Open Reduction and Internal Fixation of Supracondylar and Intercondylar Fractures
PATIENT HISTORY AND PHYSICAL FINDINGS
Distal humerus fractures occur in two age groups:Younger patients who sustain high-energy trauma Older patients with underlying osteopeniaComminution is the dominant feature of supracondylar and intercondylar fractures and complicates internal fixation. The complicated skeletal geometry of the distal humerus also contributes.The goals of the initial evaluation are to Understand the fracture patternDetermine the existence of previous symptomatic elbow pathologyDetermine the extent of associated soft tissue (open fractures) Identify associated musculoskeletal or neurovascular injuries
IMAGING AND OTHER DIAGNOSTIC STUDIES

FIG 1 • A,B. Anteroposterior (AP) and lateral radiographs showing a comminuted intra-articular supraintercondylar fracture of the distal humerus. The complexity of the fracture is difficult to appreciate fully because of the geometry of the distal humerus, fracture comminution, and fragment overlapping. C,D. The use of CT with three-dimensional reconstruction and surface rendering helps understand the fracture configuration and anticipate the surgical findings. Traction radiographs obtained in the operating room with the patient under anesthesia just before surgery also can be helpful, especially if a CT scan is not available.
SURGICAL MANAGEMENT
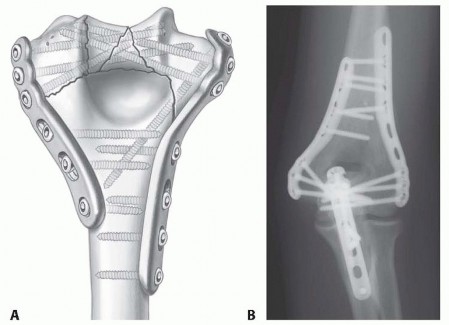
FIG 2 • A. Internal fixation using two parallel medial and lateral plates allows maximal fixation of the plates in the distal fragments and increased stability at the supracondylar level. B. This postoperative AP radiograph shows anatomic reduction of a complex distal humerus fracture and stable fixation using the principles and technique described in this chapter. The olecranon osteotomy was fixed with a plate. (A: Copyright Mayo Clinic.) Distal screw fixation contributes to stability at the supracondylar level, where true interfragmentary compression is achieved.
APPROACHES
Adequate exposure is necessary to achieve satisfactory reduction and fixation.The management of the ulnar nerve is controversial; some surgeons favor routine subcutaneous transposition, whereas others prefer to leave the nerve in its anatomic location at the end of the procedure. A number of patients will develop a transitory or permanent ulnar neuropathy, mostly sensitive, regardless of nerve management; preoperative counseling is important in this regard.Most fractures require mobilization of the extensor mechanism of the elbow through an olecranon osteotomy, triceps reflection, or triceps split. Simple fractures occasionally may be addressed working on both sides of the triceps without mobilization of the extensor mechanism.Olecranon osteotomy is the preferred surgical approach for internal fixation for most distal humerus fractures. 13 AdvantagesProvides excellent exposureOffers the potential of bone-to-bone healing, thereby limiting the risk of triceps dysfunction DisadvantagesComplications: nonunion, intra-articular adhesions Hardware removal may be needed.Limits the ability for intraoperative conversion to elbow arthroplasty May devitalize the anconeus muscleThe proximal ulna cannot be used as a template to judge reduction and motion.Triceps reflection and triceps split 9 allow preservation of the intact ulna. Avoid complications related to olecranon osteotomy.Facilitate intraoperative conversion to total elbow arthroplasty.Allow use of the proximal ulna as a template for reduction of the distal humerus articular surface.Allow assessment of extension deficit after fracture fixation, which is especially useful in fractures requiring metaphyseal shortening.Bilaterotricipital approach 1 Goals and indicationsThe goal is to provide adequate exposure for fracture fixation without violating the extensor mechanism.This approach is used only for the more simple fracture patterns (eg, extra-articular or simple intra-articular distal humerus fractures [AO/OTA A, C1, C2]) or when elbow arthroplasty is being considered.AdvantagesThis approach avoids complications related to the extensor mechanism. No postoperative protection is needed.Surgical time is decreased. DisadvantageThe procedure provides limited exposure of the articular surface.
