INTRODUCTION TO DISTAL RADIUS MALUNION
Fractures of the distal radius are among the most frequently encountered injuries in orthopedic traumatology. Despite advances in operative fixation, malunion remains a prevalent complication, particularly following nonoperative management of displaced fractures. Malunions of the distal radius are broadly categorized into extra-articular and intra-articular deformities, with extra-articular malunions further subdivided based on the direction of sagittal angulation: dorsal angulation (Colles-type) and volar angulation (Smith-type).
The biomechanical consequences of a distal radius malunion are profound. Alterations in radial length, inclination, and sagittal tilt disrupt the delicate kinematics of the radiocarpal and distal radioulnar joints (DRUJ). The opening wedge metaphyseal osteotomy, pioneered and popularized by Fernandez, remains the gold standard for correcting these complex three-dimensional deformities. By utilizing precise preoperative templating, targeted osteotomies, structural bone grafting, and rigid internal fixation, orthopedic surgeons can reliably restore wrist biomechanics, alleviate pain, and improve functional outcomes.
BIOMECHANICS AND PATHOANATOMY
Understanding the biomechanical shifts caused by distal radius malunion is critical for preoperative planning and executing a successful osteotomy.
Dorsally Angulated (Colles-Type) Malunion
Normal distal radius anatomy dictates an average volar tilt of 11 degrees, radial inclination of 22 degrees, and radial height of 11 to 12 mm. When a fracture heals with excessive dorsal tilt and radial shortening, the following biomechanical derangements occur:
* Load Transfer Alteration: A dorsal tilt exceeding 20 degrees shifts the axial load transmission across the wrist. Normally, the radius absorbs 80% of the load and the ulna 20%. With significant dorsal angulation, ulnar load-bearing can increase to over 50%, leading to ulnocarpal impaction syndrome and degenerative tears of the triangular fibrocartilage complex (TFCC).
* Kinematic Block: Dorsal angulation shifts the carpus dorsally, creating an obligate mechanical block to wrist flexion.
* DRUJ Incongruity: Radial shortening alters the relationship between the sigmoid notch of the radius and the ulnar head, leading to DRUJ subluxation, restricted forearm rotation (particularly supination), and early arthrosis.
Volarly Angulated (Smith-Type) Malunion
Fractures that unite with excessive volar inclination are less common but present unique functional challenges.
* Deformity Profile: These malunions are characterized by increased volar inclination, decreased radioulnar inclination, radial shortening, and resultant ulnar deviation of the wrist.
* Rotational Malalignment: A hallmark of the Smith-type malunion is the characteristic pronation of the distal articular fragment.
* Functional Deficits: This complex deformity causes severe incongruence and instability of the DRUJ. Forearm rotation (especially supination) is markedly limited, and the distal ulna frequently impinges on the ulnar carpus. Decreased grip strength and restricted wrist extension are primary patient complaints.
💡 Clinical Pearl: The Rule of Thumb for Osteotomy
Surgical correction is generally indicated when functional deficits and pain correlate with radiographic parameters exceeding acceptable limits: dorsal tilt >10 degrees, volar tilt >20 degrees, radial shortening >3 mm, or an intra-articular step-off >2 mm. Treat the patient's functional deficit, not just the radiograph.
PREOPERATIVE PLANNING AND TEMPLATING
Meticulous preoperative planning is the cornerstone of a successful opening wedge osteotomy.
- Radiographic Evaluation: Obtain high-quality posteroanterior (PA) and lateral radiographs of both the affected and contralateral (normal) wrists. The contralateral wrist serves as the anatomical template.
- Advanced Imaging: A computed tomography (CT) scan with 3D reconstructions is highly recommended to assess intra-articular healing, the exact geometry of the sigmoid notch, and the presence of DRUJ arthrosis.
- Templating the Correction:
- Trace the normal contralateral radius and superimpose it over the malunited radius.
- Determine the exact site of the osteotomy (typically the apex of the deformity, usually 2.5 cm proximal to the radiocarpal joint).
- Calculate the angle of correction required in the sagittal plane (to restore volar tilt) and the coronal plane (to restore radial inclination).
- Measure the required opening wedge gap in millimeters to restore radial length.
SURGICAL TECHNIQUE: DORSAL OPENING WEDGE OSTEOTOMY (FERNANDEZ)
This technique is primarily indicated for the classic Colles-type dorsally angulated malunion.
1. Patient Positioning and Preparation
- Place the patient supine with the affected arm extended on a radiolucent hand table.
- Apply a well-padded proximal arm tourniquet.
- Administer regional anesthesia (supraclavicular or axillary block) or general anesthesia.
- Prepare the ipsilateral iliac crest for structural bone graft harvesting.
2. Surgical Approach
- Make a straight dorsal longitudinal incision over the distal radius, parallel to its long axis.
- Begin the incision approximately 2 cm distal to the Lister tubercle and extend it 8 cm proximally into the distal forearm.
- Incise the extensor retinaculum over the third extensor compartment. Mobilize the extensor pollicis longus (EPL) tendon and retract it radially with a vessel loop.
