Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
DEFINITION
The distal ulna is the fixed point 7 around which the radius and the hand function (FIG 1A).Fractures of the distal ulna are often inadequately treated in comparison to its larger counterpart, the radius ( FIG 1B,C).Recent literature has devoted increased attention to the treatment and outcomes of these fractures and associated injuries. 3,10,16,19,20
ANATOMY
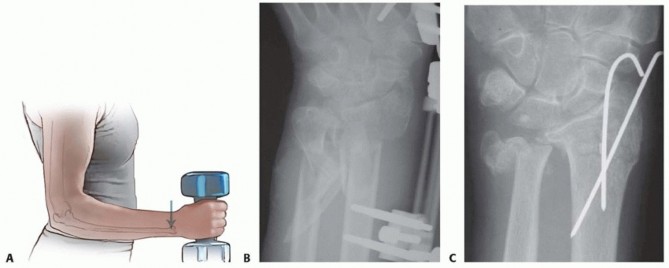
FIG 1 • A. The distal ulna is the fixed point on which performance of most daily hand activities depends. B,C. Fractures of the distal ulna are often neglected in comparison to those of its larger counterpart, the radius, which always attracts attention and treatment efforts. The outcome after distal forearm fractures could be improved if the fixed point—the distal ulna—is addressed surgically at the same time as the radius is operated on.The ligaments run from the fovea of the ulnar head and the base of the ulnar styloid to the dorsal and palmar edges of the sigmoid notch on the distal radius 1,15 (see FIG 2B).
PATHOGENESIS
Isolated ulnar fractures most commonly occur when the forearm is struck by an object, explaining the eponym “nightstick fracture.”Distal ulnar fractures are most often due to a fall on an outstretched hand.It is a common understanding that ulnar-sided injuries are more often caused by falls backward in which the forearm is in supination, loading the ulnar side of the distal forearm and wrist and causing distal ulnar fractures, triquetral chip fractures, TFCC injuries, and so forth.In contrast, radial-sided injuries are more often caused by falls forward, loading the radial side of the forearm and wrist and causing scaphoid fractures, distal radius fractures, and so forth.
NATURAL HISTORY




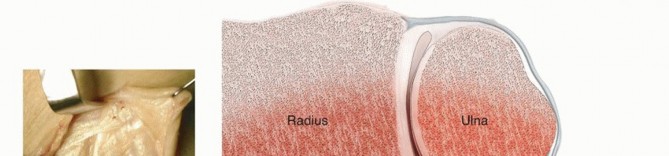
FIG 2 • A. The distal ulna is the fixed point around which the radius rotates in pronation and supination. Through the ulnocarpal ligaments, the distal ulna relates to the hand, allowing daily hand activities. B. The DRUJ is stabilized through the bony congruity between the ulnar head and the sigmoid notch on the radius as well as the dorsal and volar radioulnar ligaments. The radioulnar ligaments include dorsal and volar components that originate on the margins of the sigmoid notch and insert into the fovea and at the base of the ulnar styloid. These ligaments act as reins in the pronation and supination. C. The spheres of the two articular surfaces differ: the ulnar head has a shorter radius of curvature compared with the sigmoid notch.


