INTRODUCTION TO TALAR NECK FRACTURES
Fractures of the talar neck represent a formidable challenge in orthopedic trauma, demanding a profound understanding of osseous anatomy, biomechanics, and the tenuous extraosseous vascular supply. Typically resulting from high-energy trauma—such as motor vehicle collisions or falls from a height—these injuries are historically associated with hyperdorsiflexion and axial loading of the foot against the anterior distal tibia.
The primary goals of operative intervention are the anatomic restoration of the articular surfaces (subtalar and ankle joints), the prevention of varus malunion, and the preservation of the remaining vascular supply to mitigate the risk of osteonecrosis (avascular necrosis, AVN).
Clinical Pearl: The vascular supply to the talar body is retrograde, primarily derived from the artery of the tarsal canal (a branch of the posterior tibial artery), the artery of the sinus tarsi, and the deltoid branches. Surgical approaches must be meticulously planned to avoid disrupting the intact medial vascular sling, particularly the deltoid ligament branches.
PREOPERATIVE PLANNING AND IMAGING
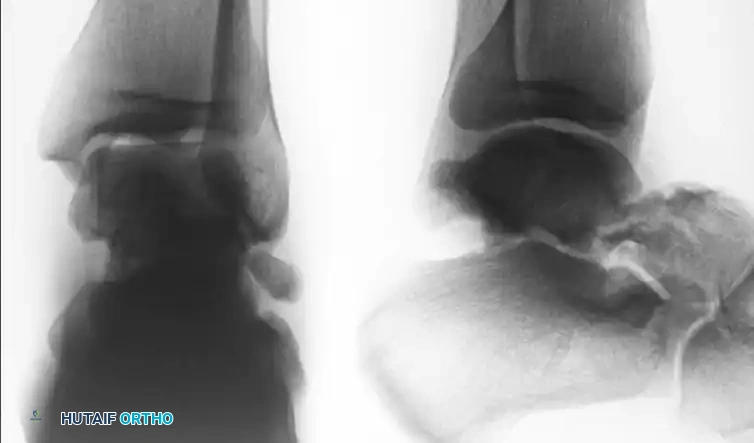
Standard radiographic evaluation includes anteroposterior (AP), lateral, and mortise views of the ankle, alongside standard foot radiographs. However, plain radiography often underestimates the degree of comminution and displacement.
The Canale View
To accurately assess varus or valgus alignment of the talar neck, the Canale view is mandatory. The foot is placed in maximum equinus and pronated 15 degrees, with the x-ray beam directed 75 degrees cephalad from the horizontal. This provides an optimal en face view of the talar neck.
Computed Tomography (CT)
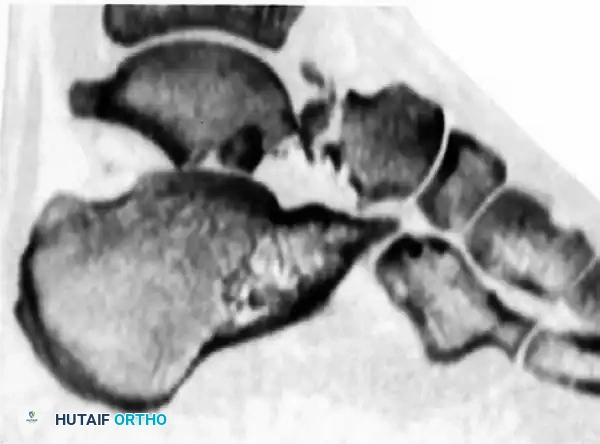
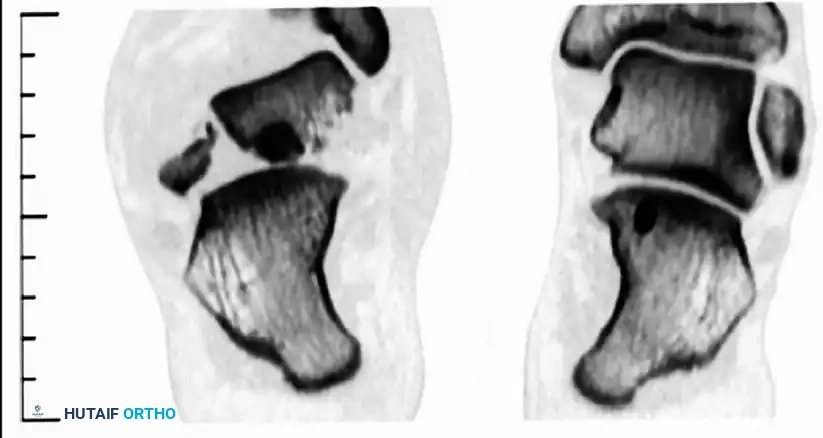
A fine-cut CT scan with sagittal and coronal reconstructions is the gold standard for preoperative planning. It delineates fracture lines, identifies intra-articular step-offs, and reveals concomitant injuries such as lateral process fractures or subtalar debris.
