INTRODUCTION TO POSTERIOR SHOULDER DISLOCATIONS
Posterior shoulder dislocations are relatively rare, accounting for approximately 2% to 5% of all glenohumeral dislocations. They are notoriously missed on initial clinical presentation, often requiring a high index of suspicion and orthogonal imaging (specifically an axillary lateral or Velpeau view) for accurate diagnosis. The classic etiology involves high-energy trauma, epileptic seizures, or electrical shock, where the powerful internal rotators (latissimus dorsi, pectoralis major, and teres major) overpower the weaker external rotators (infraspinatus and teres minor), driving the humeral head posteriorly.
A critical pathological feature of a locked posterior dislocation is the impaction fracture on the anteromedial aspect of the humeral head, commonly referred to as a "reverse Hill-Sachs lesion." When this defect engages the posterior rim of the glenoid, the shoulder becomes locked in internal rotation.
Surgical decision-making is dictated by the size of the articular defect, the chronicity of the dislocation, and the patient's functional demands. Defects are generally classified as:
* Small (<20% of the articular surface): Often manageable with closed reduction if acute, or arthroscopic/open soft tissue stabilization.
* Medium (20% to 40% of the articular surface): Require structural filling or rotational realignment to prevent engagement. Options include the McLaughlin procedure, the Neer modification, or the Keppler rotational osteotomy.
* Large (>40% of the articular surface): Typically require prosthetic replacement (hemiarthroplasty or total shoulder arthroplasty) due to the high risk of avascular necrosis and the inability to restore a congruent, stable joint.
PREOPERATIVE PLANNING AND IMAGING
Thorough preoperative evaluation is mandatory. Standard anteroposterior (AP) radiographs may only show the subtle "lightbulb sign" (due to fixed internal rotation) or a widened glenohumeral joint space (the "rim sign").
Clinical Pearl: Never accept a shoulder trauma series without an axillary lateral or modified axillary view. The axillary view definitively demonstrates the posterior displacement of the humeral head relative to the glenoid.
A computed tomography (CT) scan, preferably with 3D reconstructions, is the gold standard for preoperative planning. It allows the surgeon to accurately quantify the percentage of articular surface involvement in the reverse Hill-Sachs lesion, assess the integrity of the posterior glenoid rim, and evaluate for any concurrent fractures of the surgical neck or tuberosities.
OPEN REDUCTION VIA THE ANTEROMEDIAL APPROACH (MCLAUGHLIN PROCEDURE)
The McLaughlin procedure was originally designed to address the anteromedial humeral head defect by transferring the subscapularis tendon into the defect, thereby converting an intra-articular defect into an extra-articular one and preventing engagement on the posterior glenoid rim.
Patient Positioning and Anesthesia
- Administer general anesthesia, often supplemented with an interscalene regional block for postoperative pain control.
- Place the patient in the beach-chair position with the head secured and the operative arm draped free to allow full manipulation.
- Ensure a pneumatic arm positioner or a sterile Mayo stand is available to support the arm.
Surgical Technique (McLaughlin)
- Surgical Approach: Expose the shoulder through a standard anteromedial or deltopectoral approach. Identify the cephalic vein and retract it laterally with the deltoid or medially with the pectoralis major, depending on surgeon preference and venous anatomy.
- Deep Dissection: Incise the clavipectoral fascia to expose the conjoined tendon. Retract the conjoined tendon medially to visualize the subscapularis muscle and tendon.
- Subscapularis Tenotomy: Identify the superior and inferior borders of the subscapularis. Divide the subscapularis tendon transversely as close to its insertion on the lesser tuberosity as possible. Tag the tendon with heavy non-absorbable sutures and retract it medially.
- Joint Reduction: Attempt to reduce the shoulder manually using gentle lateral traction and external rotation.
- If manual reduction fails (which is common in locked dislocations): Insert a blunt periosteal elevator, Cobb elevator, or a specialized bone skid between the humeral head and the posterior rim of the glenoid cavity.
- Gently lever the articular surfaces apart. As soon as the posterior glenoid rim is disengaged from the anteromedial defect in the humeral head, reduction usually occurs with a palpable clunk.
- Joint Inspection: Thoroughly inspect the glenohumeral joint. Evaluate the posterior labrum, the posterior glenoid rim, and the extent of the anteromedial humeral head defect.
- Defect Preparation: Use a curet or a high-speed burr to debride the reverse Hill-Sachs defect down to bleeding cancellous bone. Remove all necrotic debris and fibrous tissue, beginning on the lesser tuberosity and extending into the defect.
- Tendon Transfer: Drill two holes transversely through the bone adjacent to the defect. Pass a heavy non-absorbable mattress suture through these osseous tunnels and through the previously tagged subscapularis tendon.
- Fixation: Pull the subscapularis tendon deep into the prepared defect in the humeral head and tie the sutures securely. This effectively fills the defect and limits internal rotation, preventing the humeral head from re-engaging the posterior glenoid.