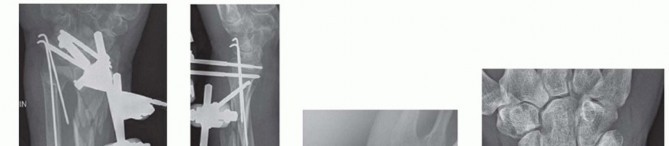
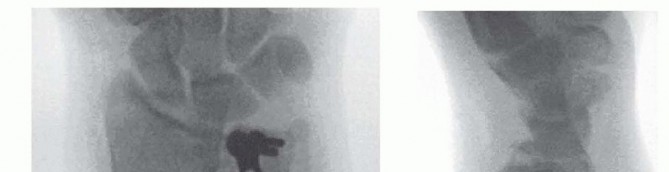
FIG 3 • A,B. Radiographs showing a distal radius fracture together with an ulnar head and styloid fracture. The complexity of the ulnar-sided injury was underappreciated. C. Intraoperative fluoroscopic image after fixation of the distal radius fracture, revealing displaced and unstable ulnar fractures.(continued)
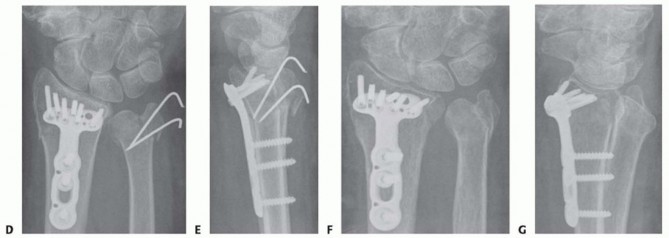
FIG 3 •(continued)D,E. The distal radius fracture was stabilized using a volar locking plate. The ulnar head and styloid fractures were partially reduced and fixed with two Kirschner wires. The surgeon adequately secured the ulnar styloid fracture but not the ulnar head fracture and postoperatively did not restrict forearm rotation. F,G. These radiographs reveal the eventual ulnar head malunion that resulted in DRUJ instability and diminished forearm rotation. The situation was salvaged using an ulnar head replacement prosthesis. DRUJ stability is an important treatment goal.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Posteroanterior, lateral, and oblique radiographs typically reveal the pathology. Computed tomography (CT) is useful in examining articular fractures of the ulnar head. Magnetic resonance imaging (MRI) can be used to evaluate the integrity of the TFCC.Arthroscopy should be considered if a radiograph leads the physician to suspect DRUJ dissociation without radiographic explanations, such as a displaced ulnar styloid base fracture.Diagnostic arthroscopy prior to excision of an ulnar styloid nonunion can be useful to evaluate TFCC integrity. 16
SURGICAL MANAGEMENT
FINDINGS AND INDICATIONS

FIG 4 • A. An undisplaced distal radius fracture with no obvious distal ulna pathology. B. The same fracture with a stress test to the DRUJ, and an obvious DRUJ dissociation is seen as a sign of a complete radioulnar ligament detachment in the absence of an ulnar styloid fracture.
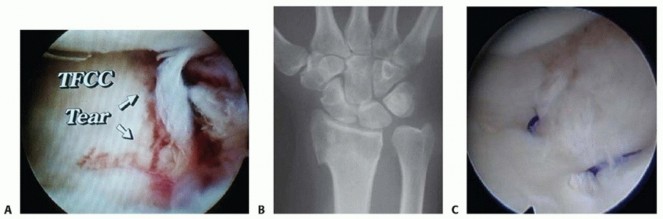

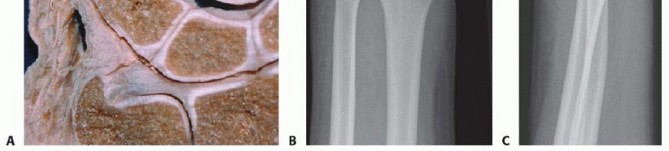

FIG 6 • A. The radioulnar ligament has superficial and deeper components, which insert at the fovea of the ulnar head and partly attach to the base of the ulnar styloid. Consequently, a fracture at the base of the ulnar styloid may or may not detach the main DRUJ-stabilizing ligament. B,C. Ulnar styloid fractures at the base may detach the radioulnar ligament and in the presence of DRUJ instability may require operative intervention. D. Radial displacement (detaching the radioulnar ligament) increases the indication for surgical treatment. E,F. Ulnar styloid tip fractures represent avulsion fractures from the ulnotriquetral collateral ligament. Treatment may not be required in an otherwise stable wrist.
