INTRODUCTION TO CHRONIC UNREDUCED ELBOW DISLOCATIONS
An old, unreduced elbow dislocation is a profoundly debilitating condition that presents a formidable reconstructive challenge to the orthopedic surgeon. Defined generally as a dislocation that has remained unreduced for longer than three weeks, the pathology is characterized by severe soft tissue contractures, myostatic shortening of the triceps, and extensive fibro-osseous proliferation.
At the time of the initial injury, the violent displacement of the radius and ulna strips the periosteum from the distal humerus. In the neglected state, this elevated periosteum generates a massive hematoma that subsequently ossifies, filling the olecranon and coronoid fossae with dense callus and scar tissue. The collateral ligaments heal in a contracted, non-anatomic position, and the articular cartilage, deprived of normal synovial fluid nutrition and subjected to abnormal mechanical pressures, begins to degenerate.
Successful management requires a meticulous, stepwise surgical approach. The primary goals are to restore ulnohumeral and radiocapitellar congruity, reconstruct the stabilizing ligaments, and regain a functional arc of motion. For cases with severe chronicity or articular destruction, salvage procedures such as interpositional arthroplasty or total elbow arthroplasty (TEA) must be considered.
PREOPERATIVE EVALUATION AND PATHOANATOMY
Clinical Assessment
Patients typically present with a rigidly fixed elbow, profound loss of motion, and significant functional impairment of the upper extremity. The carrying angle is often distorted, and the prominent olecranon is palpable posteriorly. A thorough neurological examination is mandatory, with particular attention to the ulnar nerve, which is frequently tethered, stretched, or encased in scar tissue behind the medial epicondyle.
Radiographic and Advanced Imaging
Standard anteroposterior (AP) and lateral radiographs will confirm the direction of the dislocation (most commonly posterolateral) and reveal the extent of periarticular ossification.
Clinical Pearl: A non-contrast Computed Tomography (CT) scan with 3D reconstructions is essential in chronic cases. It precisely delineates the volume of heterotopic ossification within the olecranon fossa, identifies occult osteochondral defects of the capitellum or radial head, and aids in preoperative templating for potential arthroplasty.
SURGICAL TECHNIQUE: OPEN REDUCTION AND V-Y LENGTHENING OF THE TRICEPS (SPEED TECHNIQUE)
The Speed technique remains the gold standard for addressing the severe triceps contracture and joint obliteration seen in chronic unreduced dislocations. The procedure demands extensile exposure and meticulous handling of the articular surfaces.
1. Patient Positioning and Anesthesia
The procedure is performed under general anesthesia, often supplemented with a regional block for postoperative pain control. The patient is positioned in the lateral decubitus position with the operative arm draped over a padded post, allowing for full, unobstructed flexion and extension of the elbow. A sterile tourniquet is applied high on the arm.
2. Incision and Ulnar Nerve Isolation
A posterior midline incision is utilized, curving slightly lateral to the tip of the olecranon to avoid placing the scar directly over the bony prominence. Full-thickness fasciocutaneous flaps are elevated.
The first critical deep step is the identification and neurolysis of the ulnar nerve. Due to the altered anatomy and dense scar tissue, the nerve must be identified proximally in the normal tissue of the posterior compartment and traced distally into the cubital tunnel. The nerve is completely mobilized and protected with a vessel loop. Depending on the tension following reduction, an anterior subcutaneous transposition may be required.
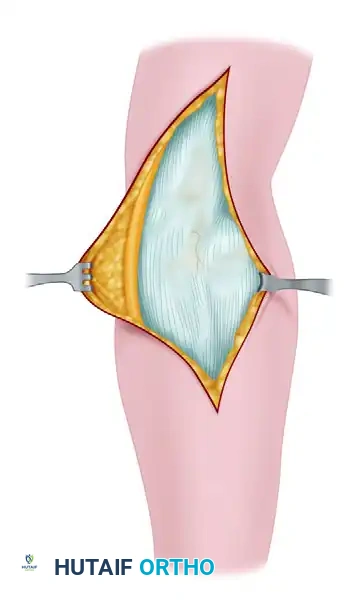
3. Triceps Reflection and V-Y Preparation
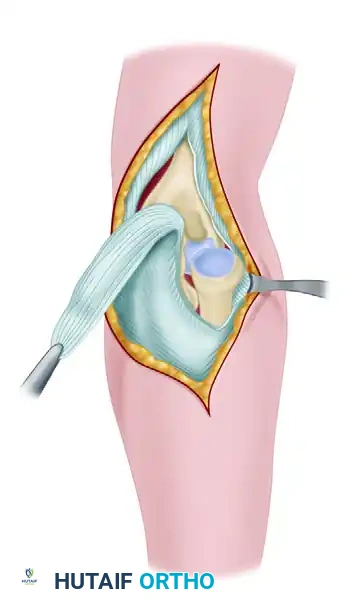
To overcome the profound myostatic contracture of the triceps, a V-Y lengthening is performed. An inverted "V" incision is made through the triceps aponeurosis, with the apex pointing proximally. The triceps muscle is then incised longitudinally.