Surgical Warning: When using a bone skid to lever the humeral head, apply force judiciously. Excessive leverage against an osteopenic humeral head or a locked surgical neck can easily cause an iatrogenic fracture of the proximal humerus.
The Neer Modification (Lesser Tuberosity Transfer)
While the classic McLaughlin procedure relies on tendon-to-bone healing, Neer introduced a biomechanically superior modification utilizing bone-to-bone healing.
- Instead of a simple tenotomy, perform an osteotomy of the lesser tuberosity, leaving the subscapularis tendon attached to the bone fragment.
- After reducing the joint and preparing the defect, mobilize the lesser tuberosity fragment and impact it into the reverse Hill-Sachs defect.
- Fix the bone fragment rigidly using one or two partially threaded cancellous bone screws (typically 4.0 mm or 4.5 mm) with washers.
- This modification provides robust immediate fixation and superior long-term healing compared to soft tissue transfer alone.
Posterior Grafting for Severe Instability
McLaughlin noted that in cases where the posterior glenoid rim is severely deficient, anchoring the subscapularis anteriorly may not provide sufficient stability. In such rare instances, a posterior approach is utilized to apply a bone graft along the posterior rim of the glenoid cavity and the neck of the scapula.
* The graft is typically harvested from the posterior iliac crest or the posterior acromion.
* It is fixed beneath the periosteum of the posterior scapular neck using cortical screws or threaded pins to create a structural buttress against posterior subluxation.
Postoperative Care (McLaughlin & Neer Modification)
- Immobilization: The arm is immobilized in a Velpeau dressing or a commercially available shoulder immobilizer in neutral to slight external rotation.
- Initial Phase (0-2 Weeks): The dressing is worn continuously until the wound has healed. Sutures are removed at 2 weeks. Gentle, active hand/wrist/elbow exercises and passive pendulum exercises for the shoulder are initiated.
- Intermediate Phase (2-6 Weeks): A shoulder immobilizer is worn strictly at night for 6 weeks. Daytime exercises are gradually increased.
- Late Phase (4-6+ Weeks): Internal rotation and overhead stretching exercises are introduced between 4 to 6 weeks, progressing to strengthening as tolerated.
DELTOPECTORAL APPROACH AND ROTATIONAL OSTEOTOMY (KEPPLER ET AL.)
For defects involving 20% to 40% of the articular surface where soft tissue transfers may fail, or in cases of chronic locked dislocations, a rotational osteotomy of the proximal humerus (as described by Keppler et al.) is a powerful joint-preserving technique. The principle is to alter the version of the proximal humerus so that the anteromedial defect remains anterior to the glenoid rim throughout the functional range of motion.
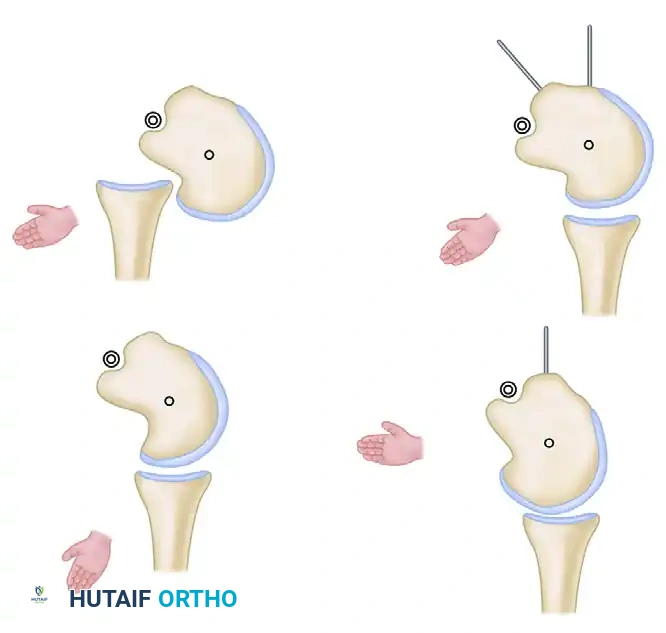
FIGURE 61-22: Diagrammatic representation of the principle of rotational osteotomy in a shoulder with a locked posterior dislocation. By rotating the humeral shaft internally relative to the head, the articular defect is rotated anteriorly, preventing engagement with the posterior glenoid rim.
Surgical Technique (Keppler Rotational Osteotomy)
- Positioning: Place the patient in the supine or modified beach-chair position.
- Incision: Make a standard 10-cm incision along the deltopectoral groove.
- Exposure: Expose the shoulder joint through an anterior deltopectoral approach. Perform minimal detachment of the anterior deltoid muscle from the clavicle only if necessary for superior exposure.
- Capsulotomy: Make an L-shaped incision through the subscapularis tendon and the underlying anterior joint capsule to expose the locked humeral head.