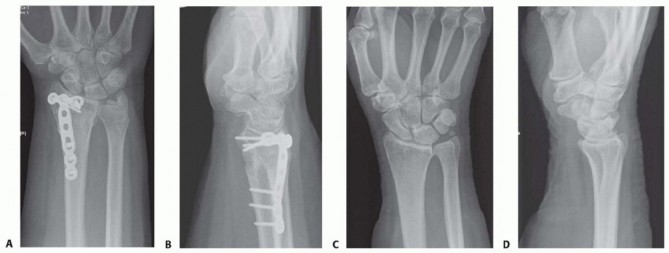
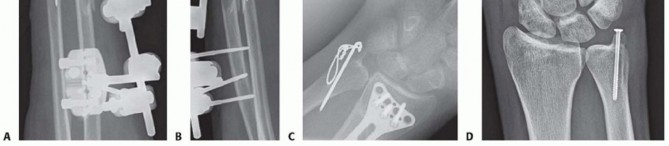
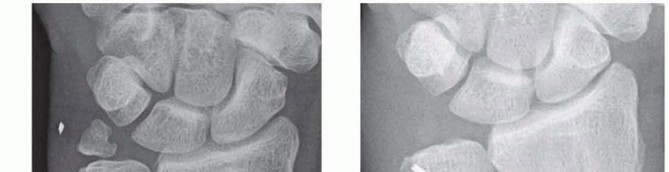
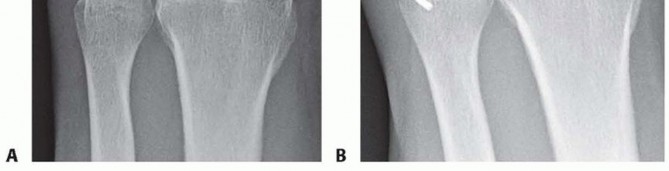
FIG 7 • A,B. Abutment of the ulnar styloid into the triquetrum on the ulnar side of the carpus. C,D. An ulnar styloid nonunion causing problems as a loose body. Ulnar-sided injuries associated with distal radius fractures should be carefully assessed radiographically and clinically after open reduction and internal fixation (ORIF) of the radius fracture.Ulnar fracture reduction and DRUJ joint stability are often improved after treatment of the radius fracture.Stable DRUJ means that the radioulnar ligament is not attached to the fractured ulnar styloid and therefore can be treated nonoperatively.Unstable DRUJ indicates that the radioulnar ligament is detachedwiththe styloid fracture. The styloid should be reduced and stabilized or the ligament reattached.Ulnar Styloid NonunionRecent literature has evaluated the effect of ulnar styloid nonunion on clinical outcomes.No differences have been reported between patients with and without ulnar styloid nonunions. 3,10,20Symptomatic ulnar styloid nonunions have been associated with TFCC tears. 16 Diagnostic arthroscopy at the time of surgical excision of a nonunion may help to identify and repair possible concomitant TFCC pathology.Physical findings of ulnar styloid nonunion may include ulnar-sided wrist pain worse with loading in rotation and tenderness over the ulnar styloid. 3,8 Symptoms from an ulnar styloid nonunion could be related to the following:DRUJ instability from a malfunctioning radioulnar ligament (peripheral TFCC detachment) 8 (see FIG 5B) Impingement of the overlying extensor carpi ulnaris (ECU) tendonAbutment on the carpus 8 (FIG 7A,B)Soft tissue irritation from the loose body ( FIG 7C,D)Ulnar Head FracturesUlnar head fractures are most often associated with distal radius fractures, and the pattern of the distal radius fracture will have a strong influence on the overall functional outcome.Ulnar head fractures are seen either alone or with involvement of extra-articular portions of the distal ulna, proximally toward the diaphysis or distally including the styloid (see FIG 3A,B).Distal Ulnar Neck and Shaft FracturesA distal ulnar neck or distal shaft fracture is a fracture that occurs within 4 cm of the distal dome of the ulnar head ( FIG 8A-D).Some distal ulnar fractures in association with distal radius fractures realign after manipulation and are considered to be stable once the radius is reduced. 17,18It is difficult to immobilize unstable fractures with a cast alone. Three-point fixation, even in an above-elbow cast, is not effective ( FIG 8E,F).Comminuted Intra-articular Distal Ulnar FracturesComminuted distal ulnar fractures that are irreducible and cannot be reconstructed present a challenge to the treating surgeon. 2,5,14,19Salvage procedures such as the Darrach procedure and Sauvé-Kapandji procedure ( FIG 9A,B) have been used as primary options with success.2,19These surgeries may be effective with appropriate patient selection, such as low-demand or elderly patients. 2In cases of severe ulnar fractures in elderly patients, fixing the radius and leaving the ulna unfixed has even been demonstrated as effective. 14If primary fixation is performed, it is generally recommended that the initial approach be geared toward restoring the anatomy and maintaining the overall alignment of the ulna and DRUJ.
APPROACH



FIG 8 • A,B. This ulnar shaft fracture is by definition within 4 cm of the distal dome of the ulnar head. C,D. This ulnar shaft fracture is more proximal and should be considered an isolated ulnar fracture. However, there may still be involvement in the DRUJ, which needs to be taken into account. The DRUJ should be examined for stability after ORIF. E,F. Unstable distal radius and ulnar fractures are difficult to immobilize with casts alone.