- Develop the interval between the second compartment (extensor carpi radialis brevis - ECRB) and the fourth compartment (extensor digitorum communis - EDC).
- Elevate the periosteum and the pronator quadratus insertion subperiosteally to expose the dorsal and radial aspects of the distal radius. Ensure adequate exposure to allow for the seating of a buttress plate.
3. Marking and K-Wire Placement
- Identify the planned osteotomy site, typically 2.5 cm proximal to the radiocarpal joint line. Mark this site with an osteotome or a sterile marking pen.
- Proximal Reference Wire: Insert a 1.5 mm Kirschner wire (K-wire) approximately 4 cm proximal to the osteotomy site. This wire must be placed strictly perpendicular to the long axis of the radial shaft in the sagittal plane.
- Distal Reference Wire: Insert a second K-wire into the distal metaphyseal fragment. The angle subtended by this distal wire and the proximal wire must exactly equal the angle of the deformity calculated during preoperative templating.
⚠️ Surgical Warning: Joint Parallelism
Before committing to the osteotomy, use fluoroscopy to confirm that the planned cut in the sagittal plane is perfectly parallel to the articular surface of the radiocarpal joint. An oblique cut will induce an unwanted coronal plane deformity when the wedge is opened.
4. Executing the Osteotomy and Deformity Correction
- Perform the osteotomy using an oscillating saw, frequently irrigating with cold saline to prevent thermal necrosis. Leave the volar periosteal hinge intact if possible, as it provides stability and aids in vascularization.
- Gently open the osteotomy dorsally using lamina spreaders or osteotomes until the two reference K-wires become perfectly parallel. This maneuver restores the normal volar tilt of 5 to 10 degrees to the distal radial articular surface.
- To restore radial length, open the osteotomy on the radial side until the gap corresponds exactly to the distance measured on the preoperative drawing.
- Once the desired three-dimensional correction (sagittal tilt, radial inclination, and length) is achieved, stabilize the fragments temporarily with an oblique K-wire driven from the radial styloid into the proximal shaft.
5. Bone Grafting
- Harvest a tricortical or bicortical structural bone graft from the ipsilateral iliac crest.
- Trim and contour the graft to precisely fit the trapezoidal dorsal-radial bone defect created by the opening wedge.
- Crucial Step: Before final impaction of the graft, assess the rotational alignment. Any pronation or supination malalignment of the distal fragment must be corrected by rotating it around the long axis of the radius.
- Insert the structural graft and tamp it firmly into place. Pack any remaining voids with cancellous autograft.
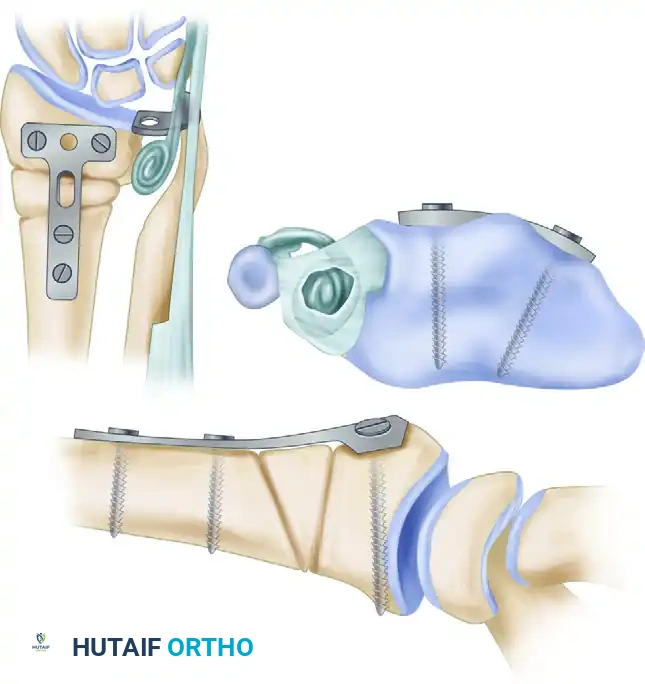
6. Internal Fixation
- Select a small T-plate (or a modern pre-contoured dorsal locking plate). Contour the plate to fit the newly restored anatomy of the dorsal radius perfectly.
- Apply the plate and secure it with a minimum of two screws in the distal fragment and two screws in the proximal fragment.
- Stability Check: The fixation must be rigid enough to allow for early postoperative mobilization. If the construct feels unstable, increase the number of screws, or place an additional oblique lag screw originating from the radial styloid, crossing the osteotomy and the bone graft, and anchoring into the opposite cortex of the proximal radial fragment.
MANAGEMENT OF THE DISTAL RADIOULNAR JOINT (DRUJ)
Restoring radial anatomy often improves DRUJ kinematics; however, chronic malunions frequently result in irreversible changes to the DRUJ that must be addressed concomitantly to ensure a successful functional outcome.
Ulnar Shortening Osteotomy
If the DRUJ is incongruent and exhibits ulnocarpal impaction, but the articular cartilage of the sigmoid notch and ulnar head remains preserved (no severe arthrosis), an ulnar shortening osteotomy is indicated. This procedure decompresses the ulnocarpal joint and tightens the ulnocarpal ligaments, stabilizing the DRUJ.