Using sharp and blunt dissection, the triceps and adjacent musculature are stripped subperiosteally from the distal humerus. This exposes the posterior aspect of the joint and the obliterated olecranon fossa.
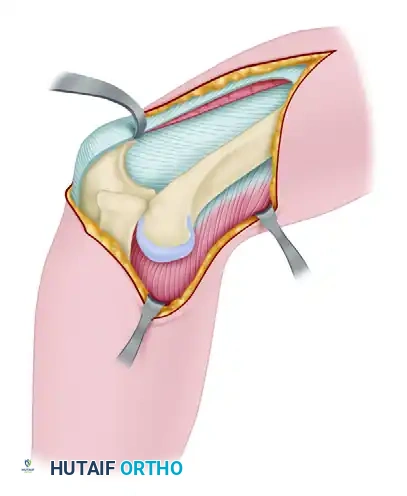
4. Joint Debridement and Extensive Mobilization
The surgeon will encounter a great deal of callus and heterotopic bone on the posterior surface of the humerus and completely filling the olecranon fossa. This is a direct result of the periosteum being stripped and elevated during the initial traumatic event.
Using rongeurs, curettes, and a high-speed burr, this callus and all intervening scar tissue must be meticulously excised. The olecranon fossa must be completely reconstituted to accommodate the olecranon tip during extension.
After completely freeing the distal humerus posteriorly, the dissection is carried anteriorly to expose the radial head and clear the trochlear notch of the ulna. The anterior capsule is often contracted and may require release.
5. The Reduction Maneuver
Reduction must be performed systematically to avoid iatrogenic damage to the fragile, nutrient-deprived articular cartilage.
- Radiocapitellar Reduction: Rotate the forearm and apply gentle, direct pressure on the anterior surface of the capitellum, levering the radial head anteriorly into its normal anatomic position.
- Ulnohumeral Reduction: Once the radial head is reduced (which restores the lateral column length), slip the coronoid process distally and then anteriorly over the trochlea.
Surgical Warning: If the radial head or ulna cannot be reduced easily, do not apply excessive force. Forceful levering will cause catastrophic iatrogenic fractures or shear off the remaining articular cartilage. Instead, dissect the soft tissues more widely, release the contracted collateral ligaments, and clear more scar tissue from the coronoid and olecranon fossae.
6. Joint Stabilization
Once reduced, the joint is carried through a full range of motion to assess stability and identify any impingement. Because the collateral ligaments are chronically attenuated or absent, the elbow is usually grossly unstable.
To maintain the reduction, the olecranon is transfixed to the distal humerus using one or two small Steinmann pins or heavy Kirschner wires. The elbow is held at exactly 90 degrees of flexion during pinning. The pins are cut short, and the proximal portions are bent to prevent intra-articular migration.
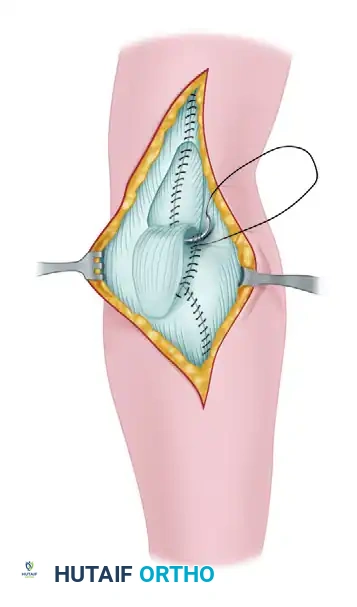
7. Triceps Advancement and Closure
The periosteum and the deep triceps muscle belly are sutured over the posterior surface of the humerus. The fascia over the radial head is repaired if possible.
Finally, the V-Y lengthening is completed. The tongue of the triceps aponeurosis (the inverted "V") is sutured into its normal position or, more commonly, advanced to a slightly more distal level to accommodate the new length of the reduced elbow without placing excessive tension on the repair.
A suction drain is placed deep in the wound to prevent hematoma formation, and the skin is closed in layers.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The postoperative rehabilitation of a chronic elbow dislocation is a delicate balance between protecting the tenuous stability and preventing recurrent stiffness.