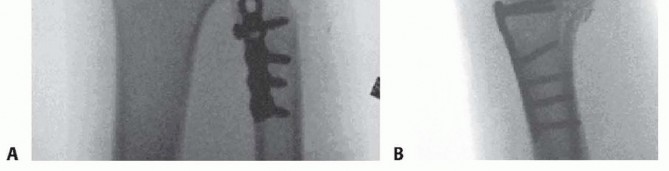
FIG 9 • A,B. AP and lateral radiographs of a Sauvé-Kapandji procedure following traumatic distal ulnar fracture. P.237
TECHNIQUES
INCISION AND EXPOSURE



TECH FIG 1 • Surgical approach to all distal ulnar fractures. A,B. A dorsal zigzag incision is made with the center directed toward the DRUJ. C. Subcutaneous dissection should be performed so that the dorsal cutaneous branch from the ulnar nerve is protected. D. The retinaculum is identified and an approach through the fifth extensor compartment is done. E. The retinaculum is elevated as an ulnarly based flap between the true retinaculum and the separate dorsal sheet for the ECU tendon (which should be preserved). The ECU is thereby kept in its tendon sheath.(continued)
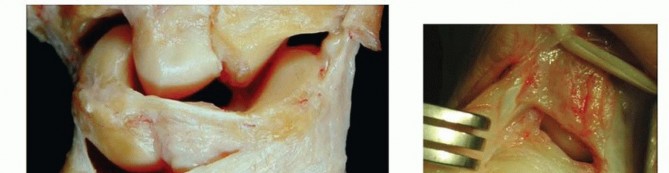
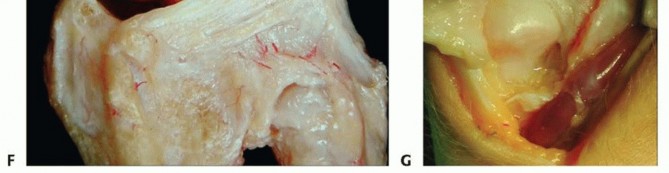
TECH FIG 1 •(continued)F. An ulnarly based capsular flap is raised from the 4-5 septum to gain access to the distal ulna. G. As shown in this dissected specimen, the ulnocarpal joint is often hidden behind the synovium over the meniscus homolog. (C,D: Courtesy of M. Garcia-Elias, Spain.)
ULNAR STYLOID FRACTURES
TECH FIG 2 • The ulnar styloid can be fixed in various ways to secure reattachment of the radioulnar ligament and thereby stabilize the DRUJ. A,B. Single (not rotationally stable) or double Kirschner wires. C. Tension band wiring. D. Screw fixation (not rotationally stable).
ULNAR STYLOID NONUNIONS
TECH FIG 3 • Intraoperative evaluation of the TFCC is essential when performing styloidectomy for ulnar styloid nonunion. A. Preoperative ulnar styloid nonunion. B. Following ulnar styloid excision, the TFCC was repaired using a suture anchor.
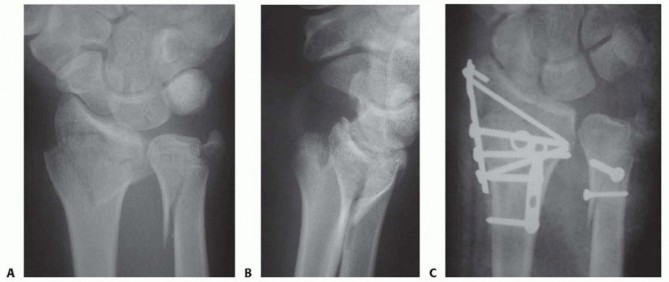
TECH FIG 5 • A,B. AP and lateral radiographs show a dorsally displaced distal forearm fracture. ORIF was performed using both a dorsoradial and a dorsoulnar approach to stabilize the fractures. C. Because of the comminution around the ulnar styloid base, fixation was achieved with a suture loop.6. Comminuted Intra-articular Distal Ulnar FracturesTreatment options exist for comminuted intra-articular distal ulnar fractures:Restoration of the anatomy and overall alignment of the ulna and DRUJ as mentioned earlierThis can be accomplished with manipulation and above-elbow cast immobilization alone or alternatively by surgical means with temporary wiring or external fixation.The potential problems with this management technique are wrist stiffness and reduced forearm rotation that may not be corrected with a late salvage procedure.Primary distal ulnar head replacement 5The theoretical advantage is reduced stiffness (from having early movement) and less DRUJ pain.Total or partial excision of the ulnar head as well as DRUJ arthrodesis with distal ulnar neck resection (Sauvé-Kapandji procedure)Distal ulnar resection with ECU tenodesis (Darrach procedure) 4Care is taken not to resect beyond the proximal portion of the sigmoid notch.
