel syndrome. The differential diagnosis must include:
- Mechanical/Overuse: Heel cord tendinitis, retrocalcaneal bursitis, posterior tibial tendinitis, peroneal tendinitis, and flexor hallucis longus (FHL) tendinitis.
- Systemic Arthropathies: In men younger than 40 years presenting with bilateral painful heels, seronegative spondyloarthropathies (Ankylosing Spondylitis, Reiter Syndrome/Reactive Arthritis) must be aggressively ruled out via HLA-B27 testing and sacroiliac imaging. Women with bilateral symptoms should be evaluated for Rheumatoid Arthritis.
- Infectious: Deep soft tissue abscesses or calcaneal osteomyelitis must be considered, particularly in diabetic or immunocompromised patients.
- Traumatic: Calcaneal stress fractures (diagnosed via MRI or bone scan).
PREOPERATIVE PLANNING AND INDICATIONS
Surgical intervention is strictly reserved for recalcitrant cases that have failed a comprehensive, 6- to 12-month regimen of conservative management (stretching, orthotics, night splints, NSAIDs, and judicious corticosteroid or PRP injections).
The Role of the Achilles Tendon
It is imperative to evaluate the patient for concomitant heel cord insufficiency or equinus contracture. However, caution is advised. Chilvers et al. described a severe heel overload syndrome associated with heel cord insufficiency following overly aggressive heel cord lengthening. Risk factors for this complication include diabetes, an insensate heel, obesity, and ipsilateral first toe amputation.
Surgical Warning: The plantar fascia is the most important static support for the longitudinal arch. Extensive laboratory studies demonstrate that complete sectioning of the plantar fascia results in catastrophic arch collapse, midfoot pain, and lateral column overload. Surgical release must be strictly limited to the medial one-third to one-half of the fascia.
OPERATIVE TECHNIQUES
Procedure 1: Partial Plantar Fasciotomy and Heel Spur Resection
Positioning and Anesthesia:
The patient is placed in the supine position. A thigh or calf tourniquet is applied. Regional anesthesia (popliteal block) combined with monitored anesthesia care (MAC) or general anesthesia is preferred.
Surgical Approach:
1. Make a 3- to 4-cm longitudinal or slightly oblique incision over the medial aspect of the heel, centered over the medial calcaneal tubercle.
2. Deepen the incision through the subcutaneous fat, taking meticulous care to identify and retract the medial calcaneal sensory nerve branches.
3. Identify the deep fascia of the abductor hallucis muscle.
Deep Dissection and Fasciotomy:
1. Retract the abductor hallucis muscle superiorly to expose the origin of the plantar fascia at the medial calcaneal tuberosity.
2. Isolate the medial band and the medial aspect of the central band of the plantar fascia.
3. Using a #15 blade, sharply release the medial one-third to one-half of the plantar fascia from its calcaneal origin.
4. Do not release the lateral band. Preservation of the lateral fascia is critical to maintaining the structural integrity of the longitudinal arch.
5. If a prominent, impinging calcaneal spur is present, it may be excised using a small osteotome or rongeur. However, routine spur resection is not mandatory if it does not mechanically impinge on the neurovascular structures, as the spur is within the FDB origin, not the fascia.
Procedure 2: Baxter's Nerve Release (Neurolysis)
If preoperative evaluation indicates neurogenic entrapment, a concurrent release of the first branch of the lateral plantar nerve is indicated.
Surgical Steps:
1. Utilizing the same medial approach, identify the superficial and deep fascia of the abductor hallucis.
2. Release the superficial fascia and retract the muscle belly.
3. Identify the deep fascial edge of the abductor hallucis. This is the primary site of entrapment for Baxter's nerve.
4. Carefully incise this deep fascia, decompressing the nerve as it dives between the abductor hallucis and the quadratus plantae.
5. Trace the nerve distally to ensure there are no secondary tethering points from the FDB or the calcaneal spur.
6. Achieve meticulous hemostasis to prevent postoperative hematoma, which could lead to recurrent perineural fibrosis.
Closure:
Irrigate the wound copiously with sterile saline. Close the subcutaneous tissues with 3-0 absorbable sutures and the skin with 4-0 non-absorbable horizontal mattress sutures. Apply a bulky, compressive soft dressing.
POSTOPERATIVE PROTOCOL
- Phase I (0-2 Weeks): The patient is placed in a well-padded short leg splint or controlled ankle motion (CAM) boot. Weight-bearing is restricted to touch-down or non-weight-bearing to allow for soft tissue healing and to prevent early catastrophic failure of the remaining fascial fibers.