SURGICAL APPROACHES
Optimal exposure often requires a dual-incision technique (anteromedial and anterolateral) to visualize both cortices of the talar neck. This ensures anatomic reduction and prevents the notorious complication of varus malunion.
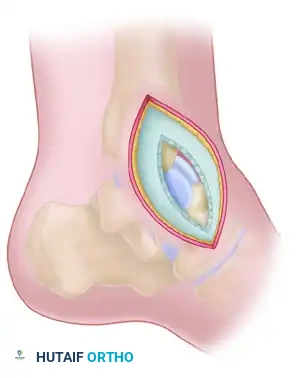
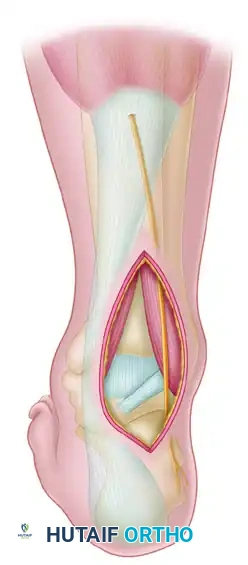
1. The Anteromedial Approach
The anteromedial approach is the workhorse for exposing the medial talar neck and head.
- Incision: Make a 7.5 to 10 cm longitudinal incision beginning proximal and just anterior to the medial malleolus.
- Trajectory: Curve the incision distalward and plantarward toward the sole of the foot, terminating on the medial side of the navicular body.
- Deep Dissection: Develop the interval between the anterior tibial tendon and the posterior tibial tendon.
- Preservation: Expose the fracture and the anteromedial aspect of the neck and body of the talus.
Surgical Warning: Strictly avoid incising the posterior tibial tendon and the neurovascular structures inferior to the medial malleolus. Preserve as much intact soft tissue as possible around the head and neck of the talus to protect the deltoid branches.


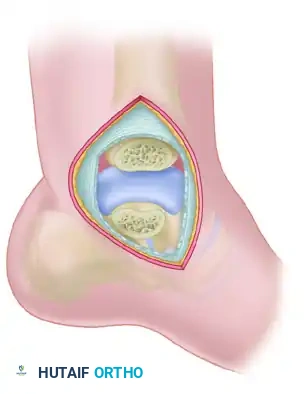
Medial Malleolar Osteotomy
If the body of the talus is extruded from the ankle mortise (Hawkins Type III or IV), or if posterior comminution prevents adequate visualization, a medial malleolar osteotomy may be required.
* Pre-drill the medial malleolus for subsequent screw fixation.
* Perform a chevron-type osteotomy directed toward the axilla of the medial clear space.
* Reflect the malleolus inferiorly on its intact deltoid hinge.


2. The Anterolateral Approach
An anterolateral approach is frequently necessary to assess the lateral cortex, which is prone to comminution, and to ensure no varus malreduction has occurred.
- Incision: Create a 5 cm incision centered over the sinus tarsi, extending toward the base of the fourth metatarsal.
- Nerve Protection: Meticulously identify and protect the dorsal intermediate cutaneous nerve (a branch of the superficial peroneal nerve) in the proximal extent of the wound.
- Deep Dissection: Incise the inferior extensor retinaculum. Reflect the extensor digitorum brevis (EDB) muscle belly plantarly to expose the lateral talar neck and the subtalar joint.