- Immediate Postoperative Phase (Days 0-14): The arm is immobilized in a well-padded posterior splint at 90 degrees of flexion. The suction drain is removed after 24 hours.
- Pin Removal (Day 14): The transarticular Steinmann pins are removed approximately 14 days after surgery in the clinic.
- Early Mobilization (Weeks 2-6): Once the pins are removed, the splint is taken off several times a day for gentle, active, and active-assisted range of motion exercises. Passive stretching is strictly avoided to prevent heterotopic ossification and joint subluxation.
- Long-Term Maintenance (Months 2-6): When a moderate range of strong active motion has been regained, the daytime splint may be discarded. However, a static progressive or dynamic splint should be worn at night for an additional 2 to 3 months to maintain extension.
Clinical Pearl: If a dislocation has been present for an extended period, the best functional results are obtained only by continuing disciplined exercises for many months. Children possess a much higher capacity for remodeling and usually regain motion more easily and completely than adults.
ELBOW ARTHROPLASTY FOR CHRONIC DISLOCATIONS
While open reduction is the treatment of choice for younger patients with viable cartilage, most authors agree that an adult elbow that has remained unreduced for longer than 3 to 6 months may require arthroplasty or arthrodesis due to irreversible articular destruction.
Distraction Interpositional Arthroplasty
For patients who are too young or active for a total elbow replacement but have significant joint degeneration or incongruity, interpositional arthroplasty is an excellent salvage option. As described by Morrey, Tan et al., and Lyons and Armstrong, this technique involves reshaping the articular surfaces and interposing a biologic graft (such as autogenous fascia lata or Achilles tendon allograft) between the humerus and the ulna. This is typically protected with a hinged external fixator, which maintains joint distraction, unloads the healing graft, and allows for early, guided range of motion.
Total Elbow Arthroplasty (TEA)
In elderly, low-demand patients with chronic dislocations, primary semiconstrained total elbow arthroplasty is a viable treatment option. Mighell et al. described a series of elderly patients with chronic dislocations (average 17 weeks dislocated) treated with TEA. While the procedure reliably restores motion and stability, surgeons must be aware that the altered soft-tissue mechanics and chronic ligamentous insufficiency can lead to excessive polyethylene wear and premature implant loosening over time.
MANAGEMENT OF ANTERIOR DISLOCATION OF THE RADIAL HEAD
Isolated chronic anterior dislocation of the radial head presents a distinct clinical entity. It may occur as a congenital anomaly, an isolated traumatic event, or in conjunction with a missed fracture of the ulnar shaft (Monteggia fracture-dislocation).
Adult Management
An old anterior dislocation of the radial head in an adult is sometimes compatible with useful function of the elbow. However, terminal flexion is often mechanically blocked by the dislocated head, and the limb usually exhibits weakness and pain. If the disability is severe enough to justify surgery, the treatment of choice in a skeletally mature patient is radial head excision. Attempting to reconstruct the annular ligament in an adult with a chronically deformed radial head is prone to failure and severe stiffness.
Pediatric Management
In a child, the management algorithm is entirely different. While a chronic dislocation may initially be compatible with useful function, as the child continues to grow, the carrying angle increases (cubitus valgus), and the radial head becomes progressively deformed and hypertrophic.
If the child is young, the dislocation is not congenital, and the injury is less than 1 year old, joint preservation is indicated. The Bell Tawse procedure is the standard of care. This involves:
1. Open reduction of the radial head.
2. Reconstruction of the annular ligament (often using a slip of the triceps fascia or lateral band of the triceps).
3. An ulnar osteotomy (to correct the bowing of the ulna and tension the interosseous membrane, which helps hold the radius in place).
Hasler et al. reported highly satisfactory results in children using a combination of open reduction, ulnar osteotomy, and temporary stabilization with an external fixator.
Surgical Warning: Radial head excision is strictly contraindicated in the growing child. Excision before skeletal maturity will lead to proximal migration of the radius, severe cubitus valgus, distal radioulnar joint (DRUJ) disruption, and chronic wrist pain (acquired Madelung-like deformity). If disability is severe, excision must be delayed until physeal closure is complete.
CONCLUSION
The surgical management of an unreduced elbow dislocation is a complex undertaking that requires a deep understanding of elbow kinematics, soft tissue balancing, and advanced reconstructive techniques. The Speed technique, utilizing a V-Y triceps lengthening and meticulous joint clearance, remains the foundation for joint preservation. However, surgeons must be prepared to employ hinged external fixators, interpositional grafts, or total joint arthroplasty when faced with irreversible articular damage. Rigorous, long-term postoperative rehabilitation is just as critical as the surgical execution in achieving a successful functional outcome.