Bowers Arthroplasty (Hemiresection Interposition)
If advanced arthrosis of the DRUJ is present, joint-preserving procedures will fail to relieve pain. In these cases, a Bowers arthroplasty is highly effective.
- Technique: The procedure involves resecting the articular surface of the ulnar head while meticulously preserving the ulnar styloid and the attached triangular fibrocartilage complex (TFCC).
- Interposition: To prevent radioulnar impingement (convergence of the distal radius and ulna), a soft tissue "anchovy" is interposed into the empty joint space. This is typically fashioned from a distally based strip of the extensor carpi ulnaris (ECU) tendon, which is rolled upon itself and sutured into the defect.
SURGICAL TECHNIQUE: VOLAR OPENING WEDGE OSTEOTOMY (SMITH MALUNION)
For extra-articular malunions with volar angulation (Smith-type), the surgical principles mirror those of the dorsal osteotomy, but the approach and biomechanical corrections are reversed.
1. Surgical Approach
- Utilize a modified Henry approach to the volar aspect of the distal forearm.
- Make a longitudinal incision over the flexor carpi radialis (FCR) tendon.
- Retract the FCR tendon ulnarly and the radial artery radially.
- Incise the floor of the FCR sheath and elevate the pronator quadratus from its radial insertion, reflecting it ulnarly to expose the volar metaphysis of the radius.
2. Osteotomy and Correction
- The osteotomy is planned at the apex of the volar deformity.
- Similar to the dorsal technique, K-wires are used to gauge the correction. The osteotomy is opened volarly to correct the excessive volar tilt and restore neutral or slight volar angulation.
- Rotational Correction: Because Smith malunions are characterized by pronation of the distal fragment, it is imperative to supinate the distal fragment relative to the proximal shaft during the correction.
3. Grafting and Fixation
- A structural iliac crest bone graft is contoured to fit the volar opening wedge defect.
- Fixation is achieved using a volar locking plate. Modern volar locking plate technology provides exceptional biomechanical stability, often negating the need for prolonged postoperative immobilization.
- Concomitant ulnar-sided procedures (ulnar shortening or DRUJ arthroplasty) are evaluated and performed as dictated by the presence of ulnar impaction or DRUJ arthrosis.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a corrective osteotomy relies heavily on a structured, phased rehabilitation program.
Phase I: Immediate Postoperative (Weeks 0-2)
- Close the wound in anatomical layers. Ensure the extensor retinaculum is repaired over the EPL tendon to prevent bowstringing, or leave the EPL transposed subcutaneously.
- Apply a bulky compressive dressing and a sugar-tong splint to control forearm rotation and support the wrist.
- Encourage immediate active range of motion (ROM) of the fingers, thumb, elbow, and shoulder to prevent stiffness and reduce edema.
- Strict elevation is maintained to mitigate swelling.
Phase II: Early Mobilization (Weeks 2-6)
- At the 2-week mark, sutures are removed.
- If rigid internal fixation was achieved (and bone quality is adequate), the sugar-tong splint is transitioned to a removable custom thermoplastic wrist splint.
- Initiate supervised physical therapy focusing on active and active-assisted wrist flexion, extension, pronation, and supination.
- The splint is worn between exercise sessions and at night.
Phase III: Strengthening and Conditioning (Weeks 6-12)
- Obtain follow-up radiographs at 6 weeks to assess graft incorporation and osteotomy healing.
- Once clinical and radiographic signs of union are present, discontinue the splint.
- Begin progressive resistance exercises to restore grip strength and forearm endurance.
- Return to heavy manual labor or contact sports is typically restricted until 4 to 6 months postoperatively, pending complete radiographic consolidation of the bone graft.
OUTCOMES AND COMPLICATIONS
Clinical Outcomes
Corrective osteotomy for distal radius malunion yields highly predictable and satisfactory results when patient selection and surgical execution are optimal. Literature, including landmark studies by Shea et al., reports satisfactory outcomes in over 72% of patients at short-to-medium-term follow-up. Patients consistently demonstrate statistically significant improvements in radiographic parameters, wrist extension, forearm supination, and grip strength.
Potential Complications
Despite high success rates, surgeons must be vigilant regarding potential complications:
* Persistent DRUJ Pain: Noted in approximately 6% of patients, often due to unrecognized pre-existing arthrosis or failure to adequately address ulnar variance.
* Hardware Irritation: Dorsal plates are particularly prone to causing extensor tendon tenosynovitis or rupture. Modern low-profile plates have reduced this risk, but hardware removal may still be required in up to 15% of cases once the osteotomy has healed.
* Nonunion/Delayed Union: Rare with the use of autologous iliac crest bone graft and rigid fixation, but risk increases in patients who smoke or have compromised bone quality.
* Complex Regional Pain Syndrome (CRPS): A devastating complication that requires early recognition. Prophylactic Vitamin C (500 mg daily for 50 days postoperatively) and aggressive early finger mobilization are recommended to mitigate this risk.