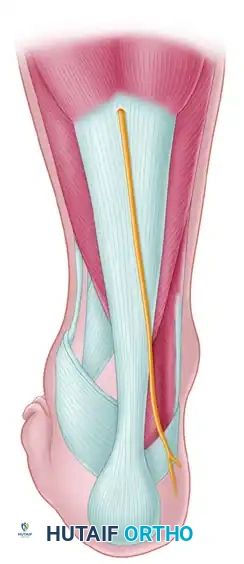
3. The Posterolateral Approach
For the placement of posterior-to-anterior (PA) screws—which are biomechanically superior due to the denser bone of the posterior talar body—a posterolateral approach is utilized.
- Positioning: The patient may need to be in a lateral or prone position, though a floppy lateral position can sometimes accommodate both anterior and posterior access.
- Incision: Utilize the Henry approach from the lateral side of the Achilles tendon.
- Interval: Develop the interval between the flexor hallucis longus (FHL) medially and the peroneal tendons laterally. Retracting the FHL medially protects the posteromedial neurovascular bundle.
REDUCTION AND INTERNAL FIXATION TECHNIQUE
Joint Preparation and Provisional Fixation
- Debridement: Thoroughly irrigate the joint to remove hematoma, osteochondral shear fragments, and interposed soft tissue debris.
- Reduction: Reduce the fracture anatomically. Try to locate interdigitating fracture lines medially or laterally to serve as a guide to reduction, even if a gap remains in the opposite cortex due to comminution.
- Provisional Stabilization: Drive two or three small Kirschner wires (K-wires) through the articular surface of the talar head, across the neck, and into the body to hold the reduction.
Pitfall: Slight varus at the fracture site is a common error that produces a devastating malunion. Varus malalignment decreases subtalar eversion, locking the transverse tarsal joint and leading to a rigid, painful foot. Always confirm reduction visually on both sides and radiographically via the Canale view.


Definitive Fixation Strategies
Anterior-to-Posterior (AP) Screw Fixation:
* Depending on the available space for fixation, utilize 4.0-mm, 4.5-mm, or 6.5-mm partially threaded cannulated screws.
* Begin just posterior to the articular surface of the head on the medial or lateral aspect of the neck.
* Crucial Step: Care must be taken to countersink the screw head. This provides a flat area for seating and prevents impingement on the navicular articular surface.
Posterior-to-Anterior (PA) Screw Fixation:
* Place the guidewire above the lateral projection of the posterior process.
* Direct the wire anteriorly toward the lateral talar head.
* Fluoroscopic guidance is essential to avoid penetrating the subtalar joint.
Plate Fixation:
* Alternatively, minifragment plates (2.0 mm or 2.4 mm) and screws can be placed, especially if there is excessive comminution of the lateral neck or limited space for fixation in the head fragment. Plates act as a buttress against varus collapse.


Management of the Fragile or Elderly Bone
If the cortex is fragile (osteoporosis) or if the fracture is highly distal, firm fixation may not be secured by placing a screw obliquely.
* In such patients, drill two Steinmann pins (3/32-inch or larger).
* Pass them proximally from the navicular, into the head of the talus, through the fracture site, and deep into the body of the talus.
* Transfixing the talonavicular joint in this manner is preferable to attempting to countersink screws below the surface of the articular cartilage in osteoporotic bone, which often leads to screw head pull-through.
Final Verification
- Check the final position with intraoperative fluoroscopy.
- Obtain a Canale view to definitively rule out varus malreduction.
- If the medial malleolus was osteotomized, reduce it anatomically and fix it with two parallel partially threaded cancellous screws.


POSTOPERATIVE CARE PROTOCOL
Rigid adherence to postoperative rehabilitation protocols is vital to prevent displacement and monitor for osteonecrosis.
- Immediate Post-op: The foot is held in a neutral position in a well-padded short-leg splint. Once swelling subsides, transition to a cast from below the knee to the toes, well molded into the arch of the foot.
- Weight-Bearing Status: Strict non-weight-bearing (NWB) is enforced for 6 to 8 weeks.
- Transition: After 6 to 8 weeks, depending on radiographic signs of early union, a walking boot is applied, and progressive weight-bearing is permitted.
- Long-Term: Three months after surgery, if union has progressed satisfactorily, the cast or boot is removed. An orthopaedic shoe with a scaphoid pad is fitted and worn for an additional 3 months to support the longitudinal arch.