TECHNIQUES
Surgical Approach
SURGICAL APPROACH
OLECRANON OSTEOTOMY


TECH FIG 1 • Olecranon osteotomy provides an excellent exposure for distal humerus fracture fixation. A. A chevron osteotomy is initiated with a microsagittal saw and completed with an osteotome. Drilling and tapping before performing the osteotomy facilitates fixation of the osteotomy if screw fixation is selected. B. Proximal mobilization of the osteotomized fragment and triceps allows ample exposure of the articular surface and columns. C. Fixation may be performed with a cancellous screw and tension band, wires and a tension band, or a plate. The author's preferred method uses K-wires plus a tension band in patients with good bone quality and plate fixation in patients with osteopenia.If screw fixation is planned, drill and tap the ulna before performing the osteotomy.Plate fixation provides improved fixation, but the risk of wound complications is increased.There is substantial interest in the development of intramedullary fixation devices locked proximally and distally; they would combine the benefits of stability and intramedullary location, which could lead to a decreased rate of wound complications and painful hardware requiring removal.
TRICEPS REFLECTION AND TRICEPS SPLIT
Bryan-Morrey triceps-sparing approach ( TECH FIG 2)The triceps is elevated from the medial intermuscular septum and the posterior aspect of the humeral shaft. The forearm fascia and periosteum are incised just lateral to the flexor carpi ulnaris.The triceps, forearm fascia, and anconeus are elevated in continuity from medial to lateral.When this approach is used for fracture fixation, the anterior bundle of the medial collateral ligament and the lateral ulnar collateral ligament must be preserved to avoid postoperative instability.Mayo-modified extensile Kocher approachThe triceps is elevated from the lateral intermuscular septum and the posterior aspect of the humeral shaft. The triceps and anconeus are elevated in continuity from lateral to medial.As noted earlier, the anterior bundle of the medial collateral ligament and the lateral ulnar collateral ligament must be preserved to avoid postoperative instability.
BILATEROTRICIPITAL APPROACH
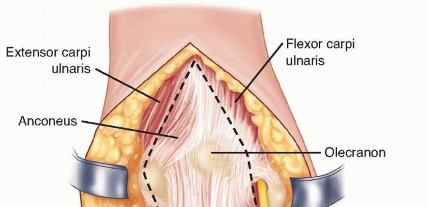
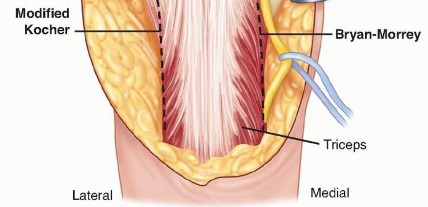
TECH FIG 2 • The extensor mechanism (ie, triceps, anconeus, and forearm fascia) may be elevated off the ulna subperiosteally in continuity from medial to lateral (Bryan-Morrey approach) or from lateral to medial (Mayo-modified extensile Kocher approach).
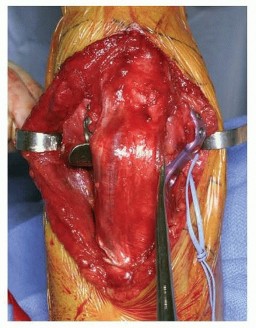
TECH FIG 3 • Fractures with no or limited articular involvement may be fixed working on both sides of the triceps. As shown in this image, the extensor mechanism is left mostly undisturbed.