- Phase II (2-6 Weeks): Sutures are removed at 14 days. The patient transitions to progressive partial weight-bearing in a CAM boot. Gentle, passive dorsiflexion stretching of the MTP joints and ankle is initiated to modulate the healing scar tissue.
- Phase III (6-12 Weeks): Transition to regular footwear utilizing a custom orthotic with a deep heel cup and medial arch support. Aggressive physical therapy focuses on intrinsic foot muscle strengthening, Achilles stretching, and proprioceptive training.
- Return to Activity: Full return to high-impact sports or heavy labor is typically delayed until 3 to 4 months postoperatively, contingent upon the resolution of pain and restoration of normal gait mechanics.
COMPLICATIONS AND PITFALLS
- Lateral Column Overload: The most devastating complication of an overzealous plantar fasciotomy is lateral column overload and subsequent cuboid syndrome or metatarsal stress fractures. This occurs due to the loss of the windlass mechanism and subsequent arch collapse.
- Recurrent Pain: Often due to inadequate release, missed neurogenic entrapment (Baxter's nerve), or failure to address concomitant Achilles contracture.
- Heel Pad Atrophy: Excessive surgical dissection can devascularize the specialized fat pad of the heel, leading to intractable, mechanically induced pain that is exceptionally difficult to salvage.
- Iatrogenic Nerve Injury: Damage to the medial calcaneal branches during the surgical approach can result in painful neuromas. Meticulous blunt dissection in the subcutaneous plane is mandatory.
📚 Medical References
- painful heel syndrome with shock waves, Clin Orthop Relat Res 387:41, 2001.
- Clement DB, Taunton JE, Smart GW: Achilles tendinitis and peritendinitis: etiology and treatment, Am J Sports Med 12:179, 1984.
- Confl itti JM, Tarquinio TA: Operative outcome of partial plantar fasciectomy and neurolysis to the nerve of the abductor digiti minimi muscle for recalcitrant plantar fasciitis, Foot Ankle Int 25:482, 2004.
- Conti S, Michelson J, Jahss M: Clinical signifi cance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures, Foot Ankle 13:208, 1992.
- Costa ML, Shepstone L, Donell ST, et al: Shock wave therapy for chronic Achilles tendon pain: a randomized placebo-controlled trial, Clin Orthop 440:199, 2005.
- Coull R, Flavin R, Stephens MM: Flexor hallucis longus tendon transfer: evaluation of postoperative morbidity, Foot Ankle Int 24:931, 2003.
- DiGiovanni BF, Nawoczenski DA, Lintal ME, et al: Tissuespecifi c plantar fascia–stretching exercise enhances outcomes in patients with chronic heel pain. A prospective, randomized study, J Bone Joint Surg 85A:1270, 2003.
- DuVries HL: Heel spur (calcaneal spur), Arch Surg 74:536, 1957.
- Fiamengo SA, Warren RF, Marshall JL, et al: Posterior heel pain associated with a calcaneal step and Achilles tendon calcifi cation, Clin Orthop 167:203, 1982.
- Frey C, Pfeffer GB: Calcaneal prominence resection. In Johnson KA, Thompson RC, eds: The foot and ankle: master techniques in orthopaedic surgery, New York, 1994, Raven. Frey C, Rosenberg Z, Shereff MJ, et al: The retrocalcaneal bursa: anatomy and bursography, Foot Ankle 13:203, 1992.
- Furey JG: Plantar fasciitis: the painful heel syndrome, J Bone Joint Surg 57A:672, 1975.
- Furia JP: High-energy extracorporeal shock wave therapy as a treatment for insertional Achilles tendinopathy, Am J Sports Med 34:733, 2006.
- Gibbon WW, Cooper JR, Radcliffe GS: Distribution of sonographically detected tendon abnormalities in patients with a clinical diagnosis of chronic Achilles tendinosis, J Clin Ultrasound 28:61, 2000.
- Gould JS: Extracorporeal shockwave therapy (ESWT) in patients with chronic proximal plantar fasciitis, Foot Ankle Int 23:309, 2002.
- Graham CE: Painful heel syndrome: rationale and treatment, Foot Ankle 3:261, 1983.
- Graves SG, Mann RA, Graves KO: Triple arthrodesis in older adults, J Bone Joint Surg 75A:355, 1993.
- Griffi th JD: Osteophytes of the os calcis, Am J Orthop Surg 8:501, 1910.