COMPLICATIONS AND SALVAGE PROCEDURES
Osteonecrosis (Avascular Necrosis) of the Talar Body
Osteonecrosis is the most feared complication following talar neck fractures. It is highly predictable based on the initial displacement: a very small percentage of nondisplaced fractures (Hawkins I) develop AVN, whereas a very large percentage of fractures with complete dislocation of the body (Hawkins III and IV) will be complicated by osteonecrosis.
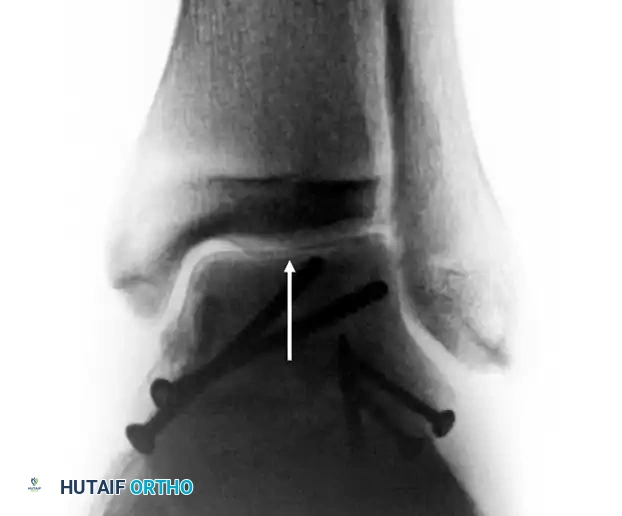
The Hawkins Sign
Between 6 and 8 weeks post-injury, an AP radiograph of the ankle should be scrutinized for the Hawkins sign.
* Positive Hawkins Sign: A thin line of subchondral radiolucency (atrophy) along the dome of the talus. This indicates that the bone is vascularized enough to undergo disuse osteopenia. It is a highly sensitive indicator that AVN will not occur.
* Negative Hawkins Sign: If the bone remains dense and sclerotic relative to the surrounding osteopenic bone, osteonecrosis is likely present.
Management of Osteonecrosis
Prolonged non-weight-bearing in hopes of preventing the collapse of the necrotic talar dome has not been sufficiently predictable to justify its routine use; in many cases, the talus collapses regardless of weight-bearing status.
When painful collapse occurs, excision alone of the necrotic body is contraindicated as it leads to severe mechanical instability. Salvage options include:
* Arthrodesis: Subtalar, ankle, or tibiotalocalcaneal (TTC) fusion, depending on the extent of joint involvement.
* Blair Fusion: A sliding bone graft from the anterior aspect of the tibia is slotted into the viable neck of the talus, combined with the excision of the necrotic talar body.
* Posterior Onlay Graft (Johnson Technique): In addition to usual approaches, arthrodesis can be achieved using an onlay graft technique through a posterior approach. This allows the placement of a massive volume of bone graft, yielding a satisfactory fusion rate while maintaining limb length and malleolar contours.
Malunion and Nonunion of the Talar Neck
Malunion (typically varus and dorsal extension) or nonunion is a relatively rare but profoundly disabling complication.
To avoid primary arthrodesis in a young patient with a malunion, a corrective osteotomy and/or revision of the nonunion can be performed—provided there is no (or only partial) osteonecrosis of the talus.
* Technique: The procedure involves re-creating the original fracture line, aggressive debridement of the nonunion site, realignment of the anatomic axes, structural bone grafting to fill the medial void, and stable internal fixation.
* Exposure: A medial malleolar osteotomy is almost always needed to obtain adequate exposure and to avoid iatrogenic damage to the remaining medial blood supply.
* Outcomes: Literature demonstrates that solid union can be achieved with high patient satisfaction rates, provided the vascularity of the body remains intact. Strict adherence to biomechanical principles during the revision ORIF is paramount.
📚 Medical References
- talar neck fractures, Clin Orthop Relat Res 199:81, 1985.
- Dabezies EJ, Shackleton R: Orthopaedic grand rounds: subtalar dislocation, Orthopaedics 5:348, 1982.
- DeLee JC, Curtis R: Subtalar dislocation of the foot, J Bone Joint Surg 64A:433, 1982.