Internal Fixation
INTERNAL FIXATION
TECHNICAL OBJECTIVES
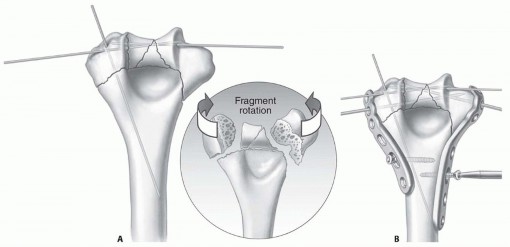
TECH FIG 4 • A. Anatomic reduction of the articular surface is maintained provisionally with fine wires placed so that they will not interfere with plate and screw application. B. The medial and lateral plates are held in place provisionally with two distal 2.0-mm pins (which later will be replaced by screws) and two proximal screws through an oval hole to allow small adjustments in plate positioning. (Copyright Mayo Clinic.) Plates are used for fixation.Plates should be applied such that compression is achieved at the supracondylar level for both columns.Plates must be strong enough and stiff enough to resist breaking or bending before union occurs at the supracondylar level. Provisional Assembly of the Articular Surface and Plate Placement Reduce the articular surface fragments anatomically.The proximal ulna and radial head may be used as templates. Rotational alignment should be carefully assessed.Use smooth K-wires to maintain the reduction provisionally ( TECH FIG 4A).Two 2.0-mm smooth wires introduced at the medial and lateral epicondyles facilitate provisional placement of the plates and can be replaced by screws later.Fine-threaded wires, absorbable pins or very small screws may be used for definitive fixation of small fracture fragments.Medial and lateral plates are placed so that one of the distal holes of each plate slides over the medial and lateral 2.0-mm smooth wires introduced at the medial and lateral epicondyles ( TECH FIG 4B).P.137One cortical screw is loosely introduced into a slotted hole of each plate to hold the plates in place; use of slotted holes for these screws facilitates later adjustments in plate positioning.
ARTICULAR AND DISTAL FIXATION
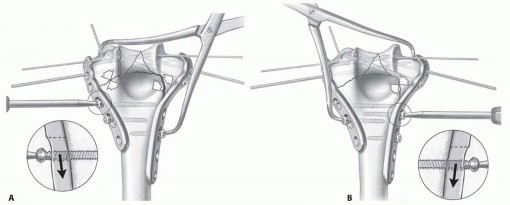
Two or more distal screws are inserted through the plates medially and laterally. As noted, the screws should be as long as possible and engage fragments on the opposite column.Before screw application, a large bone clamp is used to compress the articular fracture lines, unless there is comminution of the articular surface.The two 2.0-mm smooth pins may be replaced with distal screws without previous drilling to avoid accidental breakage of the drill when contacting the other screws. Usually, these last screws will interdigitate with the previously applied distal screws, thereby increasing the stability of the construct ( TECH FIG 5). Supracondylar Compression and Proximal Plate Fixation

TECH FIG 5 • Maximal distal plate anchorage is then achieved by insertion of multiple long screws through the plates and into the distal fragments. Usually, the screws from the medial and lateral directions will engage, creating an interlocked structure that increases fracture stability. (Copyright Mayo Clinic.)
TECH FIG 6 • A,B. Supracondylar compression is achieved with the use of a large clamp, insertion of screws in the compression mode, and slight undercontouring of the plates. The same technique is applied laterally and medially.(continued)
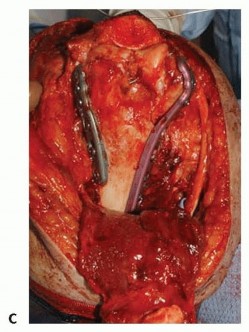
TECH FIG 6 •(continued)C. Internal fixation of a complex distal humerus fracture. (A,B: Copyright Mayo Clinic.)