- Reduction and Debridement: Reduction of a chronic dislocation is often exceedingly difficult. Unhook the humeral head from the posterior glenoid rim using a bone skid. Meticulously remove any fibrous tissue, granulation tissue, or loose bodies filling the glenoid fossa, as this debris will mechanically block concentric reduction.
- Assessment of Stability: After reduction, dynamically assess the congruity of the joint and the range of motion. The shoulder will typically re-dislocate posteriorly when the arm is brought into internal rotation, as the anteromedial defect rolls back and engages the posterior glenoid rim.
- Decision Point: If the degree of internal rotation required to maintain stability is insufficient to allow normal activities of daily living (e.g., reaching the abdomen or perineum), a rotational osteotomy is indicated.
- Osteotomy Execution: Perform a transverse osteotomy through the surgical neck of the humerus.
- Rotational Realignment: Rotate the distal humeral shaft internally relative to the proximal humeral head fragment. The degree of rotation is dictated by the size of the defect, usually ranging from 20 to 30 degrees.
- Fixation: Fix the osteotomy rigidly with an angled blade plate or a modern proximal humeral locking plate. The stabilized osteotomy ensures that the humeral head defect remains anterior to the glenoid rim during normal physiological motion.
- Closure: Repair the subscapularis and capsule. Close the deltopectoral interval, subcutaneous tissue, and skin in layers over a suction drain.
Clinical Pearl: After rigid fixation of the osteotomy, the shoulder should demonstrate normal, stable motion in all planes, with the exception of a deliberate, calculated loss of terminal external rotation.
Postoperative Care (Rotational Osteotomy)
- Immediate Postoperative Phase: The arm is held in a shoulder immobilizer. The suction drain is typically removed on the second postoperative day.
- Weeks 0-1: Physical therapy is initiated with isometric exercises for the deltoid and rotator cuff, alongside gentle passive pendulum exercises. The immobilizer is worn continuously, especially at night.
- Weeks 1-3: Guided passive exercises are begun 1 week after surgery. Motion is strictly limited to a maximum of 90 degrees of forward flexion and abduction. External rotation is permitted only to the neutral position (0 degrees) to protect the subscapularis repair and the osteotomy. The immobilizer is gradually discontinued during the day based on patient comfort.
- Weeks 3-6: An active physical therapy program in all planes is initiated. However, active or passive external rotation beyond neutral is strictly prohibited until the sixth postoperative week.
- Weeks 6-8+: If clinical and radiographic evidence of osteotomy healing is present, and good range of motion and strength have returned, advanced activities such as swimming and throwing mechanics can be gradually introduced. The angled blade plate or locking plate is highly symptomatic in some patients but is not routinely removed unless hardware irritation occurs after complete bony union.
ARTHROPLASTY CONSIDERATIONS FOR MASSIVE DEFECTS
If the anteromedial humeral head defect is massive (greater than 40% to 50% of the articular surface), or if the dislocation is highly chronic (typically >6 months) with secondary severe degenerative joint disease or avascular necrosis, joint-preserving procedures like rotational osteotomy or soft tissue transfers are unlikely to restore articular congruity and stability. In these scenarios, prosthetic replacement is the treatment of choice.
Hemiarthroplasty vs. Total Shoulder Arthroplasty (TSA)
- Hemiarthroplasty: May be considered in younger patients with an intact, pristine glenoid cartilage. However, chronic posterior dislocations often result in severe posterior glenoid wear.
- Total Shoulder Arthroplasty (TSA): Preferred in older patients or those with significant glenoid erosion.
Surgical Nuances in Arthroplasty for Posterior Dislocation
- Version Control: The primary challenge in arthroplasty for chronic posterior dislocation is managing glenoid and humeral version. The humeral head is often retroverted, and the posterior glenoid is frequently eroded (B2 or B3 glenoid morphology).
- Trialing: Humeral version must be meticulously determined by inserting trial components and dynamically testing the stability of the shoulder at the time of surgery. Adjustments to the version (often requiring less retroversion than standard cases) are made based on these intraoperative stability tests.
- Glenoid Management: Posterior glenoid wear may require eccentric anterior reaming to restore neutral version, or in severe cases, posterior bone grafting.
- Capsular Management: Chronic posterior dislocation stretches the posterior capsule, creating a redundant posterior pouch. If necessary, the posterior part of the capsule can be plicated through the anterior approach. This is technically easier to perform after the humeral head has been osteotomized but before the final prosthetic components are inserted. Plication eliminates the redundant volume and provides a static checkrein against posterior subluxation of the new prosthesis.
By adhering to strict biomechanical principles—whether through defect-filling transfers, rotational realignment, or prosthetic replacement—the orthopedic surgeon can successfully navigate the complex pathology of the locked posterior shoulder dislocation and restore functional stability to the glenohumeral joint.