- Dhillon MS, Nagi ON: Total dislocations of the navicular: are they ever isolated injuries? J Bone Joint Surg 81B:881, 1999.
- Dimon JH: Isolated displaced fracture of the posterior facet of the talus, J Bone Joint Surg 43A:275, 1961.
- Ebraheim NA, Padanilam TG, Wong FY: Posteromedial process fractures of the talus, Foot Ankle 16:734, 1995.
- Ebraheim NA, Sabry FF, Nadim Y: Internal architecture of the talus: implication for talar fracture, Foot Ankle Int 20:794, 1999.
- Ebraheim NA, Skie MC, Podeszwa DA, et al: Evaluation of process fractures of the talus using computed tomography, J Orthop Trauma 8:332, 1994.
- Elgafy H, Ebraheim NA, Tile M, et al: Fractures of the talus: experience of two level 1 trauma centers, Foot Ankle Int 21:1023, 2000.
- Fitch KD, Blackwell JB, Gilmour WN: Operation for non-union of stress fracture of the tarsal navicular, J Bone Joint Surg 71B:105, 1989.
- Fortin PT, Balazsy JE: Talus fractures: evaluation and treatment, J Am Acad Orthop Surg 9:114, 2001.
- Frawley PA, Hart JA, Young DA: Treatment outcome of major fractures of the talus, Foot Ankle 16:339, 1995.
- Gelberman RH, Mortensen WW: Arterial anatomy of the talus, Foot Ankle 4:64, 1983.
- Gissane W: A dangerous type of fracture of the foot, J Bone Joint Surg 33B:535, 1951.
- Giuffrida AY, Lin SS, Abidi N, et al: Pseudo os trigonum sign: missed posteromedial talar facet fracture, Foot Ankle Int 25:372, 2004.
- Goldner JL, Poletti SC, Gates HS, Richardson WJ: Severe open subtalar dislocations, J Bone Joint Surg 77A:1075, 1995.
- Gregory P, DiPasquale T, Herscovici D, et al: Ipsilateral fractures of the talus and calcaneus, Foot Ankle 17:701, 1996.
- Grob D, Simpson LA, Weber BG, et al: Operative treatment of displaced talus fractures, Clin Orthop Relat Res 199:88, 1985.
- Haliburton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus, J Bone Joint Surg 40A:1115, 1958.
- Hawkins LG: Fracture of the lateral process of the talus: a review of thirteen cases, J Bone Joint Surg 47A:1170, 1965.
- Hawkins LG: Fractures of the neck of the talus, J Bone Joint Surg 52A:991, 1970.
- Heck BE, Ebraheim NA, Jackson WT: Anatomical considerations of irreducible medial subtalar dislocation, Foot Ankle Int 17:103, 1996.
- Heckman JD, McLean MR: Fractures of the lateral process of the talus, Clin Orthop Relat Res 199:108, 1985.
- Higgins TF, Baumgaertner MR: Diagnosis and treatment of fractures of the talus: a comprehensive review of the literature, Foot Ankle Int 20:595, 1999.
- Inokuchi S, Ogawa K, Usami N: Classifi cation of fractures of the talus: clear differentiation between neck and body fractures, Foot Ankle Int 17:748, 1996.
- Inokuchi S, Ogawa K, Usami N, et al: Long-term follow-up of talus fractures, Orthopedics 19:477, 1996.
- Johnson KA, ed: Surgery of the foot and ankle, New York, 1989, Raven. Johnstone AJ, Maffulli N: Primary fusion of the talonavicular joint after fracture dislocation of the navicular bone, J Trauma 45:1100, 1998.
- Karasick D, Schweitzer M: The os trigonum syndrome: imaging features, Am J Radiol 166:125, 1996.
- Khan KM, Fuller PJ, Brukner PD, et al: Outcome of conservative and surgical management of navicular stress fracture in athletes: eighty-six cases proven with computerized tomography, Am J Sports Med 20:657, 1992.
- Kim DH, Berkowitz MJ, Pressman DN: Avulsion fractures of the medial tubercle of the posterior process of the talus, Foot Ankle Int 24:172, 2003.