POSTOPERATIVE CARE
P.241Stable fixation of the distal ulnar complex still requires protection postoperatively with a below-elbow splint.Intermediate stable fixation requires 4 weeks of protection using a sugar-tong-type splint to allow flexion and extension of the elbow but protect against uncontrolled pronation and supination.Unstable fixation after internal, external, or nonoperative treatment requires above-elbow protection in neutral forearm rotation to limit movement for the first 6 weeks. There is otherwise a risk that rotational forces will cause a nonunion or malunion.
OUTCOMES
Increased attention to the outcomes of ulnar-sided fractures has demonstrated a trend of equivalent outcomes regardless of treatment or presence of styloid nonunion.DRUJ stability is cited as the most important factor for postoperative satisfaction.With greater understanding of the relationship between the ulnar styloid, the radioulnar ligament, and the TFCC, improved outcomes can be achieved.
COMPLICATIONS
Stiffness of the DRUJ with limited pronation and supination Prominent hardware with operative fixationInfection NonunionMalunion
REFERENCES
- af Ekenstam F, Hagert CG. Anatomical studies on the geometry and stability of the distal radio ulnar joint. Scand J Plast Reconstr Surg 1985;19:17-25.
- Arora R, Gabl M, Pechlaner S, et al. Initial shortening and internal fixation in combination with a Sauvé-Kapandji procedure for severely comminuted fractures of the distal radius in elderly patients. J Bone Joint Surg Br 2010;92:1158-1562.
- Buijze GA, Ring D. Clinical impact of united versus nonunited fractures of the proximal half of the ulnar styloid following volar plate fixation of the distal radius. J Hand Surg Am 2010;35:223-227.
- Darrach W. Partial excision of lower shaft of ulna for deformity following Colles's fracture. 1913. Clin Orthop Relat Res 1992;(275):3-4.
- Grechenig W, Peicha G, Fellinger M. Primary ulnar head prosthesis for the treatment of an irreparable ulnar head fracture dislocation. J Hand Surg Br 2001;26(3):269-271.
- Hagert CG. Current concepts of the functional anatomy of the distal radioulnar joint, including the ulnocarpal junction. In: Büchler U, ed. Wrist Instability. Berlin: Martin Dunitz, 1996:15-21.
- Hagert CG. The distal radioulnar joint in relation to the whole forearm. Clin Orthop Relat Res 1992;(275):56-64.
- Hauck RM, Skahen J III, Palmer AK. Classification and treatment of ulnar styloid nonunion. J Hand Surg Am 1996;21(3):418-422.
- Jakab E, Ganos DL, Gagnon S. Isolated intra-articular fractures of the ulnar head. J Orthop Trauma 1993;7:290-292.
- Kim JK, Koh YD, Do NH. Should an ulnar styloid fracture be fixed following volar plate fixation of a distal radial fracture? J Bone Joint Surg Am 2010;92:1-6.
- Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar instability after distal radius fractures. J Hand Surg Am 2000;25(3):464-468.
- Lindau T, Arner M, Hagberg L. Intraarticular lesions in distal fractures of the radius in young adults: a descriptive arthroscopic study in 50 patients. J Hand Surg Br 1997;22(5):638-643.
- May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27(6): 965-971.
- Namba J, Fujiwara T, Murase T, et al. Intra-articular distal ulnar fractures associated with distal radial fractures in older adults: early experience in fixation of the radius and leaving the ulna unfixed. J Hand SurgEur Vol 2009;34:592-597.
- Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist—anatomy and function. J Hand Surg Am 1981;6(2):153-162.
- Protopsaltis TS, Ruch DS. Triangular fibrocartilage complex tears associated with symptomatic ulnar styloid nonunions. J Hand Surg Am 2010;35:1251-1255.
- Richards TA, Deal DN. Distal ulna fractures. J Hand Surg Am 2014;39:385-391.
- Ring D, McCarty PL, Campbell D, et al. Condylar blade plate fixation of unstable fractures of the distal ulna associated with fractures of the distal radius. J Hand Surg Am 2004;29(1):103-109.
- Ruchelsman DE, Raski KB, Rettig ME. Outcome following acute primary distal ulna resection for comminuted distal ulna fractures at the time of operative fixation of unstable fractures of the distal radius. Hand 2009;4:391-396.
- Zenke Y, Sakai A, Oshige T, et al. The effect of an associated ulnar styloid fracture on the outcome after fixation of a fracture of the distal radius. J Bone Joint Surg Br 2009;91:102-107.