SUPRACONDYLAR SHORTENING


TECH FIG 7 • In cases of severe supracondylar comminution, adequate interfragmentary contact and compression takes priority over anatomic reduction. The humerus may be shortened anywhere from a few millimeters to 2 cm by trimming the bony spikes of the diaphysis (A), advancing the distal segment proximally and anteriorly, and fixing it in a nonanatomic fashion (B). C. The olecranon fossa is recreated in this case by removing bone from the posterior aspect of the diaphysis with a burr. (A,B: Copyright Mayo Clinic.) The distal fragments are translated proximally and anteriorly. Anterior translation is necessary to create room for the radial head and the coronoid in flexion.The fracture is fixed in the desired position using the technique described previously.A new deep and wide olecranon fossa is created by removing bone from the distal and posterior aspect of the diaphysis ( TECH FIG 7C). Otherwise, extension will be restricted.P.139
PEARLS AND PITFALLS
POSTOPERATIVE MANAGEMENT
After closure, the elbow is placed in a bulky, noncompressive dressing with an anterior plaster splint to maintain the elbow in extension, and the upper extremity is kept elevated.In patients with severe swelling, open fractures or compromised soft tissues consideration should be given to an incisional or standard vacuum-assisted closure device.Motion is initiated according to the extent of soft tissue damage. Motion usually can be initiated on the first or second postoperative day, but it may be necessary to wait for several days in the case of open fractures or severe soft tissue damage.Most patients benefit from a program of continuous passive motion for the first week or two after fixation; some may benefit from a longer period of passive motion.When postoperative motion fails to progress as expected, a program of patient-adjusted static flexion and extension splints is implemented.Treatment with indomethacin or single-dose radiation to the soft tissues shielding the fracture site may be considered for patients with high risk of heterotopic ossification, such as those with associated head or spinal trauma as well as those who require several surgeries in a short period of time. However, failure to shield the fracture site or the olecranon osteotomy seems to lead to a higher rate of nonunion.
OUTCOMES
The results of internal fixation for fractures of the distal humerus using modern techniques are summarized in Table 1.The results of the different studies are difficult to interpret because the severity of the injuries included cannot be compared, and there may be variations in the accuracy of range-of-motion measurements.Improvements in fixation techniques have resulted in a decreased rate of hardware failure and nonunion, but range of motion is not reliably restored in every patient. In addition, other complications remain relatively common 8 as detailed below.Olecranonosteotomy1.Position the apex of the osteotomy distally.2.Use a thin oscillating saw to minimize bone loss.3.If plate fixation is preferred, consider drilling the holes for the plate before beginning the osteotomy. This facilitates plate fixation of the osteotomy at the conclusion of the surgery.4.Similarly, if tension band fixation with an intramedullary screw is preferred, predrill and tap the screw hole.Triceps reflectionand triceps split1.Subperiosteal detachment of the extensor mechanism is critical to preserve its thickness and facilitate a strongreattachment.2.Reproduce anatomic reattachment of the extensor mechanism.3.Use heavy, nonabsorbable suture (no. 5 Ethibond [Ethicon, Inc., Somerville, NJ] or no. 2 FiberWire [Arthrex, Inc., Naples, FL]) through bone.4.Protect extension against resistance for 6 weeks.Bilaterotricipitalapproach1.Separate the triceps from the underlying medial and lateral joint capsules.2.Resect the posterior capsule and fat pad to improve visualization.