- Kim DH, Hrutkay JM, Samson MM: Fracture of the medial tubercle of the posterior process of the talus: a case report and literature review, Foot Ankle Int 17:186, 1996.
- Kirkpatrick DP, Hunter RE, Janes PC, et al: The snowboarder’s foot and ankle. Paper presented at the Twenty-seventh Annual Meeting of the American Orthopaedic Foot and Ankle Society, San Francisco, Feb 1997.
- Lemaire RG, Bustin W: Screw fi xation of fractures of the neck of the talus using a posterior approach, J Trauma 20:669, 1980.
- Lin PP, Roe S, Kay M, et al: Placement of screws in the sustentaculum tali, Clin Orthop Relat Res 352:194, 1998.
- Lindvall E, Haidukewych G, DiPasquale T, et al: Open reduction and stable fi xation of isolated, displaced talar neck and body fractures, J Bone Joint Surg 86A:2229, 2004.
- McCrory P, Bladin C: Fractures of the lateral process of the talus: a clinical review: “snowboarder’s ankle,” Clin J Sports Med 6:124, 1996.
- McKeever FM: Fracture of the neck of the astragalus, Arch Surg 46:720, 1943.
- Miller WE: Operative intervention for fracture of the talus. In Bateman JE, Trott AW, eds: Foot and ankle, New York, 1980, Marcel Dekker. Morris HD, Hand WL, Dunn AS: The modifi ed Blair fusion for fractures of the talus, J Bone Joint Surg 53A:1289, 1971.
- Mulfi nger GL, Trueta J: The blood supply of the talus, J Bone Joint Surg 52B:160, 1970.
- Nadim Y, Tosic A, Ebraheim N: Open reduction and internal fi xation of fracture of the posterior process of the talus: a case report and review of the literature, Foot Ankle Int 20:50, 1999.
- Patel R, Van Bergeyk A, Pinney S: Are displaced talar neck fractures surgical emergencies? A survey of orthopaedic trauma experts, Foot Ankle Int 26:378, 2005.
- Quirk R: Stress fractures of the navicular, Foot Ankle Int 19:494, 1998.
- Ries M, Healy WA Jr: Total dislocation of the talus: case report with a 13-year follow-up and review of the literature, Orthop Rev 17:76, 1988.
- Ritsema GH: Total talar dislocation, J Trauma 28:692, 1988.
- Rockett MS, Brage ME: Navicular body fractures: computerized tomography fi ndings and mechanism of injury, J Foot Ankle Surg 36:185, 1997.
- Sanders DW, Busam M, Hattwick E, et al: Functional outcomes following displaced talar neck fractures, J Orthop Trauma 18:265, 2004.
- Sanders R: Displaced intra-articular fractures of the calcaneus, J Bone Joint Surg 83A:1438, 2001.
- Sangeorzan BJ, Benirschke SK, Mosca V, et al: Displaced intraarticular fractures of the tarsal navicular, J Bone Joint Surg 71A:1504, 1989.
- Sneppen O, Christensen SB, Krogsoe O, et al: Fracture of the body of the talus, Acta Orthop Scand 48:317, 1977.
- Swanson TV, Bray TJ, Holmes GB: Fractures of the talar neck, J Bone Joint Surg 74A:544, 1992.
- Szyszkowitz R, Reschauer R, Seggl W: Eighty-fi ve talus fractures treated by ORIF with fi ve to eight years of follow-up study of 69 patients, Clin Orthop Relat Res 199:97, 1985.
- Thordarson DB, Triffon MJ, Terk MR: Magnetic resonance imaging to detect avascular necrosis after open reduction and internal fi xation of talar neck fractures, Foot Ankle Int 17:742, 1996.
- Torg JS, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: a retrospective review of twenty-one cases, J Bone Joint Surg 64:700, 1982.
- Trillat A, Bousquet G, Lapeyre B: Displaced fractures of the neck or of the body of the talus: value of screwing by posterior surgical approach, Rev Chir Reparatrice Appar Mot 56:529, 1970.
- Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: two case reports and a comprehensive literature review, Foot Ankle Int 19:641, 1998.
- Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: results and outcomes, J Bone Joint Surg 86A:1616, 2004.
- Vallier HA, Nork SE, Benirschke SK, et al: Surgical treatment of