- Hammer DS, Adam F, Kreutz A, et al: Extracorporeal shock wave therapy (ESWT) in patients with chronic proximal plantar fasciitis: a 2-year follow-up, Foot Ankle Int 24:823, 2003.
- Hammer DS, Rupp S, Ensslin S, et al: Extracorporal shock wave therapy in patients with tennis elbow and painful heel, Arch Orthop Trauma Surg 120:304, 2000.
- Harper MC: Subluxation of the peroneal tendons within the peroneal groove: a report of two cases, Foot Ankle 18:369, 1997.
- Hassab HK, El-Sherif AS: Drilling of the os calcis for painful heel with calcaneal spur, Acta Orthop Scand 95:152, 1974.
- Hawkins BJ, Langermen RJ Jr, Gibbons T, et al: An anatomic analysis of endoscopic plantar fascia release, Foot Ankle 16:552, 1995.
- Heneghan M, Pavlov J: The Haglund painful heel syndrome, Clin Orthop 187:228, 1984.
- Hicks JH: The mechanics of the foot. II. The plantar aponeurosis and the arch, J Anat 88:25, 1954.
- Hofmeister EP, Elliott MJ, Juliano PJ: Endoscopic plantar fascia release: an anatomical study, Foot Ankle 16:719, 1995.
- Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy, Foot Ankle Int 27:952, 2006.
- Holmes GB Jr, Mann RA: Possible epidemiological factors associated with rupture of the posterior tibial tendon, Foot Ankle 13:70, 1992.
- Hughes S: Radionuclides in orthopaedic surgery, J Bone Joint Surg 62B:141, 1980.
- Hunte G, Lloyd-Smith R: Topical glyceryl trinitrate for chronic Achilles tendinopathy, Clin J Sport Med 15:116, 2005.
- Johnson KW, Zalavras C, Thordarson DB: Surgical management of insertional calcifi c Achilles tendinosis with a central tendon splitting approach, Foot Ankle Int 27:245, 2006.
- Johnston MR: Nerve entrapment causing heel pain, Clin Podiatr Med Surg 11:617, 1994.
- Jones DC: Posterior heel pain. In Pfeffer GB, Frey CC, eds: Current practice in foot and ankle surgery, vol 2, New York, 1994, McGraw-Hill. Jones DC, James SL: Partial calcaneal osteotomy for retrocalcaneal bursitis, Am J Sports Med 12:72, 1984.
- Kahn C, Bishop JO, Tullos HS: Plantar fascia release and heel spur excision via plantar route, Orthop Rev 14:69, 1985.
- Karr JP: A method to alleviate and cure the painful heel syndrome, J Am Podiatr Assoc 68:124, 1978.
- Katoh Y, Chao EYS, Morrey BF, et al: Objective technique for evaluating painful heel syndrome and its treatment, Foot Ankle 3:227, 1983.
- Keck SW, Kelly PJ: Bursitis of the posterior part of the heel, J Bone Joint Surg 47A:267, 1965.
- Keene JS: Tendon injuries of the foot and ankle. In DeLee JC, Drez D, eds: Orthopaedic sports medicine: principles and practice, Philadelphia, 1994, WB Saunders. Kenzora JE: The painful heel syndrome: an entrapment neuropathy, Bull Hosp Jt Dis 47:178, 1987.
- Kitaoka HB, Luo ZP, An KN: Mechanical behavior of the foot and ankle after plantar fascia release in the unstable foot, Foot Ankle 18:8, 1997.
- Knobloch K, Kraemer R, Lichtenberg A, et al: Achilles tendon and paratendon microcirculation in midportion and insertional tendinopathy in athletes, Am J Sports Med 34:92, 2006.
- Kolodziej P, Glisson RR, Nunley JA: Risk of avulsion of the Achilles tendon after partial excision for treatment of insertional tendinitis and Haglund’s deformity: a biomechanical study, Foot Ankle 20:433, 1999.
- Kuhns JG: Changes in elastic adipose tissue, J Bone Joint Surg 31A:541, 1949.
- Kvist H, Kvist M: The operative treatment of chronic calcaneal paratenonitis , J Bone Joint Surg 62B:353, 1980.
- Kvist MH, Lehto MUK, Jozsa L, et al: Chronic Achilles paratenonitis—an immunohistologic study of fi bronectin and fi brinogen, Am J Sports Med 16:616, 1988.
- Labib SA, Gould JS, Rodriguez-del-Rio FA, et al: Heel pain triad (HPT): the combination of plantar fasciitis, posterior tibial tendon dysfunction and