COMPLICATIONS
Infection NonunionStiffness, with or without heterotopic ossificationNeed for removal of the hardware used for fixation of the olecranon osteotomy Ulnar neuropathyPosttraumatic osteoarthritis or avascular necrosis requiring interposition arthroplasty or elbow replacementP.140 Table 1 Results of Internal Fixation for Distal Humerus Fractures Affecting the Humeral Columns Study|No.|Mean Age (Range) (y)|Followup (mo)|Fracture Type (no.) (AOClassification)|Open|Mean Degrees ROM(range)|Overall results|Complications (no.)|Reoperations (no.)---------------|---Jupiter et|34|57 (17-|70 (25-|C1 (13)|14|76%|79%|Nonunion (2)|Hardwareal 5||79)|139)|C2 (2)|(41%)|achieved|satisfactory|Refracture (1)|removal (24)||||C3 (19)||at least||Olecranon|Capsulectomy||||||30-120||osteotomy|(3)||||||||nonunion (2)|HO removal||||||||Class II HO|(1)||||||||(1)|Nerve||||||||Ulnar|decompression||||||||neuropathy|(4)||||||||(4)|||||||||Median|||||||||neuropathy|||||||||(1)|Henley et|33|32 (15-|18.3|C1 (23)|14|Mean|92%|Hardware|Repeat ORIFal 4||61)||C2 (8)C3 (2)|(42%)|extension, 19; mean flexion, 126|satisfactory * (only 25 patients evaluated)|failure (5)Infection (2) Olecranon osteotomy nonunion (2)|(2)TBW removal (6)Olecranonosteotomy||||||||Class II HO|repeat||||||||(2)|ORIF (2)Sanders|17|51 (12-|> 24|C1 (4)|7|108 (55-|76%|Delayed|Hardwareet al 17||85)||C2 (3)|(41%)|140)|satisfactory|union (2)|removal (3)||||C3 (10)||||Infection (2)|Ulnar nerve||||||||Pulmonary|decompression||||||||embolism (1)|(1)||||||||Ulnar|||||||||neuropathy|||||||||(1)|McKee et|25|47 (19-|37 (18-|C (25)|None|108 (55-|Mean|Ulnar neuritis|TBW removalal (closed||85)|75)|||140)|DASH: 20|(3)|(3)fractures) 7|||||||(0-55)|Transient radial nerve|Repeat ORIF (1)||||||||palsy (1)|Elbow release||||||||Nonunion (1)|(2)||||||||Malunion (1)|McKee et|26|44 (17-|51 (10-|C1 (5)|100%|97 (55-|Mean|Septic|Repeat ORIFal (open||78)|141)|C2 (13)||140)|DASH: 23.7|nonunion (1)|(3)fractures) 6||||C3 (8)|||(0-57.5)|Delayed||||||||60%|union (4)||satisfactoryMEPS|Transient radial nerve palsy (1)|------|---Pajarinen 21|44 (16-|24 (10-|C1 (6)|5|107 (98-|56%|Deep|Repeat ORIFet al 11|81)|41)|C2 (12)|(24%)|116)|satisfactory|infection (1)|(2)|||C3 (3)|||OTA|Nonunion (2)||||||||Traumatic||||||||nerve injuries||||||||(3)||||||||Olecranon||||||||osteotomy||||||||nonunion (1)|Gofton et 23|53 (16-|45 (14-|C1 (3)|7|122|Mean|Deep|Olecranonal 3|80)|89)|C2 (11)|(30%)|(extension|DASH: 12|infection (1)|osteotomy|||C3 (9)||loss, 19 ±|(0-38)|Olecranon|repeat|||||12;|Subjective|osteotomy|ORIF (2)|||||flexion,142|satisfaction:|nonunion (2)|Elbow release|||||± 6)|93%|Class II HO|(3)||||||87%|(3)|Capitellar||||||satisfactory|Avascular|ORIF (1)||||||MEPS|necrosis (1)||||||||Reflex||||||||sympathetic||||||||dystrophy (1)||||||||Capitellar||||||||nonunion (1)|Soon et 15|43 (21-|12 (2-|B (3)|None|109 (45-|86%|Transient|Total elbowal 19|80)|27)|C1 (4)||145)|satisfactory|ulnar neuritis|arthroplasty (1)|||C2 (4)|||MEPS|(2)|Repeat ORIF|||C3 (4)||||Hardware|(3)|||||||failure (3)|Elbow|||||||Nonunion (1)|manipulation||||||||or release (4)Sanchez- 32|58 (16-|24 (12-|A3 (3)|13|Mean|83%|Delayed|WoundSotelo et|99)|60)|C2 (4)|(44%)|extension:|satisfactory|union (1)|débridement oral 15|||C3 (25)||26 (0-55)|MEPS|Ulnar|coverage (4)|||||Mean||neuropathy|Bone grafting|||||flexion:||(6)|(1)|||||124 (80-||Class II HO|HO removal|||||150)||(5)|(4)|||||||Infection (1)|HO removal||||||||and distraction||||||||arthroplasty (1)||||||||Triceps||||||||reconstruction||||||||(1)ROM, range of motion; Class II HO, heterotopic ossification restricting motion; ORIF, open reduction and internal fixation; TBW, tension band wiring; DASH, Disabilities of the Arm, Shoulder and Hand questionnaire; MEPS, Mayo Elbow Performance Score; OTA, Orthopaedic Trauma Association.According to the Jupiter rating system.P.141*
REFERENCES
- Alonso-Llames M. Bilaterotricipital approach to the elbow. Its application in the osteosynthesis of supracondylar fractures of the humerus in children. Acta Orthop Scand 1972;43:479-490.
- Athwal GS, Rispoli DM, Steinmann SP. The anconeus flap transolecranon approach to the distal humerus. J Orthop Trauma 2006;20: 282-285.
- Gofton WT, Macdermid JC, Patterson SD, et al. Functional outcome of AO type C distal humeral fractures. J Hand Surg Am 2003;28:294-308.
- Henley MB, Bone LB, Parker B. Operative management of intra-articular fractures of the distal humerus. J Orthop Trauma 1987;1:24-35.
- Jupiter JB, Neff U, Holzach P, et al. Intercondylar fractures of the humerus. An operative approach. J Bone Joint Surg Am 1985;67:226-239.
- McKee MD, Kim J, Kebaish K, et al. Functional outcome after open supracondylar fractures of the humerus. The effect of the surgical approach. J Bone Joint Surg Br 2000;82(5):646-651.
- McKee MD, Wilson TL, Winston L, et al. Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82-A(12): 1701-1707.
- Lawrence TM, Ahmadi S, Morrey BF, et al. Wound complications after distal humerus fracture fixation: incidence, risk factors and outcome. J Shoulder Elbow Surg 2014;23(2):258-264.
- Morrey BF. Anatomy and surgical approaches. In: Morrey BF, ed. Joint Replacement Arthroplasty. Philadelphia: Churchill-Livingstone, 2003:269-285.
- O'Driscoll SW, Sanchez-Sotelo J, Torchia ME. Management of the smashed distal humerus. Orthop Clin North Am 2002;33:19-33.
- Pajarinen J, Björkenheim JM. Operative treatment of type C intercondylar fractures of the distal humerus: results after a mean follow-up of 2 years in a series of 18 patients. J Shoulder Elbow Surg 2002;11:48-52.
- Popovic D, King GJ. Fragility fractures of the distal humerus: what is the optimal treatment? J Bone Joint Surg Br 2012 94(1):16-22.
- Ring D, Gulotta L, Chin K, et al. Olecranon osteotomy for exposure of fractures and nonunions of the distal humerus. J Orthop Trauma 2004;18:446-449.
- Sanchez-Sotelo J. Distal humeral fractures: role of internal fixation and elbow arthroplasty. J Bone Joint Surg Am 2012;94(6):555-568.
- Sanchez-Sotelo J, Torchia ME, O'Driscoll SW. Complex distal humeral fractures: internal fixation with a principle-based parallel-plate technique. J Bone Joint Surg Am 2007;89(5):961-969.
- Sanchez-Sotelo J, Torchia ME, O'Driscoll SW. Principle-based internal fixation of distal humerus fractures. Tech Hand Upper Extremity Surg 2001;5:179-187.
- Sanders RA, Raney EM, Pipkin S. Operative treatment of bicondylar intraarticular fractures of the distal humerus. Orthopedics 1992;15: 159-163.
- Simone JP, Streubel PN, Sanchez-Sotelo J, et al. Low transcondylar fractures of the distal humerus: results of open reduction and internal fixation. J Shoulder Elbow Surg 2014;23(4):573-578.
- Soon JL, Chan BK, Low CO. Surgical fixation of intra-articular fractures of the distal humerus in adults. Injury 2004;35:44-54.
